Full Length Research Paper

ABSTRACT
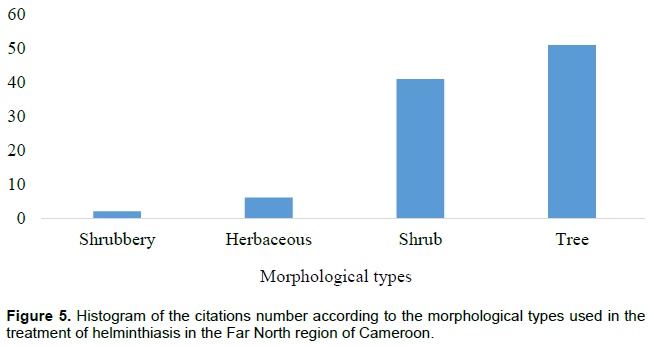
Despite the multitude of studies which have shown the use of medicinal plants in the management of parasitic diseases, little data was available on the plants used against onchocerciasis. Ethnobotanical surveys were carried out among traditional healers in the Far North region of Cameroon. Studies were conducted from July 2017 to May 2018 through direct interviews using a semi-structured questionnaire taking into consideration the socio-demographic characteristics of the respondents as well as their knowledge in the art of onchocerciasis and parasitic infections treatment using plant recipes. A total of one hundred people were interviewed in villages found in the Far North region of Cameroon: 43 were females and 57 males, among which, 71 were recognized as traditional healers. Adults were the most represented (71 respondents). The study identified 96 plant species belonging to 49 genera divided into 29 families among which the most represented was the Fabaceae (20 quotes). The most represented biotope was savannah (98%) and trees (51) were the most used followed by shrub (41). The leaves (40) are the organs which are mostly demanded and the main preparation method is a decoction (69) and 36 diseases and / or symptoms related to onchocerciasis and helminthiases were recorded. The medicinal plants identified, constitute an undeniable asset and a good database for the biological screening of plant-based antiparasitic molecules, which can lead to the manufacture of improved traditional medicines.
Key words: Onchocerciasis, medicinal plants, ethnobotanical surveys, filariasis, Cameroon.
INTRODUCTION
Parasitic diseases are a significant source of threat to human and animal health and, these include helminthiasis caused by parasitic nematode worms also called helminths. These nematodes are a major public health problem in developing countries and affecting approximately two billion people worldwide (WHO, 2017). These infestations are prevalent mainly in deprived areas of the globe, especially in tropical and intertropical areas (Molyneux et al., 2003). They promote growth of poverty rate, thereby compromising child survival and weakening the working population (WHO, 2015). Among these helminthiases are, filariasis which are parasitic infections caused by nematodes. They constitute significant obstacles to the development of underdeveloped and developing countries, in the tropics and particularly in sub-Saharan Africa (Fenwick, 2012). These neglected tropical diseases do not receive as much attention as other endemic diseases, yet they have afflicted mankind for centuries (WHO, 2017). An estimated 1 billion people are at risk of contracting filariasis and about 120 million individuals are infected with filariasis in 73 countries, predominantly in African countries (Marlieke et al., 2006; Hartman et al., 2011). Among these filariasis, there is onchocerciasis, a disease to which more than 90 million people are exposed (Turner et al., 2010). Onchocerciasis is a filariasis caused by Onchocerca volvulus, a parasitic nematode of the family Onchocercidae (Despommier et al., 1995; Magdi, 2006). It is transmitted by the bite of a blood-sucking black fly belonging to the genus Simulium which lives near fast-flowing rivers (Basanez et al., 2008; WHO, 2017). Over 120 million people worldwide are at risk of onchocerciasis, approximately 37 million are infected, 270,000 who are blind and 6.5 million suffer from skin damage (Eze and Malau, 2011; WHO, 2017).
In Cameroon, onchocerciasis is endemic in the ten regions with variable endemicity rates (Zoure et al., 2014). An estimated 10 million people are at risk and 7 million case were reported in which 32,000 are blind and 1.5 million suffer from complications due to the disease (Eze and Malau, 2011). The treatment of onchocerciasis is compromised by the multiple resistances to reference anthelmintics. In recent decades, onchocerciasis has caused economic losses of more than $ 30 million a year due to the abdication of cultivated land in the fertile valleys and the unavailability or absence of work (WHO, 2015). In fact, due to the nuisance of flies and disease, populations are obliged to desert endemic areas which are generally areas with high agricultural potential. The main consequence of this migration is a shortfall in the national economy through a weakening of the agricultural sector. As a result, several means of control have been considered in order to eradicate this disease, such as vector control, nodulectomy and chemotherapy. Currently, Levamisole® and Ivermectin® are the only conventional drugs to control onchocerciasis. Unfortunately, Ivermectin® is only microfilaricide and as the numerous harmful side effects such as asthenia, ataxia, abdominal pain, anorexia, constipation, diarrhea, nausea, vomiting, drowsiness, dizziness, tremors and leukopenia (Borsboom et al., 2003). In addition, after several years of treatment, there is an emergence of resistance as well as a re-invasion of the microfilariae in the treated patients (Kamgno et al., 2008; Tanya et al., 2013). To face problems of chemoresistance of parasites, limited innovations in onchocerciasis therapy, low therapeutic coverage and hotspots, limited funding in the fight, the need to develop new effective and well tolerated anthelmintics is not only important but urgent. Fortunately, traditional medicine could serve as a support given since 75 to 80% of the populations of the developing countries depend closely on the preparations based on local medicinal plants (Adjanohoun, 2000; Dibong et al., 2015); on the other hand, at least 25% of modern medicines derive directly or indirectly from medicinal plants, mainly thanks to the application of modern technologies to traditional knowledge (Biyiti et al., 2004). This interest in traditional medicine and more specifically in medicinal plants has led to ethnobotanical investigations which have proven to be one of the most reliable approaches for the discovery of new drugs (Koné, 2009). Through ethnobotanical studies, many plants have been identified around the world as being useful against onchocerciasis and helminthiasis (Benlamdini et al., 2014; Ndjonka et al., 2018). In Cameroon, although the flora is rich in medicinal plant species, very few investigations to record the use of plants against onchocerciasis have been carried out so far (Ndjonka et al., 2018). The treatment of onchocerciasis remains a big challenge, however, the secondary metabolites of plants have shown a greater and more rapid action than generic drugs in the treatment of many parasitic diseases in general and onchocerciasis in particular (Sereme et al., 2008; Ndjonka et al., 2018). The present study aimed to identify the plants and recipes used against onchocerciasis by the population of the far north region of Cameroon.
MATERIALS AND METHODS
Study site
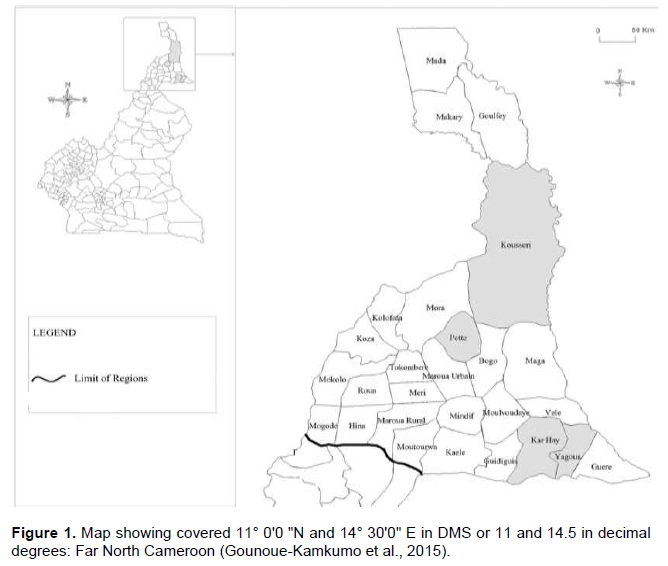
Figure 1 indicates the region covered in this study. Several factors contributed to the choice of the syrupy sites in the Far North region which is the most populated region, border of Chad and Nigeria with an area of 34,263 km², it has 6 departments, Diamaré, Logone-et-Chari, Mayo-Danay, Mayo-Kani, MayoSava, Mayo-Tsanaga with a population of 3.993 million with a density of 91 inhabitants/km. The study was carried out in the Sudano Sahelian zone with reported high endemicity of onchocerciasis and filariaris (WHO, 2016). Another reason for the choice of the study area is the distribution of the vector of the disease that lives around the rivers, this disease is also called river blindness (Demanou et al., 2003).
Survey methods
The ethnobotanical survey was carried out with practitioners of traditional medicine in the Far North region of Cameroon. They were made by direct interviews using a semi structured questionnaire. The interviewees were to give all the information related to medicinal plants directed against parasitic infections in general and onchocerciasis in particular. These surveys were prospective and cross-sectional study; they were conducted from July 2017 to May 2018. The main lines of the interview concerned on one hand, the socio-demographic characteristics of the respondents (region of origin, sex, age, ethnicity, profession and experience) and on the other hand, information on the plants used in the recipes of medicinal preparations used against onchocerciasis (symptoms and/or manifestations) and parasitic infections in general (the local name, the scientific name, the family, the provenance, the biotope, the harvest period and method, the plant parts used, the morphological type, the methods of preparation of the recipes, the methods of administration, the modes of conservation, the preparation time, the associations, the quantity and type of solvents, the routes of administration, the nature of knowledge acquisition as well as the other diseases treated by these plants). Interviews of local population were carried out in French and local languages. Access and maintenance in the villages was facilitated by indigenous village guides who also translated local languages into French. The exchanges were facilitated by the purchases of medicinal plants presented by herbalists, traditional healers and users of medicinal plants.
Identification methods
The collection of samples at the study sites was done in situ thanks to the knowledge holders, herbalists and traditional healers who made themselves available for the harvest of plants around huts or in the bush. These samples were kept in a control herbarium according to the techniques and methods of Schnell (1960).
The identification was done using appropriate scientific documentation, by comparison of the vernacular and/or trade names obtained from the respondents, samples of the control herbarium with the data available in the literature, the reference documents of the library of the Faculty of Sciences of the University of Ngaoundere and the material available at the Laboratory of Physiology of Plant Organisms of the University of Ngaoundere. The identification was confirmed by the botanists of the Department of Biology of Plant Organisms of the Faculty of Sciences of the University of Ngaoundere and those of the Department of Biology of Plant Organisms of the Faculty of Sciences of the University of Maroua. It was also confirmed by the botanists of the botany and traditional medicine laboratory of the Institute of Medical Research and Studies of Medicinal Plants and equally with the help of the different volumes of flora of Cameroon stored in the national herbarium from Cameroon. The samples collected were characterized by the types of geobotanical distribution, the morphological types, as well as the types of biotopes (Aubreville, 1962; Evrard, 1968; Letouzey, 1985).
Data analysis methods
The data was first analyzed by entering the various recipes and their characteristics by region and by informant on a Microsoft Excel Version 2018 spreadsheet. The variables were presented as percentages in tables and in a graph form.
RESULTS
Socio-demographic characteristics of the respondents
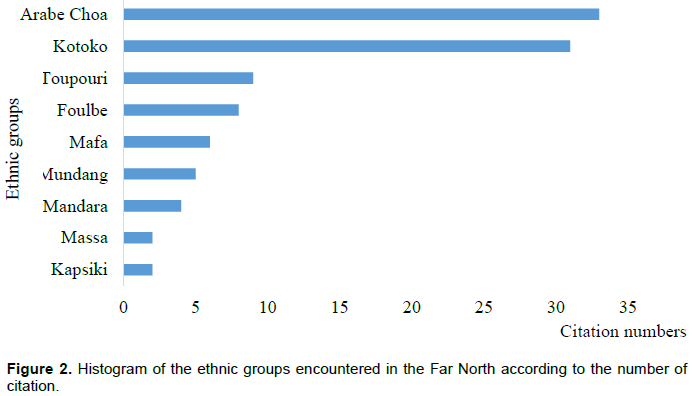
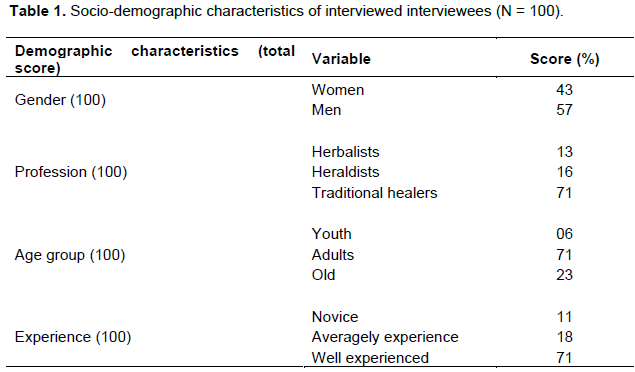
One hundred (100) people in the Far North region were interviewed on the traditional knowledge and importance of medicinal plants used in the treatment of onchocerciasis. The most represented ethnic groups were Araba choa (38) and Kotoko (31) (Figure 2). The sociodemographic characteristics of this study are listed in Table 1.
Floristic characteristics of plants directed against onchocerciasis
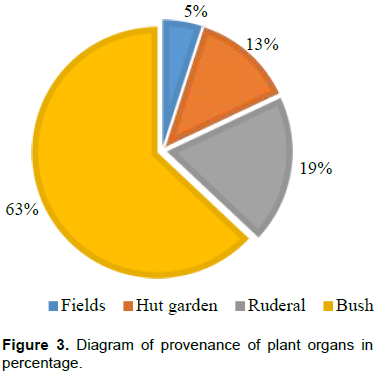
The floristic inventory identified 96 plant species belonging to 49 genera and divided into 29 families. The most represented families being those of Fabaceae (20 citations), followed by Apocynaceae (12) and Combretaceae (9). The most represented genera were Acacia (4). The 96 medicinal plants listed mainly came from the bushes (63) followed by ruderal species (19), the case gardens (13) and field species (5) (Figure 3).
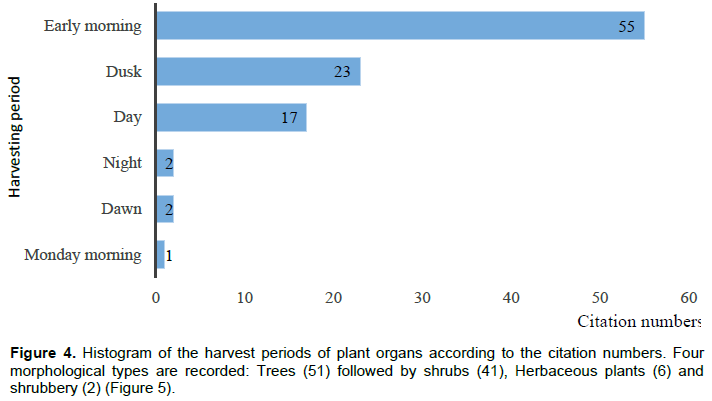
The identified species have two types of biotopes: Savannahs (98) and meadows (2). The registered plants were mainly harvested at dawn (57) followed by dusk (23), day (17), night (2) and Monday morning (1) (Figure 4).
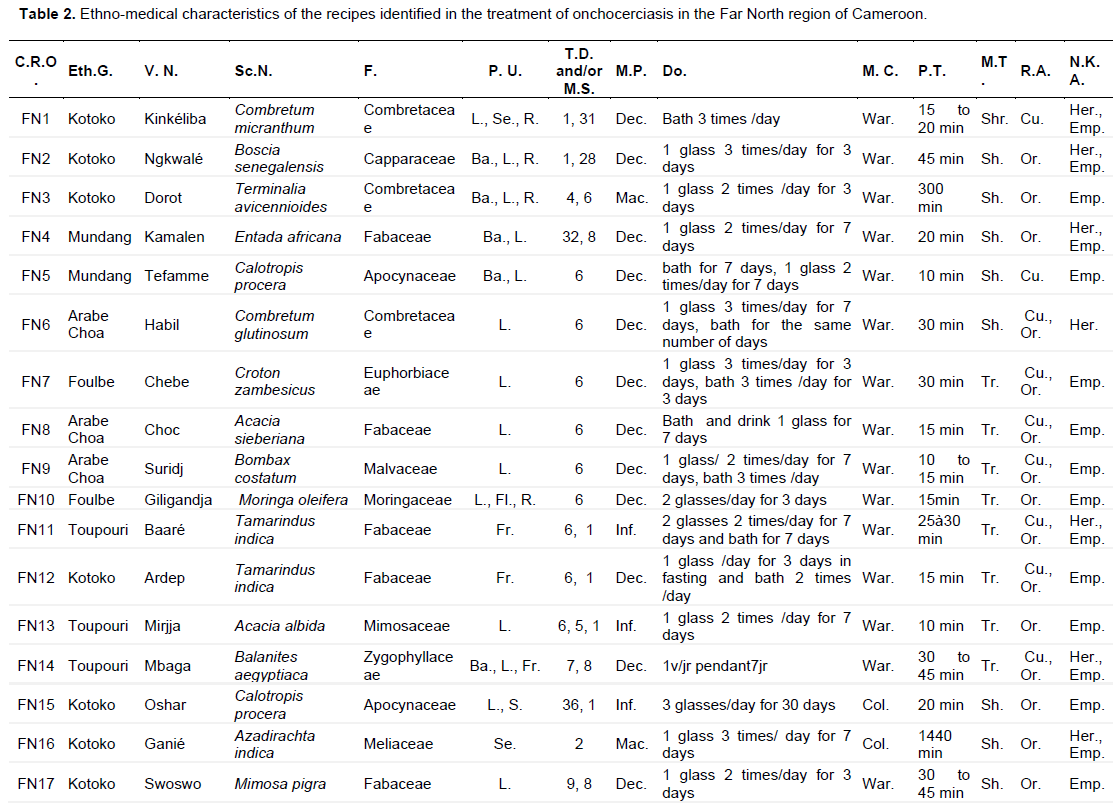
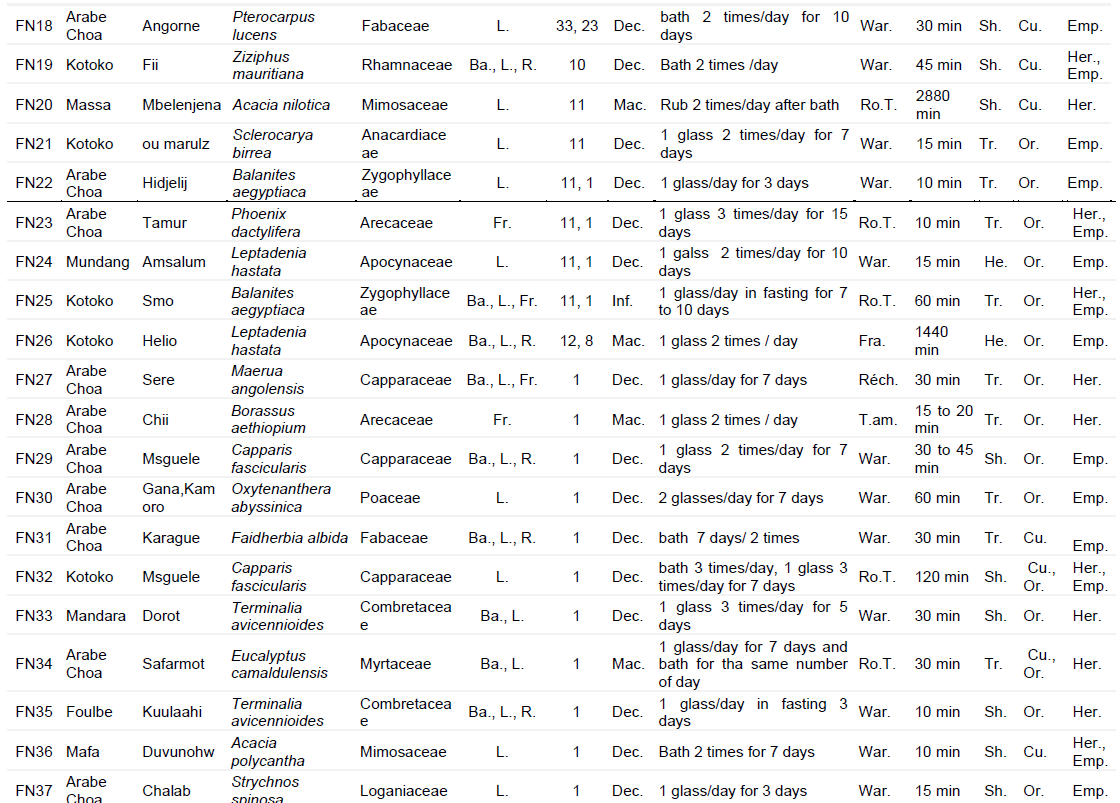
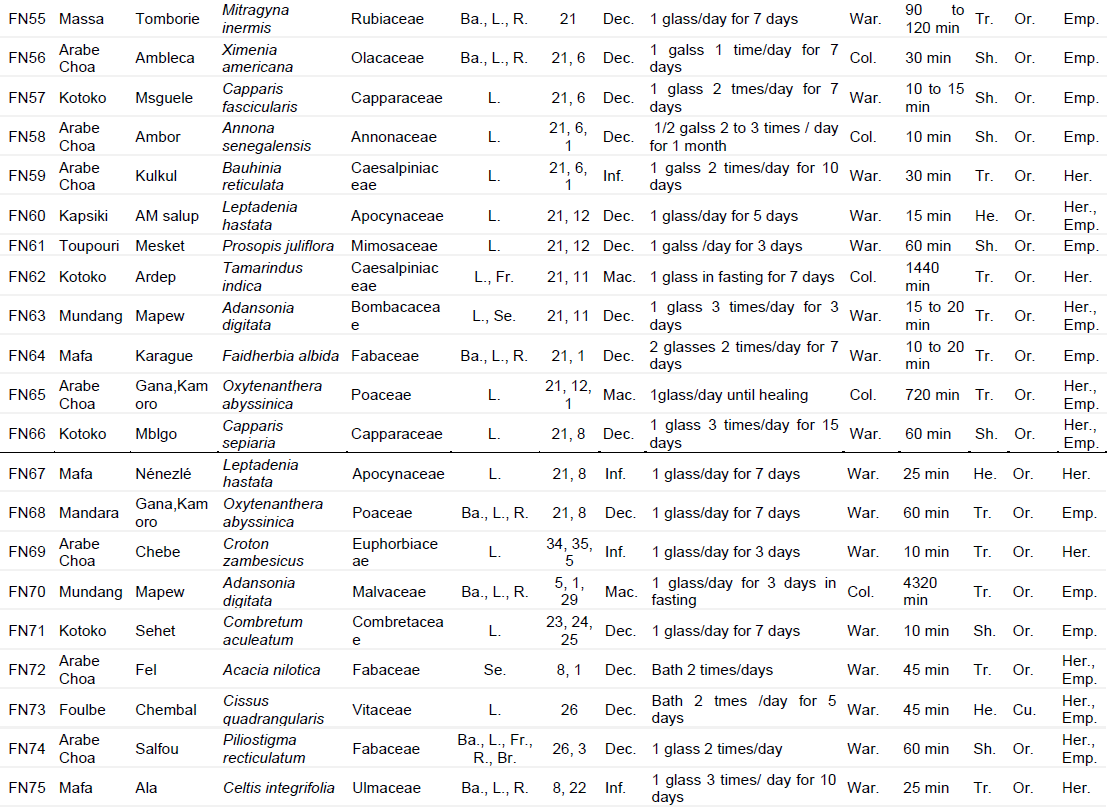
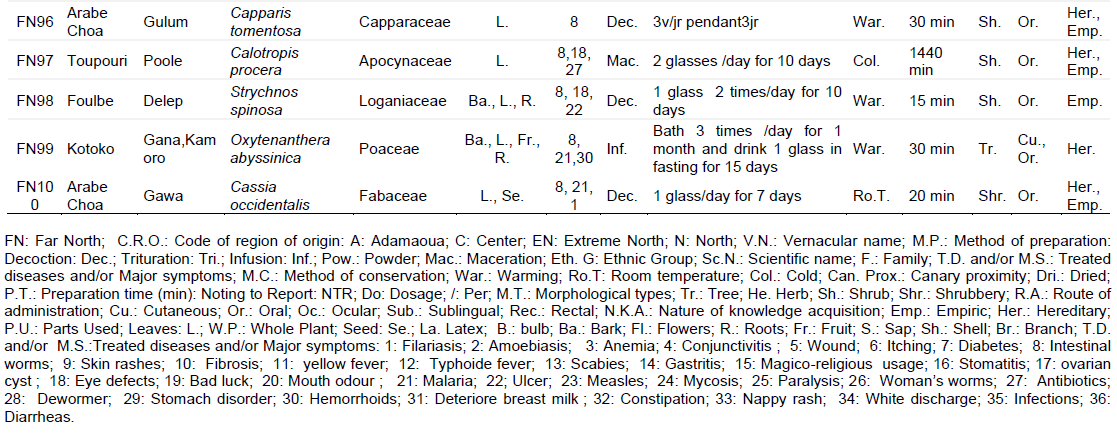
The most common preparation method was decoction (69) followed by maceration (16) and infusion (15). For the various preparations, the most widely used solvent was water (97). Drug are mostly warmed (73) but the different recipes were preferably reheated and stored at cold (17) followed by ambient temperature (10). The most widely used route of administration has been the oral route (76) followed by the dermal and oral route (14), dermal route (9), oral and rectal route (1). Eighteen plant organs were used to prepare the various traditional recipes. The most represented were the leaves (40) and the leaf-bark-root mixture (25). The herbal medicines identified made it possible to obtain two hundred recipes with their method of preparation and administration for 36 diseases and or symptoms related to parasitic infections in general and onchocerciasis in particular (Table 2).


DISCUSSION
In Africa, traditional medicine contributes up to nearly 80% of primary health care among rural populations. In this study, out of 100 interviewed, 43 women were identified; similarly, study conducted in Pakistan revealed that women were afraid of exchange with strangers and particularly the male gender (Umair et al., 2017). This is also due to the inability of women to enter forests for plant samples collection, although they hold the same traditional knowledge. On the other hand, ethnobotanical surveys carried out in the coastal region of Cameroon showed rather a high proportion of women compared to men (Ladoh Yemeda et al., 2016). In this present investigation, 75% of respondents were adults. This could be linked to the fact that the practice of traditional medicine requires an initiation and that is often acquired over time. Besides, it is from a certain age that practitioners are credible and able to exercise like mastering of the use of plants in the treatment of vaginal infections (Ndjib et al., 2017). Although all age groups were involved in the present surveys carried out, the age group greater than 60 (23%) no longer seems interested in the transmission of traditional knowledge. In addition, only a few young people under the age of 29 (06%) follow and exercise the medicinal practices and traditional knowledge transmitted by adults. This is also the case in a study carried out in Nigeria in which young people were less represented because they are very attached to modern life (Bouasla and Bouasla, 2017) and this constitutes a high risk of ancestral knowledge loss in Africa (Ndjib et al., 2017). That situation was also reported from Nepal (Joshi and Edington, 1990). The transmission of knowledge about medicinal plants is most often by inheritance from grands-parents to the descendants. Thus, the fact that young people are losing the interest in traditional medicine for the benefit of their education and various other hobbies, might lead to a risk of a permanent loss of therapeutic uses of medicinal plants in rural areas, or in the national territory (Mpondo et al., 2017). The Foulbe and Choa Arab ethnic groups are the most represented in this present study. This may be explained by the fact that these ethnic groups migratory cattle-breeders living in pasture zones, exposed to high risk of onchocerciasis and for treatment, they use medicinal plants. Traditional healers were the most represented in this study (71%). This could be explained by the fact that traditional healers were more opened to people inquiries compared to heraldists or holders of rural knowledge who exercise in addition, other activities. The important proportion of respondents (71%) possessed a large experience more than 10 years of practice in the exercise and knowledge of the use of medicinal plants. The studied population inherited knowledge from their ascendants. The traditional use of herbal medicines, transmitted in by inheritance, forms the basis of medicine for the treatment of onchocerciasis in populations living in the areas studied. Knowledge about the practice of traditional medicine is transmitted from the ascendants to the descendants but also empirically, each individual holds a secret which was transmitted to him either by his ancestors, or during the training with the holders or what he has acquired over the years of experience, but communication between individuals remains a priority. In fact, in Africa, the practice of traditional medicine remains a family affair. Some authors reported that knowledge is traditionally and empirically transmitted from father to son (Dibong et al., 2015; Adjanohoun, 2000). From Figure 5, the ethnobotanical survey carried out in the Far North region of Cameroon identified 96 species divided into 29 families belonging to 49 genera. In the department of Lom and Djerem in eastern Cameroon, 115 species, belonging to 59 families and grouped into 105 genera were reported (Etame-Loe et al., 2018). It emerges from this study that the diversity of plant species obtained is linked to the degree of knowledge and use of plants by populations who are accustomed to their use and benefiting from them for their well-being. Botanical identification has shown that from the 29 families identified, Fabaceae (20 species); also called legumes, is the one that people masters best because it provides most of their plant food. Besides this, the preponderance of this family accounts for its importance in traditional medicine. Fabaceae family is well-known in Africa and contributes to the treatment of several diseases such as hemorrhoids (Dibong et al., 2015), vaginitis (Ndjib et al., 2017), helminthiasis (Bajin Ba Ndob et al., 2016). The similarity between the predominant families elsewhere and those of the regions studied, testifies to the richness of these areas flora. The savannah represents the main type of biotope, characteristic of agro-ecological zones representing the Far North region. This result shows that people use the plants around their environments to treat onchocerciasis. This is comparable to the study carried out in Haut Nkam where the populations had mentioned semi-mountainous species, characteristic of the region of West Cameroon (Mpondo et al., 2017). The plants used in this study are preferably harvested at dawn. Indeed, the harvest period plays an important role when it comes to the nature of compounds which gives them medicinal importance. Dibong et al. (2015) reported that plants harvested at dawn are the most therapeutic in traditional medicine. By grouping the medicinal plants identified in this study, trees mainly represented the morphological type. This is particular because they provide the necessary materials (leaves, bark, fruit, roots, etc.) which are used to prepare medication recipes, but also because they last for several years (Tsabang et al., 2017).
The administration of herbal drugs was made easier by the different preparation methods. Decoction is the most mode of preparation of the drugs employed in this study. Indeed, boiling is the method which allows the extraction of the maximum active ingredients and also sterilizes the drug. Decoction has been mentioned in a multitude of ethnobotanical studies, it could be the best mastered mode by local populations (Dibong et al., 2015; Mpondo et al., 2017). The best solvent is water; this could be justified by the fact that water is not only more accessible but also better controlled and would not exhibit any interaction with drugs derived from the plant (Ndjib et al., 2017; Kidik Pouka et al., 2015). The oral route is the most used in the traditional treatment of onchocerciasis. This could be justified by the fact that assimilation is easier after consumption (Ghedadba et al., 2014; Lougbégnon et al., 2015). The drugs prepared in the treatment of onchocerciasis are often warmed before being consumed but also kept cool and at room temperature; this is also the case for drugs prepared for the treatment of diseases such as hemorrhoids and vaginitis (Dibong et al., 2015; Ndjib et al., 2017). The leaves are the parts which are mostly used in the areas studied and harvested by simple cutting. That plant part is the seat of secondary metabolites responsible for the biological properties of the plant. The bioactive compounds are synthesized in the leaves and stored in the roots; these organs constitute the storage places of basic materials, protectors of the organism thus promoting a high yield in the capacity to treat (Mangambu et al., 2014; Ngoule et al., 2015).
CONCLUSION
Ethnobotanical surveys of the populations of the Far North region of Cameroon have revealed that several medicinal plants are used for the treatment of diseases and symptoms similar to helminthiasis (Figure 5). Indeed a total of 96 plant species grouped in 49 genera and belonging to 29 families were identified. Trees mainly found in Savannah and belonging to Fabaceae and Apocynaceae families were the most represented. Plant parts commonly used included roots and mostly the leaves. Decoction constituted the prevailing preparation method. In these regions, population knowledge on medicinal plants was inherited from the ancestors. One hundred recipes treating 36 diseases, symptoms and/or uses for therapeutic or preventive purposes, related to parasitic infections were identified. These findings may constitute a relevant Cameroonian database for biological screening in the search for plant-based antiparasitic molecules, especially for antihelminthiasis purposes.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
REFERENCES
|
Adjanohoun E (2000). Biodiversity in the face of the development of the African pharmaceutical industries. In Network of "medicinal woody species", Eyog Matig O, Adjanohoun E, de Souza S and Sinsin B (eds). Report of the first network meeting held December 15-17, 1999 at the IITA Cotonou Station, Benin. pp. 88-103. |
|
|
Aubreville A (1962). Chronological position of Gabon. Flore du Gabon 2:3-11. |
|
|
Bajin ba Ndob I, Mengome LE, Bourobo Bourobo HP, Yvon (2016). Ethnobotanical survey of medicinal plants used as anthelmintic remedies in Gabon. Journal of Ethnopharmacology 191:360-371. |
|
|
Basanez MG, Pion SD, Boakes E, Filipe JAN, Churcher TS, Boussinesq M (2008). Effect of single-dose ivermectin on Onchocerca volvulus: A systematic review and meta-analysis. Lancet Infectious Diseases 8:310-322. |
|
|
Benlamdini N, Elhafian M, Rochdi A, Zidane L (2014). Floristic and ethnobotanical study of the medicinal flora of the Eastern High Atlas (Haute Moulouya). Journal of Applied Biosciences 78:6771-6787. |
|
|
Biyiti LF, Meko'o DJL, Tamzc V, Amvam Zollo PH (2004). Research of the antibacterial activity of four Cameroonian medicinal plants. Pharmacopoeia and African Traditional Medicine 13:11-20. |
|
|
Borsboom GJ, Boatin BA, Nagelkerke NJ, Agoua H, Akpoboua KL (2003). Impact of ivermectin on onchocerciasis transmission: Assessing the empirical evidence that repeated ivermectin mass treatments may lead to elimination/eradication in West Africa. Filaria Journal 2(1):1-25. |
|
|
Bouasla A, Bouasla I (2017). Ethnobotanical survey of medical plants in north eastern of Algeria. Phytomedicine 36:68-81. |
|
|
Demanou M, Enyong P, Pion SDS, Basanez MG, Boussinesq M (2003). Experimental studies on the transmission of Onchocerca volvulus by its vector in the Sanaga valley (Cameroon): Similium squamosum B. Intake of microfilariae and their migration to the haemocoel of the vector. Annals of Tropical Medicine and Parasitology 97(4):381-401. |
|
|
Despommier DD, Gwadz RW, Hotez PJ (1995). Onchocerca volvulus (Leuckart 1893) in Parasitic Disease. Springer New York, pp. 47-53. |
|
|
Dibong SD, Mvogo Ottou PB, Vandi D, Ndjib RC, Monkam Tchamaha F, Mpondo Mpondo E (2015). Ethnobotany of anti hemorrhoidal medicinal plants in the markets and villages of the Center and the Littoral Cameroon. Journal of Applied Biosciences 96:9072-9093. |
|
|
Etame-Loe G, Ngoule CC, Mbome B, Kidik Pouka C, Ngene JP, Yinyang J, Okalla Ebongue C, Ngaba GP, Dibong SD (2018). Contribution to the study of medicinal plants and their traditional uses in the department of Lom and Djerem (East, Cameroon). Journal of Animal and Plant Sciences 35(1):5560-5578. |
|
|
Evrard C (1968). Ecological research on the forest stand of hydromorphic soils of the Congolese central basin. Publish. INEAC. Sér. Science. N°110 Bruxelles, 295p. |
|
|
Eze J, Malau BM (2011). Assessment of the epidemiology of Onchocerca volvulus after treatment with ivermectin in the federal capital territory, Abuja, Nigeria. International Journal of Recent Research and Applied Studies 7(3):319-325. |
|
|
Fenwick A (2012). The global burden of neglected tropical diseases. Public Health 126(3):233-236. |
|
|
Ghedadba N, Hambaba L, Aberkane MC, Oueld-Mokhtar SM, Fercha N, Bousselsela H (2014). Evaluation of the in vitro hemostatic activity of the aqueous extract of the leaves of Marrubium vulgare L. Algerian Journal of Natural Products 2:64-74. |
|
|
Gounoue-Kamkumo R, Nanna-jeunga HC, Bopba J, Akame J, Tarini A, Kamgno J (2015). Loss of sensitivity of immune chromatographic test (ICT) for lymphatic filariasis diagnosis in low prevalence settings: consequence in the monitoring and evaluation procedures. BMC Infectious Diseases 15:579. |
|
|
Hartman W, Haben I, Fleischer B, Breloer M (2011). Pathogenic nematodes suppress humoral responses to third-party antigens in vivo by IL-10-mediated interference with Th cell function. The Journal of Immunology 187:4088-4099. |
|
|
Joshi A, Edington J (1990). The use of medicinal plants by two village communities in the central development region of Nepal. Economic Botany 44:71-83. |
|
|
Kamgno EJ, Labrousse F, Bousinesq M, Nkegoum B, Thylefors BI, Mackenzie CD (2008). Case report: Encephalopathy after ivermectin treatment in a patient infected with Loa Loa and Plasmodium spp. American Journal of Medicine and Hygiene 78:546-551. |
|
|
Kidik Pouka MC, Ngene JP, Ngoule CC, Mvogo Ottou PB, Ndjib RC, Dibong SD, Mpondo Mpondo E (2015). Characterization of medicinal plants with flavonoids from the markets of Douala (Cameroon). International Journal of Biological and Chemical Sciences 9:1494-1516. |
|
|
Koné D (2009). Ethnobotanical survey of six Malian medicinal plants-extraction-identification of alkaloids - characterization, quantification of polyphenols: Study of their antioxidant activity. Doctoral thesis University of Bamako, Mali. 157p. |
|
|
Ladoh Yemeda CF, Vandi D, Dibong SD, Mpondo Mpondo E, Wansi JD, Betti JL, Choula F, Ndongo Din, Tomedi Eyango M (2016). Ethnobotanical study of medicinal plants sold in the markets of the city of Douala, Cameroon. Journal of Applied Biosciences 99:9450-9466. |
|
|
Letouzey R (1985). Phytogeographic map of Cameroon at 1/500000 n04. IRAICIV, University of Toulouse, France. 240p. |
|
|
Lougbégnon OT, Gbesso GH, Codjia JTC (2015). Diversity and forms of use of the medicinal plants sold on the markets of the commune of Ouidah in the south of Benin. Geography review of the Leïdi Laboratory, 263p. ISSN 0851-2515-No 13, December 2015. |
|
|
Magdi MMA (2006). Immunologic aspects of the pathogenesis of human onchocerciasis. PhD thesis, Department of Immunology, The Wenner-Gren Institute, Stockholm University, Sweden. ISBN 91-7155-202-2 pp. 1-68. |
|
|
Mangambu MJD, Mushagalusa KF, Kadima NJ (2014). Contribution to the phytochemical study of some anti-diabetic medicinal plants from the city of Bukavu and its surroundings (Sud-Kivu, R.D. Congo), Journal of Applied Bioscience 75:6211-6220. |
|
|
Marlieke EA, Wilma A, Stolk, Gerrit J, van O, Habbema JDF (2006). Model-based analysis of trial data: microfilaria and worm-productivity loss after diethylcarbamazine-albendazole of ivermectine-albendazole combination therapy against Wuchereria bancrofti. Tropical Medicine and International Health 11:718-728. |
|
|
Molyneux DH, Bradley M, Hoerauf A, Kyelem D, Taylor MJ (2003). Mass drug treatment for lymphatic ï¬lariasis and onchocerciasis. Trends in Parasitology 19:516-522. |
|
|
Mpondo ME, Ngene JP, Mpounze Som L, Etame Loe G, Ngo Boumsong PC, Yinyang J, Dibong SD (2017). Traditional knowledge and uses of medicinal plants in the Haut Nyong Department. Journal of Applied Biosciences 113:11229-11245. |
|
|
Ndjib RC, Dibong SD, Mvogo Ottou PB, Nyegue MA, Eto B (2017). Ethnobotanical study of medical plant used in the treatment of vaginal infection in four towns in Cameroon. Saudi Journal of Biological Sciences 2(9):366-373. |
|
|
Ndjonka D, Djafsia B, Eva L (2018). Review on medicinal plants and natural compounds as anti Onchocerca agents. Parasitology Research 117:2697-2713. |
|
|
Ngoule CC, Ngene JP, Kidik Pouka MC, Ndjib RC, Dibong SD, Mpondo Mpondo E (2015). Floristic inventory and characterization of medicinal plants with essential oils from the Douala Est markets (Cameroon). International Journal of Biological and Chemical Science 9(2):874-889. |
|
|
Schnell R (1960). Techniques for herbalisation and conservation of plants in countries tropical. Journal d'agriculture traditionnelle et de botanique appliquée 7:1-48. |
|
|
Sereme A, Millogo-rasolodimby J, Guinko S, Nacro M (2008). Therapeutic properties of tannin plants in Burkina Faso. African Pharmacopoeia and Traditional Medicine 15:41-49. |
|
|
Tanya VN, Wandji S, Kamgno J, Achukwi DM, Enyong PAI (2013). Recent advances in onchocerciasis research and implication for control. The Cameroon Academy of Sciences. Yaounde, Cameroon, 91p. |
|
|
Tsabang N, Yedjiou CG, Tchounwou PB (2017). Phytotherapy of High Blood Pressure in three phytogeographic regions of Cameroon. Pharmaceutica Analytica Acta 8(1). |
|
|
Turner JD, Tendonfor N, Esum M, Johnston KL, Langley RS, Ford L, Faragher B, Specht S, Mand S, Hoerauf A, Enyong P, Samuel W, Taylor MJ (2010). Macrofilaricidal activity after doxycycline only treatment of Onchocerca volvulus in an area of Loa loa co-endemicity: A randomized controlled trial. PLoS Neglected Tropical Diseases 4(4):1-14. |
|
|
Umair M, Altaf M, Abbasi AM (2017). An ethnobotanical survey of indigenous medicinal plants in Hafizabad district, Punjab-Pakistan. PloS ONE 12(6):e0177912. |
|
|
WHO (World Health Organization) (2015). Investing to overcome the global impact of neglected tropical diseases: Third WHO report on neglected diseases. 211p. ISBN 978 92 4 156486 1. |
|
|
WHO (2016). Analytical health profile of Cameroon, Minister of Public Health. 145p. |
|
|
WHO (2017). Progress report on the elimination of human onchocerciasis, Weekly epidemiological record, Switzerland. 2016-2017. 45(92):681-700. |
|
|
Zoure HG, Noma M, Tekle AH, Amazigo UV, Diggle PJ, Giorgi E, Remme JH (2014). The geographic distribution of onchocerciasis in the 20 participating countries of the African Programme for Onchocerciasis Control: (2) pre-control endemicity levels and estimated number infected. Parasites and Vectors 7(1):326. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


