ABSTRACT
The aim of this study is to investigate the impact of psychological counselling on victims with Posttraumatic Stress Disorder (PTSD) from the Rana Plaza tragedy. Data was collected from two different groups using the Impact of Event Scale translated and validated in Bengali. Participants of one group consist of 50 who received life skills training and the other group of 71 who had no such training. PTSD was significantly reduced in both groups of the participants after receiving 6 consecutive sessions of psychological counselling, t(120) = 17.11, p<.05. Statistical significance was observed in the effectiveness of counselling between the two groups indicating the impact of counselling is enhanced among the individuals with life skill training. Significant outcome was observed in the impact of counselling when considering factors such as, educational level, and their profession, skilled or unskilled. Moreover, present employment status had a significant impact. Financial aid was beneficial to certain extent without any doubt, hence the results of this research helped to understand the effectiveness of psychological treatment and the necessity of providing such support alongside life skills.
Key words: Counselling, posttraumatic stress disorder, disaster, survivors.
Posttraumatic stress disorder (PTSD) has been a major health concern around the world. According to the American Psychological Association (2015), “posttraumatic stress disorder or PTSD is an anxiety problem that develops in some people after extremely traumatic events, such as combat, crime, an accident or natural disaster”.
PTSD could be after-effect of war, rape, abuse, accidents, witnessing death or injury of others and so on. According to The Diagnostic and Statistical Manual of Mental Disorders-V (5th ed.; DSM–5; American Psychiatric Association, 2013), a person directly experiencing or witnessing an event involving actual or threatened death or sexual violation and such disturbance affects the individual’s ability to engage in social interactions, work and other areas of functioning. When describing traumatic events, it has been mentioned that trauma is often a very personal thing because what traumatizes one person may not have the same significance to others (Posttraumatic Stress Disorder Patient Treatment Manual, 2010). As the personality of every individual, their beliefs, values and previous experiences, especially related to other traumatic events of their lives, are different; therefore the reaction of people towards an event may vary (Posttraumatic Stress Disorder Patient Treatment Manual, 2010). However, common reactions to traumatic events are intense fear, helplessness and horror.
On 24thApril, 2013, a disastrous event took place in Bangladesh, at a place named Savar, near the capital of the country. A building collapse in Savar, Bangladesh took approximately 1,134 lives and 2,515 people were left injured (The Guardian, 2015). Rana Plaza, a building housing several garments factories, caved in on a working day. A large number of people connected with the tragedy – those who witnessed or experienced the event, families and friends of the victims and the rescuers – were at high risk of developing PTSD. PTSD may develop after events such as a building collapse; victims and their family and friends, rescuers, or those simply watching are at high risk of suffering from PTSD (Di Santo, 2013).
PTSD has been identified as the most prevalent type of psychiatric morbidity after disasters (Yildiz and Göker, 2004). Even though the idea of posttraumatic stress disorder has a long history, the concept was much discussed only after the Vietnam War and it was included in DSM- III afterwards as “posttraumatic stress disorder” (Word Press, 2015). Generally, anywhere between 5 and 40% of trauma survivors may develop PTSD (PTSD Patient Treatment Manual, 2010).
PTSD is not simply a mental health concern; rather a concern connected to a number of factors like maintaining relationships, social and employment issues, etc. Sometimes they are triggered by their surroundings which remind them about their traumatic event which may cause to be isolated from others (National Council on Disability, 2009). Irritability, fear and anger grasp over rational decision making and other cognitive abilities (She Knows: Health and Wellness, 2015). Besides that, they face difficulty in concentrating on job tasks, related stress or maintain attendance. There are also other symptoms of PTSD that they face complexity while working with others and follow instruction (National Council on Disability, 2009). Researches also revealed that PTSD is positively associated with unemployment and over 60% companies of the United States prefer not to recruit someone with PTSD (Anderson, 2014).
Considering the severity of the harm caused by PTSD, numerous medical and psychological treatment options are offered; since PTSD has become a major worldwide health concern nowadays. Psychological treatment or combinations with medical treatments are available for the PTSD patients (Sidran Institute, 2015). Providing skills-based training is also very useful to help victims of PTSD to increase their employability and re-establish anormal active lifestyle (Precin, 2011). An individual with PTSD may receive psychological interventions and yet have to deal with critical social and environmental situations (Shea and Zlotnick, 2002).
Counselling and skills training were found equally significant in reducing PTSD and individuals who experienced trauma emphasized social support and skills as factors for personal growth after the trauma (Murray et al., 2005; Lekskes et al., 2007). Female victims of trauma as a result of childhood abuse reported major reduction in their PTSD after receiving skills training along with psychotherapy (Cloitre et al., 2002).
After the tragic event of Rana Plaza collapse, financial aid was received but the psychological injuries were yet to be healed. Not many research studies were available on the current mental health condition of the victims of Rana Plaza tragedy. One of the research reports included majority of the Rana Plaza survivors developed PTSD alongside physical injury (Hossain et al., 2013). Reports revealed that as after effects, victims seemed lost and lacked cognitive abilities such as decision-making and memory. Self-medication often with excessive antidepressants and even cases of suicide after major depressive episodes were also reported (Motlagh, 2013). A recent finding suggested that PTSD was present in 75.69% of the participants within a chosen population from the victims of the Rana Plaza tragedy (Fitch et al., 2015).
The aftermath of trauma can have a severe impact on the lives of the victims of PTSD and the ones around. It is evident from the prior discussion that psychotherapies and skills training are effective introducing PTSD. The purpose of this piece of research is to identify the effect of psychological counselling among the victims of the Rana Plaza tragedy.
The study further aimed to observe the two groups; one of the groups received a vocational skills training course after the tragic event, and the other group did not – to compare whether life skills training enhances the influence of psychological counselling. The researchers will also explore if factors such as education, job status, previous counselling advice, enhance the impact of counselling received by the participants.
Participants
Total number of participants was 121 who were victims, rescuers and family members of the Rana Plaza tragedy. Among them 80 females and 41 males took part in this study. They were selected using the purposive sample method. A list of victims was collected and those who lived nearby Savar, the area of disaster, were invited to participate. Those who came and gave consent from the available survivors were included in the study. Among them, 50 participants received vocational and micro business skills training prior to the study and they were taken as the “skill training group” in this research. Other 71 participants were the “no-skill training group” who did not have such prior training exposure.
Materials
The researchers used the Impact of Event Scale (IES-R) in order to measure the level of PTSD among the participants.
The impact of event scale
This scale is self-administered, developed by Weiss, D., revised in 2013. This scale was translated and validated by the Institute of Educational Development and BRAC University (IED – BU), 2014. This questionnaire could be applied on the adults after a traumatic event and has three subscales, intrusion, avoidance and hyper arousal. It is a 22 item Likert scale with 5 point response scale. The responses are ranged from; 0 = Not at all, 1 = Slightly, 2 = Moderately, 3 = Quite a bit and 4 = Extremely. Any score between 1 to 11 indicates that the individual does not have any symptoms of PTSD and no action is required therefore. An IES score between 12 to 32 indicates several symptoms of PTSD are present in the person and monitoring is required. A score equal to or greater than 33 indicates severe posttraumatic stress disorder (PTSD) for majority of the people and further assessment and treatment are required at this point. There is no specific cut off score. A total IES score of 33 or over from a theoretical maximum of 88 signifies the likely presence of PTSD. A demographic form was also filled in for each participant that included information like their name, sex, their level of academic education, if they were employed, if they had any existing skills and if they had received psychological counselling before etc.
Psychological counselling
Psychological counselling provided to the participants was a combined model including psychotherapeutic techniques like Cognitive-Behavioural Therapy (CBT), some techniques of psycho-traumatology, and Neuro-linguistic Programming (NLP). In total, 30 trainee counselling psychologists provided counselling to the participants – 10 trainee counselling psychologists for the training group and 20 for the non-training group. The psychologists all did their post-graduate specializations in counselling psychology and all the counsellors received two-day training on trauma counselling prior to counselling service delivery. The trainee counselling psychologists were under regular supervision.
Procedure
In order to accomplish the study, the researchers called the victims from the list and invited only those who live in or around the Savar area. Once the participants arrived, the researchers obtained some basic demographical information from them. Once they were done with answering the demographical questions, the researchers rated the IES-R scales based on the participants’ responses. Data from the non-training group was collected almost twenty months after the Rana Plaza tragedy, in early February 2015. A total of 108 survivors of the tragedy came for the first session and 71 participants, or, 65.74% of them completed the counselling sessions. These participants did not receive any prior training from any organization. The participants of the training group took part in the research almost eighteen months after the event, in late November, 2014. This group received vocational and micro business skills training from non-governmental organisation (NGO). Sixty participants were called by phone to take part in the study and among them, 50 (83.33%) showed up for the study. Pre-post methods were used to collect data on PTSD by administering IES-R. The researcher assisted the illiterate participants in filling up the self-rated IES-R scale.
Ethics and confidentiality
The research was conducted with the consent of the participants. The participants were assured about their confidentiality. Code numbers were used to protect the privacy of the participants. Also, the researchers stated to the participants that they could withdraw from the study at any time without any prejudice.
Descriptive statistics and test of significance were computed by using IBM SPSS 20. T-tests and ANOVA were done in order to observe any significant difference between the impacts of psychological counselling in reducing PTSD in general and among different study variables.
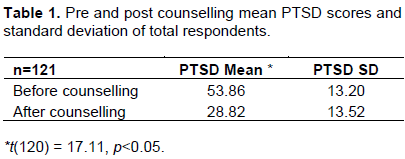
The pre and post counselling mean and standard deviation scores of PTSD of total respondents are presented in Table 1. A total score of 33 or above indicates the presence of PTSD among the respondents; table 1 clearly shows that all the respondents were experiencing a high level of PTSD before receiving counselling. The mean PTSD score of the respondents was 53.86 before receiving counselling service, which significantly decreased to 28.82 (t = 17.11, p<0.05) after receiving counselling. This shows the positive impact of counselling in reducing PTSD symptoms.
Demographic data indicates considerable variation among the respondents on the study variables to account for analysis of variance (Table 2). Impact of counselling for other study variables like gender, education, employment, type of profession were analyzed and presented in Tables 3 to 6.

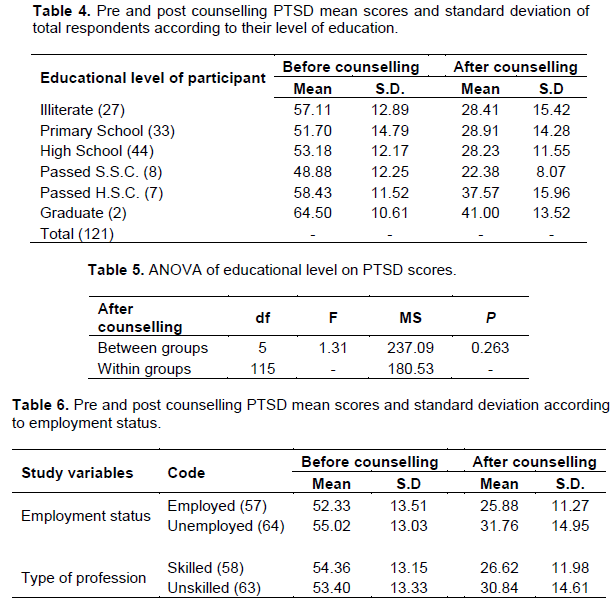
Table 3 shows the mean and standard deviation scores of males and females of both groups of respondents. The PTSD score of the male respondents was 54.10 the mean score decreased to half (27.95) of it after the counselling service was provided. The mean PTSD score of the female respondents was also decreased mean score 53.74 to 29.26 after receiving counselling service. When observing the male and female respondents separately, no significant difference was found in the before counselling was provided, t(119)= .14, p>0.05 and also no significant differences were observed in t-test scores after the respondents received counselling, t(119)= -.50, p>0.05 . The findings imply that both male and female were equally benefited by counselling in reducing PTSD. Table 4 has shown that level of PTSD was not depended on their education level. For all the educational groups PTSD score has dropped. ANOVA was used to test the significance between groups post counselling PTSD scores (Table 5).There was no significant difference in the impact of counselling when considering the educational level of respondents (F (5, 115)] = 1.31, p= 0.26) therefore education does not significantly enhance the impact of counselling.
Table 6 shows that the number of respondents who were employed during the time of the data collection was 57. Their mean PTSD score before receiving counselling was 52.33 and it decreased to 25.88 after receiving counselling. The S.D. scores before and after counselling were 13.51 and 11.27 respectively. The unemployed respondents (64 in total) had a mean PTSD score of 55.02 which went down to 31.76 and the S.D. scores were 13.03 and 14.95 before and after counselling respectively.
Further according to type of profession, it was found that 63 respondents were in unskilled job and 58 respondents were in skilled job. The mean PTSD score of the skilled respondents was 54.36 before they received counselling and it was less than half (26.62) after receiving counselling. PTSD score of the unskilled respondents before receiving counselling was 53.40 and it decreased to 30.84 after counselling was received. The standard deviation scores of the skilled respondents before and after receiving counselling were 13.15 and 11.98 and for the unskilled respondents, it was 13.33 and 14.61respectively before and after receiving counselling. No significant outcome was found for type of profession; before counselling sessions; t= -.40, p>.05 and after the sessions, t = 1.73, p>0.05 (Table 6).
However, significant outcome was found when considering the current employment condition of the respondents. Even though the outcome was not significant before they received the counselling service, t (117) = 1.10, p>0.50 post–test results were significant: t(117) = 2.41, p< 0.05. This indicates that counselling was more effective for those who were currently employed than their unemployed counterpart (Table 6).
After the Rana Plaza tragedy, different organizations provided mental health advice to the victims and this was considered in this piece of research. Among 121 respondents in total, 80 respondents had exposure to such mental health advice previously and 41 of them did not (Table 7).

The PTSD score of those having prior exposure was 54.26 before the counselling sessions and the score went down to 28.61 after the sessions were completed. The S.D. scores were 12.63 and 13.61, before and after the counselling sessions. The mean PTSD score of the other respondents, who had no prior exposure of mental health advice, was 53.07 and the score dropped to 29.22 after the counselling sessions. S.D scores were 14.38 (before counselling) and 13.54 (after counselling sessions). No significant outcome was observed for prior exposure of mental health: before counselling sessions, t (119) = -0.47, p>.05 and after the sessions t(119) = .23, p>0.05. This implies that counselling provided during this study was effective without any confounding effect of prior exposure to mental health advice. No significant difference among the groups at pre-counselling PTSD scores also indicate the significance of structured counselling help to reduce PTSD symptoms (Table 7).
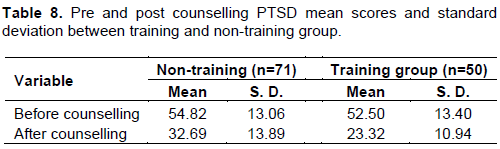
Table 8 shows that non-training group had a mean PTSD score of 54.82 before receiving counselling, which declined to 32.69 after counselling. The standard deviation scores before and after counselling were 13.06 and 13.89 respectively. The PTSD score of the training group was 52.50 before the counselling sessions and the S.D was 13.40.
The mean PTSD score went down to 23.32 and the S.D. was 10.94 after the counselling was received by the respondents of this group. No significant difference was found before receiving counselling between the two groups, t(119) = 0.95, p>.05. Significant difference was found among the two groups after receiving counselling, t(119) = 3.10, p< 0.05 indicating that both the groups were benefited yet the group who received social and business skills training were able to apply the counselling more in their lives (Table 8).
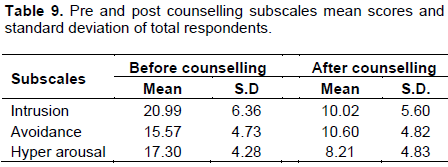
The mean score on the intrusion, avoidance and hyper arousal scale of PTSD was 20.99, 15.57 and 17.30 respectively before counselling was provided and the score was reduced in all the subscales after receiving counselling. Paired sample t-tests were conducted to identify any significant difference in the subscales. Significant differences were found in all the three subscales: Intrusion scale, t(120) = 17.02, p<0.05; Avoidance scale, t(120) = 8.63, p<0.05 and on Hyper arousal scale, t(120) = 17.94, p<0.05. This indicates positive impact of counselling in reducing PTSD symptoms (Table 9).
In order to explore the influence of training on the effectiveness of counselling, mean scores of non-skill training group and skill training group were compared and findings are presented in table 10 to 11. Training group were those who had received social and business skills training prior to study and no- skill training group were those who did not receive any such training (Table 10).
The mean score of intrusion, avoidance and hyper arousal scale in the non-training group was 21.46, 15.63 and 17.72 consecutively and after receiving counselling, the score of this subscale went down to 11.48, 12.11 and 9.10 accordingly. It is indicating that counselling had an impact (Table 10).
The mean score of intrusion scale in the group that received skills training was 20.32 and the standard deviation was 6.84. After receiving counselling, the scores of the intrusion subscale decreased to 7.94 and 4.50 respectively on mean and S.D. The mean score was 15.48 and the S.D. score was 4.13 on the avoidance scale. After counselling was provided, the scores on the avoidance scale fell to 8.44 (mean) and 3.95 (S.D.). The mean score of the hyper arousal scale was 16.70 with a standard deviation of 4.40 before receiving counselling, and after the training group receiving counselling, the mean score was noticeably lower; 6.94 with an S.D. score of 3.86 (Table 11).
A t-test was run in order to identify any statistical significant of outcomes. There was no significant outcome in the subscales before counselling was received. Intrusion scale, t(119) = .98, p>0.05; Avoidance scale, t(119) = .17, p>0.05 and on Hyper arousal scale, t(119) = 1.29, p>0.05. However, significant results were found between the training and non-training groups after the counselling service was provided to the respondents. Intrusion scale, t(119) = 3.59, p<.05; Avoidance scale, t(119) = 4.44, p<0.05 and on Hyper arousal scale, t(120) = 2.45, p<0.05. The findings indicate greater impact of counselling in reducing all the PTSD symptoms in skill training group than the no-skill training group.
The present study highlighted the positive impact of psychological counselling on PTSD symptoms of victims from the Rana Plaza tragedy. The impact of counselling was statistically significant in all aspects of PTSD. Statistics clearly indicated that the participants immensely and intensely benefited from the psychological counselling sessions that they received. Significant statistical difference was found in reducing PTSD among all the participants from both groups after receiving counselling and also for all the three subscales (Tables 1 and 9). This finding supports previous studies which demonstrate the effectiveness of psychological treatment on PTSD victims (Ehlers et al., 2005; Bisson et al., 2007; Foa et al., 1999; Etten et al., 1998).
The moderating impact of training on enhancing the effect of counselling was also observed. The second hypothesis was established as significant difference (Tables 8, and 10 to11) was found between the two groups, received training or not, after receiving counselling. It indicates that participants who have undergone life skills training are more likely to benefit from psychological counselling than those who have not. This is in accord with previous literature identifying that psychological treatment and other support should be provided hand in hand (Ellison et al., 2012). Previous researchers also argued that psychological treatment or skills training are much effective when received together, which supports the outcome of the current study (Cloitre et al., 2002; Shea and Zlotnick, 2002; Precin, 2011). Previous findings suggest that a lower level of education is major risk factor of PTSD, and unemployment which leads to a lower economic status could be another factor which increases PTSD (Halligan and Yehuda, 2000; Engelhard, Van Den Hout and Schouten, 2006).
The researchers explored the effect of education and employment status on effectiveness of counselling. Education and type of profession did not have any significant effect (Tables 4 to 6), however current employment status enhanced the impact of counselling among the respondents (Table 6).This is noteworthy because economic security is an important factor for sense of life success; thereby contributing to satisfaction and wellbeing on the whole (WHO, 2011; Anderson, 2014).
Another vital finding is that focused counselling has greater impact in reducing PTSD symptoms. After Rana Plaza tragedy, international and national organizations offered funds and support to improve conditions in the garments sector, in general (Duncan and Greening, 2014).
However, it is easily noticeable from the results of the present study that almost two years after the disaster, they have received financial aid but their psychological injuries were in need to heal. This piece of research indicates that psychological counselling could effectively reduce the trauma of the victims of the Rana Plaza Tragedy. Especially if skills training and psychological interventions could be combined, the impact will be strong and positive.
This study was conducted on survivors living in or around Savar. Many victims left Savar and Dhaka for the countryside, and their mental and physical health condition remains unnoticed. The results of this research can help and guide future research studies in this area. It also emphasize on increase awareness and willingness to offer and access counselling service to improve the condition of the victims of disaster.
The authors have not declared any conflict of interests.
REFERENCES
|
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders (5th Eds.). Washington, DC
|
|
|
|
Anderson P (2014). Unemployment Biggest Predictor of PTSD Symptom Severity. The Medscape Medical News.
|
|
|
|
Bisson IJ, Ehlers A, Matthews R, Pilling S, Richards D, Turner S (2007). Psychological Treatments for Chronic Post-traumatic Stress Disorder. Brit. J. Psyc. 190:97-104.
Crossref
|
|
|
|
Cloitre M, Konen K, Cohen L, Han H (2002). Skills Training in Affective and Interpersonal Regulation Followed by Exposure: A Phase-Based Treatment for PTSD Related to Childhood Abuse. J. Consult. Clin. Psychol. 70:1067-1074.
Crossref
|
|
|
|
Di Santo J (2013). Survivors of Traumatic Events May Experience PTSD. The Penn Current.
View
|
|
|
|
Duncan A, Greening J (2014). Rana Plaza: One Year On - UK aid to improve Bangladesh's Garment Sector. Government of UK.
View
|
|
|
|
Ehlers A, Clark MD, Hackmann A, McManus F, Fennell M (2005). Cognitive Therapy for Posttraumatic Stress Disorder: Development and Evaluation. Behav. Res.Therapy 43:413-431.
Crossref
|
|
|
|
Ellison ML, Mueller L, Smelson DA, Corrigan PW, Torres S, Rosalie A, Bokhour BG (2012). Supporting the Education Goals of Post-9/11 Veterans with Self-Reported PTSD Symptoms: A Needs Assessment. [Abstract]. Psychiatric Rehabilitation J. 35(3):207
Crossref
|
|
|
|
Engelhard IM, Van Den Hout MA, Schouten EG (2006).Neuroticism and Low Educational Level Predict the Risk of Posttraumatic Stress Disorder in Women After Miscarriage or Stillbirth. Gen. Hosp. Psychiat. 28(5):414-417.
Crossref
|
|
|
|
Etten V, Michelle L, Taylor S (1998). Comparative Efficacy of Treatments for Post-traumatic Stress Disorder: A Meta-Analysis. Clin. Psychol. Psychot. 5:126-144.
Crossref
|
|
|
|
Fitch T, Villanueva G, Quadir M, Alamgir H (2015). Prevalence and risk factors for PTSD in Injured Workers in Bangladesh: A Study of Surviving Workers from the Rana Plaza Building Collapse [Abstract].
Crossref
|
|
|
|
Foa BE, Dancu VC, Hembree AE, Jaycox JL, Meadows AE, Street PG (1999). A Comparison of Exposure Therapy, Stress Inoculation Training, and Their Combination for Reducing Posttraumatic Stress Disorder in Female Assault Victims. J. Consult. Clin. Psychol. 67(2):194-200.
Crossref
|
|
|
|
Halligan LS, Yehuda R (2000). Risk Factors for PTSD. The National Centre Post Traum. Stress Disord. 11(3):1-8.
|
|
|
|
Hossain IM, Nahar N, Nayan JM, Jahan A, Arafat YM (2013).Experience of Bangladeshi Occupational Therapists with "Rana Plaza Tragedy" Survivors: Recovery and Rehabilitation Phases of Disaster Management. World Fed. Occup. Ther. Bull. 68(1):14-19.
Crossref
|
|
|
|
Lekskes J, Van Hooren S, DeBeus J (2007). Appraisal of psychosocial interventions in Liberia. International Journal of Mental Health: Psychosocial Work & Counselling in Areas of Armed Conflict. 5(1):18-26.
Crossref
|
|
|
|
Motlagh J (2013). Bangladesh: Rana's Survivors. The Washington Post.
|
|
|
|
Murray R, Jane FS, Bronwyn M, Newbury J (2005). A Mixed-Method Analysis of Post-Trauma Outcomes: Trauma Severity and Social Support from a Psychotherapeutic Perspective. Can. J. Couns. 39(2):86-100.
|
|
|
|
National Council on Disability (2009). Post-Traumatic Stress Disorder (PTSD) and Traumatic Brain Injury (TBI).
View
|
|
|
|
Posttraumatic Stress Disorder Patient Treatment Manual (2010).
View
|
|
|
|
Precin P (2011). Return to Work After 9/11. Impact. World Sci. 38:3-11.
|
|
|
|
Shea MT, Zlotnick C (2002). Understanding and Treating PTSD: Introduction. J. Clin. Psychol. Session: Psychother. Pract. 58(8):869-875.
|
|
|
|
She Knows: Health and Wellness (2015). PTSD: How does trauma affect relationships?
View
|
|
|
|
Sidran Institute, Traumatic Stress Education & Advocacy (2015).
View
|
|
|
|
The Guardian (2015).
View
|
|
|
|
Weiss D (2013). The Impact of Event Scale – Revised. The Hartford Institute of Geriatric Nursing.
|
|
|
|
World Health Organization (WHO) (2011). Impact of economic crises on mental health. WHO, P 34.
|
|
|
|
Word Press. (2015). History of PTSD.
View
|
|
|
|
Yildiz M, Göker KM (2004). Psychiatric Comorbidity in Post-traumatic Stress Disorder among People Seeking Treatment after the Marmara Earthquake. Int. J. Mental Health 33(1):59-66.
|