Full Length Research Paper
ABSTRACT
Microbial contamination of air in the operating theatre (OT) is considered to be a risk factor for surgical site infections (SSI) and quality of air can be considered as a mirror of the hygienic condition of these rooms. This study intended to determine the bacterial load and antibiotic susceptibility pattern of isolates in OT indoor air of Hawassa University Referral Hospital. A cross sectional study was conducted to measure indoor air microbial quality of OT from November 2014 to January 2015. 120 indoor air samples were collected from six sites in ten rounds using purposive sampling technique by Settle Plate Method (Passive Air Sampling following 1/1/1 Schedule). Sample processing and antimicrobial susceptibility testing was done using standard microbiological methods. The mean bacterial load of major OT 85.6 and 8.6 CFU/dm2 were recorded at active and passive time respectively. Likewise, 387.05 and 375.3 CFU/dm2 were observed in sterilization room and sterilized material store respectively. The finding was under acceptable range based on standard set by Fisher. Among the isolated five bacteria, S. aureus 54/120 (45%) and coagulase negative Staphylococci (CNS) 45/120 (37.5%) were the predominant species and highly resistant to penicillin and tetracycline (83.3 and 81.5%) respectively. Even though the overall mean CFU lied under the acceptable range, 65% of 120 samples were under the unsatisfactory level of bacterial load. The finding implies that the high bacterial load is a risk factor for surgical site infection (SSI). Therefore to reduce the load of bacterial contamination at critical area as well in the hospital environments, the hospital infection prevention and patient safety (IPPS) should be improved.
Key words: Indoor air, hospital environment, Southern Ethiopia.
INTRODUCTION
Microbial contamination of indoor hospital, especially in an operating theatre and other specialized units had continued to increase prevalence of nosocomial infections with resultant effect of high morbidity and mortality rate among patient admitted for post-operative surgery, patients (Napoli et al., 2012; Jyotshna et al., 2011).
Surgical site infection (SSI) is the second most common health care associated infection next to hospital acquired urinary tract infection (WHO, 2009). The rate of SSI varies from country to country depending on level of adherence to infection prevention practice measures in a given health care setting (Jroundi et al., 2007). The infection, which is an important clinical indicator for quality of patient care and infection control (Imai et al., 2008), is primarily determined by the overall contamination level of hospital environment like indoor air together with the surgeon’s technique during the operation, patient’s degree of susceptibility, insertion of foreign material or implants, suitability of surgical preparation, adequacy and timing of antimicrobial prophylaxis (Dharan and Pittet, 2002). Thus, to achieve acceptable performance in operating rooms (ORs) the hospital at large should achieve a complex range of infection prevention and patient softy (IPPS) measures by considering different contamination risks for SSI .(Kallel et al., 2005).
The importance of the estimation of the quantity and types of airborne microorganisms are that these values can be used as an index for the cleanliness of the environment as well as an index they bear in relation to human health and as source of hospital-acquired infections. The indoor air environment can potentially place patients at greater risk than the outside environment because enclosed spaces can imprison aerosols and allow them to build up to infectious levels (Landrinet al., 2007).
Most of the infections arising from indoor air could potentially be prevented through adequate application of infection control practices (CDC, 2003). For instance, measuring the degree of bacterial contamination of indoor air and the susceptibility pattern of the isolates to commonly used antibiotics in the area will help to select appropriate antibiotics for empirical therapy. This also helps to revise and if necessary, design appropriate hospital infection prevention protocols in an effort to minimize the incidence of costly SSI. Moreover, it provides the tools needed to localize the source and control the spread of SSI (CDC, 2003). Therefore, this study aimed to determine the degree of bacterial contamination of ORs indoor air with respect to acceptable bacterial load standards and measure antimicrobial susceptibility pattern of the isolates.
MATERIALS AND METHODS
Study area
This was a descriptive cross-sectional study conducted between November 2014 and January 2015, at Hawassa Referral Hospital, Hawassa, Southern Ethiopia. Hawassa, the capital of Southern Nations, Nationalities, and Peoples' Region (SNNPR) and it is located 275 km from the capital city of Ethiopia, Addis Ababa. The altitude of the town is 1697 km above sea level with mean annual temperature and rainfall of 20.9° o C and 997.6 mm respectively. The total population of Hawassa town is 130,579 with one to one male to female ratio. Hawassa Referral Hospital was inaugurated in November, 2005; it has 850 beds and serves about 12 million people. The hospital has about 300 daily outpatient visits.
Study design and sampling
A descriptive cross-sectional study was conducted between November 2014 and January 2015 in Hawassa Referral Hospital.
The air samples for the study was taken from six sites; from critical zone (the main surgery OR and gynaecology OR), intermediate zones which comprises female clothing room (FCR) and male clothing room (MCR), and from non-critical zone which include SR (sterilizing room) and sterilized material store (SMS).
Air samples were collected using settle plate or passive air sampling method following 1/1/1 schedule [(a 9cm in diameter sterile Petri dish with 5% Sheep’s blood agar ([9 mm diameter)] was left open to the air for an hour, a meter above the floor and a meter from the wall]) in OR units (Pasquarella et al., 2000). During air sampling sterile gloves, mouth masks and protective gown was worn to prevent self-contamination of the 5% Sheep’s blood agar plate (Oxoid, UK).
The air samples in critical zone of ORs were collected during both active and passive times whereas samples from Intermediate and non-critical zone of ORs was collected in the morning and afternoon in each ward round per week. Then, blood agar plates were transported to the microbiology laboratory and incubated aerobically for 24 hours at 37ºC. The total number of colony forming units (CFU) was enumerated using colony counter and results were expressed in CFU/dm2 (Andersson et al., 2012). The colonies were assessed further using the biochemical tests following standard bacteriological techniques to isolate species (WHO, 2010).
The antimicrobial susceptibility testing was done on Mueller-Hinton agar (Oxoid, UK) for every potential pathogenic bacteria isolates with 12 antibiotics each by Kirby-Bauer disk diffusion method matching the test organism to 0.5 McFarland turbidity standards. Then, the susceptibility result was interpreted according to the principles established by Clinical and Laboratory Standards Institute (CLSI) by measuring the zone diameter of inhibition (CLSI, 2005). Reference strains S. aureus (ATCC 25923); E. coli (ATCC 25922) and P. Aeruginosa (ATCC 27853) were used as a quality control for culture and susceptibility testing throughout the study.
All data was analyzed using statistical package for Social Sciences (SPSS) version 16.0 and Microsoft Office Excel. Results were interpreted according to baseline values suggested by Fisher (Fisher et al., 1972; Pasquarella et al., 2000) and values of p<0.05 was considered as statistically significant. The ethical clearance was obtained from Hawassa University ethical review board.
RESULTS
A total of 120 air samples were collected twice per day from six different sites over a period of 10 weeks. The study revealed that the FCR of the OT had the highest bacterial counts (654 CFU/dm2) and the OR room had the lowest bacterial count (3.2 CFU/dm2) (Table 1). The mean bacterial load of major ORs rooms when it was active (85.6 CFU/dm2) and when it was passive (8.6/CFU/dm2) were recorded. According to Fisher’s index of microbial air contamination (Pasquarella et al., 2000), air microbial count of OR at rest and in activity must not exceed 9.0 and 91.0 CFU/dm2 respectively (Table 1).
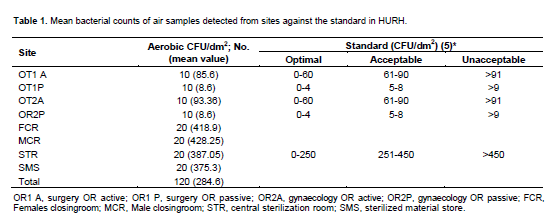
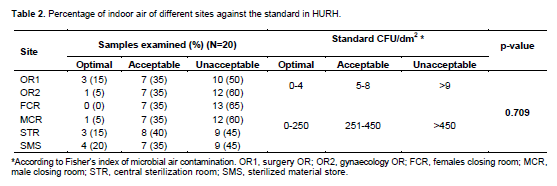
Sterilization room and sterilized material store also showed maximum of 543 and 560 CFU/dm2/h, respectively with mean aerobic colony counts of 387.05 and 375.3 CFU/dm2 respectively. The mean colony counts in all sites except gynaecology OR when active were found to be within the acceptable limit as shown in the Table 1. On the other hand, among the 20 samples from each site 50% of major OT, 60% of gynaecology OT, 65% of FCR and 60% of MCR were beyond the tolerable limit compared to the standard (Table 2).
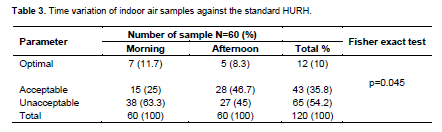
In regard to timing the highest bacterial populations recorded in the afternoon samples 45% were beyond the tolerable limit while the morning time samples were 63.3% unacceptable compared to standard set by fisher. It was statically significant, p=0.045 (Table 3).
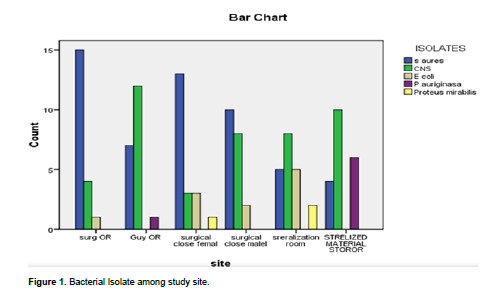
Five bacterial species were identified. Among these S. aureus 54 (45%) and CNS 45 (37.5%) were the predominant species. Regarding to site, S aureus recorded 15 (27.8%) at major OR and 13 (24%) at MCR of the OR. On the other hand the prevailing isolates at genecology OR and sterilized material store room was CNS 12 (26.7%) and 10 (22.2%) respectively. The isolation rate (40.7%) of S. aureus was higher in the two OR than non- OR sites (Figure 1).
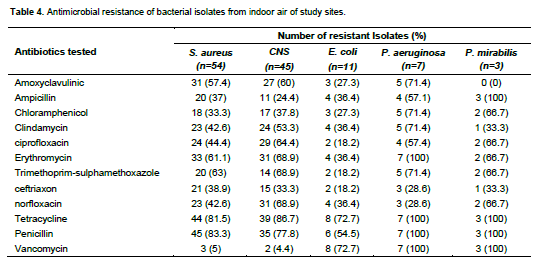
The antimicrobial susceptibility patterns of isolates showed that S. aureus was highly resistant to penicillin, tetracycline and to trimethoprim sulphamethoxazole at 83.3%, 81.5% and 63% level respectively. CNS also shows comparable resistance for tetracycline and penicillin (Table 4).
DISCUSSION
Microbial contamination of air in the OR is commonly well thought-out to be a risk factor for surgical site infections in clean surgery. According to (Pasquarella and colleagues et al., (2000) microbiological quality of air may be considered as mirror of the hygienic condition of the operation theatres. It is also understood that the quality of indoor air depends on internal sources, such as ventilation, cleaning procedures of the surgical team and their activity.
The microbial load in hospital indoor air is highly influenced by the number of occupants, their activity and the ventilation. Ventilation causes dilution thus reducing the microbial load. So, indoor bacterial load analysis is very important to know the state of ventilation and cleanness of critical areas within the hospital.
In this study the mean colony counts obtained (Table 1) from all sites except the 93.36 CFU/dm2 of gynaecology OT while at active were almost in the acceptable range of bacteriological standard set by Fisher (Pasquarella et al., 2000). Although mean CFU indicates the tolerability range, from the collected 20 samples of each site almost half (10 samples result) shows the unacceptable range. For instance the major OT 50%, gynaecology OT 60% and MCR 60% were under unacceptable level. The possible explanation for the increased load of CFU counts could be the human trafficking particularly students in these room as HURH is a teaching and referral hospital in the region. Besides, the cleaning state of rooms and continues follow-up of sterility of critical areas of the hospital might have offered for the undesirable aerobic bacterial load observed in these rooms. This finding goes in line with the study conducted in Northern Ethiopia (Tewelde et al., 2015) in Jordan (Qudiesat et al., 2009) and also the standard by Fisher (Pasquarella et al., 2000) which explained that the bacterial load of indoor air of OR is higher when it is active than when it is passive. But this studies result was different compared to the findings of the study done in Jimma Ethiopia (Genet et al., 2011) which reported that both ORs were not in the acceptable range.
The mean colony count 85.6 CFU/dm2 and 93.4 CFU/dm2 obtained from major OT and genecology OT at active time respectively (Table 1) were comparable with a study conducted in Northern Ethiopia (Tewelde et al., 2015) that reported mean colony count of 91.8, 44.9 and 17.2 CFU/dm2 for OR respectively.
The highest bacterial populations recorded in the afternoon 27 (45%) samples were beyond the tolerable limit compared to the 38 (63.3%) of the morning samples which were unacceptable compared to standard set by fisher (P=0.045) (Table 3). This result was in line with the finding in Northern Ethiopia (Tewelde et al., 2015b). But, disagree with Jimma South west Ethiopia finding (Genet et al., 2011) that reported that the colony counts in all OTs except sterilized cloth store were found to be higher in the afternoon than in the morning.
Five bacteria were isolated from a total of 120 air samples examined. Among these S. aureus 54 (45%) and CNS 45 (37.5%) were dominant. In addition, S. aureus was isolated in all sites even though the higher rate was recorded at major OR as a whole (both the critical area along with non-critical area (MCR and FCR). The finding was almost comparable with most of the studies elsewhere, (Shiaka et al., 2014; Qudiesat et al., 2009) which indicates the carrier state of health workers at major OR. On the other hand, the predominant isolates at genecology OR and sterilized material store room was CNS; the finding is similar with studies conducted in Jimma (Genet et al., 2011), India (Chacko et al., 2003) and Iraq (Ensayef et al., 2009). The source is more often endogenously from the normal skin flora of patients or exogenously from health workers.
The high level of resistance of S. aureus and CNS to penicillin and tetracycline found in our study has been widely reported throughout the world, (Genet et al., 2011; Tewelde et al., 2015; AlLaham, 2012) and this might be due to emergence of penicillin resistant beta-lactamase producing strains. There was low resistance to amoxcilin, ceftriaxone and vancomycin. The possible explanation for this might be these drugs not intensively used and not easily available outside the hospitals. For P. mirabilies the absence of resistance to amoxyclavulinic in this study make these drugs excellent choices. Ciprofloxacin, trimethoprim-sulphamethoxazole and ceftriaxon were sensitive for to E. coli as well.
CONCLUSIONS
In general half of the 20 indoor air samples of major OR were unacceptable bacterial load compared to the standard. As to the entire site, 65% of sampled sites were under the unsatisfactory level of bacterial load. The finding imply that the high bacterial load of indoor air judges it as a risk factor for SSI since there is a linear relationship between bacteria count in air and surgical site infection rate (Cheesbrough., 2005). On the other hand, the isolates found (S. aureus and CNS) are indicators of the hygiene status of these critical areas. Hence, to reduce the load of bacterial contamination at critical area as well in the hospital environments, the hospital infection prevention and patient safety (IPPS) should be improved and such type of surveillance should be strengthen.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
AlLaham NA (2012). Distribution and Antimicrobial Resistance Pattern of Bacteria Isolated from Operation Theaters at Gaza Strip. J. Al Azhar University-Gaza. 14:19-34. |
|
|
Andersson A E, BerghI, Karlsson J, Eriksson BI, Nilsson K (2012). Traffic flow in the operating room: An explorative and descriptive study on air quality during orthopedictraumaim plant surgery. Am. J. Infect. Control. 40(8):750-755. |
|
|
Centers for Disease Control and Prevention, Healthcare Infection Control Advisory Committee. Guidelines for environmental infection control in healthcare facilities. Atlanta. 2003. |
|
|
Chacko L, Jose S, Isaac A, Bhat KG (2003).Survival of nosocomial bacteria on hospital fabrics. Indian J. Med. Microbiol. 21(4):291. |
|
|
Cheesbrough M (2005).District laboratory practice in tropical countries volume II: microbiology. Cambridge (UK).pp. 26-196. |
|
|
Dharan S, Pittet D (2002). Environmental controls in operating theatres (review). J. Hosp. Infect. 51:79-84. |
|
|
Ekhaise FO, Ighosewe OU, Arakpovi OD (2008). Hospital indoor airborne microflora in private and government owned Hospital in Benin City, Nigeria. World J. Med. Sci. 3:19-23. |
|
|
Ekhaise FO, Isitor EE, I dehen O, Emogbene OA (2010). Airborne microflora in the atmosphere of an hospital environment of University of Benin Teaching Hospital (UBTH), Benin City, Nigeria. World J. Agric Sci. 6:166-170. |
|
|
Ensayef S, AlShalchi S, Sabbar M (2009).Microbial contamination in the operating theatre: A study in a hospital in Baghdad. East Mediter. Health J. 15(1):219-223. |
|
|
Fisher G, Fodré S, Nehéz M (1972). Das Ergebnis der Untersuchungenzur Feststellungs von Gesamtkeimzahl- Grenzwerten in der Luft von Operations raumen. English version can be found on a review article by Pasquarella CetalZ GesHyg1972; 18:729-733. |
|
|
Genet C, Kibru G, Tsegaye W (2011). Indoor air bacterial load and antibiotic susceptibility pattern of isolates in operating rooms and surgical wards at Jimma University specialized hospital, south west Ethiopia. Ethiop. J. Health Sci. 21(1):9-17. |
|
|
Imai E, Ueda M, Kanao K, Kubota T, Hasegawa H, Omae K, Kitajima M (2008). Surgical site infection risk factors identified by multivariate analysis for patient undergoing laparoscopic, open colon, and gastric surgery. Am. J. Infect. Control. 36:727-31. |
|
|
Jroundi I, Khoudri I, Azzouzi A, Zeggwagh, AA, Benbrahim NF, Hassouni F, Oualine M, Abouqal R, (2007). Prevalence of hospital-acquired infection in a Moroccan university hospital. Am. J. Infect. Control 35(6):412-416. |
|
|
Jyotshna M, Helmut B (2011).Bio aerosols in Indoor Environment-A Review with Special Reference to Residential and Occupational Locations. The Open Environ. Biol Mon. J. 4:83-96. |
|
|
Kallel H, Bahoul M, Ksibi H, Dammak H, Chelly H, Hamida CB, Chaari A, Rekik N, Bouaziz M (2005). Prevalence of hospital-acquired infection in a Tunisian hospital. J. Hosp. Infect. 59(4):343-347. |
|
|
Landrin A, Bissery A, Kac G (2005). Monitoring air sampling in operating theatres: Can particle counting replace microbiological sampling? J. Hosp. Infect. 61(1):27-29. |
|
|
Napoli C, Marcotrigiano V, Montagna MT (2012). Air sampling procedures to evaluate microbial contamination: A comparison between active and passive methods in operating theaters. BMC Public Health, 12(1):594. |
|
|
National Committee for Clinical Laboratory Standards. Performance standards for antimicrobial susceptibility tests; fifth informational supplement. 5th ed. M100-S15; 25(1) Wayne, 2005. |
|
|
Pasquarella C, Pitzurra O, Savino A (2000). The index of microbial air contamination (review).J. Hosp. Infect. 46:24156. |
|
|
Qudiesat K, Abu-Elteen K, Elkarmi A, Hamad M, Abussaud M (2009). Assessment of airborne pathogens in health care settings. Afr. J. Microbiol. Res. 3(2):066-076 February, 2009. |
|
|
Shiaka, G. Peter, Yakubu S (2014). Indoor Airborne Bacterial Concentration of a Private-Owned Hospital Laboratory in Samaru-Zaria J. Biol. Agric. Healthcare 4:20. |
|
|
Splendlore JC, Fanin KF (1983).Source significance and control of indoor microbial aerosols: Human health aspects. Public Health, 98:229-244. |
|
|
Tewelde TG, Kibrom GD, Yibrah BZ, Saravanan M (2015). Microbial load of operating theatre at Ayder Referral Hospital, Northern Ethiopia. Afr. J. Microbiol. Res. 9(9):639-642. |
|
|
WHO (1991). Basic laboratory procedures in clinical bacteriology. Geneva. |
|
|
WHO (2002). Prevention of Nosocomial infections: A practical guide. Malta: Department of communicable Disease, Surveillance and Response. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


