Full Length Research Paper
ABSTRACT
The culture of the people is central to the traditional medicine knowledge, uses and trade. This indigenous knowledge is orally passed from one generation to the next and is shared through efficacious communication with the ancestral spirits, dreams and oral narratives. This traditional medicine knowledge is invaluable in the treatment of sociocultural illnesses or syndromes, for instance, bad luck, bad dreams, cultural curses, and are resourceful in the administration of significant cultural rites and ceremonies. The traditional medicine sold in the medicine markets of Kenya is a true reflection of the cultural norms, beliefs and interactions among various cultures in a particular area. Cultural evolution phenomenon often takes place as a result of immigration, assimilation, interaction and acculturation. As a result these cultural changes affect; the autochthonous culture of their newly adopted homes and provides a sense of belonging to the people.
Key words: Culture, traditional medicine knowledge, cultural evolution, changes.
INTRODUCTION
Traditional medicine in African continent has been linked more to the culture of the indigenous people with regard to their social life, tribal set up, cultural beliefs and more so their daily activities (Fajinmi et al., 2017). The broader concept of traditional medicine is clearly defined as the cumulative knowledge, skills and practices that is cultural specific and important in the maintenance of both physical and mental health, and often exploited in the prevention, diagnosis, and treatment of diseases (Gakuya et al., 2020). In Kenya, the development of Traditional Medicine (TM) has grown over the years and has been regulated by health laws and policies. This has enabled the formalization of a largely informal industry. The most conspicuous distraction was the colonial Witchcraft Law of 1925 which criminalized some aspects of Traditional Medicine, for instance, in the possession of charms and amulets. The practice of TM was considered a threat to the Colonial Government and crackdown on active practitioners by the imperial administration slowed the growth of TM, many TM practitioners were scared from TM practice. Traditional hallucinogenic substances have been prescribed for ceremony related conditions, and others dispensed for cleansing ceremonies using holy water, perfumes or even flower bath; some patients are however given protective herbal amulets or charms.
TM markets in Kenya
There exists little information about medicinal plants trade in Kenya with respect to the nature and volume of trade. However, it is reported that frequently traded medicinal plant species do account for a high annual volume per kg translating in a higher annual retail value. Only seven out of thirty recorded species in Moyale and Marsabit medicine markets accounted for an annual volume of 5500 kg and an annual retail value of US$ 25,900.00. Most TM traders decry little income from TM and thus have learnt to diversify into other goods, for instance, candy, tobacco, beads and jewelry, foodstuffs, and even clothes. Few ethnobotanical studies in Kenya have reported massive number of medicinal plant species used in the treatment of various diseases. Most of the species are traded within counties and some are area specific as dictated by varying cultural and societal beliefs. Just like many other Kenyan TM markets, Kajiado, Narok and Nairobi medicine markets have revealed that TM markets are dominated by older practitioners, female traders, and most of the traders demonstrated low literacy levels. Area plant use specificity is influenced by varying ethnic compositions, cultural beliefs and norms (Delbanco et al., 2017; Mwaura et al., 2020). However, heightened trade in TM particularly in urban medicine markets may pose a serious biodiversity threat in the respective plant sources, mainly those sourced from the wild (Muriuki et al., 2012). The main pool of customers for urban and peri-urban TM markets is the passers-by mostly comprised of the local inhabitants. Therefore, the TM markets present the frequently traded and harvested species, plant parts utilized and enable conservationists to draw botanical checklists for conservation and sustainability of the TM trade and indigenous knowledge.
Sociocultural illnesses
It has been documented that most rural communities, for instance, the indigenous Samburu people of Kenya believe that sociocultural illnesses are mainly caused by sorcery attacks and can be addressed by community approved diviners who have the capacity and blessings to administer ritual protective medicines. These cultural-bound illnesses are largely thought to be unusual occurrences and are often triggered by mystical or mythical causes like curses from kinsmen.
Traditional medicine is culturally believed to eliminate the effects of witchcraft and help appease the spirits not to cause unforeseen harm or bad luck (Tabuti et al., 2003). Up to 70% of the infamous ethnic Maasai of Kenya approve the use of ethnomedicine (Kiringe, 2006). Most cleansing ceremonies are performed by sprinkling or spraying of mixtures of several traditional medicine or medicinal plants solutions onto their patient’s body to exorcise or purge evil spirits in order to obliterate societal or cultural inflicted curses. Rituals and ceremonies often mark important life events of the indigenous, local, tribal or cultural bound communities (Fajinmi et al., 2017).
Current regulatory environment for TM
The TM industry in Kenya was a vibrant and acceptable enterprise before colonialism then it entered a stationary phase during the colonial period. This was necessitated by the illusion that the TM practitioners were averse to the colonial administration and that the freedom fighters used charms and amulets as weapons of productive resistance. Before a TM practitioner commences practice, he or she must first comply with the cultural norms, taboos and beliefs of the community in what can be termed as the silent and informal rules of the game. Currently, with the new constitutional dispensation, TM is governed by parliamentary bills and acts, government policies and county by-laws. The respective counties regulate the practice in both designated locations or non-designated market sites like shop front spaces or town avenues and streets. The assigned county staff charge daily market levies which varies from KES 30 to KES 50 per day.
Lack of compliance on the part of TM traders may signal arrests or market expulsion by county authorities. The progressive Constitution of Kenya 2010 sets the stage for a sustainable exploitation, utilization, management and conservation of natural resources and biodiversity, equitable sharing of the accruing benefits, and calls for protection of the indigenous knowledge of biodiversity and genetic resources of the communities (Constitution of Kenya, 2010). Generally speaking, the CoK 2010 under the Bill of Rights guarantees the right to health care for every Kenyan citizen. The history of law and policy formulation for TM practice is impressive, Kenya has several good laws governing TM and the only thing left is their improvement and enforcement as summarized by Chebii et al., 2020. Given a bad start by the punitive Witchcraft Act of 1925, great legislations and policies have been passed and formulated respectively. The Ama Ata Declaration of 1978 set the agenda for provision of primary health care to all and challenged governments to formulate efficacious health policies, strategies and plans of action. Quite significant was the Development Plan (1989-1993), which was a boost to TM practitioners by recognizing the TM practice, TM practitioners’ social welfare, good working environment and registration of all practitioners. The Kenya National Drug Policy of 1994 acknowledged TM as a key component of our culture. Huge strides were realized with the Sessional paper of 2009 where it fosters TM regulation, set up relevant robust institutions, emphasized on the contribution of TM in health care delivery, safety and drug efficacy. Lastly, the Sessional paper of 2009 propagates both ex situ and in situ conservation of threatened medicinal plants. The Health Act No. 21 of 2017 empowers the Department of Health to provide policies and regulatory institutions that properly guides the TM practice. Like the Kenya’s National Drug Policy (1994), the Health Laws Act, No. 5 of 2019 also recognized TM as a health product. Currently, improvements are being made on the past bills particularly the Health Act, No. 21 of 2017 under the parliamentary amendment bill dubbed the Health Laws (Amendment) Bill of 2021.
METHODOLOGY
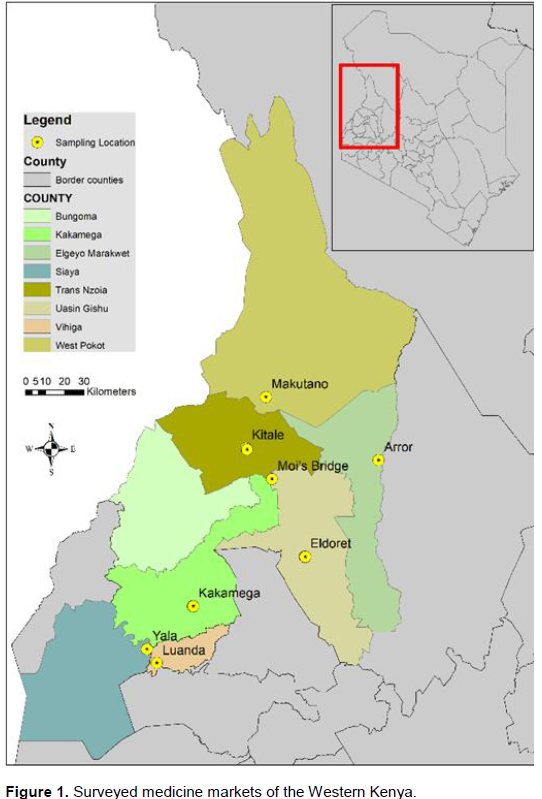
The field survey was conducted in the TM markets of Western Kenya in the purposively selected counties of Uasin Gishu (Eldoret market), Trans Nzoia county (Moi’s Bridge and Kitale markets), West Pokot county (Makutano market), Elgeyo Marakwet county (Arror and Kaptabuk markets), Kakamega county (Kakamega market), Vihiga county (Luanda market), and Siaya county (Yala market). The traditional medicine traders were interviewed with the aid of a pre-tested semi-structured questionnaire using purposive sampling with elements of snow ball sampling. The purposively, knowledgeable and willing TM traders were allowed to recruit other knowledgeable traders practicing in the sampled medicine markets. Overall, thirty (30) practicing TM traders were interviewed (February to September 2019) after obtaining oral prior informed consents and educated on the purpose of the interviews. The GPS coordinates were recorded and sampled locations shown in Figure 1.
In a nut shell, the TM traders were asked to provide information on the importance of TM in tackling sociocultural illnesses and syndromes, the medicinal plants used and their respective plant parts. Mixed methodologies employed in the study included consented sound recordings, and photography, direct observations.
RESULTS
From the field sociocultural survey, the informal trade and practice of TM showcased the treatment of largely non-empirical sociocultural bound illnesses or syndromes, for instance, bad luck, bad dreams, tracing of lost items or person and in fighting imaginary enemies. A high number of medicinal plant species were mentioned to cure a wide range of sociocultural ills or syndromes namely bad air, bad wind, fright, evil eyes or returning a lost or stolen property. The TM traders emphasized the use of pure TM in the treatment of these sociocultural syndromes and discouraged the use of allopathic medicine in this regard. Quite intriguing was the mention of fatalities due to injections on patients possessed or inflicted with sociocultural illnesses. Culturally sensitized customers often buy these traditional medicines from the traders supported by simple verbal or oral medical prescriptions on their safe use. The TM traders intentionally display scanty morphological, vegetative or floral characters that make identification of these frequently traded traditional medicines cumbersome for clients. This helped the traders in protecting their hard earned indigenous medical knowledge, which remain largely undocumented, unregistered and lack intellectual property rights (IPR). Other means used by the TM traders in safeguarding their wealth of indigenous medical knowledge include revealing scanty details about their practice, medicinal plants, drug administration and exact plant location or habitat. On extreme cases, the TM collection mostly from the wild are conducted in the dawn, dusk or in the dead of night to preclude exposing the medicinal plants habitat to uncontrolled exploitation. Other traders source their TM from a small group of trusted TM collectors. The TM traders also mostly used vernacular plant names extracted from the dominant ethnic languages in the respective medicine markets. The established traders passed this rich knowledge to close relatives via competent apprenticeship, attachment and local patient referrals. The exchange of traditional medicine knowledge and the associated cultures is also manifested in the local medicine markets of Western Kenya as demonstrated by the Yala and Luanda medicine markets where predominantly Luo vernacular plant names are trade names in the Luhya-ethnic dominated medicine markets. For instance, the Yala and Luanda medicine market traders share vernacular plant names as exemplified by Ochuoga (Carissa spinarum L.), Abaki (Warburgia ugandensis Sprague), Tido (Ekebergia capensis Sparrm) and Ajua (Toddalia asiatica (L.) Lam Cadaba farinosa Forssk. was frequently traded as a blending drug for all medicine, and surprisingly, the seeds were prescribed as an herbal remedy to confuse and scatter enemies. Chasmanthera dependens Hochst. was sold as a blending drug for all female patients. Finally, Dicliptera laxata C.B Clarke, Hypoestes spp. and the rutaceous Toddalia asiatica (L.) Lam was sold as an herbal remedy for cultural and societal inflicted curses.
Leadership at the medicine markets often follow a patriarchal pattern where traditional medicine traders mostly nominate, appoint or elect men TM traders as their preferred market representative even in women dominated markets.
DISCUSSION
Traditional medicines are extremely significant in the broader context of cultural systems and are significant in addressing spiritual fitness and matters divine that involve clarity of thoughts and dreams (Sobiecki, 2014). Rituals involving the use of traditional medicine have been practiced for years by indigenous cultures but have now found their way to the local medicine markets and also used by immigrants outside their ancestral areas. Several ritual cures have been documented; the indigenous Kenyan Samburu tribal diviners are known to dispense several medicinal plants to treat various sociocultural illnesses or syndromes. For instance, the root barks of Toddalia asiatica (L.) Lam (l-paramunyo) and Rhamnus staddo A. Rich. (l-kukulai) are normally grounded and mixed to cure madness, fits and epileptic seizures, whereas Ficus wakefieldii Hutch. is dispensed to treat women barreness or long term infertility (Fratkin 1996). The concept of cultural export in traditional medicine by immigrants worldwide is therefore a harsh reality. The new migrants import traditional medicine from their former home country and therefore contribute in shaping the autochthonous culture of their newly adopted home. Indigenous cultures are often vulnerable to change due to emigration and integration forces over a period of time (Bussmann and Sharon, 2006; Volpato et al., 2009). In the course of acculturation, the immigrants tend to modify beliefs toward their autochthonous indigenous cultures and slowly adapt to their host culture (Barimah and van Teijlingen, 2008).
A broad-based ethnobotanical survey in the cultural-rich Tharaka-Nithi County in Kenya revealed some vital cultural medicinal plants that were exploited for rituals and sacred ceremonies. Abrus precatorius L. legume producing elegant mixed black-red colouration was found useful in male initiation ceremonies. Other cultural plant species include Ricinus communis L, Solanum incanum L, Podocarpus latifolius (Thunb). R.Br. ex Mirb. and Senna didymobotrya (Fresen) H. S. Irwin and Barneby (Kathambi et al., 2020). Leading cultural factors that are significantly valued in traditional medicine realm include the language used, social networks created and the true meaning response of the medicinal plants which serves to express diverse traditional plant uses (Menendez- Baceta et al., 2015).
Similar to the study findings, ethno-taxa are widely used in these informal medicine markets and are normally derived from the dominant ethnic languages in the urban or peri-urban areas (Otieno et al., 2015). As much as most TM traders learnt TM from their close relatives, others claimed to have learnt their TM knowledge through communication with their ancestral spirits, nature spirits or even dreams (Tabuti et al., 2003). Quite remarkable is the transmission of these cultural medicine knowledge through folklore songs and narratives, some of which are gender specific (Kathambi et al., 2020). Medicinal plants form a huge component of traditional medicine and are largely maintained by local customs and indigenous knowledge. Most of these cultural and traditional therapies are culturally intertwined and are prone to erosion courtesy of the ever changing lifestyles, societal perceptions, social transformations and acculturation (Kunwar et al., 2013). Cultural erosion is also exacerbated by many factors including spread of western religion, western education and promotion of allopathic medicine (Kiringe, 2006). The trade in traditional medicine, particularly those directly attached to the market value chain retains immense wealth of knowledge on medicinal plant uses (Salim et al., 2019).
The major drawback of ethno-taxa or indigenous nomenclature as compared to the globally accepted botanical nomenclature is their non-specific nature and lack of universality in application where one common name may refer to multiple plant species (Bussmann and Sharon, 2006). Cultural based medicine knowledge and informal trade is formally regulated at the medicine markets through a systematic vetting process where traditional medicine traders are issued with a certificate of practice by the Department of Culture. Furthermore, the local county governments charge market levies. Licensing of cultural practice can be partly construed as a validation of the traditional medicine knowledge, although this is a contestable proposition. Nationally, the TM industry is regulated by a myriad laws and policies (Chebii et al., 2020). However, the traditional medicine traders suffer societal prejudices by some people classifying them as witchdoctors. This erratic condemnation of cultural practices contributes to the slowing of the TM industry in the developing nations.
The administration of these somewhat informal traditional medicine markets is culturally guided by traditional governance practices, where in some African cultures, menstruating women are considered impure and thus barred from active practice. In addition, medicine administered to different gender have unique blending medicine, and more punitive is barring men from conjugal activities as they proceed to conduct traditional healing in an embodiment of purity (Chebii et al., 2020). Ethnomedicinal uses have been established to be culturally intertwined and therefore traditional plant uses vary among communities. Cultural taboos and social restrictions have positively contributed to the informal regulation of medicinal plants harvesting and preclude over-exploitation, whereas gifted traditional healers are basically the principal custodians of the rich traditional medicine knowledge, most of which remains undocumented (Augustino and Gillah, 2005; Mathibela et al., 2015). Regarding its quintessential socio-demographic traits and pattern, the principal holders of the key sociocultural values and taboos are mainly the elderly people, most commonly the indigenous rural folk (Plieninger et al., 2020). Biopiracy and bio-prospecting missions targeting local plant resources for profit making or patent rights threatens traditional knowledge systems and cultural innovations of the local communities (Ageh and Lall, 2019). This heightens suspicion and exacerbates decline in indigenous or traditional medicine knowledge, decreased cultural practices and negatively influence the transfer to future generations (Ens et al., 2016).
CONCLUSION
TM is ideal in the treatment of most sociocultural illnesses or syndromes since it fits the requirements and expectation of cultural and societal inflicted problems like curses, bad luck, bad spells, countering enemies or adversity, tracing lost items or persons, evil eyes and a host of sociocultural bound issues. This is because these illnesses are mostly spiritual and psychological and cannot be effectively addressed using allopathic medicine. Societal and cultural beliefs are significant in the performance of rituals and sacred ceremonies. Therefore, there is need for closer emphasis on this under-researched area since most researchers focus on the uses of TM in the treatment of general diseases. TM should be integrated with allopathic medicine and explored in the treatment of mental and psychosocial illnesses. Immigrants also utilize medicinal plants exports and this has had an effect on coexistence and blending of both autochthonous and allochthonous cultures. Medicinal plants used as a whole or in parts have proved efficacious in the treatment of these sociocultural bound illnesses and have been used for ages. They should therefore be professionally determined and prioritized for conservation and protection. Voices from the TM markets should not be ignored or muted but amplified with continuous research to bolster the TM industry.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ageh PA, Lall N (2019). Biopiracy of plant resources and sustainable traditional knowledge system in Africa. Global Journal of Comparative Law 8(2):162-181. |
|
|
Augustino S, Gillah PR (2005). Medicinal plants in urban districts of Tanzania: plants, gender roles and sustainable use. International Forestry Review 7(1):44-58. |
|
|
Barimah KB, Van Teijlingen ER (2008). The use of traditional medicine by Ghanaians in Canada. BMC Complementary and Alternative Medicine 8(1):1-10. |
|
|
Bussmann RW, Sharon D (2006). Traditional medicinal plant use in Loja province, Southern Ecuador. Journal of Ethnobiology and Ethnomedicine 2(1):1-11. |
|
|
Chebii WK, Muthee JK, Kiemo K (2020). The governance of traditional medicine and herbal remedies in the selected local markets of Western Kenya. Journal of Ethnobiology and Ethnomedicine 16(1):1-24. |
|
|
Delbanco AS, Burgess ND, Cuni-Sanchez A (2017). Medicinal Plant Trade in Northern Kenya: Economic Importance, Uses, and Origin1. Economic Botany 71(1):13-31. |
|
|
Ens E, Scott M, Rangers YM, Moritz C, Pirzl R (2016). Putting indigenous conservation policy into practice delivers biodiversity and cultural benefits. Biodiversity and Conservation 25(14):2889-2906. |
|
|
Fajinmi OO, Olarewaju OO, Staden JV (2017). Traditional use of medicinal and aromatic plants in Africa. In Medicinal and Aromatic Plants of the World-Africa 3: 61-76. Springer, Dordrecht. |
|
|
Fratkin E (1996). Traditional medicine and concepts of healing among Samburu pastoralists of Kenya. Journal of Ethnobiology, 16:63-98. |
|
|
Gakuya DW, Okumu MO, Kiama SG, Mbaria JM, Gathumbi PK, Mathiu PM, Nguta JM (2020). Traditional medicine in Kenya: Past and current status, challenges, and the way forward. Scientific African 8:e00360. |
|
|
Kathambi V, Mutie FM, Rono PC, Wei N, Munyao JN, Kamau P, Gituru RW, Hu GW, Wang QF (2020). Traditional knowledge, use and conservation of plants by the communities of Tharaka-Nithi County, Kenya. Plant diversity 42(6):479-487. |
|
|
Kiringe JW (2006). A survey of traditional health remedies used by the Maasai of Southern Kajiado District, Kenya. |
|
|
Kunwar RM, Mahat L, Acharya RP, Bussmann RW (2013). Medicinal plants, traditional medicine, markets and management in far-west Nepal. Journal of Ethnobiology and Ethnomedicine 9(1):1-0. |
|
|
Mathibela MK, Egan BA, Du Plessis HJ, Potgieter MJ (2015). Socio-cultural profile of Bapedi traditional healers as indigenous knowledge custodians and conservation partners in the Blouberg area, Limpopo Province, South Africa. Journal of Ethnobiology and Ethnomedicine 11(1):1-11. |
|
|
Menendez-Baceta G, Aceituno-Mata L, Reyes-García V, Tardío J, Salpeteur M, Pardo-de-Santayana M (2015). The importance of cultural factors in the distribution of medicinal plant knowledge: a case study in four Basque regions. Journal of Ethnopharmacology 161:116-127. |
|
|
Muriuki J, Franzel S, Mowo J, Kariuki P, Jamnadass R (2012). Formalisation of local herbal product markets has potential to stimulate cultivation of medicinal plants by smallholder farmers in Kenya. Forests, Trees and Livelihoods 21(2):114-127. |
|
|
Mwaura A, Kamau J, Ombori O (2020). An ethnobotanical study of medicinal plants commonly traded in Kajiado, Narok and Nairobi counties, Kenya: Medicinal Plant Species Traded in Kenya. East African Journal of Science, Technology and Innovation 1(3). |
|
|
Otieno J, Abihudi S, Veldman S, Nahashon M, van Andel T, de Boer HJ (2015). Vernacular dominance in folk taxonomy: a case study of ethnospecies in medicinal plant trade in Tanzania. Journal of Ethnobiology and Ethnomedicine 11(1):1-7. |
|
|
Plieninger T, Quintas?Soriano C, Torralba M, Mohammadi Samani K, Shakeri Z (2020). Social dynamics of values, taboos and perceived threats around sacred groves in Kurdistan, Iran. People and Nature, 2(4):1237-1250. |
|
|
Salim MA, Ranjitkar S, Hart R, Khan T, Ali S, Kiran C, Parveen A, Batool Z, Bano S, Xu J (2019). Regional trade of medicinal plants has facilitated the retention of traditional knowledge: case study in Gilgit-Baltistan Pakistan. Journal of ethnobiology and ethnomedicine 15(1):1-33. |
|
|
Sobiecki J (2014). The intersection of culture and science in South African traditional medicine. Indo-Pacific Journal of Phenomenology 14(1). |
|
|
Tabuti JR, Dhillion SS, Lye KA (2003). Traditional medicine in Bulamogi county, Uganda: its practitioners, users and viability. Journal of Ethnopharmacology 85(1):119-129. |
|
|
Volpato G, Godínez D, Beyra A, Barreto A (2009). Uses of medicinal plants by Haitian immigrants and their descendants in the Province of Camagüey, Cuba. Journal of Ethnobiology and Ethnomedicine 5(1):1-9. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


