Full Length Research Paper
ABSTRACT
The arterial switch operation (ASO) is considered the gold standard for repair of D-transposition of the great arteries. However, when patients present after the third week of life, the early operative outcomes may be less predictable. Current guidelines recommend extra corporeal membrane oxygenation (ECMO) availability when the arterial switch is performed on patients between 3 to 6 weeks of age. Controversy remains regarding the safe upper age limit for a successful arterial switch operation. An objective assessment of the efficacy of a treatment requires a comparison of the treatment outcome with the natural history. We reviewed the literature and used the most externally valid data to create a composite survival curve that facilitates the comparison of surgical outcome and natural history. The data suggest that, where ECMO is available, the ASO is the best option for patients at any age up to 14 weeks old. The ASO is also the best option for patients up to 2 weeks of age where ECMO is not available. The atrial switch operation (AtSO) is the best option for patients between 2 weeks and 14 weeks of age where ECMO is not available. The ASO or the AtSO should be offered as soon as possible after birth; surgery after 14 weeks of age may not improve 10 year survival compared to the natural history.
Key words: Pediatric, transposition great arteries, operative, outcomes.
INTRODUCTION
The introduction of the atrial switch operation (AtSO) improved the long-term survival of patients with D-transposition of the great arteries (D-TGA) (Wells, 2000). Later, the arterial switch operation (ASO) was introduced; this provided better long-term survival than the AtSO and is considered the gold standard for repair of D-TGA (Kiener et al., 2018). However, when patients present after the third week of life, the early operative outcomes may be less predictable (Bigdelian and Sedighi, 2020). Current recommendations advise that the ASO be offered to patients who present up to 6 weeks of age; extra- corporal life support (ECLS) support should be available for patients over 3 weeks of age (Sarris et al., 2017). This is a class IIa recommendation and Level B evidence; the level of evidence for surgical options after 3 weeks of age is essentially Level C. Controversy remains regarding the safe upper age limit for a successful arterial switch operation. The goal of surgery is to improve the quality and quantity of life. Reliable and valid surgical outcome data, applied in the context of reliable and valid natural history data, optimises surgical decision making. We reviewed the literature to find the most reliable and valid natural history data for D-TGA and to find the most reliable and valid surgical outcome data for repair of D-TGA. A pilot study suggested that there would be insufficient data to conduct a credible meta-analysis or receiver operator curve analysis. For this reason we used the ‘Proximal Similarity Model’(PSM) to determine which natural history and surgical outcomes studies had the greatest external validity (Polit and Beck, 2010). As the observed survival from a natural history curve is an estimate of the probability of survival, it can be directly compared with the postoperative Kaplan-Meier survival curves (http://ocw.jhsph.edu/courses/fundepi/pdfs/ Lecture9.pdf). We used the most externally valid studies to generate a composite survival curve. This curve graphically demonstrates the surgical survival benefit as a function of age at the time of surgery.
PATIENTS AND METHODS
The proximal similarity model
According to this model, there are essentially 3 major threats to external validity; these relate to the study subjects, the study location and the study time. The proximal similarity model endeavours to establish which study most closely resembles the population of interest (that is, which study has the greatest external validity). Table 1 shows which parameters were used to choose the most externally valid natural history and surgical outcome studies.

A paper was chosen to construct the surgical outcome curve for one or more of the following reasons:
1. It was the largest study retrieved.
2. It examined surgical outcomes in neonates
3. It examined surgical outcomes in infants older than 60 days of age
4. It was from a surgical era that reflects current surgical practice and outcomes.
5. It followed up a sufficient number of patients to detect 10 year mortality rate of 9.3% with a 90% confidence level.
Search strategy and selection criteria
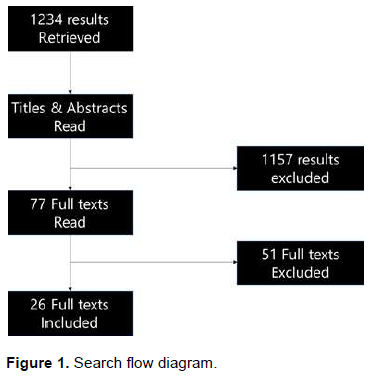
PUBMED and Google Scholar were searched systematically from January 1st 1966 until October 11th 2021. Table 2 shows the search terms and strategy. Google scholar searches used “all in title” option; PUBMED searches used “title/abstract” option. All search terms were combined with “AND”. Titles and abstracts were reviewed and full-text articles were obtained when the abstract indicated that there was a possibility that data pertaining to natural history or long-term surgical outcomes might be present. Papers on congenitally corrected transposition were excluded expect for assessment of left ventricular retraining (LVR). Non-English language studies and non-human studies were also excluded. A recent large study by Santens et al. (2020) showed that the late surgical mortality rate was 9.3%. In view of this, we only considered surgical outcome studies that examined a sufficient number of patients to detect this degree of late mortality with a 90% confidence Level. This essentially meant that studies with a sample size of less than 92 patients at 10 years follow-up were excluded. This sample size ‘cut-off’ was determined using a free online sample size calculator (https://www.calculator.net/sample-size-calculator.html). The search flow is shown in Figure 1.

Creation of the composite graph
The most externally valid natural history data were used to create a natural history curve. We then examined the long-term postoperative survival data of relevant retrieved full-texts. The most externally valid studies were used to generate the composite graph. The chosen surgical outcome curve was then superimposed on the natural history curve by sliding its origin along the natural history curve until the survival predicted by the curve at 10 years post repair could be said to be the same as that predicted by the natural history curve.
RESULTS
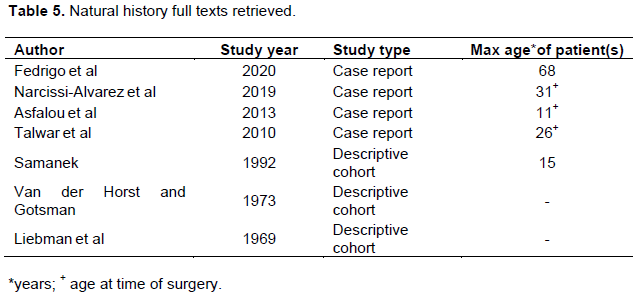
The search yielded 1,234 results; 77 relevant full-texts were obtained after examining titles and abstracts. Nine full-texts related to the natural history of D-TGA and 68 related to the surgical outcome of repair. The references of these full texts were examined for additional relevant references. The important details of the studies included for consideration when developing the postoperative survival branch of the composite survival curve are shown in Table 3. A list of excluded full texts that may have followed-up enough patients for 10 years, but survival data could not be determined from the texts, are shown in Table 4. A list of the retrieved natural history full texts is included in Table 5. The list of papers used to examine the results of techniques used to improve late ASO outcomes is shown in Table 6. The natural history curve for D-TGA is shown in Figure 2; the composite graph is shown in Figure 3.





There are two methods used to determine the natural history of a disease:
1. Follow-up a group of live patients to determine when patients die.
2. Perform an autopsy study on a group of patients thought to have died from the disease to determine the age pattern at the time of death.
Despite an extensive search, only 2 studies were found that could potentially be used to generate our natural history curve. The first study followed 946 patients with congenital heart disease (CHD) over 27 years (Samánek, 1992). This study was conducted in the Central Bohemia of the Czech Republic under circumstances that may not occur again. At that time, in Central Bohemia, all congenital heart disease was managed at one institution. Minimal surgery was performed locally and patients did not travel abroad for surgery. Patient follow-up was rigorous and post-mortems in children were mandatory. These factors combined to provide an ideal opportunity to study the natural history of CHD. We used the data from this study to develop our natural history curve for the first 15 years of life. There were 100 patients with TGA in this study (Samánek, 1992; Samánek et al., 1988). The 15 year natural history mortality was 62% (+/- 9.5%; 95% confidence interval). The second study was by Liebman study (Liebman et al., 1969); although it was larger, patients were free to leave the study area; 25% of the patients included in the study had surgery;16.4 % of the mortalities were surgically related and 6.8% of patients who died did not have an autopsy. We thought that these factors could significantly distort the natural history data, so we did not use this data.
The largest contemporary ASO outcome series was that of Fricke (Tyson et al., 2020); the median age at surgery was 10 days and it followed up a sufficient number of patients up to 10 years postoperatively. The study by Fraser (Fraser et al., 2020) was the most contemporary study that followed a sufficient number of patients up to 10 years postoperatively. We thought this study had the most externally valid ASO outcome data, for patients up to 14 days old at the time of surgery; we used it to generate the ASO arm of the composite survival curve. Although we examined 14 full-text articles on the surgical outcome of the AtSO, only 2 of these papers had patients with a median age at surgery of 30 days or less. These papers were published during the same era and gave an identical 10 year survival figure of 84% (Williams et al., 2003; Wells, 2000). Both papers showed that the longterm outcome after the Mustard AtSO was better than that following the Senning AtSO. The paper by Wells (2000) showed the survival figures for the Mustard and Senning techniques separately; we used their Mustard data to generate the AtSO survival arm of our composite graph. The natural history and surgical outcome studies did not distinguish between D-TGA with an intact ventricular septum (D-TGA IVS) and D-TGA with a VSD; however for most surgical outcome studies, D-TGA IVS (also referred to as simple D-TGA) accounted for about 60 to 70% of patients. Eight studies on left ventricular retraining (LVR), representing 153 patients, were retrieved. Three techniques of LVR were represented; Pulmonary Artery Band (PAB) was the most prevalent.
Although not depicted by the composite graph, all the curves (except the one for ASO after 60 days of age) essentially remain flat up to 15 years of age or 15 years after surgery. This means that the composite graph essentially shows almost identical short-term and long-term outcomes for the ASO and the AtSO performed before 2 weeks of age; the ASO curve is superimposed on the AtSO curve. For patients up to 14 days old at the time of surgery, we used the curves provided by Fraser (Fraser et al., 2020) and Wells (2000) to draw the ASO and AtSO curves respectively. The short-term and long-term outcomes of the ASO and the AtSO are slightly worse when they are performed on patients older than 60 days old; even with ECMO availability for the ASO. For patients over 60 days old at the time of surgery, we used the curves provided by Bisoi (2014) and Williams (2003) for ASO and AtSO respectively. ASO operative mortality was 1.3% for patients up to 2 weeks of age and 8.3% for patients older than 60 days (Fraser et al., 2020; Bisoi et al., 2014). The AtSO operative mortality was 4% for patients up to 2 weeks of age and 5.7% for patients older than 60 days (Roubertie et al., 2011; Wells, 2000). When the ASO was performed on patients older than 60 days old, 20% (+/- 7.5%; 95% CI) required ECMO (Bisoi et al., 2014). The ECMO requirement post ASO in patients up to 2 weeks of age was 3.9 %(+/-1.2%; 95% CI) (Tyson et al., 2020). By 2 weeks of age, about 20% of unoperated patients with D-TGA have died and by 8 weeks of age 50% have died. Three out of four of the chosen surgical survival curves follow-up a sufficient number of patients for 10 years to give a confidence level of 95% for the long-term mortality. The curve for ASO surgical outcomes on patients older than 60 days is the exception, it has a mean follow up of 28 months (range 18-84 months); as this was the most externally valid data on this subset of patients we used to generate the composite curve.
Comment
A meta-analysis of randomized clinical trials (RCT’s) or observational studies is the preferred method of reviewing scientific literature. Our search did not yield any RCT’s and the observational studies found had insufficient data for a meta-analysis or receiver-operator curve analysis. We chose the PSM technique to examine each study’s attempt at minimising bias and confounding. The most externally valid studies where then used to create the composite curve.
The composite curve clearly demonstrates 3 things:
1. A delay in offering surgery results in a higher mortality: if surgery is delayed to 14 days of age, over 20% of patients with D-TGA will have died.
2. The ASO after 60 days of age has short-term and long-term mortality that are essentially the same as an AtSO, provided that ECMO is available post ASO.
3. Surgery after 14 weeks of age may not improve 10 year survival compared to the natural history.
A major argument against the AtSO is that a morphologically right ventricle supporting the systemic circulation will eventually fail. Another concern is the high likelihood that patients will require a permanent pacemaker after the AtSO. Although some literature suggests that an ASO in older patients may be associated with poorer short-term outcomes (Bisoi et al., 2014), the argument that ‘the superior long-term outcome of an ASO mitigates the inferior short-term outcome of a late ASO’ is often cited as a reason for striving to perform an ASO in older patients (Kiener et al., 2018). One of the only 2 large studies on the AtSO performed in neonates found that 60% of patients are still in NYHA class 1 up to 12 years postoperatively; the vast majority of the rest were in NYHA class 2 (Wells, 2000). The other study found that the need for a pacemaker was 11% at 15 years (Williams et al., 2003). Another large AtSO study, where the median age at surgery was 6 months, reports 6 patients alive 40 years after their AtSO (Raissadati et al., 2017). In this study, the survival curve had essentially remained flat from 20 years post- surgery; 159 patients had been followed for 20 years and 6 patients for 40 years, the mortality over this period was 3%. The mortality One other large study, where the AtSO was performed in infants, supports these findings; the 20 year survival was about 87% (Görler et al., 2011). Although concerns about the RV in the systemic circulation are valid, results from these 4 large studies show that the right ventricle, in the systemic position, can reliably maintain a patient in NYHA class 1 or 2 for the long-term.
Attempts have been made to identify the upper age limit for a “low risk” successful ASO. Morphological parameters such as ventricular wall thickness, ventricular muscle mass and the ‘position’ of the interventricular septum have been proposed as predictors of a successful ‘low risk’ ASO (Lacour-Gayet et al., 2001). A period of left ventricular retraining (LVR), either by banding the main pulmonary artery or stenting a patent ductus arteriosus (PDA) have also been advocated as a means of increasing the likelihood that the left ventricle will support the systemic circulation after the ASO (Raissadati et al., 2017; Leong et al., 2019). Postoperative mechanical support of the left ventricle has also been proposed as method of increasing the chance that the left ventricle will tolerate an ASO (Malankar et al., 2020). We examined available evidence for the support of these techniques; our results are summarised in Table 6. We found 8 studies representing 153 patients; in none of these studies did LVR deliver better short-term outcomes compared to an ASO or AtSO in patients over 60 days of age. Taken as a homogenous group, assuming that all techniques are based on exposing the left ventricle to a pressure load, 115 out of 153 patients (75.2% +/- 6.84%; 95% CI) had a successful ASO. Although the number of patients represented is small, the available evidence suggests that LVR may be inferior to ASO with ECMO availability or the AtSO in patients older than 60 days of age.
Almost 4% (3.9%) of patients who have an ASO up to 2 weeks of age will require ECMO. It is assumed that if ECMO was not available, these patients would die. It is reasonable to infer that if the ASO switch was performed on patients up to the age of 2 weeks in a centre that did not have ECMO, the operative mortality would be a least 4%. This is very similar to the operative mortality of 4% of the AtSO on patients up to the age of 2 weeks old.
Similarly, 20% of patients who have an ASO operation after 60 days of age will require ECMO. If the ASO is performed, on this subset of patients, in a centre that does not have ECMO, the operative mortality would be a least 20%. This level of operative mortality is significantly higher than the 5.7% associated with the AtSO in patients older than 60 days of age. Although the composite curve does not examine surgical outcomes of patients between the ages of 2 weeks and 60 days; it would be reasonable to extrapolate that the ECMO requirement after an ASO would rise with increasing age up to the level seen after an ASO on patients older than 60 days old. The operative mortality for the AtSO operation may not be significantly different between the ‘up to 2 week’ old group and the ‘over 60 days of age’ group (4 and 5.7%, respectively). Available evidence suggests that the Mustard procedure offers superior short-term and long-term outcomes compared to the Senning procedure (Williams et al., 2003; Wells, 2000). Interestingly, our search strategy yielded one study that suggested that delaying the ASO past 3 days of age increased operative morbidity (Anderson et al., 2014) and yielded two studies that suggested that delaying the ASO past 6 days of age increased operative mortality (Kirklin et al., 1992; O'Byrne et al., 2018). The study by O'Byrne (O'Byrne et al., 2018) is particularly noteworthy as it examined 2159 neonates from 40 hospitals.
Our results suggest the following:
1. The best option for a patient presenting at any age up to 14 weeks old, where ECMO is available, would be the ASO.
2. The best option for a patient presenting up to 2 weeks of age, is the ASO, even if ECMO is not available.
3. The best option for patients after 60 days of age, where ECMO is not available, is the AtSO.
4. The best option for patients between 2 weeks old and 60 days old, where ECMO is not available, is probably the AtSO.
5. Surgery for D-TGA should be offered as soon as possible, preferably within the first 3 days of life.
6. The best option, in terms of survival, for patients presenting anywhere after 14 weeks of age, may not be surgical.
In conclusion, we have examined the literature to find the most externally valid data regarding surgical outcomes for repair D-TGA. Available evidence suggests that the ASO, where ECMO is available, is the best option for patients at any age up to 14 weeks old. The AtSO is the best option for patients between 2 weeks and 14 weeks of age where ECMO is not available. Surgery should be offered as soon as possible after birth; surgery after 14 weeks of age, may not improve 10 year survival.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Anderson BR, Ciarleglio AJ, Hayes DA, Quaegebeur JM, Vincent JA, Bacha EA (2014). Earlier arterial switch operation improves outcomes and reduces costs for neonates with transposition of the great arteries. Journal of the American College of Cardiology 63(5):481-487. |
|
|
Angeli E, Formigari R, Pace Napoleone C, Oppido G, Ragni L, Picchio FM, Gargiulo G (2010). Long-term coronary artery outcome after arterial switch operation for transposition of the great arteries. European Journal of Cardiothoracic Surgery 38(6):714-720. |
|
|
Asfalou I, Touati Z, Amri R, Cherti M (2013). Simple D-transposition of great arteries operated at the age of 11 years. Journal of Saudi Heart Association 25(2):99-101. |
|
|
Bigdelian H, Sedighi M (2020). Comparative Outcomes of Primary Arterial Switch Operation for Transposition of Great Arteries within the First Month of Life. The Journal of Tehran University Heart Center 15(1):1-5. |
|
|
Birnie D, Tometzki A, Curzio J, Houston A, Hood S, Swan L, Doig W, Wilson N, Jamieson M, Pollock J, Hillis WS (1998). Outcomes of transposition of the great arteries in the era of atrial inflow correction. Heart 80(2):170-173. |
|
|
Bisoi AK, Ahmed T, Malankar DP, Chauhan S, Das S, Sharma P, Saxena A, Boopathy NS (2014). Midterm outcome of primary arterial switch operation beyond six weeks of life in children with transposition of great arteries and intact ventricular septum. World Journal of Pediatric and Congenital Heart Surgery 5(2):219-225. |
|
|
Co-Vu JG, Ginde S, Bartz PJ, Frommelt PC, Tweddell JS, Earing MG (2013). Long-term outcomes of the neoaorta after arterial switch operation for transposition of the great arteries. Annals of Thoracic Surgery 95(5):1654-1659. |
|
|
Daebritz SH, Nollert G, Sachweh JS, Engelhardt W, von Bernuth G, Messmer BJ (2000). Anatomical risk factors for mortality and cardiac morbidity after arterial switch operation. The Annals of thoracic surgery 69(6):1880-1886. |
|
|
Dibardino DJ, Allison AE, Vaughn WK, McKenzie ED, Fraser CD Jr (2004). Current expectations for newborns undergoing the arterial switch operation. Annals of Surgery 239(5):588-596. |
|
|
Fedrigo M, Frescura C, Angelini A, Thiene G (2020). Complete Transposition of Great Arteries With Dominant Left Ventricle: Long-Term Survival in Natural History. Case Reports 2(13):2107-2110. |
|
|
Fraser CD Jr, Chacon-Portillo MA, Well A, Zea-Vera R, Binsalamah Z, Adachi I, Mery CM, Heinle JS (2020). Twenty-Three-Year Experience With the Arterial Switch Operation: Expectations and Long-Term Outcomes. In Seminars in Thoracic and Cardiovascular Surgery 32(2):292-299. |
|
|
Genoni M, Vogt P, von Segesser L, Seifert B, Arbenz U, Jenni R, Turina M (1999). Extended follow-up after atrial repair for transposition of the great arteries: a younger age at surgery improves late survival. Journal of Cardiovascular Surgery 14(4):246-551. |
|
|
Görler H, Ono M, Thies A, Lunkewitz E, Westhoff-Bleck M, Haverich A, Breymann T, Boethig D (2011). Long-term morbidity and quality of life after surgical repair of transposition of the great arteries: atrial versus arterial switch operation. Interact Cardiovascular and Thoracic Surgery 12(4):569-574. |
|
|
Hörer J, Schreiber C, Cleuziou J, Vogt M, Prodan Z, Busch R, Holper K, Lange R (2009). Improvement in long-term survival after hospital discharge but not in freedom from reoperation after the change from atrial to arterial switch for transposition of the great arteries. Journal of Thoracic and Cardiovascular Surgery 137(2):347-54. |
|
|
Hutter PA, Kreb DL, Mantel SF, Hitchcock JF, Meijboom EJ, Bennink GB (2002). Twenty-five years' experience with the arterial switch operation. Journal Thoracic Cardiovascular Surgery 124(4):790-797. |
|
|
Khairy P, Clair M, Fernandes SM, Blume ED, Powell AJ, Newburger JW, Landzberg MJ, Mayer JE Jr (2013). Cardiovascular outcomes after the arterial switch operation for D-transposition of the great arteries. Circulation 127(3):331-339. |
|
|
Kiener A, Kelleman M, McCracken C, Kochilas L, St Louis JD, Oster ME (2018). Long-Term Survival after Arterial Versus Atrial Switch in d-Transposition of the Great Arteries. The Annals of thoracic surgery 106(6):1827-1833. |
|
|
Kirklin JW, Blackstone EH, Tchervenkov CI, Castaneda AR (1992). Clinical outcomes after the arterial switch operation for transposition. |
|
|
Patient, support, procedural, and institutional risk factors. Congenital Heart Surgeons Society. Circulation 86(5):1501-1515. |
|
|
Kothari SS, Ramakrishnan S, Senguttuvan NB, Gupta SK, Bisoi AK (2011). Ductal recanalization and stenting for late presenters with TGA intact ventricular septum. Annals of Pediatric Cardiology 4(2):135-138. |
|
|
Koubský K, Gebauer R, Tláskal T, Mat?jka T, Poruban R, Ji?ínská D, Hu?ín B, Janoušek J, Chaloupecký V (2021). Long-Term Survival and Freedom from Coronary Artery Reintervention After Arterial Switch Operation for Transposition of the Great Arteries: A Population-Based Nationwide Study. Journal of the American Heart Association 10(13):e020479. |
|
|
Lacour-Gayet F, Piot D, Zoghbi J, Serraf A, Gruber P, Macé L, Touchot A, Planché C (2001). Surgical management and indication of left ventricular retraining in arterial switch for transposition of the great arteries with intact ventricular septum. European Journal of Cardiothoracic Surgery 20(4):824-829. |
|
|
Leong MC, Ahmed Alhassan AA, Sivalingam S, Alwi M (2019). Ductal Stenting to Retrain the Involuted Left Ventricle in d-Transposition of the Great Arteries. Annals of Thoracic Surgery 108(3):813-819. |
|
|
Liebman J, Cullum L, Belloc NB (1969). Natural history of transpositon of the great arteries. Anatomy and birth and death characteristics. Circulation 40(2):237-262. |
|
|
Ma K, Hua Z, Yang K, Hu S, Lacour-Gayet F, Yan J, Zhang H, Pan X, Chen Q, Li S (2014). Arterial switch for transposed great vessels with intact ventricular septum beyond one month of age. Annals of Thoracic Surgery 97(1):189-195. |
|
|
Mainwaring RD, Patrick WL, Ibrahimiye AN, Watanabe N, Lui GK, Hanley FL (2018). An Analysis of Left Ventricular Retraining in Patients With Dextro- and Levo-Transposition of the Great Arteries. The Annals of Thoracic Surgery 105(3):823-829. |
|
|
Malankar DP, Patil S, Mali S, Dhake S, Mhatre A, Bind D, Soni B, Kandavel D, Garekar S (2020). Primary Arterial Switch Operation for TGA/IVS and Regressed Left Ventricle: How and When to Use Left Ventricular Assist Device. World Journal for Pediatric and Congenital Heart Surgery 11(1):97-100. |
|
|
Moons P, Gewillig M, Sluysmans T, Verhaaren H, Viart P, Massin M, Suys B, Budts W, Pasquet A, De Wolf D, Vliers A (2004). Long term outcome up to 30 years after the Mustard or Senning operation: a nationwide multicentre study in Belgium. Heart 90(3):307-313. |
|
|
Narcisse-Alvarez JF, Pumacayo-Cardenas SC, Espinola-Zavaleta N (2019). Natural history of complex transposition of great arteries in an adult: A case report. Cardiology in the Young 29(5):720-724. |
|
|
O'Byrne ML, Glatz AC, Song L, Griffis HM, Millenson ME, Gillespie MJ, Dori Y, DeWitt AG, Mascio CE, Rome JJ (2018). Association Between Variation in Preoperative Care Before Arterial Switch Operation and Outcomes in Patients With Transposition of the Great Arteries. Circulation 138(19):2119-2129. |
|
|
Oda S, Nakano T, Sugiura J, Fusazaki N, Ishikawa S, Kado H (2012). Twenty-eight years' experience of arterial switch operation for transposition of the great arteries in a single institution. European Journal of Cardiothoracic Surgery 42(4):674-9. |
|
|
Polit DF, Beck CT (2010). Generalization in quantitative and qualitative research: Myths and strategies. International Journal of Nursing Studies 47(11):1451-1458. |
|
|
Raissadati A, Nieminen H, Sairanen H, Jokinen E (2017). Outcomes after the Mustard, Senning and arterial switch operation for treatment of transposition of the great arteries in Finland: a nationwide 4-decade perspective. European Journal of Cardiothoracic Surgery 52(3):573-580. |
|
|
Roubertie F, Thambo JB, Bretonneau A, Iriart X, Laborde N, Baudet E, Roques X (2011). Late outcome of 132 Senning procedures after 20 years of follow-up. Annals of Thoracic Surgery 92(6):2206-2213. |
|
|
Samánek M (1992). Children with congenital heart disease: probability of natural survival. Pediatric Cardiology 13(3):152-158. |
|
|
Samánek M, Benesová D, Goetzová J, Hrycejová I (1988). Distribution of age at death in children with congenital heart disease who died before the age of 15. British Heart Journal 59(5):581-585. |
|
|
Santens B, Van De Bruaene A, De Meester P, Gewillig M, Troost E, Claus P, Bogaert J, Budts W (2020). Outcome of arterial switch operation for transposition of the great arteries. A 35-year follow-up study. International Journal of Cardiology 316:94-100. |
|
|
Sample size calculator. |
|
|
Sarris GE, Balmer C, Bonou P, Comas JV, da Cruz E, Chiara LD, Di Donato RM, Fragata J, Jokinen TE, Kirvassilis G, Lytrivi I, Milojevic M, Sharland G , Siepe M, Stein J, Büchel EV, Vouhé PR (2017). Clinical guidelines for the management of patients with transposition of the great arteries with intact ventricular septum. European Journal of Cardio-Thoracic Surgery 51(1):e1-e32. |
|
|
Sologashvili T, Wannaz L, Beghetti M, Aggoun Y, Prêtre R, Myers PO (2018). Two-stage arterial switch for late-presenting transposition of the great arteries. Interactive Cardiovascular and Thoracic Surgery 27(4):581-585. |
|
|
Swartz MF, Sena A, Atallah-Yunes N, Meagher C, Cholette JM, Gensini F, Alfieris GM (2012). Decreased incidence of supravalvar pulmonary stenosis after arterial switch operation. Circulation 126(11 Suppl 1):S118-122. |
|
|
Talwar S, Malankar D, Choudhary SK, Saxena A, Airan B (2010). An alternative technique for the atrial switch operation for transposition of the great arteries in an unoperated adult patient. Journal of Cardiovascular Surgery 25(4):406-409. |
|
|
Tyson AF, Douglas B, Michael D, d'Udekem Y, Christian PB, Nelson A, Igor EK (2020).The influence of coronary artery anatomy on mortality after the arterial switch operation, The Journal of Thoracic and Cardiovascular Surgery 160(1):191-199. |
|
|
van der Horst RL, Gotsman MS (1973). The spectrum and natural history of complete transposition of the great arteries. South African Medical Journal 47(13):553-558. |
|
|
van der Palen RLF, Blom NA, Kuipers IM, Rammeloo LAJ, Jongbloed MRM, Konings TC, Bouma BJ, Koolbergen DR, Hazekamp MG (2021). Long-term outcome after the arterial switch operation: 43 years of experience. European Journal of Cardiothoracic Surgery 59(5):968-977. |
|
|
Vejlstrup N, Sørensen K, Mattsson E, Thilén U, Kvidal P, Johansson B, Iversen K, Søndergaard L, Dellborg M, Eriksson P (2015). Long-Term Outcome of Mustard/Senning Correction for Transposition of the Great Arteries in Sweden and Denmark. Circulation 132(8):633-638. |
|
|
Watanabe N, Mainwaring RD, Carrillo SA, Lui GK, Reddy VM, Hanley FL (2015). Left Ventricular Retraining and Late Arterial Switch for D-Transposition of the Great Arteries. The Annals of Thoracic Surgery 99(5):1655-1661. |
|
|
Wells WJ, Blackstone E (2000). Intermediate outcome after Mustard and Senning procedures: A study by the Congenital Heart Surgeons Society. In Seminars in Thoracic and Cardiovascular Surgery: Pediatric Cardiac Surgery Annual 3(1):186-197. |
|
|
Williams WG, McCrindle BW, Ashburn DA, Jonas RA, Mavroudis C, Blackstone EH, Congenital Heart Surgeon's Society (2003). Outcomes of 829 neonates with complete transposition of the great arteries 12-17 years after repair. European Journal of Cardiothoracic Surgery 24(1):1-9. |
|
|
Wilson NJ, Clarkson PM, Barratt-Boyes BG, Calder AL, Whitlock RM, Easthope RN, Neutze JM (1998). Long-term outcome after the Mustard repair for simple transposition of the great arteries: 28-year follow-up. Journal of the American College of Cardiology 32(3):758-765. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


