Full Length Research Paper

ABSTRACT
The influence of aqueous extract of millet on the crystallization and the dissolution of calcium oxalate (CaOx) crystals were investigated in detail under supersaturated and artificial urinary circumstances in order to understand the effect of the water-soluble components of millet on CaOx kidney stones in humans. To investigate the inhibition effect, different volumes of millet extract were added separately to the combined supersaturated and artificial urinary solutions while the crystal deposition process was monitored by UV-Vis and conductivity measurements. The harvested crystals were characterized by FT-IR, SEM, TGA, XRD and redox titrations so as to determine the structure and the morphology of CaOx crystals formed. Our findings indicate that the crystals obtained from inhibition and dissolution experiments were mainly calcium oxalate monohydrate (COM), the thermodynamically more stable phase. Furthermore, the results show that the millet extract has a promising inhibition effect in the supersaturated solution and in artificial urinary circumstances showing ~34 and ~26% decrease in crystal deposition, respectively, with 50 mL of millet extract compared to control experiments. The dissolution effect of millet extract is far superior to that of the inhibition effect. One gram of COM crystals completely disappeared when the crystals were washed ten times with 300 mL millet extracts. Under the same conditions, the control experiment showed only ~44% dissolution of COM crystals. Further investigations conducted with actual kidney stones under artificial urinary circumstances showed approximately 20% dissolution when washings were carried out using 300-mL portions of millet over one week. This novel finding may shed the light on the possible use of millet as a potential natural antiurolithic remedy to treat CaOx kidney stones in humans.
Key words: Calcium oxalate, kidney stones, millet, inhibition, dissolution effect.
INTRODUCTION
Over several centuries, millions of people have been affected by kidney stone disease around the world. (Evan et al., 2019; Sakhaee, 2009; Tang et al., 2006). Kidney stones are collections of gravel-like chemicals deposited in any area from kidney to bladder. (Wesson and Word 2007). Calcium Oxalate (CaOx) is one of the leading constituents found in human kidney stones and it crystallizes in three different forms: CaC2O4.H2O (COM), CaC2O4.(2+x) H2O (x = 0.5) (COD), and CaC2O4.3H2O (COT). (Bouropoulos et al., 2001; Fischer and Mun?oz-Espí, 2011; Franceschi and Nakata, 2005). COT is very rare and approximately 60% of kidney stones account for the sum of COM and COD recorded in humans. (Moe, 2006; Scales et al., 2012). Microcrystalline, bio-mineralized aggregates of CaOx crystals can grow into several centimeters in size with prolonged retention in the urinary track. Any kidney stone less than 2 to 5 mm in size may pass with the urine and any crystallites bigger than that are retained in the body causing severe pain to the patient when they move in the urinary system. (Golzari et al., 2014; Peng et al., 2012; Segura et al., 1997; Ouyan et al., 2003). Even though the kidney stone disease is currently a global health issue, few therapeutic protocols are effective to treat and to avoid the reoccurrence of kidney stones after surgical removal (Gravina et al., 2005; Xie et al., 2015). Commercially available drugs such as tamosulosin, alfuzosin, nifedipine, doxazosin, and terazosin have been prescribed to patients as ureter muscle relaxants to ease the passage of kidney stones with the urine (Lipkin and Shah 2006). These drugs may not be effective for either achieving 100% stone passage (Ahmed and Al-sayed, 2010; Porpiglia et al., 2004; Sio and Autorino, 2006) or for expelling relatively large stones without interventional therapies. (Gravina et al., 2005; Junuzovic et al., 2014; Resim et al., 2005).
Renacidin, a drug which is a mixture of magnesium carbonate, citric acid, and glucono delta-lactone, has been used as a common non-pyrogenic irrigation solution to dissolve relatively large bladder calculi over last five decades. (Gonzalez et al., 2012) Renal and ureteral damage are the common problems reported with the prolong use of Renacidin as a clinical drug. (Fostvedt and Barnes, 1963; Manzoor et al., 2019; Polat and Eral, 2022) And also, lack of well characterized COM dissolution agents make it difficult to establish calcium stones dissolution therapy. (Chutipongtanate et al., 2012) Therefore, the identification of new formulae or remedies to dissolve large kidney stones with ease and with minimal damage to the urinary track is an urgent and an essential task. (Polat and Eral, 2021). At the same time, preventing the reoccurrence of kidney stones is also important as the composition of the urine can influence the risks of stone reoccurance. (Batinic et al., 2000) Factors can be developed for the risks of stone formation resulting from the imbalance of promoting and inhibiting factors. (Basavaraj et al., 2007; Das et al., 2017). One set of factors related to urolithiasis was the ratio of oxalate/citrate × glycosaminoglycans. (Batinic et al., 2000). Children showing a value for this ratio >34 were the subjects of increased oxalate excretion and other children showing a value <10 were the subjects of decreased glycosaminoglycans excretion. Citrate has been observed to inhibit calcium oxalate monohydrate crystal formation along with another compound hydroxycitrate. (Chung et al., 2016). These agents bind to different crystallographic planes to inhibit the growth of the crystal along the axes characteristic of the planes.Inhibition of crystal growth along these indicated axes occurs as a result of the increased local strain on the crystal lattice that causes the local dissolution of the cations/anions. Another set of risk factors regulate the formation of COM versus COD crystals through the interplay of Escherichia coli and melamine. (Zhao et al., 2014). In the absence of E. coli secretion, only the thermodynamically stable crystal was formed: COM.
When E. coli was present in the urine, only COD was formed. From this same study, the extreme sensitivity was observed for the presence of melamine upon the formation of calcium oxalate crystals in urine. Fundamental studies of calcium oxalate monohydrate solubility showed increased solubility as the calcium cation was exchanged by sodium, potassium, or magnesium (Ibis et al., 2020).
This short literature summary shows that (1) altering the bulk solution properties can be used to increase solubility of calcium oxalate stones, and (2) introducing certain agents at the solution/calcium oxalate crystal interface causes dissolution of this interface; thereby, altering the stone solubility using very little of the therapeutic agent. Finally, the most effective treatment protocols combine several active agents. In this regard, natural remedies have attracted considerable interest over synthetic drugs due to the presence of high levels of inhibitors with relatively high efficiency. (Atmani et al., 2004). The use of medicinal plants for the treatment of kidney stones have been studied extensively, however, many showed diuretic properties rather than dissolution or formation-prevention properties. (Alok et al., 2013; Chitme et al., 2010; Himani et al., 2013). In recent years, due to the popularization of social media and related internet usage, millet has been the subject of many reports showing its effectiveness for treating CaOx kidney stones, however, there are no experimental evidences available in the literature to explain its action on kidney stones. (www.cuisinandhealthy.com Accessed by 2018. 08. 05.; www.healthyfoodvision.com Accessed by 2018. 08. 05.; www.secretlyhealthy.com Accessed by 2018. 08. 05.; www.staynaturallyhealthy.com Accessed by 2018. 08. 05).
Therefore, the current study is designed to investigate the antiurolithic properties of millet as an effective inhibiting and dissolution agent to treat CaOx kidney stones found in humans. Millet seeds are rich in proteins, carbohydrates, lipids, minerals and vitamins. (Baptist and Perera, 2007; Geervani and Eggum, 1989; Kalinova and Moudry, 2006; Qiu et al., 2005). The major fatty acids found in millet are linoleic, oleic, and palmitic acids (Table S-1, Supplementary Information). (Ghodsizad and Safekordi, 2012). Several chemical and biological compounds e.g. citrate, phosphates, proteins, macromolecules, such as organic acids and vitamins are known to act as molecular modifiers or inhibitors to prevent the solid phase crystal formation or to retard the nucleation, aggregation and growth of crystals. (Chung et al., 2016; Gul and Monga, 2014; Jung et al., 2004; Qiu et al., 2004; Roberto et al., 2019; Sheng et al., 2003; Taller et al., 2007). Since millet is rich in more of the aforementioned compounds (vide supra), the main aim of this study is to investigate the possible use of millet as an effective inhibiting and dissolution agent to treat calcium oxalate kidney stones found in humans.
MATERIALS AND METHODS
Sodium oxalate (Na2C2O4), potassium permanganate (KMnO4), sulfuric acid (H2SO4), sodium citrate (Na3C6H5O7), magnesium sulfate (MgSO4) and sodium sulfate (Na2SO4) were obtained from Merck chemical company. Sodium chloride (NaCl), sodium dihydrogen phosphate (NaH2PO4) and potassium chloride (KCl) were purchased from BDH chemical company. Calcium chloride (CaCl2) was obtained from Cancaster chemical company in GPR grade. Calcium chloride monohydrate (CaCl2.H2O) was supplied from Sigma chemical company. All of the other chemicals were obtained in GPR grade and used as received without further purifications. Actual CaOx kidney stones were collected from general hospital, Colombo, Sri Lanka from percutaneous nephrolithotomy cases. The calcium stones were characterized by redox titrations to confirm the identity. The obtained results were compared with an authentic sample of 99% pure COM purchased from Sigma Aldrich chemical company.
Inhibition experiments
Different varieties of millet are grown commercially such as finger millet, pearl millet, and proso millet. Proso millet (Panicum miliaceum) was used for the current study which grows well in south Asia. Millet grains were purchased from the local market in Matara, Sri Lanka and the identity was confirmed with the help of the plant genetic resource center at Gannoruwa, Sri Lanka. Millet solutions were prepared by soaking 200 g of dehulled millet grains in boiled water (~95°C, 1 L) for 12 h. The resulted solution was filtered and this filtrate was used for all experiments. To investigate the inhibition effect, different volumes of millet extract were added separately to supersaturated solutions as well as to artificial urinary solutions. CaOx super saturated solutions were prepared according to the procedure reported in literature, however, the concentrations used in the current study were approximately 25 times greater than the supersaturated level used in the literature. (Zhao et al., 2014). 5mmol of Na2C2O4 were dissolved in 40 mL of deionized water under magnetic stirring (6 rpm). 4 mmol of CaCl2 were dissolved separately in 50 mL of deionized water and added to the aforementioned Na2C2O4 solution at a rate of 5 mL/min. The pH value of the solution was adjusted to 7.3 by adding few drops of 0.01 M HCl and kept at 37.5°C. This solution was used as the supersaturation solution, herein. Initially, small volumes of millet (5, 10, 15, 20, 25 and 30 mL) were added separately to the supersaturation solutions to avoid the dilution of Ca2+ and C2O42- ions. Control experiments were performed using adequate volumes of deionized water (5, 10, 15, 20, 25 and 30 mL). Additional experiments were completed, increasing the volume up to 35, 40, 45, and 50 mL. After keeping these solutions under static conditions for 24 h, at 37.5°C, the solutions were filtered and CaOx crystals were collected and dried at 105°C. The mass of harvested crystals was recorded. A separate experiment was performed using CaCl2 and Na2C2O4 alone under the same conditions to harvest CaC2O4 which was used to calculate the %inhibition. Typical %inhibition calculations were performed using the following equation.

A typical standard reference artificial urine solution was prepared to simulate the natural urine conditions. .(Miyake et al., 1988). The composition of the artificial urinary system comprises 0.634 g of NaCl (sodium chloride), 0.0869 g of NaH2PO4 (sodium dihydrogen phosphate), 0.2606 g of Na3C6H5O7 (sodium citrate), 0.0489 g of MgSO4 (magnesium sulfate), 0.258 g of Na2SO4 (sodium sulfate), 0.450 g KCl (potassium chloride), 0.089 g of CaCl2.2H2O (calcium chloride dihydrate), 0.161 g of NH4Cl (ammonium chloride) in 200 mL of deionized water. The pH of the solution was adjusted to 7.3 by adding few drops of 0.01 M HCl. 4 mM of CaCl2 was dissolved in 50 mL of deionized water and 5 mM of Na2C2O4 was dissolved in 40 mL of deionized water. These two solutions were injected into the aforementioned artificial urinary system prepared in a conical flask at a constant velocity under 37.5°C. Ten milliliters of millet extract was added to the solution and was kept in an incubator at 37.5°C for 6 h and the solution was filtered off and the formed crystals were collected. The mass of crystals was recorded after drying at 105°C. The aforementioned procedure was repeated using 20, 30, 40 and 50 mL of millet. The control experiments were carried out using 10, 20, 30, 40 and 50 mL of deionized water. The mass of the crystals formed was recorded after drying the collected crystals at 105°C. Experiments were conducted in triplicate whenever possible.
Dissolution experiments
Approximately 1 g of CaC2O4.H2O crystals was measured into a conical flask and 300 mL of millet solution was added into it and was kept for 6 h under static conditions. After that the solution was filtered and the weight of the undissolved crystals was determined after drying at 105°C. This procedure was repeated with fresh 300 mL samples of millet until all the solids dissolved. Control experiments were performed using 300 mL volumes of deionized water and approximately 1 g of CaOx crystals. The dissolution effects of millet on actual kidney stones were investigated using approximately 0.2 g of CaOx kidney stones. The stone was washed with deionized water and dried at 105°C prior to use. A three hundred wash solution was added to the calcium stones in a conical flask which was maintained under artificial urinary conditions at 37.5°C and an equaling pH of 7.3. The system was then left alone under static conditions for 6 h. The solution was filtered, stones were collected, and then dried at 105°C. Likewise, the whole procedure was repeated seven times.
Characterizations
The obtained CaOx crystals in all experiments were analyzed by redox titrations, TGA, FT-IR, XRD, and SEM. The crystal deposition process was monitored by measuring the free oxalate concentration using UV-Vis spectrophotometer (HITACHI, UH 5300 UV/VIS). Infrared spectra of pure CaOx and CaOx obtained in the presence and absence of millet were recorded on a Thermo Scientific Nicolet IS10 spectrometer. Ion mobility of the solution was measured using Conductivity meter (WGCON 1103, Wagtech). X-ray powder diffraction studies were carried out using Ultima IV diffractometer scanning form 0-60° with 0.02 step width. Phase and morphology identification of CaOx crystal was completed using a Scanning Electron Microscope (SEM- Hitachi SU 6600 with 35.0 k magnification). Thermal Gravimetric Analyses (TGA) were performed on a TAQ 600 TGA under a stream of dry air. For the determination of metal ion concentrations in millet extracts, iCE 3000 AA015121002 vl-30 atomic absorption spectrometer was used (Flame type: air-C2H2, burner height 11.0 mm, wavelength 422.7 nm, bandpass 0.5 nm, and neubilizer uptake 4 s were used). The compositions of the ethanoic millet extracts were determined by the Gas chromatography – Mass spectrometer (Agilent technology 5977 A. with a heating rate of 20°C min-1 from room temperature to 250°C with a 5 min hold time followed by 25°C min-1 until 400°C). The nitrogen content of the millet extracts was evaluated by Kjeldahl digestion method.
RESULTS AND DISCUSSION
Inhibition effect of millet in supersaturated solutions
The dynamics of the CaOx deposition process in the supersaturated solutions were examined by UV-Vis spectroscopy for successively increasing volumes of the millet solution (Figure 1).
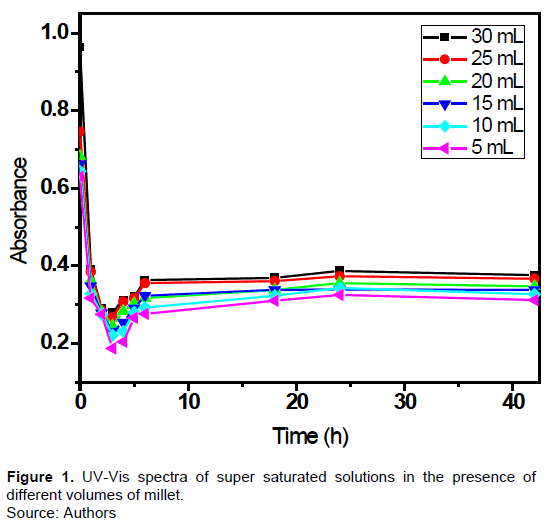
The variation in the UV-Vis peak at 214 nm was correlated to the C2O42- ion concentration in the solution. (Carvalho et al., 2006). The oxalate concentration in solution decreased rapidly at the onset of crystallization for each of the experiments having different volumes of wash solution. Moreover, in each case, the oxalate concentration reached a minimum concentration at some time, and then the C2O42- anion concentration increased slightly to a steady value for several hours. This non-monotonic behavior in the anion concentrations may be due to the establishment of dissolution precipitation equilibrium in the solution after rapid precipitation. The final concentrations of oxalate anion at 40 h were lowest for the smallest, initial wash volume (5 mL) and highest for the largest wash volume (30 mL) indicating that the high millet concentrations have an inhibition effect on CaOx crystallization. The UV- Vis data alone were not sufficient to differentiate the effect of varying millet concentrations on CaOx crystal deposition. To shed light on these crystallization dynamics, the amount of CaOx crystals formed in supersaturated solutions in the presence and absence of millet was measured and is as shown in Figure 2.
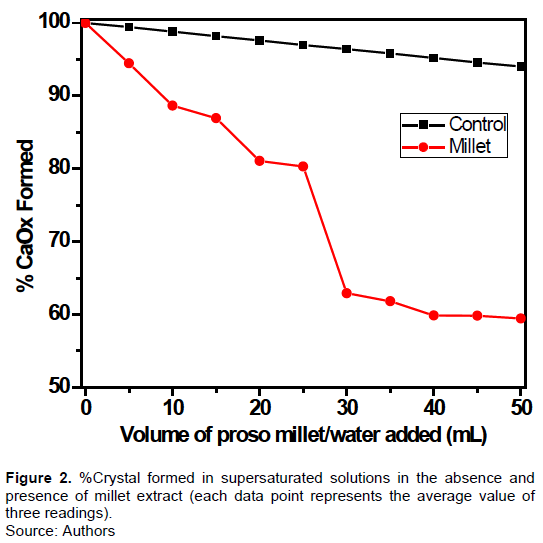
The CaOx precipitation declined with increasing volumes of millet and water. Compared to control experiments, it is obvious that the crystal deposition process is inhibited in the presence of millet. With the addition of the first 5 mL of solutions, nearly 99.4% of crystals precipitated from the control solution; whereas, only 94% of the crystals formed in the millet-treated solution. In a similar fashion, with subsequent aliquots of control and millet in simulated urine solutions, we observed increased inhibition of the formation of oxalate crystals: 98.3% of crystals formed in the control versus 88% of crystals formed in the millet-simulated urine solution with the next 5 mL of wash solutions. Roughly, a stepwise, consistent inhibition effect was observed in the presence and absence of millet (~0.6% for control and presence and absence of millet (~0.6% for control and ~6% for millet-treated experiments for every 5-mL volume increment, respectively) with increasing volumes up to 25 mL. As there was a sudden decrease in the CaOx formation with aliquot showing 30-mL millet volume (80% CaOx in 25 mL vs ~63% CaOx in 30 mL), the millet volume was increased up to 50 mL (Figure 2). After 30 mL millet volumes treated solutions, the crystal formation was not significantly affected by the increased millet volumes showing only 59% with 50 mL millet volume. In all experiments, we used fixed amount of Ca2+ and C2O42- ions. Therefore, based on these observations, it can be concluded that the 30-mL millet extract composed of inhibitors has the maximum inhibition effect. Even though the inhibitor concentration increases, after the addition of 30 mL of millet volumes, only a certain fraction actively participate for slowing down the CaOx precipitation.
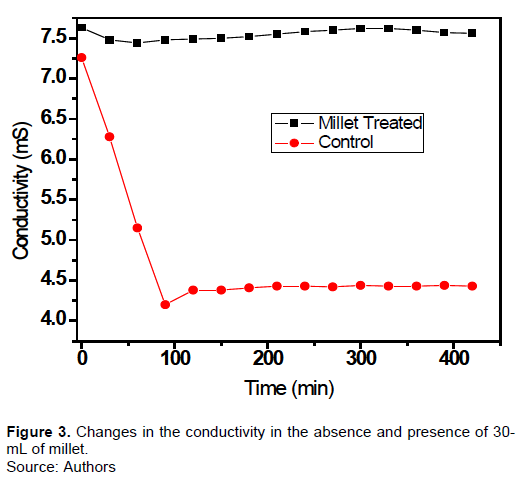
The conductivity of these solutions depends upon the concentration of the ionic species. Figure 3 shows the changes in conductivity of the two solutions in the presence and absence of 5-mL millet solutions. The conductivity of the control sample fell by 38% suggesting that some of the ions were removed from the solution by crystallization. In millet-treated sample, the initial conductivity was slightly higher than that of water-treated sample indicating the presence of ionic species in millet solution, vide infra. We speculate that these chemical species might prevent the formation of CaOx crystals by holding Ca2+ and C2O42- in soluble state.CaOx can be precipitated in three different forms as discussed previously. Therefore, several tests were completed to characterize the as-formed crystals. As the first step, oxidation-reduction titrations (MnO4- vs C2O42-) were conducted to investigate the oxalate content in the precipitates obtained from control and millet-treated experiments. The mean oxalate contents of crystals obtained in the absence and presence of 30-mL millet were 60.45 ± 0.31 and 60.70 ± 0.26%, respectively. Theoretically calculated values for the oxalate contents for CaC2O4.H2O and CaC2O4.2H2O are 60.27 and 53.66%, respectively. Therefore, the C2O42- content in the CaOx precipitate closely matches with CaC2O4.H2O. To investigate any structural differences present in CaOx obtained in control and millet-treated samples, FT-IR, TGA, XRD, and SEM analyses were completed.
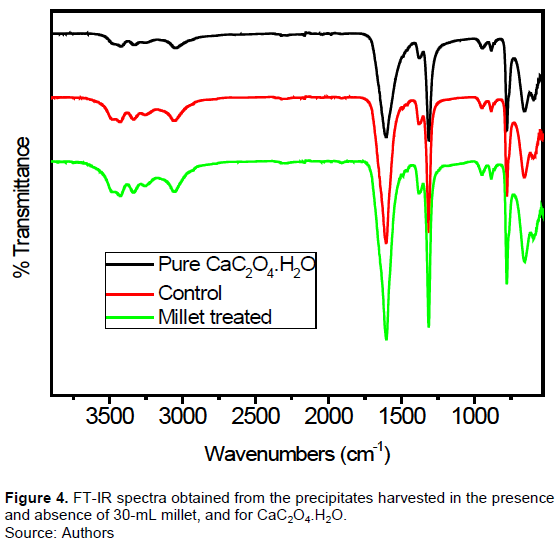
The infrared spectra of CaOx obtained from treating millet and de-ionized water were recorded as shown in Figure 4. The multiple peaks observed in the region of 3000 - 3500 cm-1, are due to stretching of O-H bond in coordinated water. Two strong bands were observed at 1312 and 1605 cm-1 for all samples prepared in the presence and absence of millet. (Carmona et al., 1997). The strong band at 1605 cm-1 is due to the antisymmetric stretching mode of carbonyl group of oxalate. (Maurice-Estepa et al., 2000). The value is slightly shifted from the literature value at 1614 cm-1. The band at ~1312 cm-1 is assigned to the C=O symmetric stretching mode. FT-IR spectroscopy showed spectra obtained from the millet-treated and control samples that were identical to an authentic sample of COM. Most interestingly, absence of additional IR peaks in the millet-treated sample compared to pure authentic COM confirms the association of negligible amount of any other foreign substances other than CaOx in the harvested precipitates during CaOx nucleation, crystal aggregation and crystal growth.
Pure COM was thermally decomposed under stream of air and decomposition kinetic data are depicted in Figure 5. The mechanism of the CaC2O4.H2O thermal decomposition involves three stages as follows. (Frost and Weier, 2004; Qin et al., 2021).
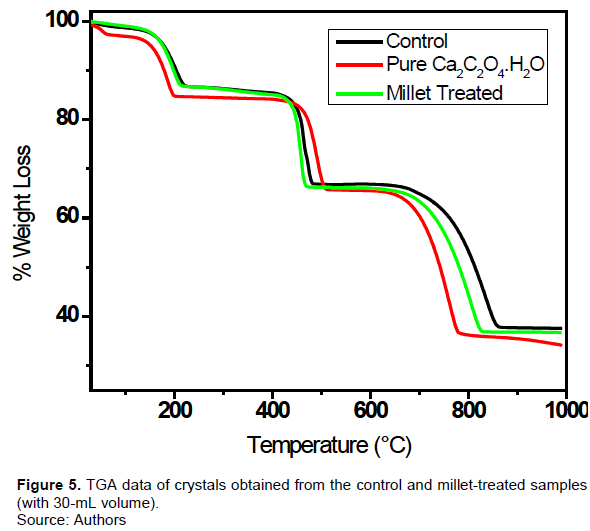
Water treated samples showed the same decomposition kinetic data as pure CaC2O4.H2O. The first weight loss of pure CaC2O4.H2O is 12.30% at 186°C and the value is consistent with the theoretical value of 12.33% as shown in the first equation. The small weight loss observed at 52°C in authentic CaC2O4.H2O is may be due to the physically absorbed water molecules in the CaOx crystals.
The small weight loss at 491°C is due to the oxidation of CO under air sweeping and perfectly agrees with the data reported for COM. The ~44% weight loss expected for the third weight change of the decomposition mechanism was not observed under air sweeping and higher temperatures may be required other than 762°C. In millet-treated samples, the decomposition kinetic data is consistent with three major weight changes. However, slight changes could be identified in each sample. The second weight loss occurs at a slightly lower temperature than that of the pure CaOx crystals (~ 483°C vs ~ 491°C). The last decomposition process seems to be more difficult in the millet-treated sample compared to the pure CaOx crystal as it occurred at 793°C (~ 793°C vs ~ 762°C). CaOx crystals obtained from the control experiments experience further difficulties of the third decomposition. The enthalpy of dehydration is 66.5 kJ/mol attending to the loss of one water molecule from the calcium oxalate monohydrate, reaction (Equation 1).
The enthalpies of reaction for reactions (Equations 2 and 3) are 341 and 178 kJ/mol, respectively (Supplemental Information, Table 2). Notice that all of these reactions are endothermic which implies that the interiors of these crystals will be cooler than the exteriors under the dynamics expected for the DSC experiment. Under the case of heat transfer control, this difference in external/internal temperatures can influence the rate of thermolysis so that the characteristic temperature of the weight loss may be different for oxalate crystals of different sizes.
Crystals harvested in the presence and absence of 30-mL of millet were characterized by powder X-ray diffraction technique (Figure 6). The millet-treated sample showed several intense peaks having 2θ values 15.00, 24.48, 30.20, 36.06, and 38.26° and these peaks correspond to the miller indices of (-101), (020), (-202), (301), and (130) of COM. (Kesavan et al., 2012; Zhao et al., 2014). However, 2θ values of authentic COM and CaOx obtained from the control experiment were slightly shifted. The authentic COM had 2θ values at 14.92, 24.38, 30.12, 35.96, and 38.28°. The CaOx crystals obtained from the control sample showed peaks at 14.92, 24.40, 30.12, 35.96, and 38.30°. These slight changes indicate the possible small differences in the crystal structure of the three samples. XRD data confirms the absence of peaks at 2θ values of 14.32, 20.07, 22.72, 32.23 and 40.17° which resembles the reflections of COD (Zhao et al., 2014).
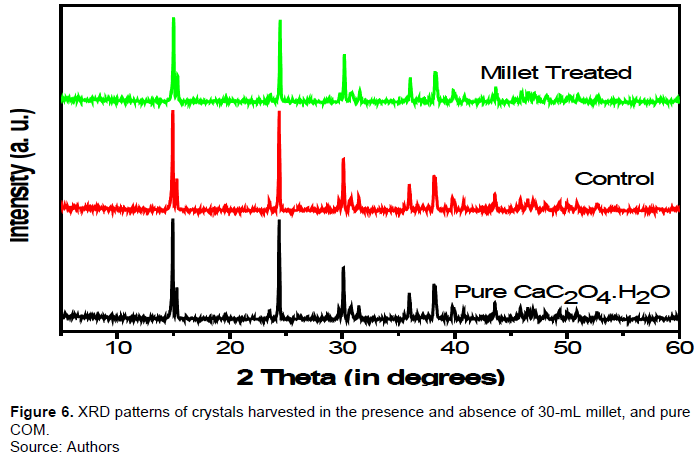
Overall, these data are consistent with the conclusion that the obtained crystals do not contain many impurities, however, there may be some slight changes in the crystal structure of the CaOx obtained from millet-treated samples. In order to investigate this hypothesis, SEM images were recorded for crystals obtained in the presence and absence of millet and compared them with pure COM.
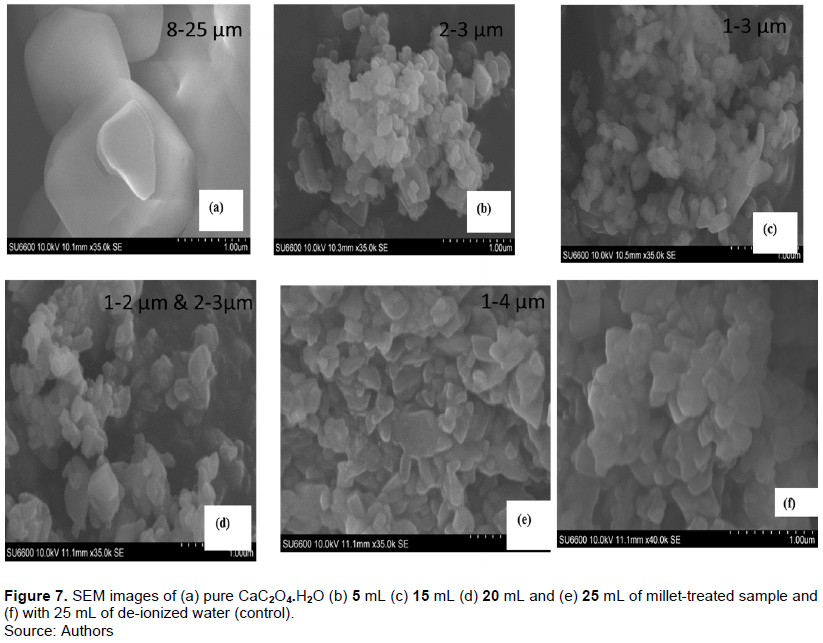
SEM images of authentic samples showing calcium oxalate-monohydrate (dumbell-shaped), and erythrocytes (circular) are as shown in Figure 7. Figure 7a is our data for the SEM of pure COM which demonstrates the characteristic dumbell shape (> 1 µm). Figure 7b-e shows the crystals harvested after treatment with 5, 15, 20, and 25 mL of millet-treated solutions. The sizes of the crystals are as follows: (b) 2-3 µm; (c) 1-3 µm; (d) 1-3 µm; 2-3 µm; (e) 1-4 µm. We observed other features in the SEM that were not dumbbell shaped. The detailed investigations of the precipitates harvested by treating 5 and 15 mL of millet extract showed small crystallites which are sitting on the top of the precipitates. The size of those particles was ~1 μm. Relatively large, aggregated, plate like crystallites having sizes 2-3 μm, can be visible underneath those small particles. The crystals collected by treating 20 mL of millet extract still exhibits some of those small particles but the amount is less. With the highest millet concentrations, those small particles are almost absent whereas the bottom layer of crystals are clearly visible which contain inter connected, 2-3 μm size plates. We propose two hypotheses to explain these morphology habits. The first hypothesis is that with increasing millet concentrations, precipitation of the top layer of crystals with relatively small crystals is stopped by the inhibitors present in millet. The second hypothesis is that the small crystallites are still formed in high millet concentrations and those small particles are then dissolved in the millet solution by chemolysis. We conclude that the second hypothesis is in operation under supersaturated conditions as the evidences provided by the conductivity measurements. As shown in Figure 3, the conductivity of the solution declined during the first 100 min and then gradually increased until 400 min due to the dissolution of precipitated CaOx crystals. The initial declined in the conductivity suggests the formation of both large and small crystallites whereas the later increasing values of conductivity is consistent with the dissolution of probably the small crystallites. In the control sample (Figure 7f), most of the small particles are absent due to the absence of either promoters or inhibitors. In control sample, CaOx particles stick together to form relatively large crystallites suggesting the occurrence of aggregation and growth of CaOx. In comparison, shapes of the pure CaOx crystals are different from the morphology habits observed for millet-treated samples. In millet-treated samples, the particle sizes of CaOx crystals are small due to poor aggregation which is caused by the inhibitors present in the millet extract. These results confirm that the crystals obtained from inhibition experiments are identical to that of pure COM crystals.
Dissolution effect of millet
CaOx crystals were dissolved in deionized water as well as in millet (Figure 8). In control experiments, the mass of CaOx crystals decreased almost linearly with each washing. This is mainly due to the dissolution of constant amount of CaOx crystals in 300 mL of fresh de-ionized water. In contrast, there was a rapid dissolution effect upon washing with millet extract.
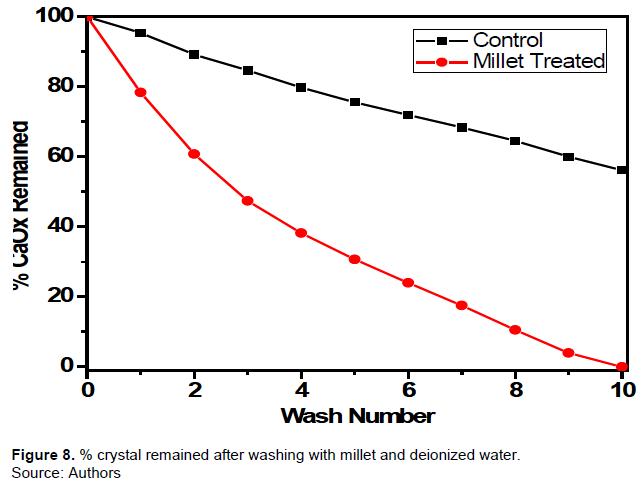
Initial washings with millet extracts showed rapid dissolution of COM crystals, however, with subsequent washing steps, the dissolution rate decreased. After ten days of washings, almost 0% of CaOx crystals remained in the millet-treated sample whereas about 56 wt% of CaOx crystals remained in the control wash. These data clearly indicate that millet has a promising dissolution effect on CaOx crystals and it could be a potential remedy to cure CaOx stones in patients who are suffering from kidney stones.
To support this enhanced dissolution effect of millet, the electrical conductivity of the solution was recorded for the first 8 h. These data are reported in Figure 9. In these experiments, 0.2002 and 0.2004 g of CaOx crystals were dissolved separately in 300 mL of water and millet, respectively.
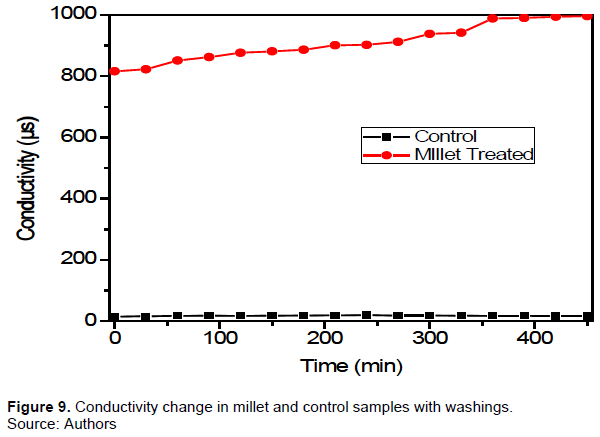
In control experiments, the conductivity increased until 240 min (15 μS at t = 0 and 19 μS at t = 240 min) and then slowly decreased until 450 min (16.4 μS at 450 min). No linear relationship was observed in the incline or decline process from the control experiment until 240 min, where Ca2+ and C2O42- start to precipitate and tends to reach a dynamic equilibrium. In contrast, initial conductivity in the millet extract treated sample was greater by few orders of magnitude due to the presenceof large amount of ionic species in the millet solution (300 mL). Furthermore, the conductivity of the solution increased continuously up to 450 min (816 μS at t = 0 and 996 μS at t = 450 min). This suggests that CaOx crystals continuously dissolve in the millet solution even until 450 min.
Inhibition effect of millet in synthetic urine
The inhibition effect and the dissolution effect of millet extract on CaOx crystals are quite fascinating in aqueous medium; we wanted to determine if this behavior observed in vitro could be observed in solutions that mimic in vivo systems. Accordingly, we report in Figure 10 the behavior of millet on crystal deposition in synthetic urine.
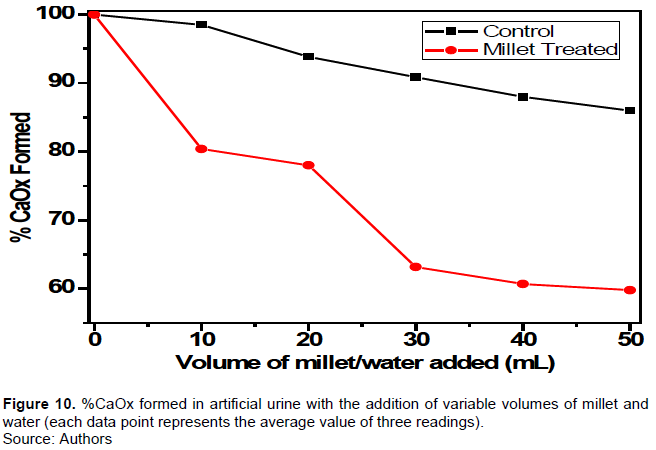
Both in millet-treated and control experiments, the %CaOx crystal formation were declined with the volume added. Addition of 10-mL volume increments to the control samples, ~ 3% decrease was observed. Approximately, ~10% decrease was observed in millet-treated samples. As shown by the graph in Figure 10, millet extract is effective in preventing the formation of CaOx crystals in artificial urine. An interesting inhibition effect was observed when the volumes of the millet extract change from 20 to 30 mL which is consistent with the previous observations reported under supersaturated conditions. The inhibition effect of millet is 25% greater in millet-treated sample in contrast to control experiment (50 mL millet extract vs 50 mL of deionized water). The formed crystals under artificial urine were also characterized by FT-IR, TGA, and SEM. The collected data were identical to those data that were observed for pure COM crystals (Figures S-1 to S-4 in supplementary information). Based on experimental data reported so far, it is noteworthy to accept that the fact that the millet extract has a noticeable effect on preventing the formation of CaOx crystals as well as dissolving calcium stones even under synthetic urine condition.
Dissolution effect of millet on actual kidney stones
Since millet showed a significant inhibition and dissolution effect on CaOx crystals at high supersaturation levels, dissolution experiments were extended to using actual CaOx kidney stones collected from the general hospital in Colombo, Sri Lanka. The stones and artificial urine solution were added to a 300-mL millet solution which was maintained at 37.5°C under static condition for 6 h. Then the solution was filtered and calcium stones were collected, dried overnight at 105°C and weighed. Likewise, the stone was washed seven times with 300-mL portions of millet and we found ~20 wt% of the stone dissolution (by weight, Figure 11).Initially, there was a rapid dissolution and later, the dissolution rate slowed down with subsequent washings similar to what was observed for authentic Ca2C2O4.H2O crystals dissolution.
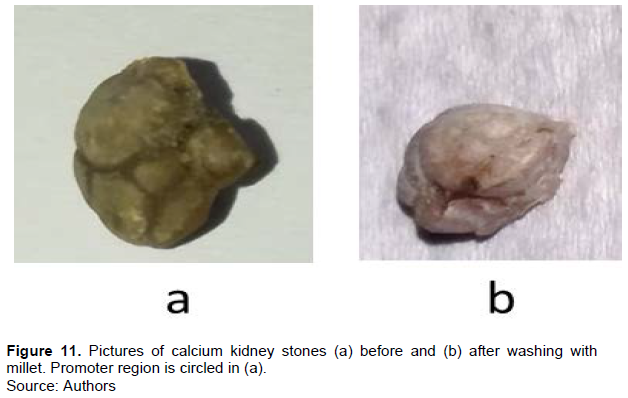
In typical bio mineralization, the stone formation occurs through the attachment of preformed microcrystals onto a surface of an existing stone or onto cell debris which act as a promoter region for the crystal growth. In Figure 11a, we identified the promoter region which is marked with a circle. With subsequent washings, this promoter region disappeared and as a result, the stone was dissolved. The wash solution confirms the presence of Ca2+ and C2O42- ions; as a result, we propose that these ions may have originated from the surface of existing small stones.
The data shown here provide convincing evidence that chemicals present in the millet, either singly or in concert, are effective in suppressing the precipitation of CaOx from supersaturated solutions in the presence of a synthetic urine solution. Moreover, these chemicals under the same conditions are even more effective for dissolving COM crystals. Both tests were conducted in the presence of a control wash solution: deionized water. The chemical composition of proso millet has been evaluated extensively Sun et al., (2018). However, to understand the mechanism of millet on COM dissolution and inhibition, a complete investigation was carried out to reveal the chemical composition of the aqueous extract of millet. Data obtained from AAS studies showed that the millet extract contains Mg (49 ppm), Ca (<0.1 ppm), K (26 ppm), Na (2 ppm), and PO43- (3 ppm). GC-MS analysis showed the presence of 1-2-dibenenedicarboxylic di-iso-octyl ester, 9,12-octadecadienoic acid, and botulin as major compounds in an ethanoic extract of millet. The other possibility is that the hydrolysis of 1,2-benzenedicarboxylic acid, di-iso-octyl ester in the solution providing 1,2-benzene dicarboxylic acid which can chelate with calcium as HCl was added to adjust the pH of the solutions. Nitrogen analysis of the same aqueous extract showed protein (~5.5% by weight) and main amino acids present in proso millet were Leucine, aspartic acid, glutamic acid, and proline acid (Baptist and Perera, 2007; Sun et al., 2018).
Magnesium ions form a water-soluble complex with oxalate ions (vide supra), thus preventing CaOx complexation under sufficiently high concentrations of added Mg cations. To investigate this effect, supersaturated solutions were incubated with 10 to 50 ppm magnesium solutions and we observed a negligible effect on the mass of the precipitate as ksp value of magnesium oxalate is higher than the calcium oxalate. As a result, we concluded that magnesium ions do not contribute to reduce the mass of CaOx precipitates. Next, we turn our attention to the organic acids found in millet extract. Organic acids are macromolecules which act as molecular modifiers to inhibit the CaOx formation in supersaturated solutions. The role of organic acids is to attach on to the crystal surface and thereby induce the crystal dissolution without affecting the rate of crystal growth. The dissolution results in the formation of water-soluble organic acid-calcium salts. According to recent findings, the role of organic acids on CaOx dissolution is different from the conventional mechanisms. Surface energy of the crystal surface changes as organic acids adsorb onto the terrace or step. When the solute-crystal interactions are in a less favorable condition with respect to organic acid-crystal surface interactions, the absorbed organic acids then creates a localized strain on the CaOx lattice surface (vide supra). As a result, the step or the terrace dissolve to release calcium and oxalate ions and to expose the inner surface for crystal-inhibitor interactions. In a similar fashion, the CaOx crystal dissolution takes place in the super saturated and artificial urine circumstances. Organic acids act as agents to bind with Ca2+ ions in the solution, thus, suppress the number of Ca2+ ions available to bind with oxalate ions.
It is possible that the proteins in the millet extract inhibit the nucleation and aggregation and growth of CaOx crystals from the supersaturated solutions. For example, urinary proteins have been functioning as inhibitors for CaOx crystallization. Proteins with anionic functional groups such as aspartic acid and glutamic acid, have shown significant reduction in CaOx crystal formation. (Jung et al., 2004; Qiu et al., 2004; Taller et al., 2007). Osteopontin, which is rich in aspartic acid, is known to suppress the CaOx crystal formation. (Grohe et al., 2007; Thurgood et al., 2010; Wesson et al., 2003). Especially, aspartic and glutamic acids containing proteins have shown dual role on CaOx crystallization acting as an inhibitor at low concentrations and as a promoter in high concentrations. The individual effect of these proteins mainly depends on the pH and ionic strength of the growth solution, and inhibitor concentrations (Farmanesh et al., 2014). In artificial and urinary solutions, acidic groups, e.g. carboxylic groups in proteins, directly interacting with Ca2+ ions on the crystal surfaces to form calcium bridges through (crystal)COO-….Ca2+…..-OOC-(protein) cationic groups of the protein interact with the negatively charged oxalate groups on the surface to form (crystal)COO-….+H3N(protein), however, surface Ca2+ ions generate repulsive forces as the interactions are Ca2+……+H3N(protein) type. Furthermore, large macromolecules in the millet solutions prevent the direct interaction between calcium and oxalate ions. The crystal growth is also inhibited due to the presence of limited interactions of those kinds.
It was claimed that these findings are important in several aspects. First, the net dissolution effect of millet on CaOx stones in artificial urine is encouraging for exploring the possible use of millet to treat CaOx kidney stones. This study reports the activity of millet in very high level of supersaturated solutions but the actual concentrations of Ca2+ and C2O42- ions in human urine are comparatively very low. That means, millet may have an enhanced inhibition effect in actual urine. Second, the depletion of growth regions in actual kidney stones may prevent the initial crystal nucleation on cell debris as well as adherence to the epithelial cell lining during crystal growth. Millet would also reduce the size of the relatively large calcium stones as an irrigation solution making them prone to pass with urine which may eliminate the expensive medical procedures such as shock wave lithotripsy or surgical removals. The inhibition effect of millet could suppress the reoccurrence of calcium stones when they are properly washed with millet solution. However, more clinical work is necessary to understand the actual effect of millet on calcium stones as the actual mechanism is still poorly understood in the human body (Xie et al., 2015).
CONCLUSIONS
Successfully, we have demonstrated the influence of millet extract on CaOx crystal formation and dissolution. Our data clearly support the fact that the CaOx crystal formation is inhibited by the action of several inhibitors present in millet. The net CaOx precipitation was declined by ~34% in supersaturated solution and by ~25% in synthetic urine. Our characterization protocols confirmed the identity of formed crystals as thermodynamically more stable COM. The millet extract has also influenced the crystal habits and morphological characteristics of COM crystals formed. In the presence of millet, the formed COM crystals were relatively small due to poor aggregation and crystal growth whereas in the absence of millet, COM particles grew bigger showing aggregation of small crystals into clusters. The millet extract is capable of dissolving actual CaOx stones as we found ~20% weight loss with seven washings. Although it is not possible to draw definite conclusions on how individual inhibitors in millet act on CaOx formation and dissolution, we propose the most effective dissolution and inhibition protocols combine several active agents present in millet.
To sum up, we report that the overall dissolution and inhibition activity of millet on CaOx and calcium stones mainly arises by the action of organic acids and proteins present in millet. In order to understand the detailed mechanism, active compounds should be separated and treated individually under the same condition and it is out of this scope.
CONFLICT OF INTERESTS
The authors have declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors thank Dr. Asitha T. Cooray and the Department of Chemistry, University of Sri Jayewardenepura, Sri Lanka for providing the facilities to collect IR data.
REFERENCES
|
Atmani F, Farell G, Lieske JC (2004). Extract from Herniaria Hirsuta Coats Calcium oxalate monohydrate crystals and blocks their adhesion to renal epithelial cells. Journal of Urology 172:1510-1514. |
|
|
Ahmed AA, Al-sayed AS (2010). Tamsulosin versus Alfuzosin in the Treatment of Patients with Distal Ureteral Stones: Prospective, Randomized, Comparative Study. Korean Journal of Urology 51:193-197. |
|
|
Alok S, Jain SK, Verma A, Kumar M, Sabharwal M (2013). Pathophysiology of kidney, gallbladder and urinary stones treatment with herbal and allopathic medicine: A review. Asian Pacific Journal of Tropical Disease 3:496-504. |
|
|
Baptist NG, Perera BPM (2007). Essential amino-acids of some tropical cereal millets. British Journal of Nutrition, 10:334-337. |
|
|
Basavaraj DR, Biyani CS, Browning AJ, Cartledge J J (2007). The Role of Urinary Kidney Stone Inhibitors and Promoters in the Pathogenesis of Calcium Containing Renal Stones. EAU-EBU 5:126-136. |
|
|
Batinic D, Milos?evic' D, Blau N, Konjevoda P, Sÿtambuk N, Barbaric' V, Sÿubat-Dez?ulovic' M, Votava-Raic' A, Niz?ic' L, Vrljic?ak K (2000). Value of the Urinary Stone Promoters/Inhibitors Ratios in the Estimation of the Risk of Urolithiasis. Journal of Chemical Information and Computer Sciences 40(3):607-610. |
|
|
Bouropoulos N, Weiner S, Addadi L (2001). Calcium Oxalate Crystals in Tomato and Tobacco Plants: Morphology and in Vitro Interactions of Crystal-Associated Macromolecules. Chemistry-A European Journal 7(9):1881-1888. |
|
|
Carmona P, Bellanato J, Escolar E (1997). Infrared and Raman spectroscopy of urinary calculi: A review. Biospectroscopy 3(5):331-346. |
|
|
Carvalho M, Lulich JP, Osborne CA, Nakagawa Y (2006). Defective urinary crystallization inhibition and urinary stone formation. Investigative Urology 32:342-349. |
|
|
Chitme HR, Alok S, Jain SK, Sabharwal M (2010). Herbal treatment for urinary stones. International Journal of Pharmaceutical Sciences and Research 1(2):24-31. |
|
|
Chung J, Granja I, Taylor MG, Mpourmpakis G, Asplin JR, Rimer JD (2016). Molecular modifiers reveal a mechanism of pathological crystal growth inhibition. Nature 536:446-450. |
|
|
Chutipongtanate S, Chaiyarit S, Thongboonkerd V (2012). Citrate, not phosphate, can dissolve calcium oxalate monohydrate crystals and detach these crystals from renal tubular cells. European journal of pharmacology 689(1-3):219-225. |
|
|
Das P, Gupta G, Velu V, Awasthi R, Dua K, Malipeddi H (2017). Formation of struvite urinary stones and approaches towards the inhibition-A review. Biomedicine and Pharmacotherapy 96:361-370, |
|
|
De Sio M, Autorino RDLG (2006). Medical Expulsive Treatment of Distal-Ureteral Stones Using Tamsulosin: A Single-Center Experience. Journal of Endourology 20(1):12-16. |
|
|
Evan AL, Coe FL, Worcester E (2019. Dual Roles of Melamine in the Formation of Calcium Oxalate Stones. Crystal Growth and Design 19(7):3998-4007. |
|
|
Farmanesh S, Chung J, Sosa RD, Kwak JH, Karande P, Rimer JD (2014). Natural Promoters of Calcium Oxalate Monohydrate Crystallization. Journal of American Chemical Society 136(36):12648-12657. |
|
|
Fischer VL, Mun?oz-Espí RM (2011). Inorganic nanoparticles prepared in miniemulsion. Crystal Growth and Design 1:1880-1890. |
|
|
Fostvedt GA, Barnes RW (1963). Complications During Lavage Therapy for Renal Calculi. Journal of Urology 89(3):329-331. |
|
|
Franceschi VR, Nakata PA (2005). CALCIUM OXALATE IN PLANTS: Formation and Function. Annual Review of Plant Biology 56:41-71. |
|
|
Frost RL, Weier ML (2004). Thermal treatment of whewellite-a thermal analysis and Raman spectroscopic study. Thermochimica Acta 409(1):79-85. |
|
|
Geervani P, Eggum BO (1989). Nutrient composition and protein quality of minor millets. Plant Foods for Human Nutrition 39:201-208. |
|
|
Ghodsizad G, Safekordi AA (2012). Oil Extraction from Millet Seed -Chemical Evaluation of Extracted Oil. Journal of Food Biosciences and Technology 2:71-76. |
|
|
Golzari SE, Soleimanpour H, Rahmani F, Zamani Mehr N, Safari S, Heshmat Y, Bakhtavar, HE (2014). Therapeutic Approaches for Renal Colic in the Emergency Department: A Review Article. Anesthesiology Pain Medicine 4:e16222. |
|
|
Gonzalez RD, Whiting BM, Canales BK (2012). The History of Kidney Stone Dissolution Therapy: 50 Years of Optimism and Frustration with Renacidin. Journal of Endourology 26(2):110-118.. |
|
|
Gravina GL, Costa AM, Ronchi P, Galatioto GP, Angelucci A, Castellani D, Narcisi F, Vicentini C (2005).Tamsulosin treatment increases clinical success rate of single extracorporeal shock wave lithotripsy of renal stones. Urology 66(1):24-8. |
|
|
Grohe B, O'Young J, Ionescu DA, Lajoie G, Rogers KA, Karttunen M, Goldberg HA, Hunter GK (2007) Control of calcium oxalate crystal growth by face-specific adsorption of an osteopontin phosphopeptide. Journal of the American Chemical Society 129(48):14946-51. |
|
|
Gul Z, Monga M (2014). Medical and Dietary Therapy for Kidney Stone Prevention. Korean Journal of Urology 55(12):775-779. |
|
|
Himani B, Seema B, Bhole N, Mayank Y, Vinod S, Mamta S (2013). Misai kuching: A glimpse of maestro. International Journal of Pharmaceutical Sciences Review and Research 22(2):55-59. |
|
|
Ibis F, Dhand P, Suleymanli S, Heijden AEDMV, Kramer HJM, Eral HB (2020). A Combined Experimental and Modelling Study on Solubility of Calcium Oxalate Monohydrate at Physiologically Relevant pH and Temperatures. Crystals 10(10):924. |
|
|
Jung T, Sheng X, Choi CK, Kim WS, Wesson JA, Ward MD (2004). Probing Crystallization of Calcium Oxalate Monohydrate and the Role of Macromolecule Additives with in Situ Atomic Force Microscopy. Langmuir 20(20):8587-8596. |
|
|
Junuzovic D, Prstojevic JK, Hasanbegovic M, Lepara Z (2014). Evaluation of Extracorporeal Shock Wave Lithotripsy (ESWL): Efficacy in Treatment of Urinary System Stones. Acta Informatica Medica 22(5):309. |
|
|
Kalinova J, Moudry J (2006). Content and quality of protein in proso millet (Panicum miliaceum L.) varieties. Plant Foods for Human Nutrition 61(1):43-47. |
|
|
Kesavan M, Kaliaperumal R, Eevera T, Shanmugam K (2012). In vitro evaluation of calcium oxalate monohydrate crystals influenced by Costus igneus aqueous extract. Scand. Scandinavian Journal of urology and nephrology 46(4):290-297. |
|
|
Lipkin M, Shah O (2006). The Use of Alpha-Blockers for the Treatment of Nephrolithiasis. Reviews in Urology 8(Suppl 4):S35. |
|
|
Manzoor MAP, Mujeeburahiman M, Duwal SR, Rekha PD (2019). Investigation on growth and morphology of in vitro generated struvite crystals. Biocatalysis and Agricultural Biotechnolgy 17:566-570 |
|
|
Maurice-Estepa L, Levillain P, Lacour B, Daudon M (2000). Advantage of zero-crossing-point first-derivative spectrophotometry for the quantification of calcium oxalate crystalline phases by infrared spectrophotometry. Clinica Chimica Acta 298:1-11. |
|
|
Miyake O, Yoshimura K, Yoshioka T, Koide T, Okuyama A (1998). High urinary excretion level of citrate and magnesium in children: potential etiology for the reduced incidence of pediatric urolithiasis. Urological Research 26:209-213. |
|
|
Moe OW (2006). Kidney stones: pathophysiology and medical management. Lancet 367:333-44. |
|
|
Ouyang JM, Duan L, Tieke B (2003). Effects of Carboxylic Acids on the Crystal Growth of Calcium Oxalate Nanoparticles in Lecithin−Water Liposome Systems. Langmuir 19(21):8980-8985. |
|
|
Peng H, Ouyang JM, Yao XQ, Yang RE (2012). Interaction between submicron COD crystals and renal epithelial cells. International Journal of Nanomedicine pp. 4727-4737. |
|
|
Phillips R, Hanchanale VS, Myatt A, Somani B, Nabi G, Biyani CS (2015). Citrate salts forpreventing and treating calcium containing kidney stones in adults. Cochrane Database of Systematic Reviews (10):1-42. [CD010057]. |
|
|
Polat S, Eral HB (2021). Elucidating the role of hyaluronic acid in the structure and morphology of calcium oxalate crystals. Advanced Powder Technology 32(10):3650-3659. |
|
|
Polat S, Eral HB (2022). Effect of hyaluronic acid on the struvite crystallization: A structural, morphological, and thermal analysis study. Journal of Crystal Growth 592:126734 |
|
|
Porpiglia F, Ghignone G, Fiori C, et al. (2004). Nifedipine Versus Tamsulosin for the management of Lower Ureteral Stones. Journal of Urology 172(2):568-571. |
|
|
Qin L, Putnis CV, Wang L (2021). Facet-Specific Dissolution-Precipitation at Struvite-Water Interfaces. Crystal Growth and Design 21(7):4111-4120. |
|
|
Qiu SR, Wierzbicki A, Orme CA, Cody AM, Hoyer JR, Nancollas GH, Zepeda S, De Yoreo JJ (2004). Molecular modulation of calcium oxalate crystallization by osteopontin and citrate. Proceedings of the National Academy of Sciences 101(7):1811-1815. |
|
|
Qiu SR, Wierzbicki A, Salter EA, Zepeda S, Orme CA, Hoyer JR, Nancollas GH, Cody AM, De Yoreo JJ (2005). Modulation of Calcium Oxalate Monohydrate Crystallization by Citrate through Selective Binding to Atomic Steps. Journal of American Chemical Society 127(25):9036-9044. |
|
|
Resim S, Ekerbicer H, Ciftci A (2005). Effect of tamsulosin on the number and intensity of ureteral colic in patients with lower ureteral calculus. International journal of urology 12(7):615-620. |
|
|
Sakhaee K (2009). Recent advances in the pathophysiology of nephrolithiasis. Kidney international 75(6):585-595. |
|
|
Scales Jr, CD, Smith AC, Hanley JM, Saigal CS, Urologic Diseases in America Project (2012). Prevalence of kidney stones in the United States. European urology 62(1):160-165. |
|
|
Segura JW, Preminger GM, Assimos DG (1997). Ureteral Stones Clinical Guidelines Panel Summery Report on the Management of Ureteral Calculi. The Journal of urology 158(5):1915-1921. |
|
|
Sheng XX, Ward MD, Wesson JA (2003). Adhesion between Molecules and Calcium Oxalate Crystals: Critical Interactions in Kidney Stone Formation. Journal of the American Chemical Society 125(10):2854-2855. |
|
|
Sun X, Zhang C, Bhadja P, Ouyang J (2018). Preparation, properties, formation mechanisms, and cytotoxicity of calcium oxalate monohydrate with various morphologies. Crystal Engineering Communication 20(1):75-87. |
|
|
Taller A, Grohe B, Rogers KA, Goldberg HA, Hunter GK (2007). Specific Adsorption of Osteopontin and Synthetic Polypeptides to Calcium Oxalate Monohydrate Crystals. Biophysical Journal 93(5):1768-1777. |
|
|
Tang R, Nancollas GH, Giocondi JL, Hoyer JR, Orme CA (2006). Dual roles of brushite crystals in calcium oxalate crystallization provide physicochemical mechanisms underlying renal stone formation. Kidney international, 70(1):71-78. |
|
|
Thurgood LA, Cook AF, Sorensen ES, Ryall RL (2010). Face-specific incorporation of osteopontin into urinary and inorganic calcium oxalate monohydrate and dihydrate crystals. Urological research 38:357-376. |
|
|
Wesson JA, Johnson RJ, Mazzali M, Beshensky AM, Stietz S, Giachelli C, Liaw L, Alpers CE, Couser WG, Kleinman JG, Hughes J (2003). Osteopontin is a critical inhibitor of calcium oxalate crystal formation and retention in renal tubules. Journal of the American Society of Nephrology 14(1):139-147. |
|
|
Wesson JA, Word MD (2007). Pathological Bio-mineralization of Kidney Stones. Elements 3(6):415-421. |
|
|
Xie B, Halter TJ, Borah BM, Nancollas GH (2015). Aggregation of Calcium Phosphate and Oxalate Phases in the Formation of Renal Stones. Crystal growth and design 15(1):204-211. |
|
|
Zhao Z, Xia Y, Xue J, Wu Q (2014). Role of E. coli-Secretion and Melamine in Selective Formation of CaC2O4•H2O and CaC2O4•2H2O Crystals. Crystal growth and design 14(2):450-458. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


