Full Length Research Paper
ABSTRACT
Diabetes and its complications are responsible for premature death. However, mortality linked to diabetes remains under-estimated because many developing countries do not have data related to this affection. This study aimed to determine the causes of death in hospitalized diabetic patient in our context. We carried out a retrospective study in the Endocrine and Metabolic Disease Unit of the Yaoundé Central Hospital during a period of 36 months. We included all patients admitted in the unit with a diagnosis of diabetes and/or diabetic complication.Non diabetic patients were excluded. For statistical analysis, Kaplan-Meier cumulative survival plot was used to assess mortality over time and the log rank test to assess differences of the survival functions by group. Hazard ratios (HR) together with their 95% confidence interval (CI) were calculated from the Cox regression. We analyzed a total number of 1005 medical records. The total number of deaths recorded was 73 (40 men and 33 women). The mean age of hospitalized patients was 55 (±16 ) years; and 57 years for deceased patients.The main presenting complain on admission were: poor glycemic control in 653 (65%) cases followed by diabetes foot wounds: 150 (15%) and fever 85 (8.4%). Mortality rate during this period was 7.3%. Septic shock was the principal cause of death in 42.4% of deceased patients. The other causes were hyperosmolar Non ketotic States (19.1%) ketoacidosis (16.4%). However, 21.9% of patients died in the first 24 h of admission. In 47.9% of deceased patients diabetes was newly diagnosed. Infection remains a major problem and the principal cause of death in diabetes patients in our African context.
Key words: Infection, diabetes, mortality.
INTRODUCTION
Diabetes and its complications are responsible for premature deaths. In developed countries diabetes related mortality is dominated by cardiovascular and renal causes (Magliano et al., 2015; Romon et al., 2008), meanwhile the predominance of infectious diseases and acute metabolic complications has been reported in African Journals (Omenai and Ezenkwa, 2020; Azevedo and Alla, 2008. Diabetes accounts for 11.3% of global deaths in the word and 6.8% of all deaths in Africa (IDF Diabetes Atlas, 2019). One of the peculiarities in Africa is that diabetes becomes the bed of many other debilitating conditions including tuberculosis, which makes its morbidity and mortality high. In Cameroon, only mortality related to acute metabolic complications has been reported (Sobngwi et al., 2009; Dehayem et al., 2008). Knowing the proportion and causes of death in people with diabetes, will enable health policy makers to better draft the management of these patients; hence reduce preventable deaths. Cameroon does not yet have data on overall mortality attributable to diabetes. Since population studies are not easily feasible in a context of limited resources, we undertook a hospital based study in the endocrinology-diabetology department of Yaoundé Central Hospital (HCY) to determine causes of death in diabetic patients.
MATERIALS AND METHODS
This was a 36-months (from January 2015 to Decembrer 2018) retrospective study that analyzed the records of patients who died during their stay in the endocrinology unit at Yaounde Central Hospital. We included in the study all diabetic patients admitted to the department. Non diabetic patients were systematically excluded. We proceeded to overall review of the hospitalization register. Data collected were as follows: the age of the patient, the reason for hospitalization, the date of admission, discharge or death. For each deceased patient, the medical file was analyzed for the following information: age, gender, time of admission and death, reason for hospitalization, place of origin. We also specified the presence or absence of complications as well as comorbidities associated with deaths. We conducted a clinical evaluation with particular interest in the vital parameters: respiratory status (assessed by respiratory rate), hemodynamic status: blood pressure and pulse rate, and state of consciousness. The Glasgow coma scale was used to characterize the level of consciousness of these patients. The capillary blood glucose at admission was precised.
The causes of death were determined according to the information on the patient's death certificate, completed by the attending physician, or based on the clinical and / or biological picture presented by the latter prior to death. Each death was the subject of a morbi-mortality staff to clarify the exact causes of death.
Statistical analyzis
The data was analyzed by SPSS software version 18.0. The results were expressed in number or percentage, on average ± SD, or medians (inter-quartile ranges). The survival curve was established by the Kaplan-Meier method. The duration of the follow-up in hospitalization was defined from the time of admission in hospitalization until the date of discharge, death, or transfer to another service. The death incidence rate was determined by the ratio of the total number of deaths observed during the study period over the total risk period. The Hazard Ratio (HR) was calculated by the Cox regression method with a 95% confidence interval (CI). Fisher's test was used to study correlations between quantitative variables. The threshold of significance was set at a value p <0.05.
Ethical consideration
Approval was obtained from the Institutional Committee for Research on Human Health of University of Douala N°1580CEI-UDo/04/2018T.
RESULTS
Epidemiological data
During the defined period, 1005 patients were hospitalized, 517 (51.8%) men versus 488 (48.6%) women. The number of patients with diabetes was 996 (99.1%), and 9 (0.89%) for non-diabetics. The average age was 55 years (± 16 years). The main reason for hospitalization was glycemic imbalance: 653 (65%) cases, followed by diabetic foot wounds: 150 (15%) and fever 85 (8.4%) cases (Table 1).

Study of mortality
Characteristics of the deceased patients
During the period, 72 deaths related to diabetes were recorded including 39 men out of 517 men hospitalized against 33 women died out of 488 hospitalized women. The majority of the deceased patients had type 2 diabetes (83.6%) while 11% had type 1 diabetes; 4.1% have an unclassable diabetes and the time of admission. The average age of the deceased patients was 57 years.
Mortality following the duration of diabetes
The overall mortality at the end of the 3-year study was 7.2%. Death was observed in 47.9% of newly diagnosed patients. The average length of hospital stay before death was 5 days; however, 21.9% of patients died within the first 24 h of admission.
Causes of death
The causes of death were determined based on the diagnosis mentioned on the death certificate or based on the clinical and / or biological presentation of the patient at the time of death. Infections were at the forefront of causes of death (42.4%), followed by acute metabolic complications, namely, Hyperosmolar non Ketotic state (HONK) (19.1%) and ketoacidosis (16.4%).
Survival curve over time
The total period at risk which represented the cumulative duration of hospitalization was 4379 days. The maximum risk period was 95 days and the average survival period during hospitalization was 73 days [IQR: 27 - 93].
Mortality analysis: Kaplan-Meier method and Cox regression
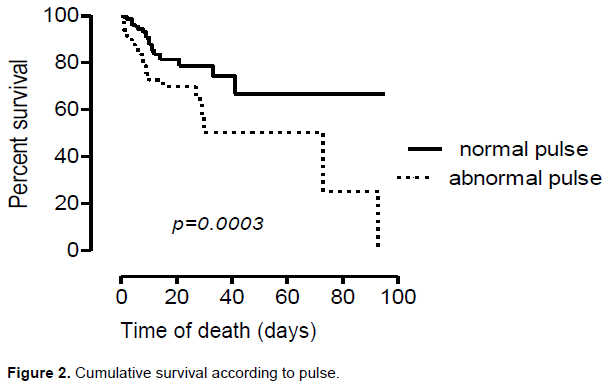
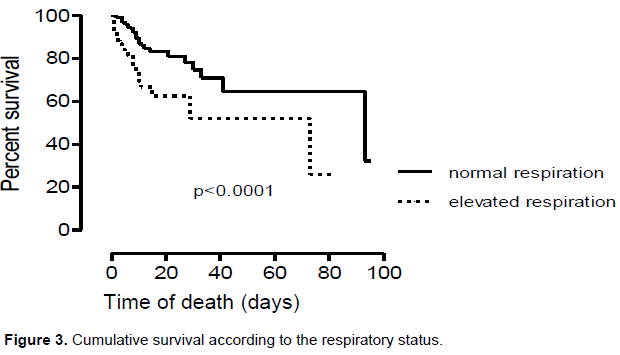
The survival functions were significantly different by comparing the respiratory status (p <0.0001) the pulse (p = 0.0003) and the state of consciousness (p <0.0001) (Figures 1 to 3). Uniform Cox proportional hazard analysis indicated that these independent variables influenced mortality: temperature ≥37.5°C at admission (HR = 3.78 [95% CI: 1.59-8.99]), high respiratory rate (HR = 2.72 [95% CI: 1.67 - 4.34]), abnormal pulse (HR = 2.41 [95% CI: 1.47 - 3.96]), and altered consciousness (HR = 6.56 [95% CI: 4.01 - 10.73]) (Table 2).
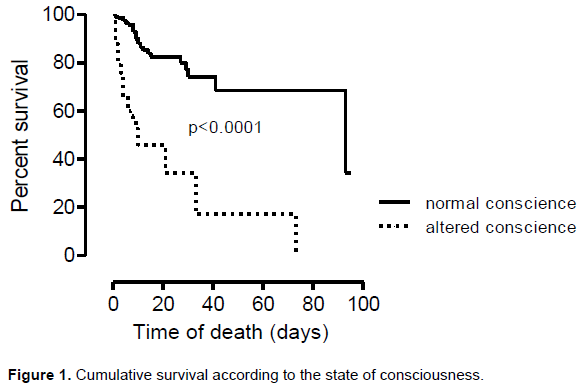
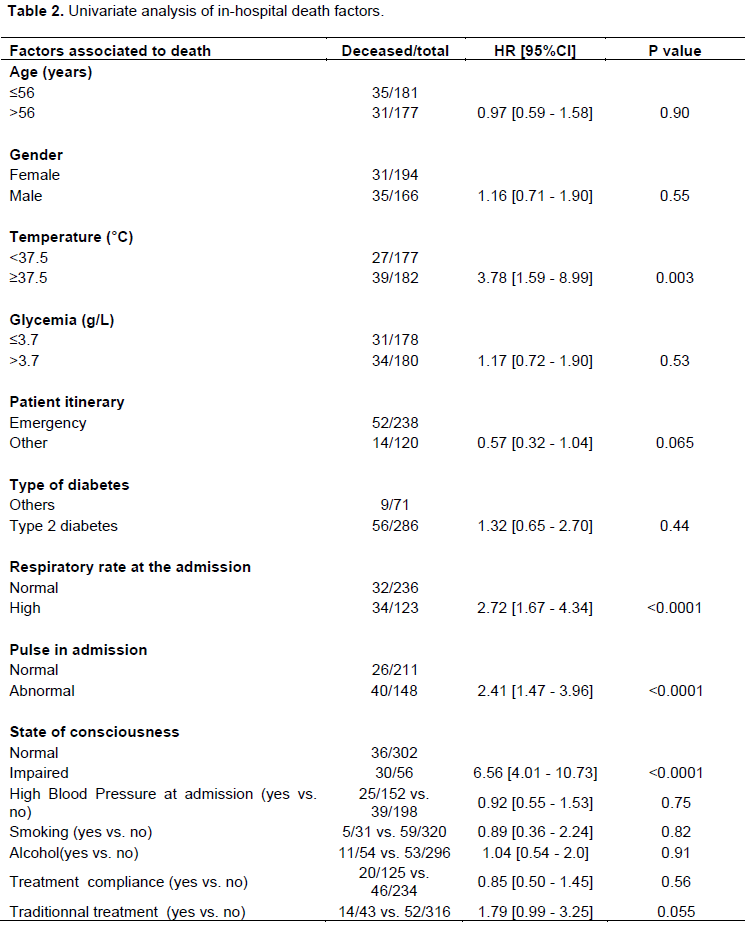
Analyzes show that patients who arrived with impaired consciousness had a higher risk of death compared to patients admitted with normal consciousness (HR = 5.27, 95 CI: 3.02-9.08, p <0.0001). Also, patients with inlet fever (≥ 37.5°C) also had a high risk of death compared with those who entered normal temperature.
DISCUSSION
This study reviewed the various causes of death in diabetic patients and the associated factors during a hospitalization stay. Our findings showed that among the 996 diabetic patients admitted in the unit, 72 died. That is a mortality rate of 7.2%. The main cause of death was infections followed by acute metabolic complications of diabetes. An important point was that 47.9% of death occurred in newly diagnosed patients and 21.9% of patients died within the first 24 h of admission. Altered vital parameters were strongly associated to death. Regarding hospital admissions, the high proportion of patients admitted to hospital with a glycemic imbalance, show that most patients are not sufficiently educated about the concept of this chronic disease and the need to take treatment continuously, since many of them had stopped or did not take their treatment regularly; this to the benefit of the traditional pharmacopoeia.
The maximum duration of hospitalization was 95 days. This relatively long time spent in hospital mainly concerned patients who were admitted for a diabetic foot ulcer. A particular aspect is that diabetic foot infections were polymicrobial making antibiotic combinations quite complex. In fact, the therapeutic strategy adopted in the department was, in the first instance, a conservative treatment based on daily local care and antibiotics, and secondly, in the absence of clinical improvement, amputation could be proposed. However, one of the limiting factors in this treatment was the cost of antibiotics which is very often high, which does not allow the regular administration of antibiotics and therefore a delay in the healing process and control of infection. Both of these parameters were taken into account for patient discharge.
Death observed within 24 h after admission in 22% of cases, signifies the degree of severity of the patient's condition at admission or delay transfer between medical emergencies and specialized services. Some African studies have revealed that the main causes of death related to diabetes are mainly hyperglycemic emergencies (hyperosmolar states and ketoacidosis) (Unachukwu et al., 2008). We found infectious causes in the first line, followed by hyperosmolar states and ketoacidosis. Similarly, in Morocco, a study (Azevedo and Alla, 2008) found a high proportion of in-hospital deaths related to diabetes whose cause were infections (32.5%), followed by acute metabolic complications from all causes (30.8%). Omenai in Nigeria identified infection as the leading cause of death in diabetics (Omenai and Ezenkwa, 2020). These results are in agreement with ours. Indeed, especially poorly balanced diabetes is a breeding ground for infections (Brisseau et al., 1989; Sathasivam, 2018), moreover it is well known that the infection itself is sufficient to imbalance acute diabetes. In our study, the clinical picture of hospitalized patients was indeed that of an underlying infection causing the hyperosmolar state or ketoacidosis that they presented on admission. In addition, the limited access to appropriate therapies due to the low or even zero rate of patients benefiting from health insurance contributes significantly to avoidable mortality. The causes of death from cardiovascular diseases poorly represented in our study (6.8%) are explained by the fact that patients are often referred to other appropriate services when necessary. It is currently shown that infections are the most common causes of death in people with diabetes in developing countries, unlike cardiovascular causes, which are more prevalent in industrialized countries (Hass and McDonnell, 2018; Balakumar and Maung, 2016).
We also studied the factors that may be associated with death, and it appears that abnormal vital parameters during hospital admission was associated with increased mortality. Impairment of consciousness has been identified as a factor of poor prognosis in these patients. Alteration of consciousness in the diabetic patient can be of multiple causes: besides the metabolic causes (hypoglycemia or hyperglycemia), vascular causes (stroke) and infectious (encephalitis / meningoencephalitis) can be encountered. A study previously done in the same department (Dehayem et al., 2008) identified as causes of coma in these diabetic patients, hypoglycemia (28.8%), ketoacidosis or hyperosmolar state (25%) and stroke in 5.7% of cases. Central nervous system infections were reported in 5.7% of cases. Our study did not analyze the different causes of impairment of consciousness. However, since the alteration of consciousness may be the stage preceding death, this could indeed be the consequence of the aforementioned causes which sometimes coexist in the same patient: namely, a severe infection which precipitates a hyperosmolar state and or ketoacidosis that can lead to the alteration of consciousness by various mechanisms. In fact, the admitted patients often had an underlying infectious factor which contributed to increase metabolic imbalance and simultaneously altered vital parameters through a systemic inflammatory response. Our study shows the comorbidities associated with diabetes that may increase in -hospital mortality. We can think, as some authors do, that mortality in diabetes patients with an acute metabolic complication is not always the direct consequence of the metabolic disorder that they present, but of the different co-morbidities associated with infections (Caroll and Matz, 1983; Seki, 1986).
RECOMMENDATIONS
The establishment of a national death register to identify the various causes will allow the implementation of a strategy to reduce the causes of preventable deaths in hospitals and other health institutions. Health- policy maker should facilitate access to care for these chronic patients who often arrive with severe conditions.
LIMITATIONS OF THE STUDY
The limits of this study is that, certain files were not exploitable because these one were conceived with essentially clinical aim and not necessarily for medical research; therefore, some data were missing. In addition, the study was not multicentric, the analyzes were done in a single diabetic clinic. However, the Yaoundé Central Hospital and therefore the endocrinology unit being a reference center, the sample is representative of the Cameroonian population. These results can therefore be extrapolated to the whole population.
CONCLUSION
Infection remains a major problem in diabetes patients in our context, compared to studies conducted in developed countries where cardiovascular causes are at the forefront. The alteration of vital parameters at admission, particularly the state of consciousness, is essential to monitor and correct because they increase mortality among our patients. Finally, there is still a concern about providing education and information on diabetes care because many of our patients do not take their medication or abandon it in favor of parallel therapy.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Azevedo M, Alla S (2008). Diabetes in sub-Saharian African : Kenya, Mali, Mozambique, Nigeria, South Africa, and Zambia. International Journal of Diabetes in Developing Countries 28(4):101-108. |
|
|
Balakumar P, Maung UK (2016). Jagadeesh. Prevalence and prevention of cardiovascular disease and diabetes mellitus. Pharmacological Research 113(A). |
|
|
Brisseau JM, Murat A, Raffi F, Ramee JF, Lucas V, Barrier JH, Guillon J (1989). Diabetes mellitus and infections. Revue de Médecine Interne 10(5):435-441. |
|
|
Caroll P, Matz R (1983). Uncontrolled diabetes mellitus in adults: Experience in treating diabetic ketoacidosis and hyperosmolar non ketotic coma with low-dose insulin and uniform treatment regimen. Diabetes Care 6:579-585. |
|
|
Dehayem M, Kengne AP, Choukem SP, Simo NL, Awah KP, Mbanya JC (2008). The spectrum of coma among people with diabetes in Cameroon: An appraisal of implications and challenges at the Yaounde Central Hopital. Annals of Tropical Medicine and Parasitology 102:73-78. |
|
|
Hass AV, McDonnell ME (2018). Pathogenesis of Cardiovascular Disease in Diabetes. Endocrinology and Metabolism Clinics of North America 47(1):51-63. |
|
|
IDF Diabetes Atlas (2019). Africa at a glance. In: IDF Diabetes Atlas. Ninth edition.p. 62. |
|
|
Magliano D, Cohen K, Harding J, Shaw J (2015). Residential distance from major urban areas, diabetes and cardiovascular mortality in Australia. Diabetes Research and Clinical Practice 109(2):271-278. |
|
|
Omenai SA, Ezenkwa US, Ajani MA (2020). Mortality patterns in patients with diabetes mellitus at a Nigerian tertiary hospital: A 10-Year autopsy study. Nigerian Postgraduate Medical Journal 27(2):83-86. |
|
|
Romon I, Jougla E, Balkau B, Fagot-Campagna A (2008). The burden of diabetes-related mortality in France in 2002: An analysis using both underlying and multiple causes of death. European Journal of Epidemiology. 23(5):327-334. |
|
|
Sathasivam P (2018). Head and Neck Infections in Diabetic Patients. Journal of the Association of Physicians of India 66(9):84-88. |
|
|
Seki S (1986). Clinical feature of hyperosmolar hyperglycemic non ketotic diabetic coma associated with cardiac operations. Journal of Thoracic and Cardiovascular Surgery 91(6):867-873. |
|
|
Sobngwi E, Lekoubou A, Dehayem M, Nouthe B, Balti E (2009). Evaluation of a simple management protocol for hyperglycaemic crises using intramuscular insulin in a resource-limited setting. Diabetes Metabolism 5(35):404-409. |
|
|
Unachukwu C, Uchenna D, Young E (2008). Mortality among diabetes in-patients in Port-Harcourt, Nigeria. African Journal of Endocrinology and Metabolism 7(1). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


