ABSTRACT
Amputation is one of the most dreadful complications in diabetes. Diabetic amputees are at elevated risk of psychological distress due to their disability. Thus, the current study aimed to evaluate the effect of intensive counseling on psychological outcomes among type 2 diabetic patients undergoing amputation. The study was conducted among 62 consecutive patients admitted in the diabetic centre and who underwent an amputation. These patients were randomly assigned to a routine counseling group (RCG-26) and intensive counseling group (ICG-36). World Health Quality of Life (WHQOL) was administered individually to all the patients based on inclusion criteria. In the RCG group, psychological therapy was given before amputation. For patients in the ICG group, psychological therapy was given before and every day after amputation, till the day of discharge. WHQOL questionnaire scores together with the demographic details were also recorded accordingly. The finding highlighted that the overall quality of the life improves in ICG group in both BKA and Toe amputation, as compared to the RCG group. ICG has better impact on QOL than RCG in amputation patients. Thus, intensive assessment and intervention has to be included as part of routine management among patients with diabetes when they undergo a surgical amputation.
Key words: Amputation, quality of life, psychological counseling, intensive counseling.
Patients with type 2 diabetes mellitus (T2DM) develop multiple complications such as retinopathy, nephropathy and neuropathy. Ulceration and amputation are the most important consequences in diabetic foot problem (Aalaa et al., 2012; Alavi et al., 2014; Cavanagh et al., 2005). About 4 to 10% of diabetic patients suffer from a foot ulcer (Lauterbach et al., 2010; CDC, 2005, Abbas and Archibald 2005). In a recent review on the global variability in the incidence of lower extremity amputation, about around 10.5% of patients underwent major amputations due to diabetic foot. In diabetic patients, majority of the amputation are preceded by foot infection
(ADA, 1999; Moxey et al., 2011). Hence the development of foot infection is the result of combination of infection, peripheral vascular disease, poor foot care and peripheral neuropathy (Boulton, 1996; Boulton et al., 2005). In India, diabetic foot complication is the most common cause of hospitalization among diabetic patients due to various sociocultural practices like barefoot walking, lack of knowledge on diabetic foot complications, poor education and socioeconomic conditions (Vijay et al., 1997). In India, it is found that the prevalence of foot ulcers in diabetes patients is 3%, which is lesser as compared to western population (Pendsey, 1994). Severe diabetic foot infections leads to amputation, it is estimated that diabetes leads to more than 50% of amputation (Bengalorkar and Kumar 2011), among them, nearly 85% of the amputation in diabetic patients are due to foot ulcer (Pecoraro et al., 1990). The economic and emotional consequences for the patient and the family can be enormous (Shobhana et al., 2000). Prevalence of foot ulceration is high among rural population than urban population, despite receiving similar counseling. Further, rural patients were more prone to re ulceration and need surgical intervention (Viswanathan et al., 2006). It is also reported that 25% of amputees suffer from depression, feeling of insecurity, self consciousness and restlessness (Parkes, 1976). Amputation is triple threat which Involves loss of function, sensation and body image. It is a life changing event which affects almost all aspects of the individual life. Amputations are classified into major (above/below knee) and minor (removal of toes and feet) amputations.
Worldwide, about 50% of all non-traumatic lower extremity amputations are due to diabetes (Chaturvedi et al., 2001). The risk of lower extremity amputation is 15 to 46 times higher in diabetic patients than in persons who do not have diabetes (Lavery et al., 1996). It was shown that 15% of patients with diabetes develop a foot ulcer during their lifetime (Reiber, 1996). Due to DFU, in every 30 s one leg is being amputated among T2DM patients (Richard and Schuldiner, 2008). Amputation is a major cause of substantial emotional and physical distress. It also affects the financial condition and productivity of the amputee’s, which reflects on the quality of life (Vileikyte, 2001). An alteration in an individual's body image sets up a series of emotional, perceptual and psychological reactions and also noted that limb amputation could lead to a long-term disorder in the individual's body experience (Srivastava et al., 2010). Body image is the scheme of our own body, which forms in every one’s minds. It has direct connection with psychological adjustment; its dynamic construction was subject to revision and reconstruction in response to both internal and external stimuli. Readjusting to life after amputation is associated with depression, anxiety and disturbed body image (Rybarczyk et al., 1992). Apart from physical disability, amputees suffer from psychological and psychosocial problems and not much focus is given on the psychological state of the individual who undergoes amputation unless he or she presents with behavioral abnormalities.
Amputee’s experience post-traumatic stress disorder, due to traumatic injury (Breslau, 2001). The occurrence of physical disability presents the patient with not only physiological, but also a psychological disturbances. Role of psychological intervention will not only help in adaptation but will also enhance the well being in cases with amputation and it also plays a major role in adaptation among amputee (Desmond and Maclachlan, 2002). Intervention in the amputee’s distress would address the psychological part of the injury and healing which is paramount to physical rehabilitation (Schubert et al., 1992). Recent studies emphasized significant levels of anxiety, grief and social isolation found among people with amputations (Schubert et al., 1992; Frierson and Lippmann 1987; Thompson and Haran, 1984). When compared with single counseling session, multiple counseling sessions was effective in improving the rehabilitation of the amputees (Srivastava and Chaudhury, 2014). Perhaps, there is paucity of studies which focused on the effect of intensive counseling; hence an attempt has been made here to analyze the effectiveness of intensive psychological counseling with routine psychological counseling.
A hospital based prospective follow up study was conducted among 62 consecutive patients with T2DM who underwent amputation in a tertiary care hospital, North Chennai, India, during the study period (June 2015 to February 2016). The study population includes all patients aged 40-70 with diabetic duration more of than 2 years. Psychological details were recorded accordingly. Patients with T1DM, major psychiatric disorder were excluded from the study. The study was approved by institution ethics committee. Patients were assigned to intensive counseling group (ICG) or routine counseling group (RCG) based on randomization chart. Performa measuring the quality of life was administered individually before and after amputation for both the groups.
Group-1- routine counseling
In RCG group psychological counseling was given to the patients before amputation. Pre amputation stress level was assessed using WHQOL questionnaire and post amputation stress level was assessed using the same questionnaire on the day of discharge.
Group-2- intensive counseling
In ICG group psychological counseling was given before amputation. Pre-amputation stress level was administered using WHOQL questionnaire. They were followed up and post psychological counseling were given everyday till the day of discharge addressing their specific concerns related to psychological issues and post amputation stress were measured using same questionnaire on the day of discharge.
World Health Quality of Life (WHQOL)
WHQOL was administered throughout the study. It consists of 4 domains with 26 questions which measures physical health, psychological health, social and environmental factors. SPSS software was used to assess data.
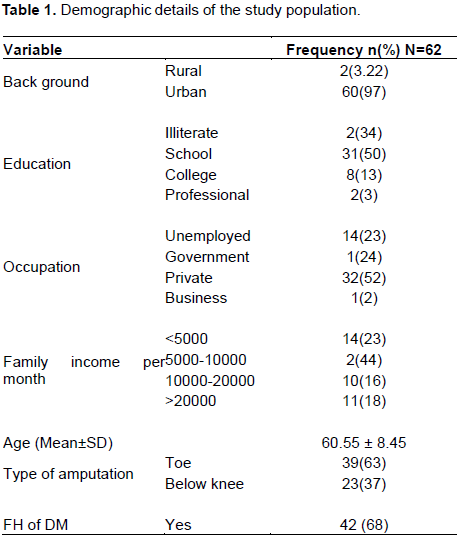
A total of 62 patients were included in the study out of which 36 patients were enrolled in the intensive counseling group (ICG) and 26 in the routine counseling group (RCG). Mean age of the RCG and ICG patients was 60.11 and 60.86, respectively. Demographic variables of patients are represented in Table 1. Majority of the patients are educated at school level and employed in private sector. Mostly, family income of patients was between 5000-10,000 Rs. hailing from an urban background. Among the study group, 63% of patient had undergone toe amputation and 37% had below knee amputation. 68% of patient’s had family history of diabetes and mean duration of diabetes in RCG and ICG was 12.76 and 13.69 years, respectively.
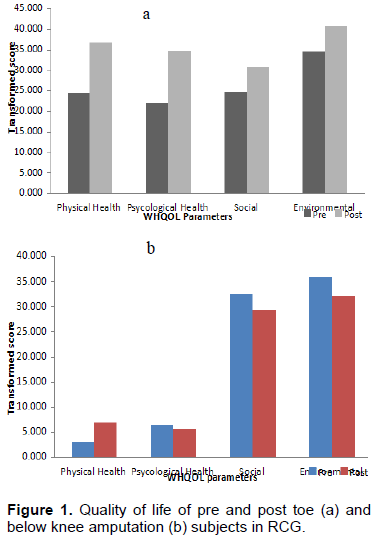
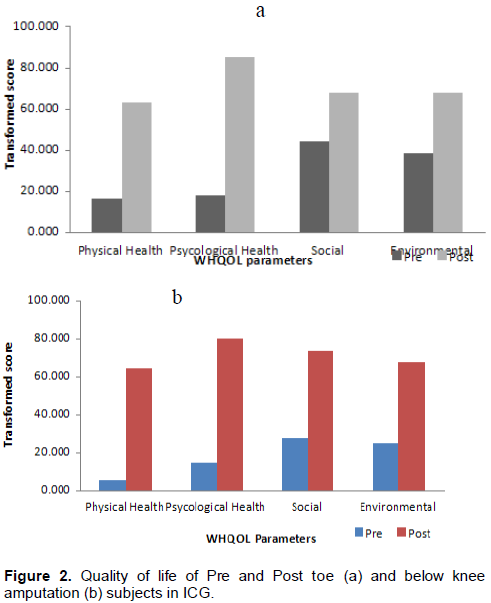
The mean score of all domains of Quality of Life in Pre & Post amputation among RCG & ICG group is presented in Tables 2 and 3. RCG group did not show a significant difference among pre & post amputation in all the four domains of WHQOL in both Toe and BKA amputation. In ICG group, significant improvement was observed in both Toe (p<0.0001) and BKA (p<0.0001) amputation in all domains of quality of life such as physical health, psychological health, social health and environmental factors. The intensive psychological counseling has better psychological outcomes on the quality of life as compared to RCG. Further finding showed that intensive psychological counseling showed better improvement in BKA amputation, as compared to toe amputation in all the domains of WHQOL.
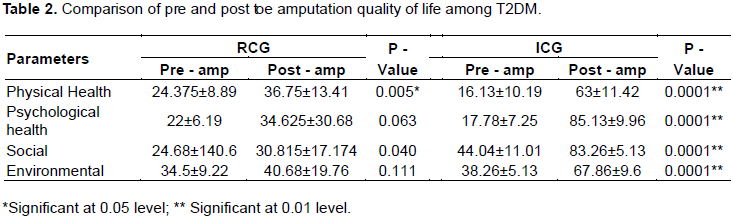
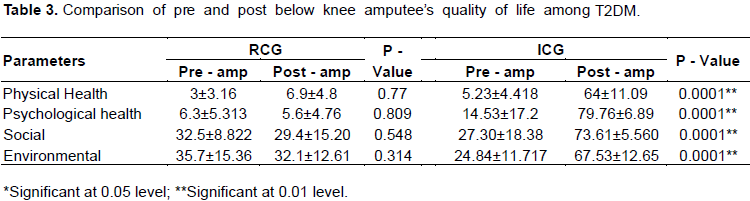
Figure 1 shows that there is no much difference found between pre and post Toe and below knee amputation subjects in control group and with single psychological counseling session, no significant improvements were found among amputees during the time of discharge.
Figure 2 clearly depicts that patient rendered with intensive psychological counseling in ICG group had vast improvements on quality of life. With one time psychological counseling, patients had no significant improvements in RCG group but with continuous intensive psychological counseling till day of discharge had significant improvement in post amputee’s quality of life as compared to pre amputee’s quality of life in same group at the time of discharge.
Psychological counseling plays an important role in managing diabetes. Psychological problems such as depression, stress and anxiety also have adverse effects in the management of diabetes. T2DM patients undergoing amputation suffer from various psychological stages of grief such as, denial, anger, bargaining, depression and acceptance which affects quality of life among amputees. Several studies have showed significant levels of anxiety, grief and social isolation among people with amputations (Schubert et al., 1992; Frierson and Lippmann, 1987; Thompson and Haran, 1984). Psychological adjustment plays a vital role among amputees quality of life, difficulties in adjustment are associated with reports of depression, feelings of hopelessness, low self-esteem, fatigue, anxiety and sometimes suicidal ideation (Desmond and MacLachlan, 2002). A multitude of related problems, including maladaptive coping behaviors (e.g, drug/alcohol consumption), greater disability, poorer social functioning, and loss of functional independence, may result from difficulties in psychological adjustment (Shobhana et al., 2000). Psychological state of the individual is equally important in understanding the total well being of the patient (Srivastava et al., 2010). Most amputees are in need of reassurance and psychological support, because amputation is a visible disability, there is usually hesitancy on the part of others to consider amputees as normal healthy individuals (Schubert et al., 1992).
The present study evaluated the effect of intensive psychological counseling on psychological outcomes among T2DM undergoing amputation and this is the first study to analyze the amputee’s quality of life and determine whether it changes with intensive psychological counseling. Psychological factors play a major role in diabetes management. The present study finding highlighted that the in ICG group, there was a significant improvement in all the domains of WHQOL such as physical health, social, psychological and environmental domains, whereas in RCG group, no significant improvement was observed in all the domains except physical health, which might be due to medication provided in the health care system.
Thus, the findings emphasized that the intensive counseling showed a better improvement in quality of life of amputees. Further with the routine counseling, the quality of life remained the same without further improvements in psychological aspects of amputees. Intensive counseling showed a significant difference in post amputation subjects in all domains of WHQOL as compared to pre amputation subjects by rendering continues sessions of counseling to the amputees till day of discharge. Amputees suffer from poor acceptance of body image, poor quality of life, providing intensive counseling and injecting strongly sense of acceptance in them and its use reduces depression and improves amputee’s quality of life. Effectiveness and usefulness of psychotherapeutic intervention in ameliorating the psychological distress of the amputees (Srivastava and Chaudhury, 2014) with regard to this study present study addresses the psychological concern of amputees during hospitalization, hence day to day intensive psychological counseling care is essential through regular observation, in order to improve amputee’s quality of life. Thus, the intensive psychological counseling among amputees was effective in alleviating psychological distress and created positive impact on quality of life of amputees.
IIn view of poor quality of life among amputees, it is recommended that psychological counseling together with regular follow up, addressing psychological related concerns has to be included as a part of overall management of amputees. Further, the role of counselor/ psychologist should be included as part of managing amputee’s quality of life.
In India, this is perhaps the first study in the domain of intensive psychological counseling till the day of discharge among amputees. This study highlighted the importance of intensive psychological counseling and showed a better impact as compared to routine psychological counseling in life of amputees. It is also proven that the patient offered intensive psychological counseling has better psychological out comes than patient offered routine psychological counseling. This study emphasizes the importance of intensive psycho-logical counseling rendered daily after an amputation till the day of discharge to reduce the sudden psychological trauma of an amputation. Thus, amputees have to be followed up with continuous psychological intervention till the day of discharge for their well-being. The study evaluated that rendering intensive psychological counseling among amputees shows significant improve-ments among psychological parameters due to which, amputees’ well-being and quality of life was improved.
The authors have not declared any conflict of interest.
REFERENCES
|
Aalaa M, Malazy OT, Sanjari M, Peimani M, Mohajeri-Tehrani MR (2012). Nurses' role in diabetic foot prevention and care; a review. J. Diabetes & Metabolic Disorders, 11(1):1.
Crossref
|
|
|
|
Abbas Z, Archibald L (2005). Epidemiology of the diabetic foot in Africa.Medical science monitor, 11(8):262-RA270.
|
|
|
|
Alavi A, Sibbald RG, Mayer D, Goodman L, Botros M, Armstrong DG, Kirsner RS (2014). Diabetic foot ulcers: part II. Management. J. Am. Acad. Dermatol. 70(1):21-e1.
Crossref
|
|
|
|
American Diabetes Association (1999). Consensus Development Conference on Diabetic Foot Wound Care: 7-8 April 1999, Boston, MA. Advances in Skin & Wound Care, 12(7):353-361.
|
|
|
|
Bengalorkar GM, Kumar TN (2011). Diabetic foot infections: A review. Int. J. Biol. Med. Res. 2:453-460.
|
|
|
|
Boulton AJ (1996). The pathogenesis of diabetic foot problems: an overview. Diabetic medicine: A journal of the British Diabetic Association, 13, S12.
|
|
|
|
Boulton AJ, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J (2005). The global burden of diabetic foot disease. The Lancet, 366(9498):1719-1724.
Crossref
|
|
|
|
Breslau N (2001). The epidemiology of posttraumatic stress disorder: what is the extent of the problem?. Journal of Clinical Psychiatry. 62 Suppl 17:16-22.
|
|
|
|
Cavanagh PR, Lipsky BA, Bradbury AW, Botek G (2005). Treatment for diabetic foot ulcers. The Lancet, 366(9498):1725-1735.
Crossref
|
|
|
|
Centers for Disease Control and Prevention (CDC. (2005). Lower extremity disease among persons aged> or= 40 years with and without diabetes--United States, 1999-2002. MMWR. Morbidity and mortality weekly report, 54(45):1158.
|
|
|
|
Chaturvedi N, Stevens LK, Fuller JH, Lee ET, Lu M (2001). WHO Multinational Study GroupRisk factors, ethnic differences and mortality associated with lower-extremity gangrene and amputation in diabetes. The WHO Multinational Study of Vascular Disease in Diabetes.Diabetologia, 44(2):S65-S71.
Crossref
|
|
|
|
Desmond D, MacLachlan M (2002). Psychosocial issues in the field of prosthetics and orthotics. JPO: J. Prosthetics and Orthotics 14(1):19-22.
Crossref
|
|
|
|
Frierson RL, Lippmann SB (1987). Psychiatric consultation for acute amputees: Report of a ten-year experience. Psychosomatics, 28(4):183-189.
Crossref
|
|
|
|
Lauterbach S, Kostev K, Kohlmann T (2010). Prevalence of diabetic foot syndrome and its risk factors in the UK. J. Wound Care, 19(8).
Crossref
|
|
|
|
Lavery LA, Ashry HR, Van Houtum W, Pugh JA, Harkless LB, Basu S (1996). Variation in the incidence and proportion of diabetes-related amputations in minorities. Diabetes Care 19(1):48-52.
Crossref
|
|
|
|
Moxey PW, Gogalniceanu P, Hinchliffe RJ, Loftus IM, Jones KJ, Thompson MM, Holt PJ (2011). Lower extremity amputations-a review of global variability in incidence. Diabetic Medicine, 28(10):1144-1153.
Crossref
|
|
|
|
Parkes CM (1976). The psychological reaction to loss of a limb: the first year after amputation. In Modern Perspectives in the Psychiatric Aspects of Surgery. Palgrave Macmillan UK. pp. 515-532.
Crossref
|
|
|
|
Pecoraro RE, Reiber GE, Burgess EM (1990). Pathways to diabetic limb amputation. Basis for prevention. Diabetes Care;13:513-521.
Crossref
|
|
|
|
Pendsey SP (1994). Epidemiological aspects of diabetic foot. Int. J. Diabetes.14:37-38.
|
|
|
|
Reiber GE (1996). The epidemiology of diabetic foot problems: proceedings of the second International symposium on the diabetic foot" Diab. Med. 13(1):6-11.
|
|
|
|
Richard JL, Schuldiner S (2008). [Epidemiology of diabetic foot problems]. La Revue de medecine interne/fondee... par la Societe nationale francaise de medecine interne, 29:S222-S230.
|
|
|
|
Rybarczyk BD, Nyenhuis DL, Nicholas JJ, Schulz R, Alioto RJ, Blair C (1992). Social discomfort and depression in a sample of adults with leg amputations. Archives of physical medicine and rehabilitation,73(12):1169-1173.
|
|
|
|
Schubert DS, Burns R, Paras W, Sioson E (1992). Decrease of depression during stroke and amputation rehabilitation. General hospital psychiatry, 14(2):135-141.
Crossref
|
|
|
|
Shobhana R, Rao PR, Lavanya A, Vijay V, Ramachandran A (2000). Cost burden to diabetic patients with foot complications a study from southern India. J Assoc Physicians India, 48:1147-1150.
|
|
|
|
Smith SR, Reed JF (2002). Prevalence of mixed infections in the diabetic pedal wound: A perspective based on a national audit. Int J Low Extrem Wounds;1:125-128.
Crossref
|
|
|
|
Srivastava K, Chaudhury S (2014). Rehabilitation after amputation: psychotherapeutic intervention module in Indian scenario. The Scientific World Journal.
Crossref
|
|
|
|
Srivastava K, Saldanha D, Chaudhury S, Ryali VSSR, Goyal S, Bhattacharyya D, Basannar D (2010). A study of psychological correlates after amputation. Med. J. Armed Forces India 66(4):367-373.
Crossref
|
|
|
|
Thompson DM, Haran D (1984). Living with an amputation. Int. J. Rehabilit. Res. 7(3):283-292.
Crossref
|
|
|
|
Vijay V, Snehalatha C, Ramachandran A (1997). Socio cultural practices that may affect the development of the diabetic foot." IDF Bulletin 42:10-12.
|
|
|
|
Vileikyte L. (2001). Diabetic foot ulcers: a quality of life issue.Diabetes/metabolism research and reviews, 17(4):246-224.
Crossref
|
|
|
|
Viswanathan V, Madhavan S, Rajasekar S, Chamukuttan S, Ambady R (2006). Urban-rural differences in the prevalence of foot complications in South-Indian diabetic patients." Diabetes care 29(3):701-703.
Crossref
|