Full Length Research Paper

ABSTRACT
In recent years safe voluntary male medical circumcision (VMMC) has been recommended by the World Health Organization (WHO) as one of the preventive strategies for human immunodeficiency virus (HIV)-infection for those countries with high HIV prevalence and low medical male circumcision rates. This study aimed to assess the level of knowledge, attitude, and acceptance of safe VMMC among male university students attending Botswana University. A survey instrument was used to collect descriptive data in this study. Out of the total number of faculties within the university (8), we purposively selected our sample from the faculty of science due to its predominant male student population of 1,045. A total of 437 students were recruited from the various departments within the faculty. A semi-structured questionnaire was used for data collection. Study results indicate that 95.4% of the participants had heard about VMMC and 64.8% of those who had heard about VMMC were uncircumcised. About 31.4% knew about the complications of VMMC. Participants having undergone VMMC were twice as likely to be aware that VMMC reduces the risk of penile cancer and that it improves penile hygiene. Participants who knew that VMMC reduces the risk of other STIs were found to be four times more likely to accept VMMC as a preventive method for HIV infection. Participants having been medically circumcised were four times more likely to disagree with the statement that VMMC decreases sexual satisfaction and ten times more likely to disagree with the statement that the tip of the penis has to be covered by the foreskin. Study findings suggest that in terms of knowledge and attitude, the most significant factor associated with men’s acceptability of VMMC was their awareness that it reduces the risk of other STIs. It is therefore concluded that even though there exist a high-level of awareness and favourable attitude towards VMMC among the young male population; such awareness does not seem to influence individuals to become medically circumcized.
Key words: Voluntary male medical circumcision, human immunodeficiency virus (HIV) prevention, sexual transmitted infections, university students.
INTRODUCTION
Male circumcision (MC) is one of the oldest and most common surgical procedures worldwide and is undertaken for many reasons such as religious, cultural, social and medical (World Health Organization/Joint United Nations Programme on HIV/AIDS [WHO/UNAIDS], 2007). Approximately 30% of the world’s male population aged 15 and above are circumcised (WHO/UNAIDS, 2007). Of these, approximately two-thirds (69%) are Muslims (living mainly in Asia, the middle east and north Africa), 0.8% are Jewish and 13% are non-Muslims/non-Jewish men living in the United States (WHO/UNAIDS, 2007). Male circumcision is common in many African countries. For instance, MC is nearly uni-versal in North Africa and much of West Africa (UNAIDS, 2012). In contrast, MC is less common in southern Africa, where self-reported prevalence of MC is approximately 15% in many southern African countries, including Botswana (WHO/UNAIDS, 2007). Botswana has been one of the hardest hit in southern African countries by HIV and AIDS with national adult (15 to 49 years) HIV prevalence exceeding 23.4% (Avert, 2012). The country has been addressing the HIV epidemic through various strategies such as condom promotion, effective treatment of sexually transmitted infections, voluntary testing, counselling and introduction of a universal anti-retroviral treatment program. Despite these measures, the number of new HIV infections was estimated at 9,000 cases (UNAIDS, 2012); there is a need for the adoption of innovative and evidence-based interventions. Evidences from various researches have demonstrated that male circumcision has been proven to have a modest protective effect from HIV infection (Auvert et al., 2005; Bailey et al., 2006; Gray et al., 2007).
According to the WHO estimates, 30% of males worldwide are circumcised; with almost 70% of them being Muslims (WHO/UNAIDS, 2007). The prevalence of MC in Africa varies from less than 20% in some southern African countries to near universal in north and West Africa (Bailey et al., 2006). The University of Botswana is the largest institution which comprises the youth population, with a total enrolment of 17,678 students as per the 2012/2013 academic year. Therefore, studying the knowledge, attitude and acceptance of safe male circumcision of this population group has paramount importance for the success of the programme itself in the country. This study was therefore the first of its kind in institutions of higher learning in Botswana. Further, the low uptake of safe male circumcision since its launching in the country in 2009 was another important reason which triggered the research team to conduct this study amongst the university students. For instance, the national voluntary male medical circumcision (VMMC) programme’s target for the number of circumcised individuals was set at 40,000 from October, 2011 to May, 2012. However, only a total of 14,353 (36%) males were eventually circumcised (Botswana Ministry of Health, 2012). Hence, the underlying aim of this study was to investigate the level of knowledge amongst male university students in Botswana (Gaborone) about the basic facts related to VMMC; their attitude/perception towards VMMC; their behaviour towards male circumcision; and finally their degree of acceptance of VMMC as a preventive strategy against HIV infection. It cannot be ignored that male circumcision is often associated with various beliefs in society especially in relation to sexual matters in every region around the world. For instance, in one study that was conducted in the Dominican Republic it was found that a proportion of about 46% of the respondents reported that male circumcision reduces sexual pleasure amongst men (Brito et al., 2009). There is still a strong belief amongst males even in the Southern region of Africa that male circumcision decreases their natural sexual ability.
METHODOLOGY
Design
A quantitative, descriptive survey design was used as it was found suitable in carrying-out this study of assessing the level of knowledge, attitude, and acceptance of VMMC among male university students in Botswana.
Population and sampling
The study was conducted amongst male students in the main campus of the University of Botswana. The university has eight different faculties with a total enrollment of 7, 953 male students during the 2012/2013 academic year. Each faculty was composed of roughly 600 to 1500 male students. Out of the total of 8-faculties, we purposively selected the faculty of science due to its large male student population of 1,045. From the head-count of 7,953 male students during the 2012/2013 academic year, then the Raosoft sample calculator was used to determine a reasonable sample population size (Raosoft, 2004), from which a sample size of 367 was calculated with a margin of error of 5%, confidence level of 95% and a distribution of 50%. In order to compensate for any eventualities as regard to the completed questionnaires (in terms of incomplete responses or wrongly completed questions), our sample size was deliberately increased and 450 participants were targeted. Each and every department within the faculty of sciences were then approached during the recruitment of participants. Students were approached while in their classes either before or after a lecture and briefed about the objectives of the study.
Data collection tool
A semi-structured questionnaire was used for data collection. The questionnaire was written in the English language as the participants were at tertiary level of education. Data collection instrument comprised three sections. These include the participants’ socio-demographic characteristics, knowledge about VMMC, and lastly attitude/perceptions towards VMMC.
Data collection
The questionnaire were pre-tested on 10 male students from the faculty of education two weeks before data collection to improve reliability and validity of the questionnaire, and not many changes were necessary in its wording. Data collection was conducted immediately after students returned to campus for their last semester. After receiving the permission from the university administration to conduct the study, data collection was carried out for a period of five-days (one-week). Arrangements were made with lecturers in visiting their lecture rooms while students were in the class rooms after a lecture. During each session, a brief description about the study was given to all students in class, and those who were willing to participate were there-after invited to remain behind. More briefing was thereafter given to those who were willing to participate. After signing their consent forms which comprised detailed information about the study including its significance and purpose, the participants were given the questionnaires including additional instructions on how to respond to the questions. This normally took them about 15 to 20 min, after which all responses were collected.
Data analysis
All responses were individually checked in order to identify some mistakes and completeness of data. Data were later entered into Microsoft Excel spread, coded and thereafter imported into both the Epi-info and Stata-10 statistical software for statistical processing and analysis. The t-test, chi-square test, and odds ratios (OR) with 95% confidence interval were used to measure associations. All statistical tests were performed using the two-tailed tests, and a p-value of less than 0.05 was considered statistically significant. Further, the logistic regression analysis was used to assess the bivariate relationship between the knowledge, attitude, and acceptance of VMMC amongst the students. Finally, findings were described using summary measures expressed as means (standard deviations), medians (ranges), modes, and proportions.
Validity, reliability and bias
Reliability was guaranteed by trying to standardize the questionnaire as much as possible. Furthermore, the questionnaire was pre-tested amongst 10 students from a different faculty which was not part of the study sample. An appropriate design was further employed and suitable variables were selected for our study objectives in order to increase the validity of the study. It was also ensured that experts from the department of public health at the University of Botswana and Medunsa validated the entire design of the study. However, in terms of our sample size, no attempt was made to extrapolate the results to the general population of the entire university student population in Botswana.
Ethical issues
The Medunsa Campus Ethics Committee (MREC) approved the study with the certificate Ref. [MREC/H/60/2013:PG]. In addition, permission to conduct the study was granted by the Health Research and Development Division in Botswana (at the Ministry of Health). Further, the office of Research and Development at the University of Botswana granted permission for conducting the study. It was ensured that all participants of the study were fully informed about the nature of study and were provided with a consent form which comprised detailed information about the study including its significance and purpose. Confidentiality of all information provided such as how and where data will be stored (in a password-accessed computer base) was explained to the participants. The study was strictly voluntary and participants were given an absolute right to refuse to participate. Furthermore, participants’ were informed that their names should not be written on the questionnaires.
RESULTS
Sample characteristics
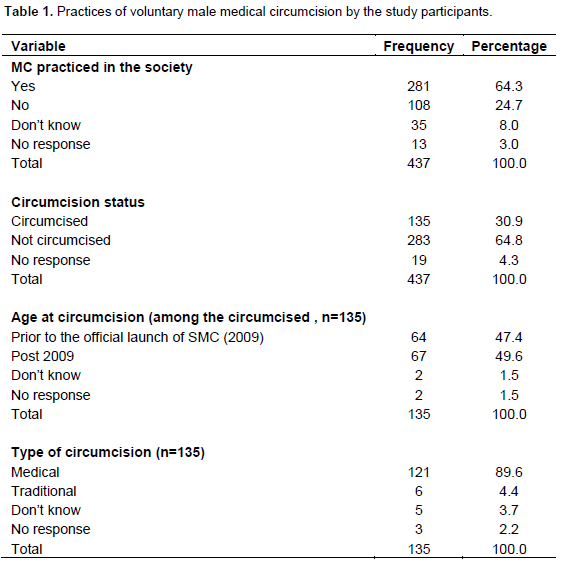
Out of a targeted total sample of 450 students, we reached a response rate of 97.1% (437). Majority of the respondents (83.3%, n=364) were aged 25 years or below and the median age was 21years. Most of the students were single, but 46.5% (n=203) of them had girlfriends. About 45% of the students (n=199) originated from the central district which is the most populous district in Botswana, and majority of the tribes in which the students belonged were: Kalanga (19%, n=83), Mongwato (14.2%, n=62), Mokgatla (8.5%, n=37) and Mokwena (7.6%, n=33). Christianity was found to be the dominant religion among the study participants (86%, n=376). Out of the 437 participants, 30.9% (n=135) were circumcised, 64.8% (n=283) were uncircumcised, and 4.3% (n=19) were not willing to reveal their circumcision status.
Knowledge of VMMC
Almost all the respondents (95.4%, n=417) reported that they have heard and know about VMMC. In regard to knowledge about benefits of VMMC, the participants mentioned the following: (i) reduction of the risk of HIV infection (55.4%, n=242); (ii) reduction of the risk of other STIs (43.5%, n=190); and (iii) improved genital hygiene (21.1%, n=92). Some of the reported complications known by the participants were: (i) improper procedure (27%, n=37); (ii) delayed wound healing (19.7%, n=27); (iii) interference with sexual activities (18.3%, n=25); (iv) excessive blood loss (10.2%, n= 14). Most respondents had high level of awareness on the fact that VMMC has no 100% HIV protection (96.8%, n=423). About 91.1%, n=398 felt there was a need for condom use after VMMC. About 90.2%, n=394 felt it was important to abstain from sex for 6 weeks post circumcision, and that VMMC improves genital hygiene (89.9%, n=393).
Attitudes about VMMC
A significantly high number of respondents believe that the tip of the penis has to be covered by the foreskin (44.9%, n=196) and male circumcision makes the penis vulnerable to environmental hazards (34.1%, n=149). Otherwise, majority of the study participants disagreed that VMMC decreases sexual satisfaction, and that circumcised men have more sexual feeling than the uncircumcised ones. However, 25.9% (n=113) of the respondents believed that women prefer circumcised sexual partner than uncircumcised ones. About 64.3% (n=281) of the respondents reported that male circumcision is practiced in their communities. According to the study participants, majority of the male circumcisions were conducted for medical reasons (44.2%, n=193). Tradition/rite as a reason for male circumcision was reported by only 13.5% (n=59) respondents. Medical reason was mentioned by the majority of the circumcised males (89.6%, n=121) as basis for them being circumcised (Table 1). Almost half of them (47.4%, n=64) did the circumcision post 2009 after the official launch of the national VMMC program in Botswana. Out of the 283 uncircumcised males, 43.8% (n=124) accepted VMMC as a preventive strategy against HIV infection and 43.8% (n=124) did not accept it and 12.4% (n=35) were not sure. Among those who accepted VMMC as a preventive strategy for HIV infection, 64.5% (n=80) had a plan to be circumcised whereas 35.5% (n=44) had no plan to be circumcised (Table 1).
Acceptability of VMMC
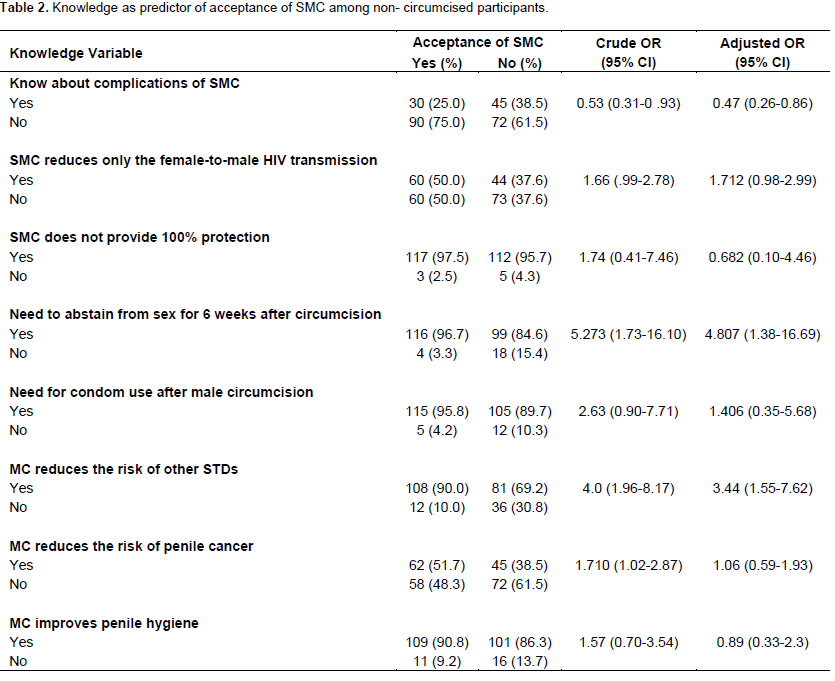
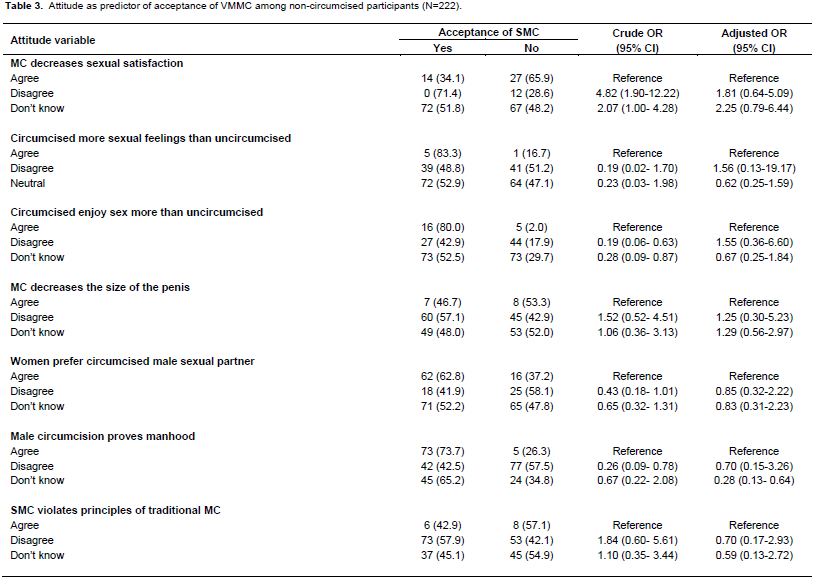
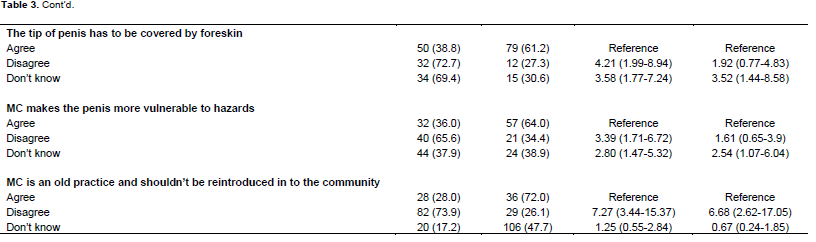
It was found out that circumcised respondents were twice likely to be aware of the fact that “VMMC reduces the risk of penile cancer” and “VMMC improves penile hygiene” than the uncircumcised ones [OR=2.47(1.59-3.83); OR=2.54 (1.03-6.27)], respectively. Otherwise, there was no significant knowledge difference on other facts of VMMC between circumcised and uncircumcised respondents. Again, circumcised participants were found to be four-times likely to disagree with the beliefs that “VMMC decreases sexual satisfaction” [OR=4.06(2.06-8.00)], and ten-times more likely to disagree with the fact that “the tip of the penis has to be covered by foreskin” [OR=9.95(5.57-17.79)]. It was further discovered that the participants were four-times likely to disagree with the statement “VMMC makes the penis more vulnerable to environmental hazards” [OR=3.79(2.19-6.56)], and six-times likely to disagree with the statement “VMMC is an old practice and should not be reintroduced in the community” [OR=6.28(2.74-14.38)] than uncircumcised participants. On the other hand, non-circumcised respondents were found to be less likely to believe that “circumcised men have more sexual feeling than uncircumcised” [OR=0.18(0.07- 0.47)], and that “circumcised men enjoy sex more than uncircumcised” [OR=0.33(0.17-0.64)]. Respondents who had the knowledge of “VMMC reduces the risk of other STIs” were found to be four-times likely to accept VMMC as a preventive strategy for HIV than those who lack this knowledge [OR= 4.0(1.96-8.17)].
Participants who accepted VMMC as a preventive strategy for HIV infection were found to be five-times likely to be aware of the fact that “it is important to abstain from sex for 6 weeks post circumcision” [OR=5.27(1.73-16.10)] than those respondents who refused to accept VMMC. However, those who have some knowledge about the complications of VMMC were found to be 53% less likely to accept VMMC as a preventive strategy for HIV infection than those who lacks the knowledge [OR=0.53(0.31-0.93)]. On the other hand, participants who accepted VMMC as a preventive strategy against HIV infection were found to be five-times likely to disagree with attitude/perceptions of “male circumcision decreases sexual satisfaction” [OR=4.82(1.90-12.22)], and four-times more likely to disagree with “the tip of the penis has to be covered by the foreskin” [OR=4.21(1.99-8.94)]. These participants were further discovered to be trice likely to disagree with the statement “male circumcision makes the penis more vulnerable to environmental hazards” [OR=3.39(1.71-6.72)], and their odds were seven-times likely to disagree with the statement “male circumcision is an old practice and should not be reintroduced into the community” [OR=7.27(3.44-15.37)] than those who did not accept VMMC as a preventive strategy against HIV infection. Acceptability and non-acceptability of VMMC as a preventive strategy for HIV infection were as follows: (i) the awareness about complications of VMMC [OR=0.53(0.31-0.93)]; (ii) VMMC reduces the risk of other STIs [OR= 4.0(1.96-8.17)]; (iii) the fact that it is important to abstain from sex for 6 weeks post circumcision [OR=5.27(1.73-16.10)] (Tables 2 and 3).
DISCUSSION
In this study, it was found that almost all participants have heard and knew about VMMC. Most significantly, just over half of them were aware of the fact that VMMC can decrease the risk of HIV infection. This is consistent with studies conducted in Jamaica and Uganda, which indicated a higher proportion of awareness of male circumcision (Wilcken et al., 2010; Walcott et al., 2013). Some differences were noted on the level of awareness about the VMMC’s protective effect on HIV amongst the respondents where we found that in our study it was higher as compared to other studies conducted in other regions such as East/Central Africa e.g. Uganda with a proportion of 38.2% (Wilcken et al., 2010) and Swaziland with a proportion of 18% (Tsela and Halperin, 2006). Perhaps such differences in terms of the awareness of male circumcision between these studies may be explained based on the fact that our study was conducted among students from an institution of higher learning. In such institutions, students have access advantage to a wide range of educational information compared to an ordinary individual in the society. However, even though such awareness of male circumcision seems to be relatively higher in our study as compared to the earlier mentioned studies, this seems to have no impact on the acceptability of VMMC amongst the participants. Based on these revelations, it can only postulate that this may be due to the fact that many participants in our study seemed to have been hesitant in believing results of the protective effect of VMMC produced by some scientific studies globally.
It was also noted that a significantly high proportion of participants were aware of the effect of VMMC in reducing the risk of Sexually Transmitted Infections (STIs) with a proportion of about 89.9%. Likewise, this was found to be consistent with a study conducted by Tsela and Halperin (2006) in Swaziland in which 81% of the respondents knew that male circumcision reduces the risk of getting STIs. On a positive note, it was noted that having the knowledge that “VMMC reduces the risk of getting STIs” had a significant effect on the acceptability of VMMC in our study in which those who had the knowledge were found to be four-times likely to accept VMMC compared to those who lack the knowledge (OR=4.00, 95% CI=1.96-8.17). Around half of the respondents in our study knew that male circumcision reduces the risk of penile cancer (50.6%). This was found to be consistent with a relatively similar study that was conducted in china which indicated a proportion of about 50%. However, those who were aware that male circumcision decreases the risk of penile cancer were twice likely to accept VMMC than those who lacked such an awareness (OR=1.71, 95% CI=1.02-2.87). This was consistent with a study conducted in China in which it was found that people, who were given health education regarding the effect of male circumcision in reducing penile cancer, increased their acceptability rate substantially (Yang et al., 2012).
It was also noted that majority of the respondents in this study had high level of awareness about the hygienic benefit of safe male circumcision (89.9%) which is consistent with other studies conducted in Kenya (Bailey et al., 2006), Malawi (Ngalande et al., 2006), and Botswana (Kebaabetwe et al., 2003). However, having the knowledge that “VMMC improves penile hygiene” was not found to be a significant predictor of SMC acceptance (OR=1.57, 95% CI=0.70-3.54).
We found a significant difference in terms of attitude towards VMMC between those who were circumcised and those who were uncircumcised. For instance, uncircumcised respondents were found to be ten times less likely to agree with the belief that “the tip of the penis has to be covered by foreskin” [OR=9.95(5.57-17.79)], and four-times less likely to agree with the statement “VMMC makes the penis more vulnerable to hazards” [OR=3.79(2.19-6.56)]. On the other hand, those who were circumcised were found to be 82% less likely to agree with the statement “circumcised men have more sexual feelings than uncircumcised men” compared to the uncircumcised respondents [OR=0.18(0.07-0.47)]. This shows that even though there is no available scientific evidence regarding human sexual-feelings and male circumcision, some favourable beliefs were discovered in this regard among the participants in this study. This will be crucial in promoting the acceptance of VMMC. It was by no surprise that even in studies conducted in Jamaica, Malawi and Uganda participants believed that male circumcision enhances sexual satisfaction (Walcott et al., 2013; Ngalande et al., 2006; Wilken et al., 2010). The acceptability of safe male circumcision among the uncircumcised respondents in our study was found to be 43.8% which was much lower than the median acceptability rate in the sub-Saharan African countries which was 65% (Westercamp and Bailey, 2007). However, these finding seem to be much lower than those of Kebaabetswe et al. (2003) in Botswana which was 60%, which later went up to 80% after a brief information session (conducted among male and female adult population in various communities in Botswana). It must be noted though that in our study the participants were tertiary level educated, male students who have the ability to question any new ideas like VMMC for HIV prevention. These could be the possible explanations for the observed differences between our study and the one conducted by Kebaabetswe et al. (2003). The other important reason given by our respondents for not accepting VMMC was the belief that the foreskin of the penis has a natural importance, which in effect, seems to be an important determinant factor for acceptability of VMMC. This however was not explored in the study of Kebaabetswe et al. (2003).
Through our findings, the factors which were found to be associated with increased acceptability of VMMC which included “the awareness that male circumcision reduces the risk of having STDs” [OR=4.0(1.96-8.17)], and that such an awareness also “reduces the risk of having penile cancer” [OR=1.71(1.02-2.87)] were also noted. In addition, participants in our study were found to be having favourable attitudes towards VMMC which resulted in higher levels of acceptability, and that those who were aware of some of the complications of male circumcision were 47% likely to accept VMMC compared to those without such awareness (OR=0.53, 95% CI=0.31-0.93). However, this is not the case in most studies conducted in the sub-Saharan African countries which indicated pain as the main limiting factor for acceptability of male circumcision (Westercamp and Bailey, 2007).
CONCLUSION
It can therefore be concluded that majority of the students at the University of Botswana are not circumcised. Further, a significantly high percentage of the students at the University of Botswana have heard and knew about safe male circumcision. The students at the University of Botswana have good knowledge about the basic facts on safe male circumcision especially, in relation to its benefits in the prevention of HIV and other STIs, improving penile hygiene, and reducing the risk of penile cancer. To us, this suggests some favourable attitude towards VMMC among the students of the University of Botswana, which is an important positive factor for the success of the VMMC program. On the other hand, we can safely state that safe male circumcision has not been well accepted by majority of the student population at the University of Botswana. This is despite the students’ adequate knowledge about such a program, and their relatively good attitude towards it.
STUDY LIMITATIONS
Possible limitations in this study include the use of a purposive sampling technique (which lacks a true probability method of sampling) of the faculty of science due to its large male population in order to reach our desired sample size of 450 male students.
CONFLICT OF INTEREST
The authors have no conflicts of interest to declare.
REFERENCES
|
Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R (2005). Randomized Controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 Trial. PLoS Med 2(11):e298. Crossref |
||||
| Avert (2012). HIV & AIDS in Botswana. Available from: http://www.avert.org/hiv-aids-botswana.htm#footnote7_nalbr2w Accessed 24/11/2014. | ||||
| Bailey RC, Moses S, Parker CB, Agot K, Maclean I, Krieger JN, Botswana Ministry of Health (2012). HIV/AIDS prevention and care: SMC MOVE Teams, [online]. Available from: http://www.hiv.gov.bw/content/safe-male-circumcision-smcAccessed6/4/2013 | ||||
|
Brito MO, Caso LM, Balbuena H, Bailey RC (2009). Acceptability of male circumcision for the prevention of HIV/AIDS in the Dominican Republic. PLoS ONE 4(11):e7687. Crossref |
||||
|
Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, Nalugoda F, Kiwanuka N, Moulton LH, Chaudhary MA, Chen MZ, Sewankambo NK, Wabwire-Mangen F, Bacon MC, Williams CF, Opendi P, Reynolds SJ, Laeyendecker O, Quinn TC, Wawer MJ (2007). Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet 369(9562):657–666. Crossref |
||||
|
Kebaabetswe P, Lockman S, Mogwe S, Mandevu S, Thior I, Essex M, Shapiro RL (2003). Male circumcision: an acceptable strategy for HIV prevention in Botswana. Sex. Transm. Infect. 79(1):214–219. Crossref |
||||
|
Ngalande RC, Levy J, Kapondo CP, Bailey RC (2006). Acceptability of male circumcision for prevention of HIV infection in Malawi. AIDS Behav. 10(4):377-85. Crossref |
||||
| Raosoft sample size calculator (2004). Raosoft Inc. Available at: http://www.raosoft.com/samplesize.html | ||||
| Tsela S, Halperin DT (2006). Knowledge, attitudes and practices regarding male circumcision in the Manzini (central) region of Swaziland. AIDS 2006 - XVI International AIDS Conference: Abstract no. CDC0611 | ||||
| UNAIDS (2012). Global report, AIDSinfo. Available from: http://www.unaids.org/en/dataanalysis/datatools/aidsinfo. Accessed 25/11/2014 | ||||
|
Walcott MM, Jolly PE, Ehiri JE, Funkhouser E, Kemp MC (2013). Factors associated with the acceptability of male circumcision among men in Jamaica. PLoS ONE 8(9):1 Crossref |
||||
|
Westercamp, Bailey RC, (2007). Acceptability of male circumcision for prevention of HIV/AIDS in Sub-Saharan Africa: A Review. AIDS Behav. 11(3):341–355 Crossref |
||||
| WHO/UNAIDS (2007). Male circumcision: global trends and determinants of prevalence, safety and acceptability. WHO, Brazzaville. | ||||
|
Wilcken A, Miiro-Nakayima F, Hizaamu RNB, Keil T, Balaba-Byansi D (2010). Male circumcision for HIV prevention - a cross-sectional study on awareness among young people and adults in rural Uganda. BMC Public Health 10(209). Crossref |
||||
| Williams CF, Campbell RT, Ndinya-Achola JO (2006). Male circumcision for HIV prevention in young men in Kisumu, Kenya: A randomised controlled trial. Lancet 24,369(9562):643-56. | ||||
|
Yang X, Abdullah AS, Wei B, Jiang J, Deng W (2012). Factors influencing Chinese male's willingness to undergo circumcision: A cross-sectional study in Western China. PLoS ONE 7(1):e30198. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


