Full Length Research Paper

ABSTRACT
Pregnancy-induced hypertension has remained a significant cause of prenatal morbidity and mortality of mothers. So this study aims to assess renal function test, serum total protein, and lipid profile concentrations among pregnancy-induced hypertension women in Asrade Zewudie Memorable hospital (ASZMPH), Gojjam, Ethiopia. A case-control study was done on 200 pregnant women: 100 with pregnancy-induced hypertension (case group) and 100 normotensives (control group) at Asrade Zewudie Memorable Primary hospital Gojjam, Ethiopia from January 24, 2020 to April 30, 2020. 5 ml of venous blood was collected on the SST test tube and analyzed for serum lipid profile, renal function test, and serum total protein. The analysis was done by using SPPS software (version 20.0). The level significance was set at a 95% confidence interval (P-value less than 0.05 was considered clinically significant). In the present study, there was a significant increase in the serum TC, TGs, blood urea, serum creatinine, and LDL (p < 0.05) and a significant decrease in HDL cholesterol in case groups as compared to normal groups (p < 0.05). The elevation of serum total protein was not significant (p >0.05). The outcome of the final multiple logistic regression model indicate that factors like BMI, habits of doing scheduled exercise, habit of drinking alcohol, habit of fruit consumption, trimester and gravidity had significant association with lipid profile tests of the study participants. In the present study, the degree of association between different risk factors selected in multiple logistic regression and lipid profile tests was more significant in case group relative with control group. According to the result of this study, early detection of altered lipid profile and renal function test in preeclamptics showed the incidence of complications can be decreased, which in turn reduces the materno-fetal morbidity and mortality.
Key words: Lipid profile, serum total protein, renal function test, PIH, and Ethiopia
Abbreviation: AOR, Adjusted odd ratio; BMI, body mass index; CDC, Center of Disease Control Center; DBP, diastolic blood pressure; GFR, glomerular filtration rate; HDL, high-density lipoprotein; HDP, hypertension disorder of pregnancy; IQC, internal quality control; LDL, low-density lipoprotein; PIH, pregnancy induced hypertension; SBP, systolic blood pressure; SOPs, standard operating procedures; SST, serum separated tube; TC, total cholesterol; TG, triglyceride; WHO, World Health Organization.INTRODUCTION
Pregnancy-Induced Hypertension (PIH) also referred to as Gestational Hypertension (GH); is a multifactorial condition occurring during pregnancy, usually appears after the 20th week of gestation and characterized by high blood pressure (over 140/90) present during pregnancy (van Balen et al., 2018 and Topel et al., 2018).
PIH can lead to more serious maternal complications called preeclampsia, which is characterized by a hypertensive state, systemic vascular disturbances, and reduced blood flow to multiple organs of both mothers and babies. If left untreated, hypertension can prevent the placenta from getting enough blood and this limits the baby from getting enough oxygen and food (Brown et al., 2018; Pauli and Repke, 2017; Mol et al., 2016; Bibbins-Doming et al., 2017; Sroussi et al., 2017).
Pregnancy-induced hypertension is classified into three main classes. The first one is chronic hypertension which is defined by women with high blood pressure (over 140/90) before pregnancy, early in pregnancy (before 20 weeks), or persisting longer than 12 weeks after delivery. The second class is gestational hypertension characterized by a woman with high blood pressure that develops after 20 weeks’ gestation in pregnancy and goes away after delivery. And the third one, preeclampsia which is defined both by chronic and gestational hypertension, can lead to this severe condition after 20 weeks of pregnancy (Brown et al., 2018; Pauli and Repke, 2017).
The incidence of preeclampsia globally is about 2 - 10 % of all pregnancies (Ghodke et al., 2017). Women with first-time pregnancy, whose parents had PIH, who are carrying multiples, younger than age 20 or older than age 40 and who had high blood pressure or kidney disease before pregnancy may have an increased risk of developing gestational hypertension (English et al., 2015). PIH continues to be a major obstetric problem in the present-day (Kar et al., 2016). Currently, some studies show that elevation of plasma lipids level occurs during pregnancy due to alteration in hormones; usually, levels of lipids revert to normal shortly after delivery physiologically. But in the case of preeclampsia endocrinological, alteration is more and change in serum lipids cannot easily revert to normal (Soma-Pillay et al, 2016). Accumulation due to systemic vascular disturbances causes endothelial dysfunction and this leads to abnormal lipid metabolism associated with oxidative stress (Gupta et al., 2005, Serrano et al., 2018; Gao et al., 2018). An association of serum lipid profile with gestational proteinuric hypertension is highly suggested to reflect some new diagnostic tools. Moreover, the hormonal imbalance is a prime factor for the pathogenesis of PIH and this endocrinal imbalance is well reflected in alteration of serum lipid profile (Yadav et al., 2018; Singh et al., 2015; Wild et al., 2015).
Serum total protein is important in regulating blood volume by maintaining the oncotic pressure (colloid osmotic pressure) of the blood compartment (Al Ghazali et al., 2014). Proteinuria in pregnancy can indicate primary preeclampsia, renal disease, or renal disease secondary to systemic disorders, such as diabetes or primary hypertension (Thadhani and Maynard, 2015, Phillips et al, 2017; Hong et al., 2016). During physiological pregnancy in most women, urinary protein excretion normally increases from its normal value because of increased GFR, the permeability of the glomerular basement membrane and reduction of tubular reabsorption of filtered protein; however, if it exceeds 300 mg/24 h, it is abnormal (Thadhani and Maynard, 2015 and Phillips et al., 2017).
Pregnancy-induced hypertension has remained a significant global public health threat in both developed and developing countries. This disorder contributes greatly to prenatal morbidity and mortality of mothers. Additionally, with its complication in mothers, it has a greater effect in a fetus, by resulting in various complications like intrauterine, preterm delivery, premature delivery, fetal growth restriction , abruption placenta, etc (Osungbade and Ige, 2011, Gaym et al, 2011; Abdella, 2010; Wolde et al., 2011; Nugteren et al., 2012; WHO, 2015).
According to 2015 WHO reports, approximately 25.7% women died globally, of which 99% of deaths occur in Latin-American, Asian and African countries. The reports also indicate that Sub-Saharan Africa account for about 56% of all maternal deaths which shows that pregnancy-related complications in developing countries are 14 times higher than in developed countries (UNICEF, 2015). In Ethiopia, PIH is a common maternal medical complication during pregnancy (Awoke et al., 2012). Studies in Ethiopia showed that the incidence of PIH is approximately 16% in association with preeclampsia/ eclampsia and increased rapidly from time to time with an incidence between 5 and 10% (Teklu and Gaym, 2006). This study aimed to assess renal function test, total protein and lipid profile concentrations among pregnancy-induced hypertension women in Asrade Zewudie Memorable Primary Hospital (AZMPH), Gojjam, Ethiopia, and to put some diagnostic indications to physicians.
MATERIALS AND METHODS
Study area/setting
The study was conducted at Asrade Zewudie Memorable Primary Hospital, the governmental hospital located in Burie town, west Gojjam (Mirab Gojjam), Amhara, Ethiopia.
Study design and period
A prospective study was done in AZMPH, Gojjam, Ethiopia. The data was collected from January 24, 2020, to March 26, 2020, an analysis was done in the period between March 29, 2020 to April 30, 2020. The study was a case-control study that is done on pregnant women by classifying them into two groups depending on the blood pressure during the pregnancy period by grouping them as cases and controls.
Population
Source population
The study population was all pregnant mothers attending the maternity centers of AZMPH, Gojjam, Ethiopia, during the study period.
Study population
The study population consists of a total of 200 pregnant women with a gestational period of greater than 20 weeks (100 for each group) divided into two groups. A case/control group was a mother diagnosed to have hypertensive disorders of pregnancy ( > 140/90 mmHg) by an obstetrician or by the physician who is assigned in the maternity wards during the antenatal period and control groups was mothers without PIH (BP < 140/90 mmHg). The two study groups were similar almost in many characteristics with the only difference between those in the presence or absence of pregnancy-induced hypertension.
Inclusion criteria
All pregnant women in the maternity ward with a gestational age greater than 20 weeks were prepared for the two groups.
Exclusion criteria
Pregnant women with a gestational age of fewer than 20 weeks, have a history of chronic hypertension before pregnancy, with complicated problems and unable to take a blood sample, mothers with previously or currently renal disorders, with the previous history of a liver disorder, cardiac disease, with a history of dyslipidemia, who are on treatment of lipidemic drugs, with a previous or current history of HIV, who are obesed, below 18 years old and mothers greater than 45 years old, who are not prepared to voluntarily donate blood samples and who have been smoking were excluded from the study.
Study variables
Dependent variables: Lipid profile, serum total protein, RFT and PIH.
Independent variables: Age, drinking alcohol, nutritional status, residence, educational status, occupation, income status, week of gestation, BMI, parity, gravidity, pregnancy status, gestational age, and trimester.
Sample size calculation
The sample size was calculated using a 95% confidence interval with 0.05 precision. The systematic study reported that the overall prevalence of pregnancy induced-hypertension in Ethiopia was 6.29% and (48) was used to calculate the minimum sample size.
The sample size was calculated based on the comparison of proportions for matched case-control study using
n = Z2P(1-P)/d2
n = 90.58 = 91
The minimum sample size was estimated to be 91. Even if the study is a prospective study, 10% was added by considering possible unforeseen attrition factors, and another 10% of this value was added to make it up to 100 pregnant women. Thus, for this study, 200 patients were recruited (100 each for both cases and the control group).
Sampling method
A prospective case-control study was done and the sampling method was convenient.
Measurement and data collection
Data collection procedure
Data was collected by using a pre-tested structured questionnaire which is developed following a thorough review of works of literature from different sources and will include information related to the socio-demographic condition, obstetrics and medical status, lifestyle, and nutritional habits of the participants. Data collection was carried out in the maternity ward (antenatal care clinic, labor ward, and delivery ward). Before the actual data collection, a pretest was carried out to evaluate the validity of the format and procedure of the study. In addition to the questionnaire, patient medical records were reviewed to abstract relevant variables related to laboratory, clinical, and obstetrics data.
The actual data was collected by face to face interviews, measurements, and reviewing medical records of the mother using a pretested structured questionnaire by trained data collectors. Data were collected only for those pregnant women who come to the hospital maternity ward only in the day time. Written informed consent was obtained. The participants were interviewed by the data collectors who were occasionally aided by trained assistants and comprising junior resident doctors; with the aid of a semi-structured, pre-tested questionnaire. The participants were allowed to sit and rest for about 5 min. The blood pressure reading was taken with the woman seated in the upright position and supine position using a mercury sphygmomanometer apparatus; and for referred women, BP was taken from referral form. Elevated blood pressure was repeated after at least 4 h.
General sample collection procedures
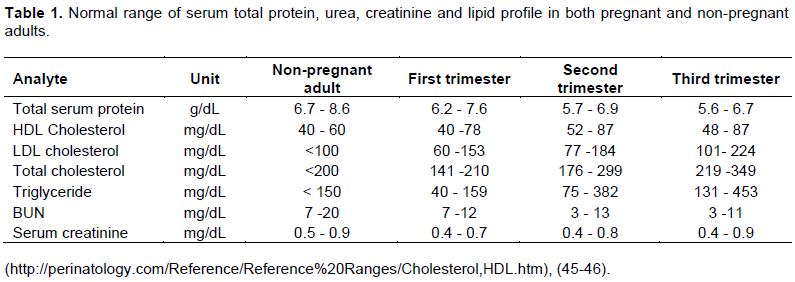
Following written informed consent, and response to the questionnaire, the participants were registered on the notebook and a serial number was given for each. Thereafter, 4-5 ml of the venous blood sample was collected from each participant in an SST test tube from the medial cubital of the forearm with swabbing by gauze or cotton moistened with 70% alcohol by the principal investigator or trained laboratory technologist professional. The whole blood sample was stored at room temperature for 10-20 min until it is coagulated. Thereafter, the blood sample was transported to the laboratory department and centrifuged at 3,000 revolutions per minute for 5 min and analyzed by the principal investigator in the Laboratory Department of the Clinical Chemistry section at AZMPH (Table 1).
Principle of the test for biochemical analysis
Serum TC, HDL, TG and LDL using standard enzymatic methods, for serum creatine, urea and serum total protein was measured by using modified Jaffe method, urease method and biuret method respectively.
Data analysis and interpretation
The result was interpreted using normal reference range specifically for pregnant women; defined by considering different factors like serum urea, creatinine, lipid profile and serum total protein in pregnant women.
Data was cleared, edited, checked for completeness manually and entered into Statistical Package for the Social Science (SPSS) for version 20.0 for Windows® (SPSS Inc., Chicago, IL, the USA) for analysis. After organizing and cleaning the data, frequencies, and percentages were calculated for all variables that are related to the objectives of the study. The extent of serum urea, creatinine, lipid profile, and serum total protein difference between case and control group was checked. The difference between the mean levels of serum lipids in the two groups was determined using Student’s t-test. Categorical variables were analyzed using the chi-square and continuous variables were analyzed with ANOVA where applicable. Pearson’s correlation was used to find a correlation between lipid profile with PIH, RFT with PIH, and serum total protein with PIH. The level of statistical significance was set at a 95% confidence interval. A P-value of less than 0.05 was considered statistically clinically significant. Finally, the result was presented using tables and other narrative forms.
Ethical considerations
The study was conducted after ethical approval was obtained from the Research and Ethics Institutional Review Board of Addis Ababa University College of Health Science, Department of Medical Laboratory Science. An official permission letter was submitted to the Amhara Health Bureau and AZMPH. Informed written consent was also obtained from each study participant before the actual data collection. Participants were informed of the risks and benefits of the study, their right to withdraw anytime, how confidentiality is maintained using codes, and their right to get their results for free. Individual’s clinically significant laboratory test analysis for tests was linked to the responsible doctor for further diagnosis and treatment accordingly.
RESULTS
A total of 200 pregnant women participated in the study. The study participants were classified into two as case and control groups. Control groups were pregnant women without pregnancy-induced hypertension; whereas case groups were pregnant women with pregnancy-induced hypertension. Each group contains 100 study participants. Out of 200 participants, pregnant women; 140 (70%) were from antenatal clinics and the rest 60 (30%) were from other maternity wards like delivery ward, postnatal care ward, and high-risk maternity wards. Demographic data related to the studied population was noted and presented in Table 2.
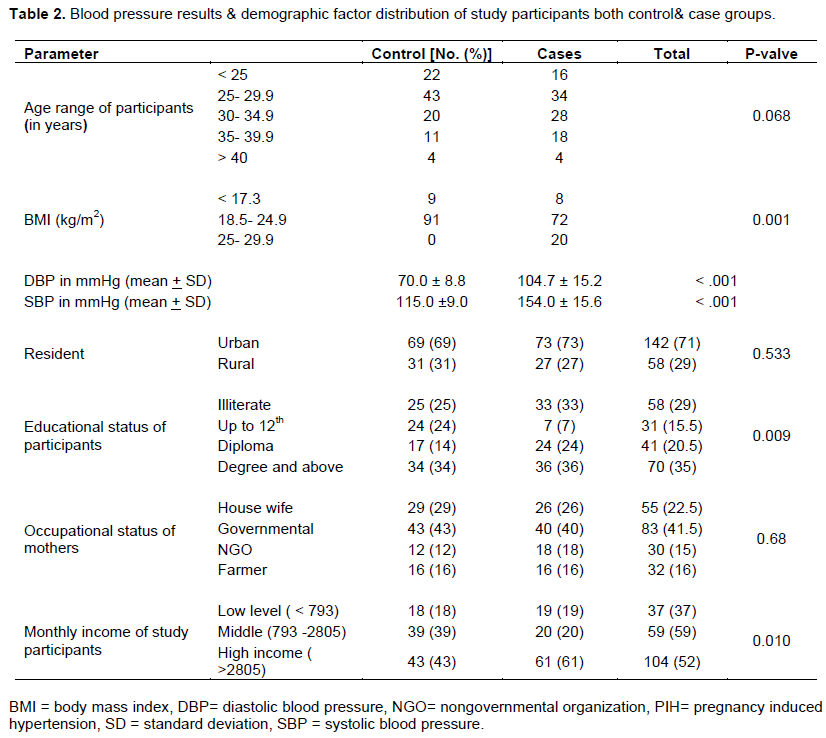
The age range of total pregnant women who participated in this study was from 18 – 41 years with a mean of 29.07 years. The mean age of pregnant women with PIH and pregnant women without PIH was 28.23 years and 29.9 years respectively. Most of the study participants of both the control and case group were found in the age range 25 - 29.9 with a percentage of 34 and 43% respectively. From a total of 200 pregnant women that participated in this study, 142 (71%) were from urban, 142 (71%) were literate, 151 (75.5%) husbands were literate, 104 (52%) of them were economically in the middle-income class, 83 (41.5%) were governmental employee (Table 2), most of the study participants were multiparious (55%), 193 (96.5%) were married, 110 (55%) of them were in the second trimester, and 125 (62.5%) had a gestational week of fewer than 37 weeks (Table 4).
Blood pressure is the main variable for this study to classify groups and parameters. In this study the distribution of diastolic and systolic blood pressure in control groups was less disperse that that of the case groups (70.0 ± 8.8 and 115.0 ± 9.03 and 104.7 ± 15.2 and 154.0 ± 15.6 respectively) (Table 2).
Most of the study participants in both groups were: from urban residence (69 and 73%), were a degree and above holders (34 and 26%), and were governmental employers (43 and 40%). Changes in demographic factors like income status and educational status in case groups were significant as compared to controls (P-valve < 0.05); and changes like occupation and residence were not significant as compared to controls (P-valve >0.05) (Table 2).
Mean BP (both SBP and DBP) was significantly increased in hypertensive pregnant women as compared to that in normotensive pregnant women (104.70/154.00 mmHg and 74.75/ 112.75 mmHg, respectively). The distribution blood pressure was more dispersed in the case group than the normal group with a standard deviation of 15.2/8.8 and 15.6/9.03 respectively (Table 2). Most of the study participants were within normal weight in both control (91%) and case groups (73%). But the percentage of overweight is higher in the case group than the normal group (19 and 2% respectively). In this study, BMI was significantly high in case groups relative to control groups (P-value < 0.001 and the result indicated that pregnant women with BMI > 25 kg/m2 had high chance of developing PIH than those with normal (P- valve < 0.001) (Table 2).
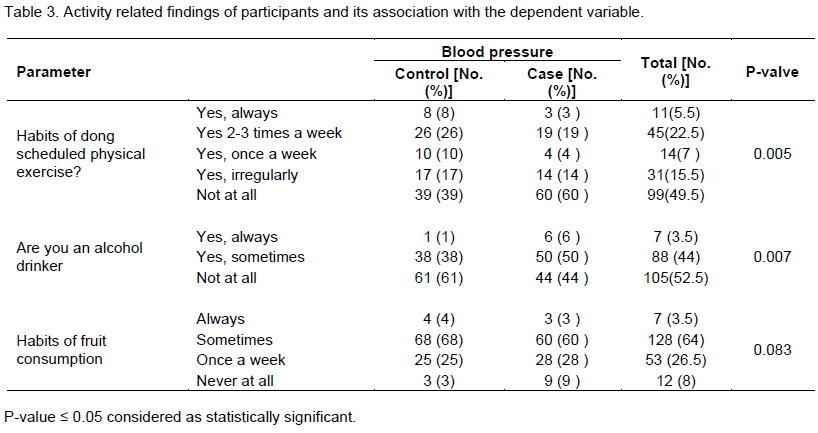
From a total of 200 study participants, 49.5% did not have a habit of scheduled exercise, 47.5% were alcohol drinkers, and 94% have a habit of fruit consumption.
According to the finding of this study, change in habit of taking alcohol and doing scheduled exercise was significantly associated with blood pressure (P-valve <0.05); whereas a change in habit of fruit consumption was not significantly associated with blood pressure (P-valve >0.083) (Table 3).
From a total of 200 pregnant women, 68% did not have a history of partner change, 96.5% were married once, 51.5% were multigravidia, and 55% were with party range of 1-4. The gestational weeks of the pregnant women range from 20 weeks to 42 weeks with a higher percentage in the third trimester (> 24 weeks) both in the control and case groups which accounts for 78 and 77% respectively (Table 4).
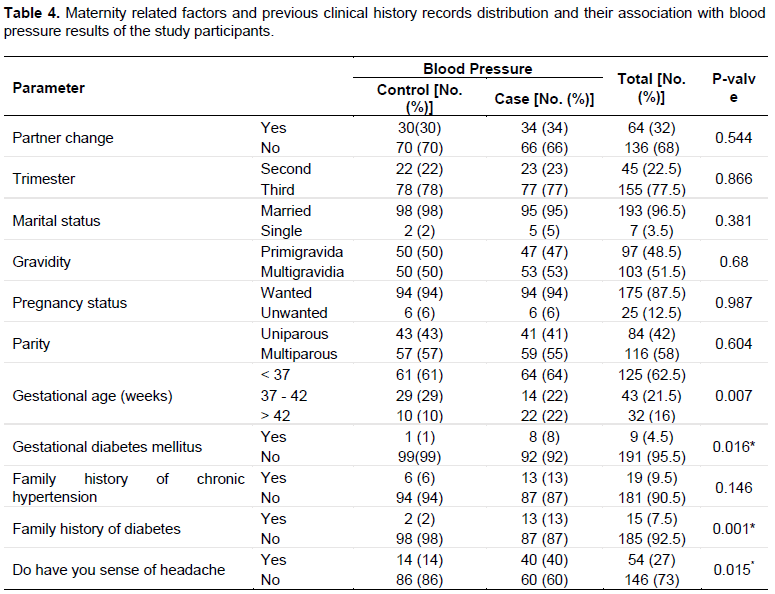
As shown in Table 4, change in gestational weeks and clinical histories like gestational DM, family history of diabetes and sense of headache were significantly associated with blood pressure results of the study participants (P <0.05) and other maternity factors like partner change, marital status, trimester, party and gravidity and like family history of diabetes, gestational diabetes mellitus, sense of headache, and history of chronic hypertension did not show significant association with blood pressure (P-valve >0.005).
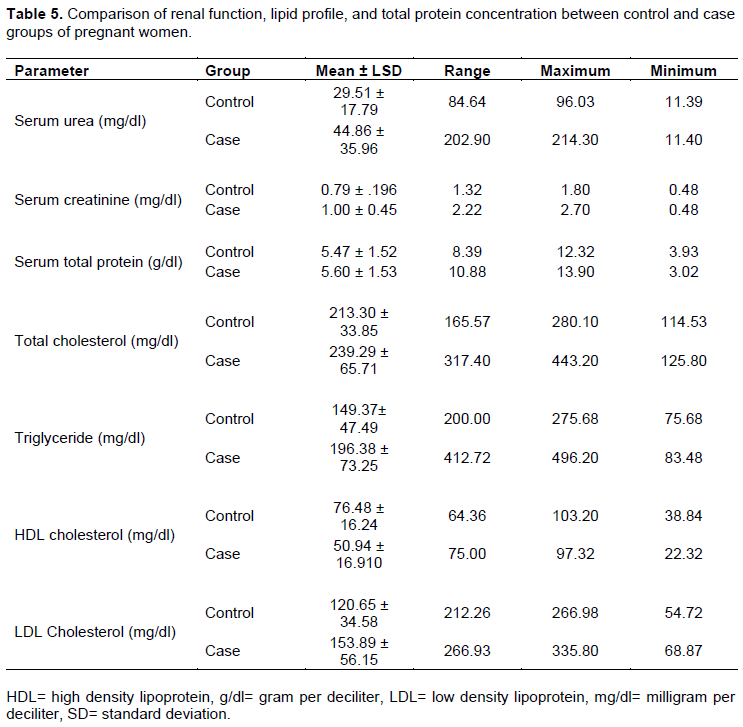
According to the present study finding; concentration of chemical analytes like BUN, TC, TG, and LDL were more dispersed and higher in case groups relative with control pregnant women (44.86 ± 35.96 in case and 29.51 ± 17.79 in control, 239.29 ± 65.71 in case and 213.30 ± 33.85 in control, 196.38 ± 73.25 in case and 149.37± 47.49 in control, 153.89 ± 56.15 in case and 120.65 ± 34.58 in control; respectively). But the level of serum creatinine and serum total protein was relatively less dispersed between the two groups, even if some higher results are seen in case groups relative with control groups (1.00 ± 0.45 in case and 0.79 ± .196 in control, 5.60 ± 1.53 in case and 5.47 ± 1.52 in control; respectively). Decreased concentration of HDL cholesterol was seen in case groups relative with the control groups (50.94 ± 16.910 in case and 76.48 ± 16.24 in control groups; respectively) (Table 5).
In the present study, the percentage of high level of TC, TG, LDL, serum creatinine and BUN level were seen in pregnant women with PIH. The level of serum total protein was nearly similar between the two groups whereas the level of HDL was very low in case group compared with control group. The serum levels of TC, TG, and LDL consistently increased, whereas the serum level of HDL consistently decreased from 2nd trimester towards 3rd trimester in hypertensive pregnant women (Table 6).
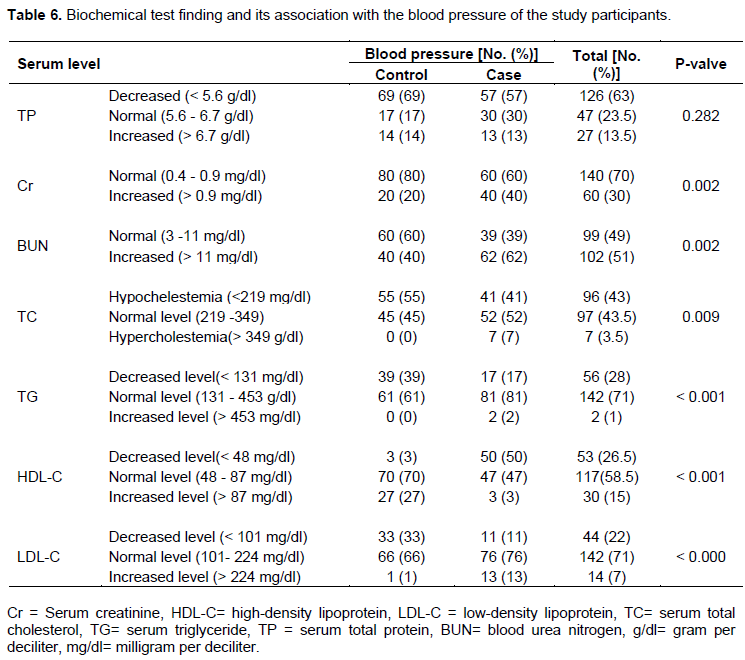
As shown in Table 6, the serum levels of TC, TGs, and LDL were significantly very high (P<0.05) and HDL was very low (P<0.05) in case group in all trimesters in case compared with control group. RFT in case group were significantly higher than the control group (P<0.05). But the change of serum total protein did not show a significant association with blood pressure (P-valve = 0.092) (Table 6).
Pregnant women in case groups with BMI > 24.9 kg/m2 had greater chance of developing abnormally increased level of TC (AOR: 6.003, 95% CI: 0.55 - 66.17, P= 004), TG (AOR: 4.315, 95% CI: 1.06 -10.05, P= 0.044), LDL (AOR: 4.565, 95% CI: 0.45 - 46.31, P = 0.012), and abnormally decreased HDL (AOR: 2.15 , 95% CI: 0.42 -11.14, P = 0.032). In the control group, the association between lipid profile tests and BMI was not significant (P-valve>0.05). Pregnant women who did not have habits of doing physical exercise have greater chance of having abnormally high level of TC (AOR: 3.135, 95% CI: 0.54 - 18.09, P-valve=0.007 in case and AOR: 2.50, 95% CI: .88 - 13.14, P-valve=0.021 in control groups), TG (AOR: 2.480, 95% CI: .55 - 11.25, P-valve=0.046 in case), serum LDL (AOR: 1.52, 95% CI: .50 - 12.67, P-valve=0.0101 in control groups) and abnormally decreased HDL (AOR: 2.907, 95% CI: 1.10 - 7.69, P-valve=0.032 in case and AOR: 2.764, 95% CI:.61 - 12.56, P-valve=0.018 in control groups) level compared with those who schedule physical exercises.
In case group, pregnant women who drinks alcohol had more chance of developing abnormally high TC level and abnormally decreased level of HDL (AOR: 2.047, 95% CI: 0.31- 13.42, P-valve=0.05 & AOR: 3.23, 95% CI: 1.25 - 8.36, P-valve=0.016, respectively). Also, in control group, increased TC, TG, LDL and decreased HDL were seen in alcohol drinking women, even if the association was not significant (P-valve >0.05). In case group, pregnant mothers who did not take fruit were more prone to having abnormally increased level of TC (AOR: 4.930, 95% CI: .40 - 1.46, P-valve=0.027) and decreased level of HDL (AOR: 2.012, 95% CI: 0.14 - 28.89, P-valve=0.048) than those who have good habits of fruit consumption (Table 7).
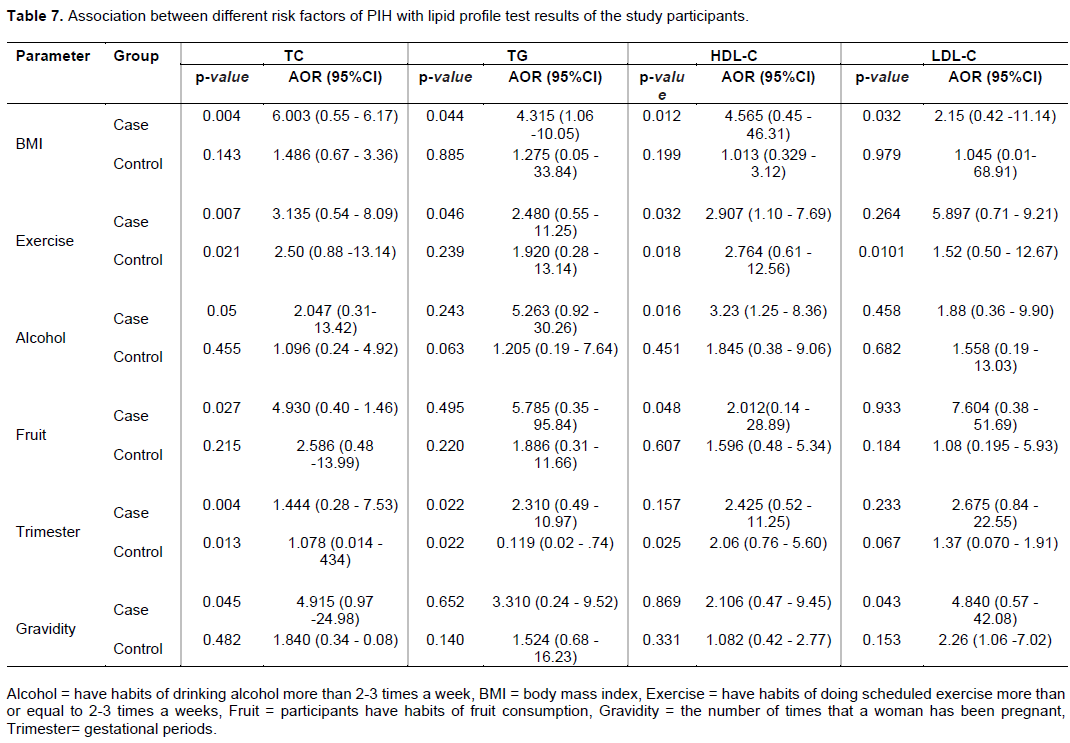
In multiple logistic regression analysis, pregnant mothers who were in the third trimester had higher chance of having increased serum TC (AOR: 1.444, 95% CI: 0.28 - 7.53, P-valve=0.004 in case group and AOR: 1.078, 95% CI: 0.014 - 8.4, P-valve=0.013 in control groups and increased level of serum TG (AOR: 2.310, 95% CI: 0.49 - 10.97, P-valve=0.022 in case group and AOR: 1.119, 95% CI: 0.02 - 1.74, P-valve=0.022 in control groups) in both groups. Also in this study, pregnant mothers in case group with multigravidia had a significant greater chance of having increased serum TC (AOR: 4.915, 95% CI: 0.97 -24.98, P-valve=0.045) and serum LDL (AOR: 4.840, 95% CI: 0.57 - 42.08, P-valve=0.043) compared with primigravida women; even when significant association was not seen in controls (Table 7).
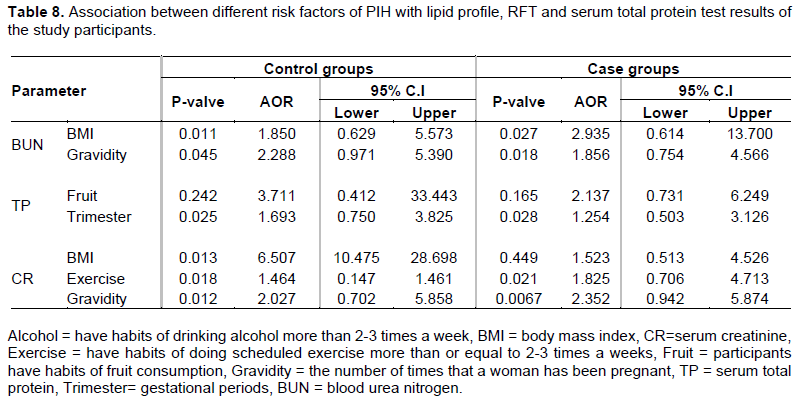
And the multiple logistic regression model indicate that factors like BMI and gravidity had significant association with blood urea nitrogen and serum creatinine test results of both groups. Pregnant women with BMI> 24.9 kg/m2 had greater chance of developing abnormally increased level of BUN level (AOR: 2.935, 95% CI: 0.614 - 13.700, P= 0.027 in case groups and AOR: 1.850, 95% CI: 0.629 - 5.573, P= 0.011 in control groups) and serum creatinine level (not significant in case groups and AOR: 6.507, 95% CI: 1.475 - 28.698, P= 0.013 in control groups). Pregnant multigravidia mothers also have high chance of increased level of serum creatinine (AOR: 2.352, 95% CI: 0.942 – 5.874, P= 0.007, in case groups and AOR: 2.027, 95% CI: 0.702 - 5.858, P= 0.012 in control groups) and blood urea level (AOR: 1.856, 95% CI: 0.754 - 4.566, P= 0.018 in case groups and AOR: 12.288, 95% CI: 0.971 - 5.390, P= 0.045 in control groups). Multiple logistic regression analysis also indicated that pregnant women in the third trimester were more prone to having abnormally low serum total protein compared with pregnant women in the second trimester in both groups (AOR: 1.254, 95% CI: 0.503 - 3.126, P= 0.028, in case groups and AOR: 1.693, 95% CI: 0.750 - 3.825, P= 0.025 in control groups) (Table 8).
In the present study, strong positive correlation was seen between serum creatinine with blood urea, serum total cholesterol with LDL cholesterol and serum triglyceride, serum triglyceride with LDL cholesterol and a strong negative correlation between HDL cholesterol with other lipid profile tests. Blood pressure had strong positive correlation with lipid profile tests like serum total cholesterol, serum triglyceride and LDL (r > 0.50); also, strong negative correlation with HDL cholesterol result of the study participants was observed (r = -0.78). Blood pressure was also strongly correlated with renal function tests.
DISCUSSION
Management of preeclampsia aims to minimize any pregnancy-related complications, avoiding unnecessary prematurity and to maximize maternal and prenatal/neonatal survival and health status. In this study, a simple screening was investigated to decrease the complications related to preeclampsia, by detection of serum lipid profile, and renal function test in early pregnancy decreases the risk that occurs due to PIH. In this study, significant increase in serum cholesterol, triglycerides, LDL, renal function tests and decreased HDL cholesterol were seen in pregnant women with PIH relative to normotensive pregnant women (p<0.05). The mean systolic blood pressure for both normal and case group pregnant women was 115.0 ± 9.03 and 154.0 ± 15.6 mmHg and mean diastolic pressure was 70.0 ± 8.8 and 104.7 ± 15.2 mmHg. BMI and blood pressure were significant variables among normal pregnancy and preeclampsia as per this study.
In the present study, pregnant mothers with multigravida, history of preeclampsia on prior pregnancy, multiple pregnancies, not receiving nutritional counseling during pregnancy, drinking alcohol during pregnancy, not consuming fruit, with BMI > 25 kg/m2, gestational weeks greater than 37 weeks, have a family history of diabetes mellitus and age > 35 years had greater significant chance of developing pregnancy-induced hypertension (P < 0.05). These risk factors in our study are in agreement with already published reports (Grum et al., 2017; Kahsay et al., 2018). Also, in the present study, pregnant mothers from urban residences have greater chance of developing PIH than pregnant mothers from rural residences; which is a opposite of the previously published study done in Tigray (Kahsay et al., 2018) and this variation may be due to lifestyle and nutritional variation between the two study participants.
In the present study, the mean serum total cholesterol level was 239.29 ± 65.71 mg/dl in case groups and 213.30 ± 33.85 mg/dl in control groups. Mean HDL in preeclampsia was 50.94 ± 16.910 mg/dl and 76.48 ± 16.24 mg/dl in normal groups. Mean LDL in pregnant women with PIH was 153.89 ± 56.15 mg/dl and normal pregnancy was 120.65 ± 34.58 mg/dl. Mean triglycerides in preeclampsia was 196.38 ± 73.25 mg/dl and normal pregnancy was 149.37± 47.49 mg/dl.
According to the finding of this study, serum TC, TG and LDL level was increased in preeclampsia when compared to normal pregnancy, and the change was also statistically significant (P<0.05). But the serum level of HDL was significantly low in case groups relative to the control groups (P<0.05). This finding was similar with the finding of different previous published studies (Roohi et al., 2015; Pusukuru et al., 2016; Rabia et al., 2013; Ali et al., 2017; Alemu et al., 2018) in which all reported that pregnant women as compared to non-pregnant had significantly increased total cholesterol, triglycerides and LDL-cholesterol (p<0.05) along with significantly lower level of HDL cholesterol (P <0.05). On the contrary, the finding of this study was not in line with the finding of a case-control study done in India which reported that the changes in lipid profile were not significant as compared to controls (Chopra et al., 2017).
In hypertensive pregnant women, the serum levels of TC, TG and LDL significantly increased and the serum level of HDL significantly decreased in the 3rd trimester of pregnancy relative to those in the 2nd trimester. The decreased levels of HDL in the 3rd trimester of hypertensive pregnant women in our study are in agreement with already published reports (Rabia et al, 2013; Ali et al., 2017; Alemu et al., 2018). From the results of our study, it can be found that serum levels of TC, TG, HDL, and LDL are more profound in the 3rd trimester of pregnancy in hypertensive pregnant women as compared to that of normotensive pregnant women (Table 7).
According to the present study finding, the mean blood urea level in preeclampsia was 44.86 ± 35.96 mg/dl and normal pregnancy was 29.51 ± 17.79 mg/dl and the mean serum creatinine level in pregnant women with PIH was 1.00 ± 0.45 mg/dl and normal pregnancy was 0.79 ± 0.196 mg/dl. Serum creatinine and blood urea level increased in preeclampsia when compared to normal pregnancy, and the change was also statistically significant (P<0.05). And this was similar with the finding of different previously published studies (Awoke et al., 2012; Ahmad et al., 2018 and Maputle et al., 2015); which all reported that a significant alternation of blood urea and serum creatinine was found with pregnant women who have PIH compared with pregnant women without PIH (P <0.05).
According to the finding of the present study, nearly all of the study participants (in both groups) had decreased level of serum total protein. The cause for this decreasing value may be due to lifestyle and nutritional based problems. The mean serum total protein level in pregnant women with PIH was 5.60 ± 1.53 g/dl and in women with normal pregnancy was 5.47 ± 1.52 g/dl. The level of serum total protein was somewhat high in case groups relative to control groups but the change was not significantly low in case groups relative to the control groups (P>0.05) which is similar with the finding of different previous studies (Ahmad et al., 2018; Maputle et al., 2015; Begum et al., 2010); which indicated that pregnant women with PIH have increased level compared with pregnant women without PIH and the change in serum total protein level was significant (p < 0.001); even if the change in this study was not significant (P>0.05). On the contrary, the finding of the current study was opposite with the findings of different previously published studies (Villar et al, 2006, Awoke et al., 2012; Chen et al., 2016; Ali et al., 2017), in which all reported that there was statistically significant decrease in the level of total protein (p<0.05). This difference may have occurred due to different variation of study participants like nutritional habit, ethnicity, follow up care during ANC, exercise and other factors which have greater effect on the protein level of study participants.
Pregnant women with BMI > 24.9 kg/m2 have greater chance of developing abnormally increased level of serum TC (AOR: 6.003, 95% CI: 0.55 - 66.17, P= 004), serum TG (AOR: 4.315, 95% CI: 1.06 -10.05, P= 0.044), LDL (AOR: 4.565, 95% CI: 0.45 - 46.31, P = 0.012), BUN level (AOR: 2.935, 95% CI: 0.614 - 13.700, P= .027 in case groups and AOR: 1.850, 95% CI: 0.629 - 5.573, P= 0.011 in control groups) and serum creatinine level (AOR: 6.507, 95% CI: 1.475 - 28.698, P= 0.013 in control groups) and abnormally decreased HDL (AOR: 2.15 , 95% CI: 0.42 -11.14, P = 0.032). But in control groups, the association between lipid profile tests and serum creatinine with BMI was not significant (P-valve>0.05) (Table 7).
Pregnant women who did not have habits of doing physical exercise have greater chance of having abnormally high level of serum TC (AOR: 3.135, 95% CI: 0.54 - 18.09, P-valve=0.007 in case and AOR: 2.50, 95% CI: .88 - 13.14, P-valve=0.021 in control groups), serum TG (AOR: 2.480, 95% CI: .55 - 11.25, P-valve=0.046 in case), serum LDL (AOR: 1.52, 95% CI: .50 - 12.67, P-valve=0.0101 in control groups) and abnormally decreased HDL (AOR: 2.907, 95% CI: 1.10 - 7.69, P-valve=0.032 in case and AOR: 2.764, 95% CI:.61 - 12.56, P-valve=0.018 in control groups) level compared with those who schedule physical exercises.
In case groups, pregnant women with habit of drinking alcohol had high chance of having abnormally high TC level (AOR: 2.047, 95% CI: 0.31- 13.42, P-valve=0.05) and abnormally decreased level of HDL (AOR: 3.23, 95% CI: 1.25 - 8.36, P-valve=0.016). In control groups, increased TC, TG, LDL and decreased HDL were seen in alcohol drinking women, even if the association was not significant (P-valve >0.05). Those not taking fruits had high chance of having abnormally increased level of serum total cholesterol (AOR: 4.930, 95% CI: .40 - 1.46, P-valve=0.027) and decreased level of serum HDL cholesterol (AOR: 2.012, 95% CI: .14 - 28.89, P-valve=0.048) than those who have good habits of fruit consumption (Table 7).
Pregnant mothers in the third trimester had higher chance of having increased level of TC (AOR: 1.444, 95% CI: 0.28 - 7.53, P-valve=0.004 in case groups and AOR: 1.078, 95% CI: 0.014 - 8.4, P-valve=0.013 in control groups), TG (AOR: 2.310, 95% CI: 0.49 - 10.97, P-valve=0.022 in case groups and AOR: 1.119, 95% CI: 0.02 - 1.74, P-valve=0.022 in control groups) and abnormally low serum total protein (AOR: 1.254, 95% CI: 0.503 - 3.126, P= 0.028, in case groups and AOR: 1.693, 95% CI: 0.750 - 3.825, P= 0.025 in control groups) compared to those in the 2nd trimester. Multigravidia was another factor that increased level of TC (AOR: 4.915, 95% CI: 0.97 -24.98, P-valve=0.045), LDL (AOR: 4.840, 95% CI: 0.57 - 42.08, P-valve=0.043), CR (AOR: 2.352, 95% CI: 0.942 - 5.874, P= 0.007), in case groups and (AOR: 2.027, 95% CI: 0.702 - 5.858, P= 0.012) in control groups, as well as BUN (AOR: 1.856, 95% CI: 0.754 - 4.566, P= 0.018 in case groups and (AOR: 12.288, 95% CI: 0.971 - 5.390, P= 0.045) in control groups; compared with primigravida women (Tables 7 and 8).
In general, the present study finding indicated that pregnant women with PIH had significantly increased level of TC, TG, LDL, RFT and significantly decreased level of HDL compared with pregnant women without PIH. The study finding also indicate that pregnant mothers with multigravida, history of preeclampsia, multiple pregnancies, not receiving nutritional counseling during pregnancy, drinking alcohol during pregnancy, not consuming fruit, with BMI > 25 kg/m2, gestational weeks greater than 37 weeks, have a family history of diabetes mellitus and age > 35 years had greater significant chance of developing pregnancy-induced hypertension (P < 0.05). Factors like BMI, schedule physical exercise, drinking alcohol, fruit consumption, trimester and gravidity showed significant association with abnormal lipid profile and RFT result of the study participants (Tables 7 and 8).
CONCLUSION AND RECOMMENDATION
Elevation of serum lipid profiles and renal function tests were seen among pregnant women with pregnancy- induced hypertension when compared with pregnant women without pregnancy-induced hypertension. Thus, the findings of the present study suggest that abnormal levels of lipid profile (TGs, TC, LDL, and HDL) and renal function test may contribute to the promotion of hypertension in pregnant women. This association may help to investigate the underlying pathological process of hypertension in pregnancy. Estimating serum lipid profile and renal function test is a simple screening test that helps to recognize dyslipidemia and renal failure in the early second trimester of patients who are at risk of preeclampsia.
Due to early detection of altered lipid profile and renal function test in preeclamptics, the incidence of complications can be decreased, which in turn reduces the materno-fetal morbidity and mortality. Therefore, serum lipid profiles and renal function tests must be continuously monitored throughout the whole pregnancy period as it would be helpful in the early detection and/or developing the strategies to prevent any obstetric- associated complication during PIH and/or at the time of delivery. We can improve the feto-maternal outcome by early detection of high-risk patients. This study results suggest that by modification of dietary pattern we can help in the prevention of pre-eclampsia; however, larger studies are required to ascertain a dietary association with pre-eclampsia.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abdella A (2010). Maternal mortality trend in Ethiopia. Ethiopian Journal of Health Development 24:1. |
|
|
Ahmad MA, Ellahi E, TAQI-UL-JAWAD SM (2018). Pregnancy Hypertensive Disorders Frequency and Obstetric Outcome. PAKISTAN Journal of Medical and Health Sciences 12(1):85-88. |
|
|
Al Ghazali B, Al-Taie AA-H, Hameed RJ (2014). Study of the clinical significance of serum albumin level in preeclampsia and in the detection of its severity. American Journal of BioMedicine 2:964-974. |
|
|
Alemu A, Abebe M, Biadgo B, Terefe B, Baynes HW (2018). Biochemical profiles of pregnant and non-pregnant women attending at the University of Gondar Hospital, Northwest Ethiopia: a comparative cross-sectional study. Ethiopian Journal of Health Sciences 28(3):331-340. |
|
|
Ali R, Farheen S, Zaheer A, Adnan B (2017). Assessment of Lipid Profile & Serum Total Protein in Patients with Hypertension. Annals of Pakistan Institute of Medical Sciences 23:8. |
|
|
Awoke A, Awoke T, Alemu S, Megabiaw B (2012). Prevalence and associated factors of hypertension among adults in Gondar, Northwest Ethiopia: a community based cross-sectional study. BMC Cardiovascular Disorders 12(1):113. |
|
|
Begum Ja, Sultana R, Naher S (2010). Serum levels of total protein, albumin and globulin in woman with hyperemesis gravidarum. Journal of Dhaka Medical College 19(1):58-60. |
|
|
Bibbins-Domingo K, Grossman DC, Curry SJ, Barry MJ, Davidson KW, Doubeni CA, Epling JW, Kemper AR, Krist AH, Kurth AE, Landefeld CS (2017). Screening for preeclampsia: US preventive services task force recommendation statement. Jama 317(16):1661-1667. |
|
|
Brown MA, Magee LA, Kenny LC, Karumanchi SA, McCarthy FP, Saito S, Hall DR, Warren CE, Adoyi G, Ishaku S (2018). Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension 72(1):24-43. |
|
|
Chen H, Tao F, Fang X, Wang X (2016). Association of hypoproteinemia in preeclampsia with maternal and perinatal outcomes: A retrospective analysis of high-risk women. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences P 21. |
|
|
Chopra S, Bedi P, Mahajan M (2017). Study of maternal serum lipids and lipoproteins in pregnancy induced hypertension. Indian Obstetrics and Gynaecology 7(3). |
|
|
English FA, Kenny LC, McCarthy FP (2015). Risk factors and effective management of preeclampsia. Integrated blood pressure control 8:7. |
|
|
Gao Q, Tang J, Li N, Liu B, Zhang M, Sun M, Xu Z (2018). What is precise pathophysiology in the development of hypertension in pregnancy? Precision medicine requires precise physiology and pathophysiology. Drug Discovery Today 23(2): 286-299. |
|
|
Gaym A, Bailey P, Pearson L, Admasu K, Gebrehiwot Y, Team ENEA (2011). Disease burden due to preâ€eclampsia/eclampsia and the Ethiopian health system's response. International Journal of Gynecology and Obstetrics 115(1):112-116. |
|
|
Ghodke B, Pusukuru R, Mehta V (2017). Association of lipid profile in pregnancy with preeclampsia, gestational diabetes mellitus, and preterm delivery. Cureus 9: 7. |
|
|
Grum T, Seifu A, Abay M, Angesom T, Tsegay L (2017). Determinants of pre-eclampsia/Eclampsia among women attending delivery Services in Selected Public Hospitals of Addis Ababa, Ethiopia: a case control study. BMC Pregnancy and Childbirth 17(1):307. |
|
|
Gupta S, Agarwal A, Sharma RK (2005). The role of placental oxidative stress and lipid peroxidation in preeclampsia. Obstetrical and Gynecological Survey 60(12): 807-816. |
|
|
Hong DSC, Oh IH, Park J-S, Lee CH, Kang CM, Kim G-H (2016). Evaluation of urinary indices for albuminuria and proteinuria in patients with chronic kidney disease. Kidney and Blood Pressure Research 41(3):258-266. |
|
|
Kahsay HB, Gashe FE, Ayele WM (2018). Risk factors for hypertensive disorders of pregnancy among mothers in Tigray region, Ethiopia: matched case-control study. BMC Pregnancy and Childbirth 18(1):482. |
|
|
Kar K, Sinha S (2016). Role of lipids, ionized calcium, and alkaline phosphatase in progress of pregnancy-induced hypertension-A prospective study in Kolkata. International Archives of Integrated Medicine 3(2):129-135. |
|
|
Maputle S, Khoza L, Lebese R (2015). Knowledge towards Pregnancy-induced Hypertension among Pregnant Women in Vhembe District, Limpopo Province. Journal of Human Ecology. 51(1-2): 47-54. |
|
|
Mol B. roberts CT, Thangaratinam S, Magee LA, de Groot CJM, Hofmeyr GJ (2016). Pre-eclampsia The Lancet 387: 999-1011. |
|
|
Nugteren JJ, Snijder CA, Hofman A, Jaddoe VW, Steegers EA, Burdorf A (2012). Work-related maternal risk factors and the risk of pregnancy-induced hypertension and preeclampsia during pregnancy. |
|
|
The Generation R Study. PloS ONE 7(6):e39263. Osungbade KO, Ige OK (2011). Public health perspectives of preeclampsia in developing countries: implication for health system strengthening. Journal of Pregnancy: Article ID 481095. |
|
|
Pauli JM, Repke JT (2017). Pitfalls with the New American College of Obstetricians and Gynecologists Task Force on Hypertension in Pregnancy. Clinical Obstetrics and Gynecology 60(1):141-152. |
|
|
Phillips JK, McBride CA, Hale SA, Solomon RJ, Badger GJ, Bernstein IM (2017). Examination of prepregnancy and pregnancy urinary protein levels in healthy nulliparous women. Reproductive Sciences 24(3):407-412. |
|
|
Pusukuru R, Shenoi AS, Kyada PK, Ghodke B, Mehta V, Bhuta K, Bhatia A (2016). Evaluation of lipid profile in the second and third trimester of pregnancy. Journal of Clinical and Diagnostic Research 10(3):QC12. |
|
|
Rabia A, Nureen Z, Kanwal R, Rabail A, Asia P, Muhammad T, Akash MS (2013). Comparative Analysis of Serum Lipid Profile between Normotensive and Hypertensive Pakistani Pregnant Women. Journal of Molecular and Genetic Medicine 7:2. |
|
|
Roohi S, Khan J, Rosaline M, Anees S, Kazi H, Kaleemullah M, Shariq B (2015). Evaluation of Lipid Profile, Calcium and Alkaline Phosphatase in Pregnancy Induced Hypertension Women. UK Journal of Pharmaceutical and Biosciences 3(2):24-28. |
|
|
Serrano NC, Guio-Mahecha E, Quintero-Lesmes DC, Becerra-Bayona S, Paez MC, Beltran M, Herrera VM, Leon LJ, Williams D, Casas JP (2018). Lipid profile, plasma apolipoproteins, and pre-eclampsia risk in the GenPE case-control study. Atherosclerosis 276: 189-194. |
|
|
Singh M, Pathak MS, Paul A (2015). A study on atherogenic indices of pregnancy-induced hypertension patients as compared to normal pregnant women. Journal of clinical and diagnostic research 9(7):BC05. |
|
|
Soma-Pillay P, Catherine NP, Tolppanen H, Mebazaa A, Tolppanen H, Mebazaa A (2016). Physiological changes in pregnancy. Cardiovascular Journal of Africa 27(2):89. |
|
|
Sroussi HY, Epstein JB, Bensadoun RJ, Sroussi Saunders DP, Lalla RV, Migliorati CA, Heaivilin N, Zumsteg ZS (2017). Common oral complications of head and neck cancer radiation therapy: mucositis, infections, saliva change, fibrosis, sensory dysfunctions, dental caries, periodontal disease, and osteoradionecrosis. Cancer Medicine 6(12):2918-2931. |
|
|
Teklu S, Gaym A (2006). Prevalence and clinical correlates of the hypertensive disorders of pregnancy at Tikur Anbessa Hospital, Addis Ababa, Ethiopia. Ethiopian Medical Journal 44(1):17-26. |
|
|
Thadhani RI, Maynard SE (2015). Proteinuria in pregnancy: Evaluation and management. Monografía internet) Glassock RJ: UpToDate. pp. 1-150. |
|
|
Topel ML, Duncan EM, Krishna I, Badell ML, Vaccarino V, Quyyumi AA (2018). Estimated Impact of the 2017 American College of Cardiology/American Heart Association Blood Pressure Guidelines on Reproductive-Aged Women. Hypertension 72(4):e39-e42. |
|
|
van Balen VAL, Spaan JJ, Ghossein-Doha C, van Kuijk SM, Spaanderman ME, Peeters LL (2018). Early pregnancy circulatory adaptation and recurrent hypertensive disease. Vascular and Renal Adjustments P 95. |
|
|
Villar J, Abdel-Aleem H, Merialdi M, Mathai M, Ali MM, Zavaleta N, Purwar M, Hofmeyr J, Campódonico L, Landoulsi S, Carroli G (2006). World Health Organization randomized trial of calcium supplementation among low calcium intake pregnant women. American Journal of Obstetrics and Gynecology 194(3):639-649. |
|
|
Wild R, Weedin EA, Wilson D (2015). Dyslipidemia in pregnancy. Cardiology Clinics 33(2): 209-215. |
|
|
Wolde Z, Segni H, Woldie M (2011). Hypertensive disorders of pregnancy in Jimma University specialized hospital. Ethiopian Journal of Health Sciences 21:3. |
|
|
World Health Organization (WHO) (2015). Trends in maternal mortality: 1990-2015: estimates from WHO, UNICEF, UNFPA, World Bank Group, and the United Nations Population Division. |
|
|
Yadav S, Agrawal M, Hariharan C, Dewani D, Vadera K, Krishna N (2018). A comparative study of the serum lipid profile of women with preeclampsia and normotensive pregnancy. Journal of Datta Meghe Institute of Medical Sciences University 13(2):83. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


