Full Length Research Paper

ABSTRACT
The aim of this study was to describe the pathologic changes in temporal bones with cochlear otosclerosis that may have implications for cochlear implantation. Fifteen human temporal bones with otosclerosis were used for this study. In each temporal bone was studied: (1) medial wall of the middle ear and in particular the horizontal segment of the facial nerve canal; (2) the round window niche and the corresponding part of the scala tympani; (3) the area of the labyrinthine segment and first genu of the facial nerve. Six temporal bones revealed otosclerotic pathology spanning the otic capsule between the cochlear endosteum and the facial nerve canal. The labyrinthine facial nerve was enveloped by otosclerosis in two cases, while the horizontal segment was involved in four temporal bones. Complete obstruction of the round window niche was observed in three cases, while round window niche obstruction was observed in four temporal bones. Otosclerosis presents difficulties for implant candidates. These otosclerotic changes with obstruction are usually present at the round window or at the scala tympani. The histology described underpins the need to counsel patients regarding the possibility of facial nerve stimulation and difficult implantation.
Key words: Cochlear otosclerosis, histopathology, round window, obstruction.
INTRODUCTION
Otosclerosis is a localized hereditary disorder characterised by disordered resorption and deposition of bone with foci which is sharply demarcated from surrounding normal bone and shows a marked affinity for certain parts of the otic capsule (Stankovic and McKenna, 2006).
Otosclerosis usually involves the stapes footplate or stapediovestibular joint presenting with conductive hearing loss. “Cochlear Otosclerosis” on the hand is a term used to describe occurrence of pure sensorineural hearing loss due to otosclerosis in an ear without a conductive loss to the hearing impairment. In other words, there is otosclerotic foci in the cochlear endosteum but it does not result in/or cause stapes fixation (de Souza and Goycoolea, 2014; Sebahattin et al., 2010).
The incidence of Otosclerosis as reported in the Minnesota Temporal collection is 12.5% in Caucasian and 1.5% in temporal bones of Japanese origin (Hueb et al., 1991; Ohtani et al., 2003). While the overall prevalence of histologic Otosclerosis is 10%, only 10% of these are clinically apparent making the overall prevalence of clinical otosclerosis approximately 1% in the population. A Belgian study (Declau et al., 2001)reported Otosclerotic foci in 2.5% of temporal bones and 3.4% of autopsy cases. Similarly, about 20% of Caucasians are said to have histologic otosclerosis while only 1% African Americans are seen with this disorder. Unfortunately, no data is available for sub-Saharan Africa.
Otosclerosis is a process of bone remodelling unique only to the Otic capsule (Michaels and Soucek, 2011; Sebahattin et al., 2010)and Ossicles (malleus and incus) (Escada et al., 2007). This bone remodelling is not readily obvious, but it is said to occur when molecular factors trigger the process in individuals who are genetically predisposed or due to environmental factors. It is inherited in an autosomal dominant manner with incomplete penetrance. Several gene loci have been implicated such as OTSC1-5, OTSC7, COL1A1, TGFβ, BMP2, BMP4, ACE, AGT and RELN gene (Chen et al., 2002; Richard et al., 2015; Sebahattin et al., 2010; Thys et al., 2007; Velegrakis, 2011)Osteoprotegerin (OPG) is a protein secreted by the spiral ligament and is a potent inhibitor of bone re-modelling; it is secreted in perilymph and acts by inhibiting recruitment, formation, and activity of osteoclasts.
According to Sebahattin et al. (2010), Cochlear otosclerosis can be classified as a “mixed type” or a “sensorineural type” based on the clinical appearance. Cochlear otosclerosis located in the otic capsule, involving the cochlear endosteum causing sensorineural hearing loss without any stapes fixation or any conductive component has two histologic phases, an early spongiotic (Otospongiosis) phase and a late sclerotic phase (Sebahattin et al., 2010). The early phase is rich in multiple cell types such as osteocytes, osteoblasts and histiocytes. This spongy appearance is due to vascular dilation secondary to osteocyte resorption of bone surrounding blood vessels. This can lead to the appearance of a red hue behind the drumhead popularly termed “Schwartz sign” (describe by Schwartz in 1873). Active otosclerosis foci appear as finger-like projections of disorganized bone, and its foremost part is particularly rich in osteocytes while the centre is composed of multinucleated osteocytes. The sclerotic phase shows dense sclerotic bone formation in the areas of previous resorption. Both the sclerotic and spongiotic as well as intermediate phases may be present at the same time. Otosclerotic foci always begin at the endochondral bone but may progress to involve endosteal and periosteal layers and even enter into the membranous labyrinth.
Cochlear Otosclerotic lesions are commonly found around or anterior to the oval window, round window niche, cochlear wall, and wall of anterior internal auditory canal and in some instances there is new bone formation in the scala tympani of the basal cochlear segment (Gildener-Leapman and Linthicum-Fred, 2011). Cavitations can also occur in severe cases of otosclerosis. The otosclerotic focus shows extensive bone resorption and replacement by vascular fibrous tissue which can subsequently form large cavities as the soft tissue undergoes dissolution. In patients with bilateral severe to profound hearing impairment due to otosclerosis, the use of cochlear implantation is a viable option. A review of the available literature shows that patients derive significant benefit from cochlear implant (Yaralı et al., 2015), but there is also evidence of misplaced electrode arrays, difficulty in inserting or partially inserted arrays, increased cochlear ossification, implant failures, and tinnitus (Balkany et al., 1996; Berrettini et al., 2002; Frijns et al., 2009; Munoz-Fernandez et al., 2012).
Cochlear otosclerotic patients have been found to derive immense benefit from cochlear implants, and in fact is now the preferred mode of managing clinical variants such as Far-advanced otosclerosis, a condition in which Otosclerotic involvement of the otic capsule has progressed to result in undetectable air- and bone-conduction hearing thresholds (Ruckenstein et al., 2001). However, a minimum speech discrimination score of 30% or lower in severe to profound sensorineural hearing losses suffices for cochlear implantation in Otosclerotic patients. This procedure presents challenges to the surgeon as a result of the pathogenic relics of Otospongiosis. These are difficulty with passing electrode arrays, partial insertion or misplaced arrays (Rotteveel et al., 2004)due to either osteoneogenesis or obliteration in the cochlear, round window niche, narrowing in the basal turn of cochlear or in the oval window.
An area of bone resorption (cavitation) may sometimes extend anteriorly from the internal auditory canal containing cerebrospinal fluid in continuity with the subarachnoid space (Michaels and Soucek, 2011). Electrode misplacement and cerebrospinal fluid gushing during cochlear implantation have been linked to third window lesions due to cavitating cochlear otosclerosis around the middle and apical turns of the cochlea (Makarem and Linthicum, 2008).
This study aims to describe histopathologic changes in human temporal bones (TB) with cochlear otosclerosis that may have implications for cochlear implantation.
MATERIALS AND METHODS
Fifteen human temporal bone sections from 12 patients with histopathologic diagnosis of otosclerosis from the archival library of the UCL Ear Institute were used for this study. Six (6) males and three (3) females and six (6) of unknown gender with age ranges from 41 to 85 years were studied. The specimens have been decalcified, embedded, and cut in horizontal sections from the upper surface of the temporal bone down to the lower section. The embedding material was low-viscosity nitro-cellulose [LVN - a substance related to celloidin] and in some sections paraffin wax. Slides embedded with LVN were cut at a thickness of 20 μm while for paraffin wax sections 7 μm thickness. Thereafter, each tenth of a section was mounted on a glass slide and stained with Haematoxylin and Eosin [H & E].
The 15 temporal bone sections were selected based on confirmation of otosclerosis from the archival library of the University College London, Ear Institute Temporal Bone Collection. The inclusion criteria included: clarity of the otic capsule and medial half of the middle ear cavity in the horizontal section and presence of otosclerosis. This will help visualize the course of the facial nerve and the surgical access into the otic capsule. A total of eleven (11) temporal bone slides were either poor slides or had localised otosclerotic involvement of only the oval window area and as such were excluded. Controls: Eight (8) non-otosclerotic temporal bone slides at approximately the same section levels were used as control.
A Lietz Dialux 22 EBB microscope with lens magnification of 2.5, 10, 20, 40 and 100× was used for observation. A camera (Sony CCD-IRIS) was mounted on the microscope and the micrograph image captured, converted and transferred through an Analogue-Digital Converter (DATAVIDEO DAC-2) projected on a laptop screen with pinnacle movie box studio 9. Photomicrographs of representative temporal bone slides were taken with the AxioVision Software.
In each of the temporal bone sections the following structures were studied thoroughly: Medial wall of the middle ear especially the tympanic segment of the facial nerve, the round window niche and round window membrane; the membranous labyrinth especially the cochlea turns and labyrinthine/first genu of the facial nerve. The level of the sections utilized was approximately from the level of the first genu of the facial nerve to the level of the round window niche. This will particularly help to view the round window niche or membrane for obstructing or bridging lesions.
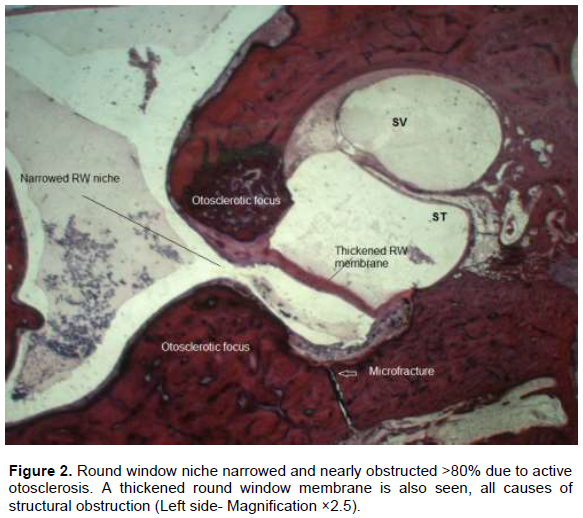
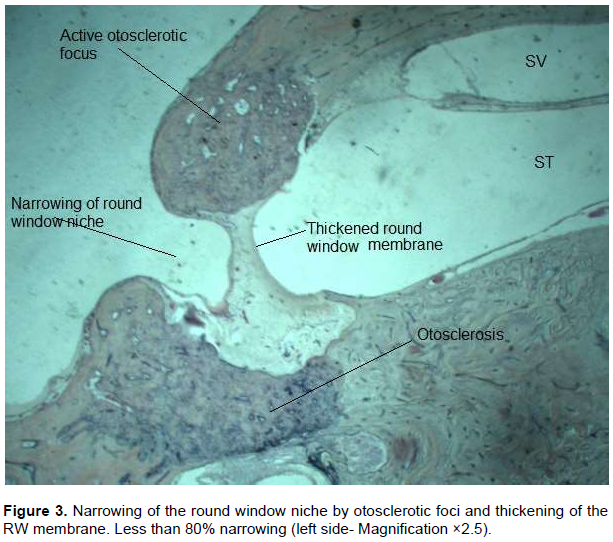
For ease of description, we arbitrarily divided the RW area into those with greater than 80% and those with less than 80% obstruction. This we hope may provide an idea of possible ease of access in the passage of electrode arrays. By this classification little or no difficulty is expected in obstructions in which less than 80% (that is, 20% obstruction or less) of the niche is obstructed with or without a thickened membrane.
Permission to use the archival temporal bone database was given by the UCL Ear Institute, ethical approval was not required in this instance.
RESULTS
A total of 15 temporal bone (TB) sections were examined. Some of the TB photomicrographs were not of good quality and artefacts were noted. The round window niche and round window membrane was obstructed and/or narrowed by Otosclerotic plaque in 6 (40%) of the temporal bone slides. The round window was affected in varying severity in 6/15 TB sections while total bridging/obstruction of the round window niche was observed in 3 out of this 6 TB sections. Otosclerosis affecting the Scala tympani with subsequent total obstruction of round window niche and round window membrane was observed in 1 of 6 TB sections (Figure 1).

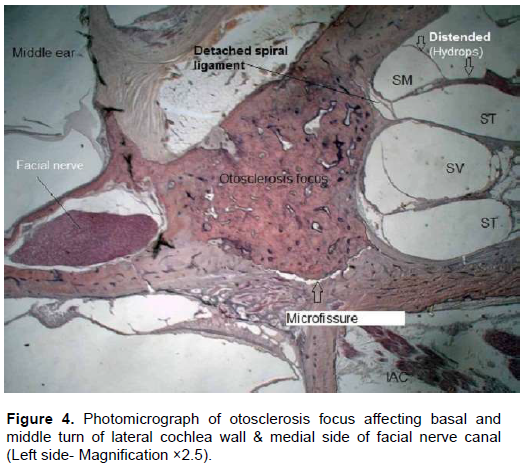
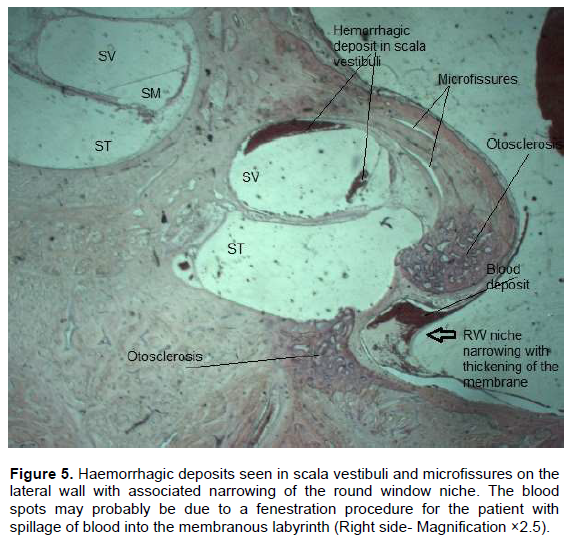
Round window niche obstruction together with thickened RW membrane was observed in 4 out of 6 of the TB sections. Two of these had greater than 80% of the RW obstructed, while the other two had less than 80% obstruction (Figures 2 and 3). The remaining 2/6 TBs had only thickening of the RW membrane. Amongst the six TB sections with otosclerosis in contact with lateral cochlea wall and facial nerve, there were features of associated atrophy and hyalinisation of spiral ligament in 3 out of 6 TB sections. Cochlear hydrops was also noted in 1/6 TB section with detachment of the spiral ligament in the middle cochlea turn (Figure 4). Evidence of microfissures and microfractures were also noted at the junction of otosclerotic and normal endochondral bone (Figures 2 to 5).
DISCUSSION
Histopathologic studies hold prospects for predicting potential difficulties during surgical procedures especially cochlear implantation. This study estimates that 1 out of every 5 persons with otosclerosis (20%) may potentially have insertion difficulties during cochlear implantation due mainly to structural obstruction from Otosclerotic foci.
However studies about otosclerosis using temporal bones (TB) are difficult due to paucity of donors, and the Ear Institute Temporal Bone archive is an invaluable source of temporal bones. Therefore, this study is unique as it is able to assess potential clinical problems from a histopathologic standpoint.
There were several limitations to this study such as missing temporal bone sections, loss of quality over time of the TB sections, lack of complete clinical and audiological data, and small sample size (15) to infer clinically-based significant conclusions. There was also some bias in the selection process due to the aforementioned reasons in order to get presentable sections. We admit that temporal bone studies can be complicated by multiple uncontrollable variables.
Insertion difficulties due to neo-ossification is particularly common in patients with otosclerosis within or around the round window and scala tympani; this was the finding of Silveira and Linthicum (2011). In this study, 6 (40%) of the temporal bone slides revealed areas of neo-ossification/obstruction of the round window, scala tympani and round window niche by active otosclerosis.
Occasionally during cochlear implantation for otosclerosis, the round window niche may be obstructed by neo-ossification thus making insertion of electrode arrays difficult. The round window and round window niche was obstructed in varying severity in 6 out of 15 TB sections. In three of fifteen TB section (20%), there was complete obstruction of the round window niche (RWN). Intra-operatively this may potentially cause difficulties with insertion of the electrode arrays necessitating drill-out procedures (Fayad et al., 1990). However, with a high index of suspicion, proper pre-operative planning with imaging studies, decisions can be made to proceed or to reschedule the procedure. Added with ossification of the round window membrane and/or scala tympani (Quaranta et al., 2005) is a dilemma which may require implantation on the contralateral ear (Figure 1). However, Fayad et al. (1990) compared results to surgical data on the extent of drilling and depth and ease of placement of the electrode in 20 patients’ deaf from otosclerosis (Fayad et al., 1990). They concluded that obstruction of the basal turn, which occurs in some otosclerotic patients, does not preclude implant surgery. This was however not the case with Rotteveel et al. (2004) who recorded problematic insertion in 10 (19%) of their cohort resulting in partial/misplaced insertion requiring revision surgery (Rotteveel et al., 2004).
Furthermore, Balkany et al. (1996) found that neo-ossification was usually partial. Fluid-filled scala tympani were identified in most cases, by imaging and/or intra-operatively, and all the electrodes were inserted successfully (Balkany et al., 1996). Moreover, in the present study, 3 out of 15 (20%) TB sections showed evidence of obstruction of the RW niche but in only one section was ossification of the basal turn/scala tympani observed. This ossification was also partial, it did not affect the entire basal turn/scala tympani (Figure 1). In comparison, Quaranta et al. (2005) in their series observed ‘ossification of the basal turn’ in 3 of 9 (33%) patients versus one out of 15 TB (>6%) sections in the present study (Quaranta et al., 2005). The higher percentage may be due to a smaller cohort compared to our TB samples, although this may not be clinically and/or statistically significant.
Round window ‘obstruction’ coupled with ‘thickened’ RW membrane was observed in four of fifteen TB sections (26.7%). Quaranta et al. (2005) in their series reported eight of nine otosclerosis patients (>88%) with ossification of the round window (RW) membrane. We observed ossification/obstruction of the RW membrane in only one of 15 TB (6.7%) sections as well. This frequency of RW obstruction by Quaranta et al. (2005) is quite high when compared with the present series despite our larger sample population (Quaranta et al., 2005). Although, our value may not be as high but it is equally significant, since more than 26.7% of our sections were similarly affected. By implication during cochlear implantation, this neo-ossification may result in damage to spiral ligament and stria vascularis due to insertional resistance. By implication, this may mean that obstructive neo-ossification in the RW is perhaps not an uncommon finding amongst patients with cochlear otosclerosis.
In addition, the low frequency of obstruction (6%) of the RW membrane of the present study due purely to ossification may not be correct since the selection was somewhat biased. Early detection therefore may be the easiest prophylaxis even though our values may not be statistically significant. This study being a post-mortem study, but in life this is readily achieved with imaging studies. The sensitivity of high resolution computer tomography (HRCT) in detecting cochlear ossification is said to be between 71 and 78%, with complimentary magnetic resonance imaging (MRI) this value is much higher (Arriaga and Carrier, 1996; Quesnel et al., 2013). Some of the features to look out for on CT are the double ring effect or enchondral banding which are radiolucent areas surrounding the cochlea. Pericochlear lucencies have been reported to be highly specific for cochlear otosclerosis (Marsh et al., 1992; Purohit and Hermans, 2014).
Furthermore, in RW areas with greater than 80% obstruction (Figure 2), some difficulty is to be anticipated requiring possible drill-out or cochleostomy via an alternative route. These obstructions/narrowing are in the form of growth by active otosclerosis obscuring the round window niche. We found 2 of 15 TB (13%) sections with less than and greater than 80% obstruction by neo-ossification, respectively. In addition, thickened RW membrane is easily perforated during or after the cochleostomy, thus, presents no real threat to insertion of the electrode arrays. In our series, only two of six TB sections revealed thickening of the RW membrane without associated narrowing of the RW niche.
Implications for cochlear implant surgeons
Balkany et al. (1996) described three ossification patterns in the cochlea of their patients: obliteration of the round window niche, obstruction confined to the lower segment of the basal turn, and complete basal turn obstruction (Balkany et al., 1996). We were able to identify two of such patterns but not complete basal turn obstruction. Meaning these observations are not uncommon and devising alternative means to electrode insertion techniques as well as substitute electrode material, is paramount if these complications are to be avoided or minimised.
Unanswered questions and future research
There were a few grey areas; this study was unable to answer such as: Why does cochlear otosclerosis have a predilection for certain parts of the otic capsule or the otic capsule in general, what other approach may avert insertion resistance?
The latter question has had several suggestions from different authors, Balkany et al. (1996) suggested a middle fossa approach. Inserting the electrode, this way obviates the need for cumbersome surgery such as radical mastoidectomy, carotid artery skeletonization, and drilling of the bone surface of the basal turn around, the modiolus. Why does facial nerve stimulation occur in otosclerotic patients before or after cochlear implantation? These unanswered questions are beyond the scope of this study and further research is required.
CONCLUSION
The outcome of this TB study revealed a 40% prevalence of narrowed or obstructed RW niches. Complications during cochlear implantation such as RW niche obstruction may be an impediment to a favourable surgical outcome among patients with otosclerosis. Neo-ossification around the RW may actually have a high frequency of occurrence and as such implant surgeons must be wary. Anterior superior cochleostomy in the RW area is the current method of choice and is adjudged to have less morbidity compared to the middle fossa approach as reported in a related study (Balkany et al., 1996). Therefore, early high-resolution imaging is advised in advanced otosclerosis to identify possible round window and/or scala tympani obstruction by otosclerotic changes. These histological features underpin the need to counsel patients regarding the possibility of facial nerve stimulation, difficult implantation and why this may occur. It is hoped that this will serve as a memoir for the cochlear implant surgeon in Nigeria.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
ACKNOWLEDGMENTS
The author sincerely thanks Professor Thanos Bibas for his unflinching patience, valuable advice and encouragement throughout the preparation of the manuscript during his stay at UCL; Professor Doris Bamiou (UCL Ear institute) and Saeed Shakeel (Royal National Throat, Nose and Ear Hospital, London) for their help, support, supervision and comments despite their tight schedules; Ruth Taylor (Ear Institute, London) who was always around to point me in the right direction in the laboratory; and indeed grateful to the entire Ear Institute staff who in one way or the other have made my stay a memorable one.
REFERENCES
|
Arriaga MA, Carrier D (1996). Mri and clinical decisions in cochlear implantation. American Journal of Otology 17(4):547-553. |
|
|
Balkany T, Gantz BJ, Steenerson RL, Cohen NL (1996). Systematic approach to electrode insertion in the ossified cochlea. [Case Reports]. Otolaryngology - Head and Neck Surgery 114(1):4-11. |
|
|
Berrettini S, Forli F, Neri E, Segnini G, Franceschini SS (2002). Scala vestibuli cochlear implantation in patients with partially ossified cochleas. [Case Reports]. Journal of Laryngology and Otology 116(11):946-950. |
|
|
Chen W, Campbell C, Green G, Van Den Bogaert K, Komodikis C, Manolidis L, Aconomou E, Kyamides Y, Christodoulou K, Faghel C, Giguere C, Alford R, Manolidis S, Van Camp G, Smith R (2002). Linkage of otosclerosis to a third locus (otsc3) on human chromosome 6p21.3-22.3. Journal of Medical Genetics 39(7):473-477. |
|
|
de Souza C, Goycoolea MV (2014). Pathology of otosclerosis. Otosclerosis: Diagnosis, Evaluation, Pathology, Surgical Techniques, and Outcomes P 3. |
|
|
Declau F, Van Spaendonck M, Timmermans JP, Michaels L, Liang J, Qiu JP, Van de Heyning P (2001). Prevalence of otosclerosis in an unselected series of temporal bones. Otology and Neurotology 22:596-602. |
|
|
Escada PA, Capucho E, Chorão M, da Silva JF (2007). Otosclerosis of the incus. [Case report]. Otology and Neurotology 28:301-303. |
|
|
Fayad J, Moloy P, Linthicum FH-Jr (1990). Cochlear otosclerosis: Does bone formation affect cochlear implant surgery? [Comparative Study Review]. American Journal of Otolaryngology 11(3):196-200. |
|
|
Frijns JHM, Kalkman RK, Briaire JJ (2009). Stimulation of the facial nerve by intracochlear electrodes in otosclerosis: A computer modeling study. [Research Support, Non-U.S. Gov't]. Otology and Neurotology 30(8):1168-1174. |
|
|
Gildener-Leapman N, Linthicum-Fred H-Jr (2011). Histopathology of cochlear otosclerosis: Implications for cochlear implantation. Otology and Neurotology 32(7):e56-e57. |
|
|
Hueb MM, Goycoolea MV, Paparella MM, Oliveira JA (1991). Otosclerosis: The university of minnesota temporal bone collection. Otolaryngology and Head and Neck Surgery 105:396-405. |
|
|
Makarem A, Linthicum FH (2008). Cavitating otosclerosis. Otology and Neurotology 29:730-731. |
|
|
Marsh MA, Coker NJ, Jenkins HA (1992). Temporal bone histopathology of a patient with a nucleus 22-channel cochlear implant. American Journal of Otology 13(3):241-248. |
|
|
Michaels L, Soucek S (2011). Origin and growth of otosclerosis. Acta Oto-Laryngologica 131(5):460-468. |
|
|
Munoz-Fernandez N, Morant-Ventura A, Achiques MT, Dualde-Beltran D, Garcia-Callejo FJ, Monrroy-Parada MV, Marco-Algarra J (2012). Evolution of otosclerosis to cochlear implantation. Acta otorrinolaringologica espanola 63(4):265-271. |
|
|
Ohtani I, Baba Y, Suzuki T, Suzuki C, Kano M, Deka RC (2003). Why is otosclerosis of low prevalence in Japanese? Otology and Neurotology 24:377-381. |
|
|
Purohit B, Hermans R (2014). Imaging in otosclerosis: A pictorial review. Insights into Imaging 5(2):245-252. |
|
|
Quaranta N, Bartoli R, Lopriore A, Fernandez-Vega S, Giagnotti F, Quaranta A (2005). Cochlear implantation in otosclerosis. [Evaluation Studies]. Otology and Neurotology 26(5):983-987. |
|
|
Quesnel AM, Moonis G, Appel J, O'Malley JT, McKenna MJ, Curtin HD, Merchant SN (2013). Correlation of computed tomography with histopathology in otosclerosis. Otology and Neurotology 34(1):22-28. |
|
|
Richard C, Doherty JK, Fayad JN, Cordero A, Linthicum FHJ (2015). Identification of target proteins involved in cochlear otosclerosis. Otology and Neurotology 36(5):923-931. |
|
|
Rotteveel LJC, Proops DW, Ramsden RT, Saeed SR, Van Olphen AF, Mylanus EAM (2004). Cochlear implantation in 53 patients with otosclerosis: Demographics, computed tomographic scanning, surgery, and complications. Otology and Neurotology 25:943-952. |
|
|
Ruckenstein MJ, Rafter KO, Montes M, Bigelow DC (2001). Management of far advanced otosclerosis in the era of cochlear implantation. Otology and Neurotology 22(22):471-474. |
|
|
Sebahattin C, Muzeyyen, Yildirim B, Michael MP (2010). Cochlear otosclerosis. Current Opinion in Otolaryngology and Head and Neck Surgery 18(5):357-362. |
|
|
Silveira ARO, Linthicum FH-Jr (2011). New bone formation in patients with cochlear implants and otosclerosis. Otology and Neurotology, 32(9):e38. |
|
|
Stankovic KMM, McKenna MJ (2006). Current research in otosclerosis. Current Opinion in Otolaryngology and Head and Neck Surgery 14:347-351. |
|
|
Thys M, Van Den Bogaert K, Iliadou V, Vanderstraeten K, Dieltjens N, Schrauwen I, Van Camp G (2007). A seventh locus for otosclerosis, otsc7, maps to chromosome 6q13-16.1. European Journal of Human Genetics 15(3):362-368. |
|
|
Velegrakis GA (2011). Otosclerosis: State of the art. [Review]. Otorhinolaryngologia - Head and Neck Surgery 43:6-16. |
|
|
Yaralı M, Özkan HB, Bajin D, Batuk M, Çınar B, SennaroÄŸlu G, SennaroÄŸlu L (2015). Cochlear implantation after failed stapes surgery in far advanced otosclerosis. Journal of International Advanced Otology P 11. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


