Full Length Research Paper

ABSTRACT
Multi Drug Resistant Tuberculosis (MDR-TB) is a public health challenge, which itself remains a global public health problem. Its impact is worsened by co-infection with Human immunodeficiency virus (HIV). In order to institute successful TB control strategies, factors for development of MDR-TB must be understood. This study aimed to identify and describe clinical and demographic determinants for development of MDR-TB among TB patients. This was a cross sectional, hospital-based study conducted between April 2017 and December 2019 involving 428 presumptive MDR-TB patients. Specimens were subjected to GeneXpert MTB/RIF assay, microscopy and Line probe assay for diagnosis of MDR-TB. A questionnaire was used to collect demographic information from patients. The odds of having MDR-TB among patients who were cigarette smokers were four-times compared to non-smoking patients (aOR=3.94; 95%CI: 1.845-8.428, p<0.001). Alcohol abuse increased the chances of having MDR-TB by ten times (aOR=9.98: 95%CI; 2.414-41.267, p=0.001). Being HIV positive strongly increased the likelihood of having MDR-TB (aOR=2266.0: 95% CI; 407.5-2599.8, p<0.001). Compared to treatment failure, relapse and non-adherence were found to be strong predictors for MDR-TB (aOR=64.22: (95% CI; 12.786-322.507) p=0.001), and (aOR=37.44: (95% CI; 3.895-359.836, p=0.002), respectively. HIV infection, TB relapse, history of irregular treatment, cigarette smoking, alcohol abuse, and treatment failure (return) is factors development of MDR-TB. Integrated TB/HIV control programs that will include the establishment of strong diagnostic and drug delivery systems, patient management, and TB resistance surveillance systems are recommended.
Key words: Tuberculosis, multi drug resistant tuberculosis (MDR-TB), HIV, M. tuberculosis, adherence; relapse.
INTRODUCTION
Multi Drug Resistant Tuberculosis (MDR-TB) is a serious and emerging public health problem and a health security threat to the world (World Health Organization (WHO), 2016). MDR-TB is defined as the simultaneous resistance to at least two primary anti TB drugs which are rifampicin (RIF) and isoniazid (INH) (Mulu et al., 2015; Shimeles et al., 2019; Wahab et al., 2009). In 2015, the World Health Organization (WHO) reported an estimated 480,000 new cases of MDR-TB globally and an extra 100,000 people with RIF resistant TB (RR-TB). In 2017, 10 million people developed TB, out of which 1.6 million died (including 330,000 patients among people with HIV). In 2017, the highest incidence of new TB cases were reported in the South-East Asia and Western Pacific regions (62% new cases), followed by the African region, with 25% of new cases (WHO, 2018). Africa is home to over 1 billion inhabitants and is disproportionately affected by TB with 2.6 million of the 10.4 million global tuberculosis cases, making Africa a key geographical area for TB interventions (Ismail et al., 2018).
According to results from 16 epidemiologic surveys conducted in East Africa, the prevalence of MDR among new cases ranges from 0.4% in Tanzania to 4.4% in Uganda, and among recurrent cases ranges from 3.9% in Tanzania to 17.7% in Uganda (Kidenya et al., 2014). As a proportion of total reported cases of TB, the number of confirmed MDR-TB cases ranged from 6/6828 (0.09%) in Burundi to 76/6784 (1.12%) in Rwanda (WHO, 2012a, b, c, d, e, f, g). In Tanzania, a total of 65,902 TB cases of all forms were notified in 2016, which is a 5.6% increase compared to cases reported in 2015, In the same year of 2016, a total of 196 MDR-TB cases were notified country wide among which 158 (82%) were started on MDR-TB treatment from 21 regions of Tanzania (Ministry of Health, Community development, Gender, 2018).
The World Health Organization (WHO) enlists number social determinants that are risks for the development resistance to anti-TB drugs, identifying inadequate therapy as the main cause of progression to MDR-TB (Desissa et al., 2018; Seyoum et al., 2014; World Health Organization, 2014). The major patient-related factor that determines the occurrence of MDR-TB is non-adherence to treatment (WHO, 2003). Reports show that only 48% of MDR-TB cases are successfully treated (Kibret et al., 2017; WHO, 2014b). This is attributed to a diverse set of factors, including co-infection with HIV, tobacco use, alcoholism, the later accelerating MDR-TB development through reduced adherence to treatment, prior TB treatment, and inadequate adherence mainly due to secondary factors such as length of treatment and adverse drug reactions (Desissa et al., 2018; Seyoum et al., 2014; World Health Organization, 2014). Several studies have shown a wide variation in predictors of treatment outcome among countries worldwide (Atif et al., 2017; Monadil et al., 2019; Tamary et al,. 2019). In Sub Saharan Africa, management of MDR-TB cases has become a challenge to the mostly insufficient healthcare systems of respective countries, especially when it is coupled with HIV co infection (Breen and Smith, 2004; Chattu and Kumaryy, 2015). In Tanzania the MDR-TB treatment success rate is estimated at 68%, lower than the WHO recommended rate of over 75% (WHO, 2018).
In order to achieve the 2020 milestones of the End TB Strategy, efforts to control TB must be intensified (Stop TB Partnership, 2018; WHO, 2015). Understanding and mitigating the factors that lead to treatment failure among MDR-TB patients is a prerequisite to such efforts. Since the effect of some of the studied determinants for MDR-TB development are likely to have changed in an era of improved TB diagnostics and management, epidemiologic information on patient determinants that accelerate the development of MDR-TB is urgent. In the present study, we aimed to define demographic and clinical determinants for development of MDR-TB among TB patients in Tanzania.
MATERIALS AND METHODS
Study area
The study was conducted at the Kibong’oto Infectious Diseases Hospital (KIDH), located in Siha District of Kilimanjaro region. The hospital provides care services to MDR-TB patients from all parts of Tanzania as referred cases. The diagnostic laboratory at KIDH which has completed external proficiency testing performs smear microscopy, Mycobacterial culture, Gene Xpert® MTB/Rif assay, and DNA probe for Mycobacterium tuberculosis complex - line probe assay (LiPA) employing Genotype MTBDR plus Ver 2.0 assay.
Study design
This was a prospective cross-sectional study conducted from April 2017 to December, 2019.
Inclusion and exclusion criteria
In this study, inclusion criteria were the presumptive MDR-TB diagnosis, being above 20 years of age and being a Tanzania resident.
Study variables
Demographic variables collected were gender, age, marital status, consumption of alcohol, cigarette smoking, occupation, education level and history of contact with MDR-TB patients. Additional clinical information regarding Treatment history, Smear, HIV status, Irregular treatment was extracted from patient files, for which written informed consent was obtained. The information collected was entered into structured data abstraction form (DAF).
Sample size determination
The minimum sample size for seroprevalence determination was estimated using the Epi Tools online sample size calculator using the formula [Z2·(p)·(1 − p)]/c2, where Z = 1.96 for 95% confidence level (CI), p = expected true proportion of 20.0%, and c = minimal tolerable error at 95% CI (0.05). Computing with the above formula gives a minimum sample size of 246. This study enrolled 428 participants to increase the power of statistical analyses.
Recruitment of participants
We applied consecutive sampling inviting participants coming as referred presumptive MDR-TB patients to KIDH to participate in the study. The study included 428 patients from district and regional hospitals located all over the country who were previously diagnosed with TB, but failed treatment and referred to KIDH as presumptive MDR-TB cases. Among the 428 cases initially enrolled in the study, 100 suspected MDR-TB cases were excluded based on negative results with the Gene Xpert assay. An addition, 20 cases were excluded because of failure to grow in Lowenstein Jensen (LJ) media with glycerol (Hardy Diagnostics, CA, USA). Of the remaining samples, 8 gave invalid results in Line probe assay and thus excluded. After exclusion of the 128 cases, only 300 qualified for the study as confirmed TB cases.
Data collection tools and procedures
The data abstraction form (DAF) used in this study was developed by the investigators. Validity and reliability of the DAF were determined using IBM SPSS ver22.0 software (IBM® Corp., Armonk, NY, USA). It was first piloted on ‘dummy’ patients before commencement of the actual study. After the pre-test, necessary adjustments in phrasing were made accordingly. Demographic information on gender, age, marital status, consumption of alcohol, cigarette smoking, occupation, education level and TB contact history with MDR-TB patients, were collected. Information on relapse or return for treatment, Sputum Smear Score, HIV status, history of irregular treatment was extracted from patient files for which written informed consent was obtained and recorded in structured DAFs.
Collection and processing of sputum samples
Two sputum samples were collected from each patient in a sterile falcon tube (BD Falcon TM BD Biosciences, Indiamart, India). For all of the samples, GeneXpert® MTB/Rif assay (Cepheid, Sunnyvale, CA) was used to test the first sputum sample for molecular confirmation of MDR-TB (Eklund, 2013; Ioannidis et al., 2011). Direct sputum smear microscopy was used to test the second sample for acid fast bacilli (AFB) using fluorescence microscopy (Ryu, 2015; Steingart et al., 2006). All positive sputum samples for AFB were cultured in solid Lowenstein-Jensen (LJ) medium with glycerol (Hi Media Laboratories, GmbH) enriched with 5-10% CO2 for 8 weeks and examined every week to observe the presence of Mycobacterium growth. Positive growths were sub cultured on fresh L.J media with glycerol for further identification. M. tuberculosis was confirmed in cultures using measurements of growth rate, colony morphology, pigmentation and by using commercial biochemical tests (niacin assay, nitrate reduction, and catalase tests) based on their growth characteristics (Kent and Kubica, 1985). Recovered M. tuberculosis from L.J. medium with glycerol culture were used to perform Line Probe Assay (LiPA), employing Genotype MTBDR plus Ver 2.0 assay (Hain Life sciences, GmbH) according to the manufacturer’s instructions (Hainlifescience, 2015).
Gene Xpert MTB/RIF assay
Gene Xpert MTB/RIF assay (Cepheid, Sunnyvale, CA) was performed for all sputum samples as described by the manufacturer. Briefly, the Xpert sample reagent (SR) was added to the samples to be tested as per manufacturer’s instructions. The mixture was shaken vigorously for 15 min during the incubation time at room temperature. Two milliliter of the mixture was transferred to Xpert test cartridge. The cartridge was then loaded into Xpert device. Finally, the results were interpreted by the Gene Xpert DX system from measured fluorescent signals and displayed automatically after 90 min.
Line probe assay
Briefly, LiPA was performed as follows: M. tuberculosis DNA was extracted from recovered M. tuberculosis growth using GenoLyse DNA extraction kit followed by polymerase chain reaction (PCR) to amplify the rpoB gene encoding the β-subunit of RNA polymerase, katG gene encoding for the catalase peroxidase and the promoter region of the inhA gene encoding for the NADH enoyl ACP reductase for the detection of mutations and determination of MDR-TB. Primers and polymerase included in the MTBDRplus Ver. 2.0 assay kit were used for amplification of the genes. The H37Rv quality control M. tuberculosis strain was used as the positive control. The mutations in the rpoB gene associated with rifampin resistance and the mutations in katG and the inhA genes associated with isoniazid resistance among M. tuberculosis were interpreted and determined by the band patterns on the LiPA strips after reverse hybridization of the gene amplicons (Meaza et al., 2017).
Data analysis
Analyses were carried out using STATA version 13 (Stata Corp, College Station, TX, USA). For patients’ baseline data, mean ± standard deviation (SD) and frequencies and proportions were used to report continuous and categorical variables respectively. Chi- square statistical test was used to assess the distributions of patients’ characteristics by MDR-TB status and whether such distributions were different between MDR-TB and non-MDR-TB cases. Accordingly, both bivariate and multivariate logistic regression analysis models were used to examine potential predictive factors associated with MDR-TB. Odds Ratio (OR) was used to present the effects of covariates to MDR-TB development. A p-value of 0.05 or less was considered as the level of statistical significance.
Ethical considerations
Ethical clearance was obtained from Kilimanjaro Christian Medical University College Research and Ethical Review Committee (CRERC). Permission from KIDH authority to conduct the study was also obtained. Before the investigation was performed, written informed consent was obtained from all study participants to allow for their clinical and demographic information to be used for research purpose.
RESULTS
Baseline characteristics of study participants
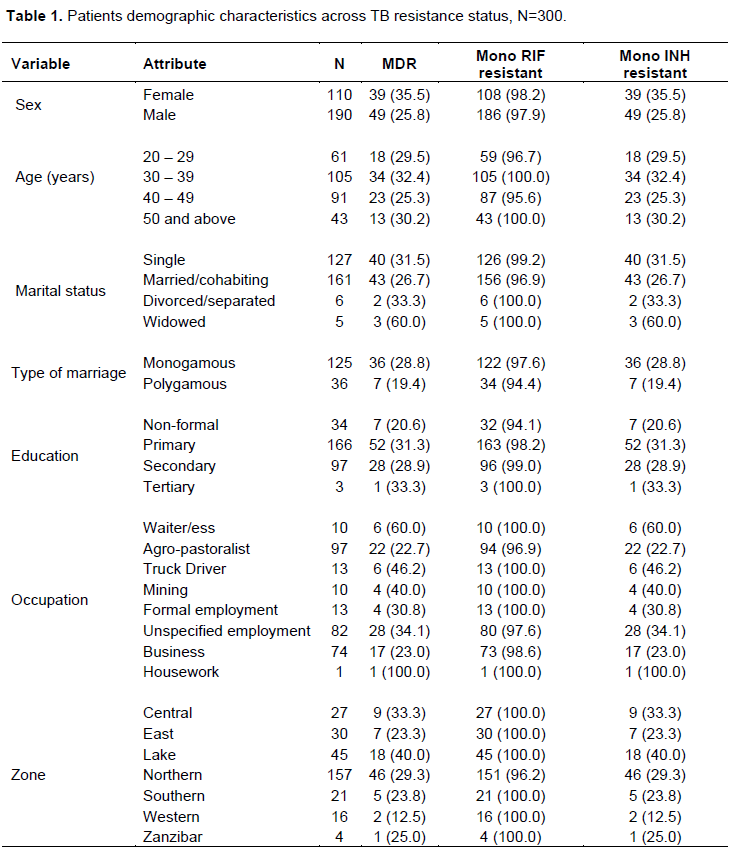
This study included a total of 300 patients who were confirmed to be TB cases by gene expert, sputum culture and LiPA. Out of these, 190 (63.3%) were males. The mean age of the patients was 18 years for males and 37.5 years for females. Majority of patients were in the age of between 30 and 49 years. Nearly half of the patients in this study were from the Northern Zone. In terms of occupation, it was found that majority, 253 (84.3%) of the patients were agro-pastoralists, traders or unspecified occupation (Table 1).
Distribution of patients’ characteristics by MDR-TB status
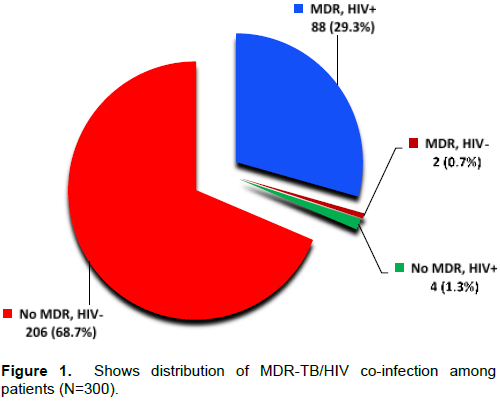
The HIV infection status of all patients was determined, and TB cases were also presented across their HIV infection status. Results presented in Figure 1 show that the proportion of patients with MDR-TB/HIV Co infection was 29.3%, while patients without HIV co-infection was 0.7%. Non MDR-TB with and without HIV co-infection were recorded among 1.3 and 68.7% of patients, respectively.
Association between demographic and clinical determinants of development of MDR-TB among HIV infected patients
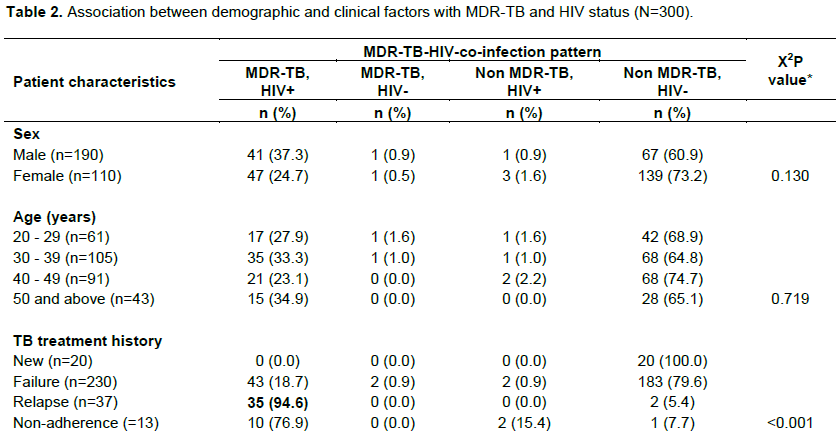
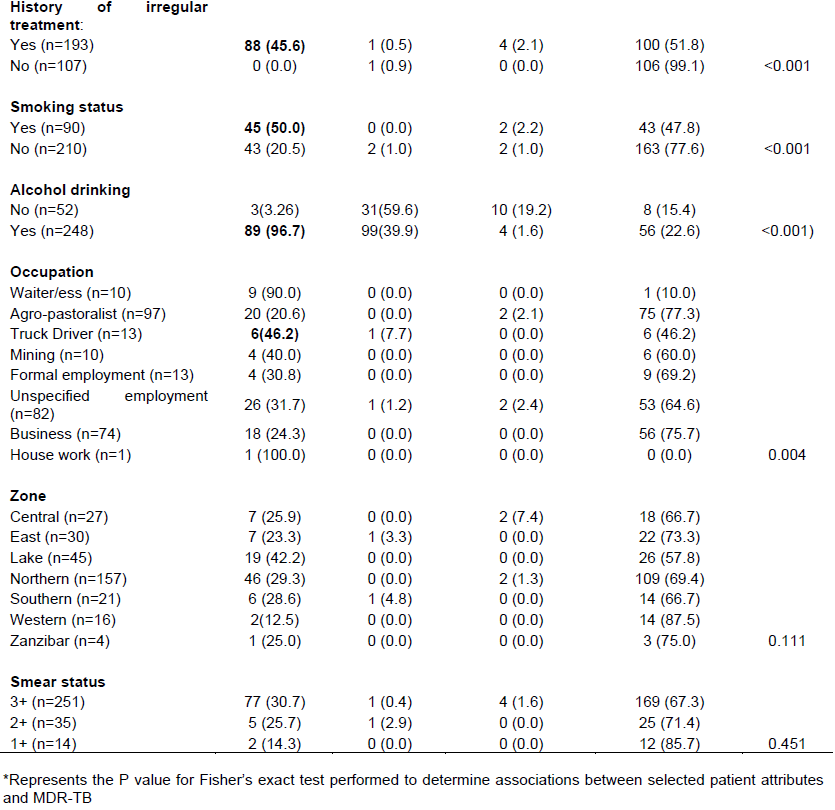
Chi square analyses of associations between patient factors (demographic and clinical factors) and MDR-TB/HIV infection status. Results are presented in Table 2. Relapse after treatment, history of irregular treatment, cigarette smoking, drinking alcohol and being a truck driver were found to be statistically associated with MDR-TB/HIV positivity. Other factors showed no statistical association with MDR-TB/HIV infection status.
Independent demographic and clinical determinants of MDR-TB
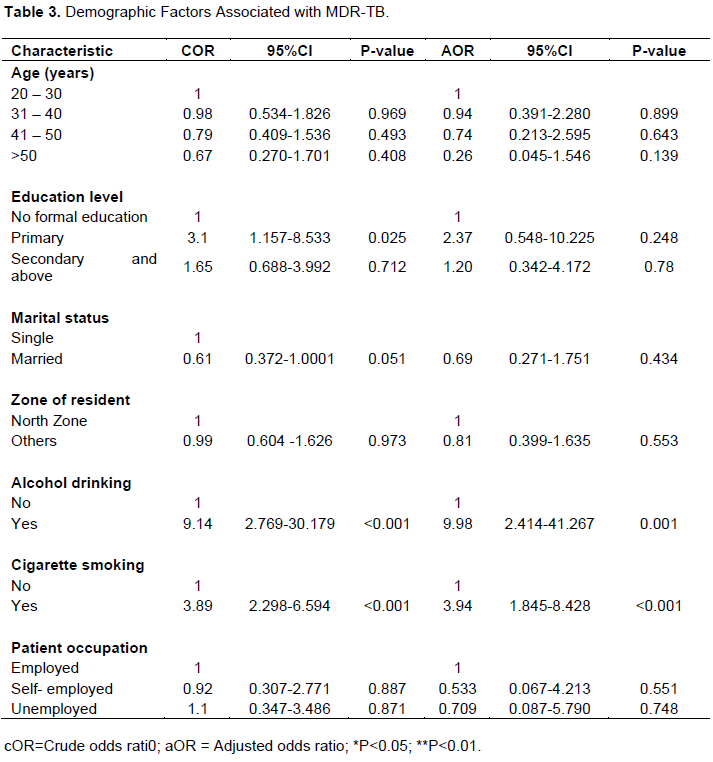
Demographic factors associated with MDR-TB
In attempt to determine risk factors for MDR-TB, data was fitted in logistic regression model. In crude analysis, alcohol drinking and cigarette smoking were found to be significant factors associated with MDR-TB (Table 3). In the multivariate logistic regression analysis, it was revealed that, the odds of having MDR-TB among patients who were cigarette smokers at least once a day were nearly 4 times the odds among patients who never smoke (aOR= 3.94; 95%CI:1.845-8.428, P<0.001), inferring that, cigarette smoking increases the chances of having MDR-TB by about 4 times. Likewise, MDR-TB patients who were alcohol drinkers to any extent were about ten times more likely to have MDR-TB than those who don’t drink alcohol at all (aOR= 9.98: 95%CI; 2.414-41.267, P=0.001). When clinical/treatment history variables were analyzed for their association with MDR-TB, it was observed that being HIV positive strongly increased the likelihood to have MDR-TB compared to their HIV negative counterparts (aOR= 2266.0: 95% CI; 407.5-2599.8, P<0.001). Compared to treatment failure, Relapse and non-adherence were found to be strong predictors for MDR-TB (aOR = 64.22: (95% CI; 12.786-322.507) P=0.001), and (aOR = 37.44: (95% CI; 3.895-359.836, P=0.002), respectively. History of irregular treatment in the intensive phase and smear culture grade were both not found to be predictors for MDR-TB. Results for this analysis are presented in Tables 3 and 4.
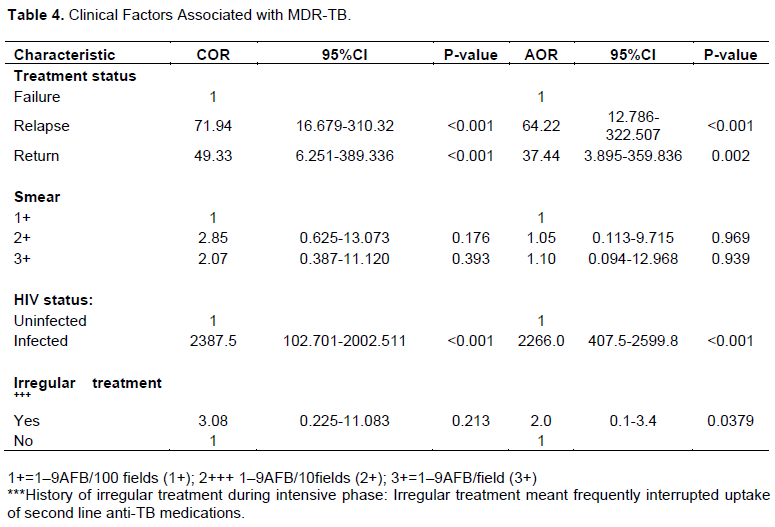
Clinical factors associated with MDR-TB
Table 4 shows results of clinical determinants of development of MDR-TB. Relapse (aOR= 64.22: 95%CI; 12.786-322.507, P=0.001), Return for treatment (aOR= 37.44: 95%CI; 3.895-359.836, P=0.002), being HIV positive (aOR=22.66: 95%CI; 407.5-2599.8, P=0.001), and irregular treatment (aOR= 2.0: 95%CI; 0.1-3.4, P=0.038) were factors that determined development of MDR-TB.
DISCUSSION
Multidrug-resistant tuberculosis (MDR-TB) is an increasing public health challenge, resulting from an array of factors. The most important factors have been described as a mixture of physician error and patient non-compliance in the course of treatment of susceptible TB (Ormerod, 2005). The burden of MDR-TB is in higher in resource-poor countries due to many factors including the weak health delivery systems (Kidenya et al., 2018). The emergency of Human immunodeficiency virus (HIV) has enhanced development of MDR-TB and extensive drug resistant tuberculosis (XDRTB), greatly complicating TB control (Meaza et al., 2017).
While several studies have shown previous TB treatment to be a strong risk factor for development of MDR-TB (Vashakidze et al., 2009; Schreiber et al., 2009), scarce data exist to show the relative contribution of this factor and other risk factors in settings with high HIV prevalence. It has previously been observed that risk factors for drug-resistant TB are likely to be different in low-resource, high HIV prevalence settings as a result of increased risk of transmission in congregate settings (Escombe et al., 2008), more rapid progression to active disease after infection (Selwyn et al., 2019), and higher mortality from TB/HIV co-infection (Gandhi et al., 2010; Brust et al., 2010). In this study, we intended to assess demographic and clinical determinants of development of MDR-TB among HIV Infected Patients in Tanzania. HIV infection, history of irregular treatment, Relapse and return, cigarette smoking, and drinking alcohol were the most important determinants for development of MDR-TB in this study. Our findings are similar to findings from other studies conducted elsewhere that showed an increased risk of acquiring MDR-TB among patients living with HIV (Mesfin et al., 2014; Gandhi et al., 2010; Mai et al., 2006; Wells et al., 2007).
Despite the fact that the likelihood for the presence of risk factors common to both HIV-positive and MDR-TB patients has not been adequately explored, in a study conducted in Moldova, a positive association between MDR-TB and HIV infection was observed among new TB patients even after adjustment for potential confounders (Jenkins et al., 2013). This observation of a positive association between MDR-TB and HIV infection underscores the need to improve on current approaches to diagnosis and treatment of the two infections. Early diagnosis of HIV allows for early initiation of ART while early diagnosis of MDR-TB which allows timely and improved access to resistance testing for TB/HIV co-infected patients and timely initiation on second-line anti-tuberculosis medications. These approaches are critical in increasing the likelihood of treatment success and survival among MDR-TB/HIV co-infected populations.
It is understood that, among other factors, the occurrence of MDR-TB is mainly attributable to human error (Sharma and Mohan, 2006). In this study, we have observed strong relationships between MDR-TB and history of irregular treatment and relapse. The principal patient-related factor that predicts the occurrence of MDR-TB is non-adherence to treatment (“Participants’ Manual: national comprehensive tuberculosis, leprosy and TB/HIV training for general health workers.,” 2011). Patient adherence to treatment is multi-factorial and involves individual patient factors, provider factors, and community factors (Deshmukh et al., 2015). In addition, MDR-TB occurs mostly in relation to improper treatment of drug-susceptible TB (Hirpa et al., 2013). One of the patient related factors for non-adherence has been reported as alcohol abuse. A study by Deshmukh and colleagues reported alcohol abuse to result not only to missed MDR-TB treatment doses and other scheduled appointments, but also in patients being unreceptive to counseling and treatment adherence messages by providers (Deshmukh et al., 2015). Relapse is reported as significant predictor of MDR-TB in this study. There is a clear link between non adherence and relapse in which case the former leads to treatment failure and hence relapse.
While it is understood that high rates of MDR-TB among newly diagnosed patients suggest problems with TB control in the past, high rates of MDR-TB among relapse cases is suggestive of existing problems in the TB control program including suboptimal treatment regimens (Meaza et al., 2017). Inadequate management of TB cases, poor mechanisms to ensure adherence to treatment and shortage or absence of anti-TB drugs are factors previously reported to contribute to the high rates of drug-resistant TB (Nino et al., 2009; Weinstock et al., 2001; Zalesky et al., 1999). It is therefore urgent that responsible ministries of health in High TB burden countries undertake rigorous restructuring of the systems and elements for improving diagnosis, management and monitoring of TB treatment to reduce the chances of progression to MDR-TB. Tobacco smoke has been reported to have various effects on the lung in both animal and human studies. More specifically, smoking has been associated with changes in pulmonary macrophages and lymphocytes that play a major role in cellular immunity. Tobacco smoking is known to compromise treatment efficacy by lowering immune mechanisms, hence compromising drug effectiveness and recovery (Carnevali et al., 2003; Leung et al, 2003). In line with our findings, other reports, including a report from the WHO, indicate that the use of alcohol increases the risk of developing MDR-TB due to poor adherence to treatment, increased risk of adverse drug effects and impaired immune responses due to oxidative stress (Liang et al., 2015; WHO, 2014a, c, 2018).
Patients involved in this study were those who failed treatment in primary and secondary health care facilities and provisionally diagnosed and referred as MDR-TB cases. Despite efforts being made by the Tanzanian Ministry of health to improve management of TB cases in every district and regional hospital, the cure rate remains a challenge partly because medications used in the treatment of MDR-TB take a long time of at least 20 months and are associated with a wide range of side effects, which is likely to compromise adherence to MDR-TB drugs. Congruent to findings in other studies, relapse could be due to many factors including delayed diagnosis, poor adherence with treatment, treatment default and factors related to development of drug resistance (Deiss et al., 2009; Duarte et al., 2011; Dye and Williams, 2000; World Health Organization, 2011). These factors underscore the importance of consolidated and sustained TB control programs.
CONCLUSION
This study report demographic and clinical determinants for development of MDR-TB in a Tanzanian setting. The factors associated with development of MDR-TB are HIV infection, TB relapse, history of irregular treatment, cigarette smoking, alcohol abuse, treatment failure (return) as the most important independent factors that contributes to development of MDR-TB. These determinants affect the development from non MDR-TB to MDR-TB through different mechanisms that either compromise adherence or reduce host immune mechanisms. From our findings, consolidated and integrated TB/HIV control programs, including establishing strong diagnostic and drug delivery systems, patient management systems that improve adherence (DOTS), and TB resistance surveillance systems are recommended.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors appreciate the Kilimanjaro Christian Medical University College (KCMUCo’s) and Kibong’oto Infectious Diseases Hospital leadership for granting permissions to conduct this study and also the statistical advice provided by Gibson Kapanda.
REFERENCES
|
Atif M, Bashir A, Ahmad N, Fatima RK, Saba S, Scahill S (2017). Predictors of unsuccessful interim treatment outcomes of multidrug resistant tuberculosis patients. BMC Infectious Diseases 17(1):655. |
|
|
Breen R, Smith CBH (2004). Paradoxical Reactions during Tuberculosis Treatment in Patients with and without HIV Co-Infection. Thorax 59:704-707. |
|
|
Brust JC, Gandhi NR, Carrara H, Osburn G, Padayatchi N (2010). High treatment failure and default rates for patients with multidrug-resistant tuberculosis in KwaZulu-Natal, South Africa, 2000-2003. The International Journal of Tuberculosis and Lung Disease 14(4):413-419. |
|
|
Chattu VVK, Kumaryy S (2015). TB-HIV co-infection and MDR-TB : major concerns for post 2015 global agenda Editorial TB-HIV Co-Infection and MDR-TB : Major Concerns for Post 2015 Global Agenda. International Journal of Current Microbiology and Applied Sciences 4:1-5. |
|
|
Carnevali S, Petruzzelli S, Longoni B, Vanacore R, Barale R, Cipollini M, Scatena F, Paggiaro P, Celi A, Giuntini C (2003). Cigarette smoke extract induces oxidative stress and apoptosis in human lung fibroblasts. American Journal of Physiology-Lung Cellular and Molecular Physiology 284:955-963. |
|
|
Deiss R, Rodwell T, Garfein R (2009). Tuberculosis and Drug Use: Review and Update. Clinical Infectious Diseases 48:72-82. |
|
|
Deshmukh RD, Dhande DJ, Sachdeva KS, Sreenivas A, Kumar AMV, Satyanarayana S, Parmar M, Moonan PK, Lo TQ (2015). Patient and Provider Reported Reasons for Lost to Follow Up in MDR-TB Treatment: A Qualitative Study from a Drug Resistant TB Centre in India. PLoS ONE 10(8):135802. |
|
|
Desissa F, Workineh T, Beyene T (2018). Risk factors for the occurrence of multidrug-resistant tuberculosis among patients undergoing multidrug-resistant tuberculosis treatment in East Shoa. Public Health, pp. 1-6. |
|
|
Duarte R, Santos A, Mota M, Carvalho A, Marques A, Barros H (2011). Involving Community Partners in the Management of Tuberculosis among Drug Users. Public Health 125: 60-62. |
|
|
Dye C, Williams BG (2000). Criteria for the control of drug-resistant tuberculosis. Proceedings of the National Academy of Sciences, 97(14): 8180-8185. |
|
|
Eklund D (2013). Mycobacterium tuberculosis and the human macrophage - shifting the balance through inflammasome activation (Issue 1372). |
|
|
Escombe AR, Moore DA, Gilman RH, Pan W, Navincopa M, Ticona E, Martínez C, Caviedes L, Sheen P, Gonzalez A, Noakes CJ (2008). The infectiousness of tuberculosis patients coinfected with HIV. PLoS Medicine 5:9. |
|
|
Gandhi NR, Shah NS, Andrews JR, Vella V, Moll AP, Scott M, Weissman D, Marra C, Lalloo UG, Friedland GH, Ferry T (2010). HIV Coinfection in Multidrug- and Extensively Drug-Resistant Tuberculosis Results in High Early Mortality. American Journal of Respiratory and Critical Care Medicine 181(20):80-86. |
|
|
Gandhi NR, Shah NS, Andrews JR, Vella V, Moll AP, Scott M, Weissman D, Marra C, Lalloo UG, Friedland GH (2010). HIV coinfection in multidrug-and extensively drug-resistant tuberculosis results in high early mortality. American Journal of Respiratory and Critical Care Medicine 181(1): 80-86. |
|
|
Hainlifescience (2015). Genotype MTBDR, pp. 1-10. |
|
|
Hirpa S, Medihn G, Girma BE (2013). Determinants of multi drug- resistant tuberculosis in patients who underwent first-line treatment Addis Ababa: A case-control study. BMC Public Health 13:2-9. |
|
|
Ioannidis P, Papaventsis D, Karabela S, Nikolaou S, Panagi M, Raftopoulou E, Konstantinidou E, Marinou I, Kanavaki S (2011). Cepheid GeneXpert MTB/RIF Assay for Mycobacterium tuberculosis Detection and Rifampin Resistance Identification in Patients with Substantial Clinical Indications of Tuberculosis and Smear-Negative Microscopy Results. Journal of Clinical Microbiology 49(8):3068-3070. |
|
|
Ismail N, Ismail F, Omar SV, Blows L, Gardee Y, Koornhof H, Onyebujoh PC (2018). Drug resistant tuberculosis in Africa: Current status, gaps and opportunities. African Journal of Laboratory Medicine 7(2):1-11. |
|
|
Jenkins HE, Plesca V, Ciobanu A, Crudu V, Galusca I, Soltan V, Serbulenco A, Zignol M, Dadu A, Dara M (2013). Assessing spatial heterogeneity of MDR-TB in a high burden country. European Respiratory Journal 42(5):1-25. |
|
|
Kent PI, Kubica GP (1985). Public health Mycobacteriology: A guide for the level III laboratory. Atlanta: Center for disease control (1st Edition). CDC. |
|
|
Kibret KT, Moges Y, Memiah P, Biadgilign S (2017). Treatment outcomes for multidrug-resistant tuberculosis under DOTS-Plus: A systematic review and meta-analysis of published studies. Infectious Diseases of Poverty, pp. 1-8. |
|
|
Kidenya BR, Webster LE, Behan S, Kabangila R, Peck RN, Mshana SE, Fitzgerald DW (2014). Epidemiology and genetic diversity of multidrug-resistant tuberculosis in East Africa. Tuberculosis 94(1):1-7. |
|
|
Kidenya B, Webster L, Behan L, Kabangila R, Mshana S, Oksana O (2014). Epidemiology and genetic diversity of multidrug-resistant tuberculosis in East Africa. Tuberculosis (Edinb) 94(1):675-680. |
|
|
Leung CC, Yew WW, Chan CK, Tam, CM, Lam CW, Chang KC, Chau CH, Lau KS, Law WS (2003). Smoking and tuberculosis in Hong Kong. International Journal of Tuberculosis and Lung Disease 7:980-986. |
|
|
Liang Y, Harris FL, LAS B (2015). Alcohol Induced Mitochondrial Oxidative Stress and Alveolar Macrophage Dysfunction. BioMed Research International, pp. 1-14. |
|
|
Meaza A, Kebede A, Yaregal Z, Dagne Z, Moga S, Yenew B, et al. (2017). Evaluation of genotype MTBDR plus Ver 2 . 0 line probe assay for the detection of MDR-TB in smear positive and negative sputum samples. BMC Infectious Diseases, P. 8. |
|
|
Mesfin YM, Hailemariam D, Biadgilign S, Biadglign S, Kibret KT (2014). Association between HIV/AIDS and multi-drug resistance tuberculosis: A systematic review and meta-analysis. PloS ONE 9(1):e82235. |
|
|
Ministry of Health, Community development, Gender (2018). TB Prevalence in Tanzania. The National Tuberculosis and Leprosy Programme |
|
|
Monadil HA, Alian AA, Mohamed AH, Dan K, Godman B (2019). Predictors of Multidrug-Resistant Tuberculosis. Antibiotics 8(90):1-11. |
|
|
Mulu W, Mekonnen D, Yimer M, Admassu A, Abera B (2015). Risk factors for multidrug resistant tuberculosis patients in Amhara National Regional State. African Journal of Health Sciences 15(2):368-377. |
|
|
Nino M, Ekaterina Z, Natalia V, Ekaterina K, Henry MB, George K, Carlos del R, Archil S, Kourbatova, Thea Jibuti, Natalia Shubladze TK (2009). High Prevalence of Multidrug-Resistant Tuberculosis in Georgia. International Journal of Infectious Diseases 12(6):635-644. |
|
|
Ormerod LP (2005). Multidrug-resistant tuberculosis (MDR-TB): epidemiology, prevention and treatment. British Medical Bulletin 73(1):17-24. |
|
|
Participants' Manual: National comprehensive tuberculosis, leprosy and TB/HIV training for general health workers (2011). Federal Ministry of Health of Ethiopia, pp. 1-233. |
|
|
Mai TQ, Martinez E, Menon R, Van Anh NT, Hien NT, Marais BJ, Sintchenko V (2006). Drug resistance among smear-positive tuberculosis patients in Ho Chi Minh City, Vietnam. International Journal of Tuberculosis and Lung Disease 10:160-166. |
|
|
Ryu YJ (2015). Diagnosis of Pulmonary Tuberculosis: Recent Advances and Diagnostic Algorithms. Tuberculosis and Respiratory Diseases 78(2):64. |
|
|
Schreiber YS, Herrera AF, Wilson D, Wallengren K, Draper R, Muller J, Dawood H, Doucette S, Cameron DW, Alvarez GG (2009). Tuberculosis retreatment category predicts resistance in hospitalized retreatment patients in a high HIV prevalence area. The International Journal of Tuberculosis and Lung Disease 13(10):1274-1280. |
|
|
Selwyn PA, Hartel D, Lewis VA, Schoenbaum EE, Vermund SH, Klein RS, Walker AT, Friedland GH (2019). A prospective study of the risk of tuberculosis among intravenous drug users with human immunodeficiency virus infection. New England Journal of Medicine 320(9):545-550. |
|
|
Seyoum B, Demissie M, Worku A, Bekele S, Aseffa A (2014). Prevalence and Drug Resistance Patterns of Mycobacterium tuberculosis among New Smear Positive Pulmonary Tuberculosis Patients in Eastern Ethiopia. Tuberculosis Research and Treatment pp. 1-7. |
|
|
Sharma SK, Mohan A (2006). Multidrug-resistant tuberculosis: A menace that threatens to destabilize tuberculosis control. Chest 130:261-272. |
|
|
Shimeles E, Enquselassie F, Tilahun M, Mekonnen A (2019). Risk Factors for Multidrug-Resistant Tuberculosis and Characteristics of Cases : A Case-Control Study of Patients Attending ALERT General Hospital in Addis Ababa, Ethiopia. Journal of Respiratory Disease 9:1-17. |
|
|
Steingart KR, Henry M, Ng V, Hopewell PC, Ramsay A, Cunningham J, Urbanczik R, Perkins M (2006). Fluorescence versus conventional sputum smear microscopy for tuberculosis: A systematic review. Lancet 6:570-581. |
|
|
Stop TB Partneship. (2018). Global Plan to End TB: 2018-2022, pp. 1-32. |
|
|
Tamary HL, Isack L, Edson M, Kajiru GK (2019). Predictors of Treatment Outcomes among Multidrug Resistant Tuberculosis Patients in Tanzania. Hindawi Tuberculosis Research and Treatment, pp. 1-10. |
|
|
Vashakidze L, Salakaia A, Shubladze N, Cynamon M, Barbakadze K, Kikvidze M, Papitashvili L, Nonikashvili M, Solomonia N, Bejanishvili N, Khurtsilava I (2009). Prevalence and risk factors for drug resistance among hospitalized tuberculosis patients in Georgia. The International Journal of Tuberculosis and Lung Disease 13(9):1148-1153. |
|
|
Wahab F, Ashraf S, Khan N, Anwar RAM (2009). Risk factors for multidrug resistant tuberculosis in patients at Tertiary Care Hospital, Peshawar. Journal of the College of Physicians and Surgeons Pakistan 19:162-164. |
|
|
Weinstock DM, Hahn O, Wittkamp M, Sepkowitz KA, Khechinashvili GBH (2001). Risk for tuberculosis infection among internally displaced persons in the Republic of Georgia. International Journal of Tuberculosis and Lung Disease 5(2):164-269. |
|
|
Wells DC, Peter CJ, Nelson LJ, Laserson KF, Holtz TH, Finlay A, Castro KG, Weyer K (2007). HIV infection and multidrug- resistant tuberculosis-the perfect storm. Journal of Infectious Diseases 196:S86-S88. |
|
|
World Health Organization (2016). World Health Organization. Multidrug-resistant tuberculosis (MDR-TB) 2016 Update. Geneva. |
|
|
World Health Organization (2003). Adherence to Long - Termtherapies pp. 1-16. |
|
|
World Health Organization (2012a). Global Tuberculosis Report. |
|
|
World Health Organization (2012b). Report on MDR-TB (Issue 1). |
|
|
World Health Organization (2014a). Global status report on alcohol and health. |
|
|
World Health Organization (2014b). Global tuberculosis report pp. 1-118. |
|
|
World Health Organization (2014c). World Health Organization. Antimicrobial resistance: global report on surveillance. |
|
|
World Health Organization (2015). End TB strategy pp. 1-20. |
|
|
World Health Organization (2017). Global Tuberculosis. |
|
|
World Health Organization (2018). Global tuberculosis report. |
|
|
World Health Organization (2011). Guidelines for the programmatic management of Multidrug-resistant Tuberculosis. |
|
|
World Health Organization (2014). Companion handbook. |
|
|
World Health Organization (2012c) . Burundi tuberculosis profile 2012. Geneva, Switzerland: WHO; 2012. |
|
|
World Health Organization (2012d). Kenya tuberculosis profile 2012. Geneva, Switzerland: WHO; 2012. |
|
|
World Health Organization (2012e). Rwanda tuberculosis profile 2012. Geneva, Switzerland: WHO; 2012. |
|
|
World Health Organization (2012f). Tanzania tuberculosis profile 2012. Geneva, Switzerland: WHO; 2012. |
|
|
World Health Organization (2012g). Uganda tuberculosis profile 2012. Geneva, Switzerland: WHO; 2012. |
|
|
Zalesky R, Abdullajev F, Khechinashvili G, Safarian M, Madaras T, Grzemska, Englund E, Dittmann S, Raviglione M (1999). Tuberculosis control in the Caucasus: Successes and constraints in DOTS implementation. International Journal of Tuberculosis and Lung Disease 3(5):394-401. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


