Full Length Research Paper

ABSTRACT
Breast cancer (BC) is a leading cause of cancer morbidity and mortality within the female population in sub-Saharan Africa. Growing cancer incidence and mortality are multidimensional, and often associated with the so-called ‘’westernization’’ of lifestyle in African countries, including Niger, where there is no recent update of the cancer registry. The intent of this paper was to analyze 27 years of Niger cancer registry data and produce updated cancer trends and figures. The Niger cancer registry was established in 1992 and compiled on Canreg4. It is a member of African cancer registry network. The total number of cases included in this study was 12,340 patients and the study was conducted in 2020. Incidence trends (joint point) and survival (Kaplan Meier and Cox proportional hazards model) were used to analyze the data. Breast cancer showed high frequency among women, 18.9% (18.3-19.6) followed by gynecological cancers, with cervical and ovarian cancers accounting for 11.0% (10-12.1) and 5.4% (5.0-5.8) of total cases, respectively. Followed by liver cancer, at 13% (12.4-13.6), skin 7.1% (5.5-7.8) and colon/rectum cancer at 4.2% (3.4-5.1). The average cancer patient age was 44.7 (44.4-45.0) years. Despite a slow startup, cancer case registration in Niger showed a significant increase, with an annual percentage change (APC) of 3.7 (1.5-6.0), from 1992 to 2018. Overall, 14.1% (13.5-14.7) of cancer patients reportedly died. Breast cancer survival was found to be associated with sex, age and diagnostic method. Cancer incidence in Niger is growing significantly; breast and gynecological cancers are the most frequent and reported mortality data suggest low survival in Niger. Multicentric cancer screening centers and systematic reporting are necessary for a wider coverage of the cancer registry.
Key words: Niger, cancer registry, breast cancer, survival.
INTRODUCTION
Breast cancer (BC) remains a leading cause of cancer morbidity and mortality within the female population (Youlden et al., 2012; Samuel et al., 2017 ; Joko?Fru et al., 2020a); its public health burden, in sub-Saharan Africa specifically, is not well established (Mohammed and Harford, 2014; Adeloye et al., 2018). Growing cancer incidence imultidimensional, it is often associated with the so-called ‘’westernization’’ of lifestyle in African countries (urbanization, diet change, alcohol/tobacco intake) and even changes in the maternal profile of women (Bray et al., 2018).
In Niger, BC has been identified as the main cause of cancer-related incidence and mortality accounting for 18.3 and 14.6% of the overall cancer burden in the country, respectively (WHO Cancer Country Profiles, 2020). The Niger population is very young, as it is in many sub-Saharan African countries. According to the 2012 Niger Population Census (RGPH, 2012), the Niger population was estimated to be 17.138.707, with 8.518.818 men (49.7%) and 8.619.889 women (50.3%). The current population is approximately 24.088.564, based on the latest United Nations data projections (https://worldpopulationreview.com/countries/niger-population/). Citizens aged over 15 years have a cumulative proportion of 48.3%. Age groups 0-4 years (21.6%), 5-9 years (17.5%) and 10-14 years (12.6%) have the highest proportions in the Niger population age structure. 69% of the Niger population is rural, while 31% is urban. Niger also has one of the lowest literacy rates in the world (UNICEF, https://www.unicef.org/niger/ education) and UNESCO (http://uis.unesco.org/en/ country/ne).
According to WHO Cancer Country Profiles 2020, the country does not yet have operational cancer management guidelines or palliative care included in their operational integrated NCD plan. In addition, there is no national breast cancer screening program. Mammographic screening facilities are very restricted. There are 2.3 radiologists and 1.2 public cancer centers per 10,000 cancer patients in the country. Pathology services and palliative care are rated as “generally not available’’ in the country. A national center for the fight against cancer (Centre National de Lutte Contre le Cancer, CNLC) was recently created (2018). It has chemotherapy services but does not yet have radiotherapy or mammography facilities. In the absence of mammography in low-income countries like Niger, screening methods such as clinical breast examination or breast self-examination, if well performed, could be alternative options (Black and Richmond, 2019; Onyije et al., 2010). Studies in relation to the epidemiology of cancer in Niger are scarce. Some studies (Zaki et al., 2013; Mamoudou et al., 2013; Nayama et al., 2006) contributed basic descriptions of cancer patients in the country without a deep epidemiological analysis of cancer registry data. Younger age and late diagnosis were reported as common features of BC patients in Niger (Zouladeny et al., 2015).
The latest published analyses of Niger cancer registry data were in 2013 and they analyzed data up to 2009 (Salamatou et al., 2013), after more than a decade, there is a real need to produce an updated analysis of the cancer registry data in the country.
METHODOLOGY
The Niger cancer registry data
The Niger cancer registry data is hosted by the Laboratory of Pathological Anatomy and Cytology, (which provides histopathology and cytology services for the whole country) Faculty of Health Sciences, Abdou Moumouni University, Niamey, Niger. It was established in 1992 and is a member of the African cancer registry network. The data is compiled on CanReg4, a tool produced by the International Agency for Research on Cancer (IARC) in collaboration with the International Association of Cancer Registries (IACR).
The data is collected via a network of hospitals, primarily the university teaching hospital where it is physically located and to which most of the cancer patients are primarily referred. Then follow the maternity reference hospital (Maternity Issaka Gazobi, MIG), the national reference hospital, the national center on reproduction, the regional hospitals and even recently some private clinics. There is a team (two pathologists, one data manager, one cancer registrar, a nurse, often assisted by medical students, and the epidemiologists of the national center for the fight against cancer) who conduct the data collection and entry. They travel around the different hospitals in Niamey and the inpatient services (surgery, urology, medicine, gynecology, pediatrics and biology laboratory services) to collect data (see data collection form in the annexes section) that are required by the registrar. The team also consults records they find in these services to track cancer cases. As of 2019, the WHO office in Niger and the West African Health Organization (WAHO) also provides support to the cancer registry. Data collection is not systematically done in view of the limited available human resources. Quality control tools are in place to ensure accuracy and refinement of the collected data. For instance, some variables such as age are compulsory for registering the patient and there is duplication recognition. The coverage of the Niger cancer registry is not very high but is continuously growing. While it was limited to Niamey and the surroundings in the first phase of its implementation, the support of the national center for the fight against cancer has helped the network of data collection extend to other parts of the country, with periodic supervision and data collection trips by the cancer registry team. The data is compiled using the International Classification of Disease - Oncology (ICD-O) and Classification Internationale des Maladies pour l’oncologie (CIM-O, third version-V3).
Data analysis and tools
The data was analyzed retrospectively in two steps: firstly, the overall cancer database was analyzed to give statistical summaries and global incidence trends, and then a subset of data of all BC patients from 1992 to 2018 was analyzed to focus on BC disease.
Summary statistics
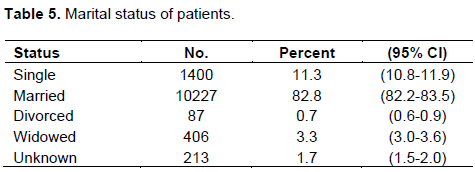
The proportion of cancer types, age, sex, ethnic group, marital status, diagnosis method, stage and reported mortality were given specific attention. Frequencies, percentages and 95% confidence interval (CI) were computed in Epi data analysis v2.2.2.183 and IBM SPSS Statistics v27.
Trends analysis
A chronological evolution of reported cases from 1992 to 2018 was performed, and an annual percentage change (APC) was computed for the overall cancer registry data. A regression model was fitted using joint point analysis (https://surveillance.cancer.gov/ joinpoint/), the reference population was obtained from the 2012 national census.
Survival analysis
Kaplan Meier curves were used to perform the first step of the survival analysis. Out of the 2347 BC patients introduced earlier, we took a data sample for the 10 years from 2009 to 2018 (1347 patients). This was to have the most recent overview of the reported BC mortality. Then a Cox proportional hazards model was used to assess factors associated with breast cancer survival using hazard ratio. R studio Version 1.3.1093 was used to perform these analyses.
The study was approved by the Head of the Laboratory of Pathological Anatomy and Cytology and the Dean of the Faculty of Health Sciences, Abdou Moumouni University, Niamey, Niger. Patients’ nominal information was coded in the data set using a dossier ID.
RESULTS
Description of the sample
Overall cancer sample
According to results summarized in Table 1, the main types of cancer cases recorded in Niger, breast is the most common cancer 18.9% (18.3-19.6) followed by gynecological cancers with cervical and ovarian accounting for 11.0% (10-12.1) and 5.4% (5.0-5.8) of total cases, respectively. Liver 13.0% (12.4-13.6), skin 7.1% (5.5-7.8) and colon/rectum cancers 4.2% (3.4-5.1) are next in frequency.
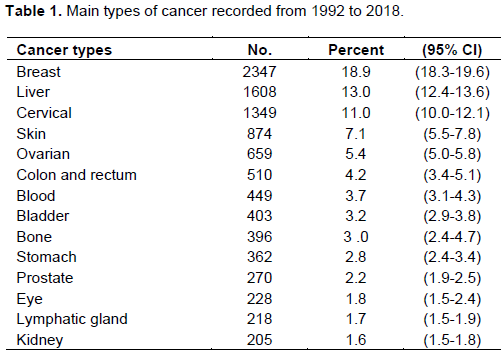
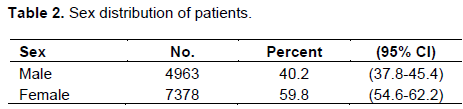
About 60% of reported cancer cases in Niger are female, linked with the predominance of breast and gynecological cancers.
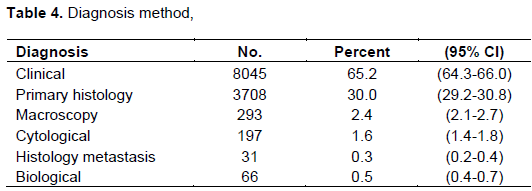
It was observed that two out of three cancer cases are diagnosed clinically in Niger, and most of the time, these clinically diagnosed cases are the ones presenting to the clinicians at late stage. Only 30% had a histological confirmation. Reported mortality (the proportion of cancer patients that died from the startup of cancer registry) for all cancer cases is 14.1% (13.5-14.7).
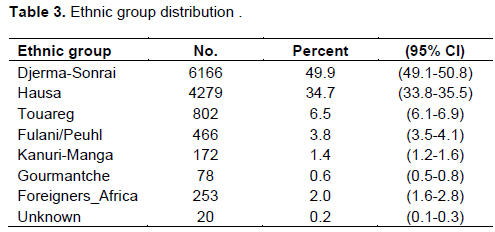
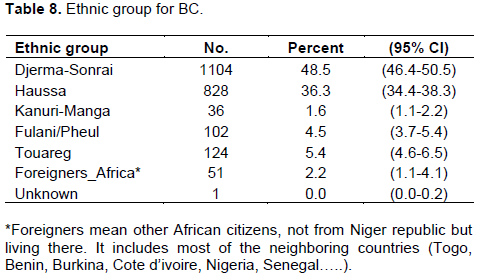
From this sample, the main reported ethnic groups are Djerma-Sonrai 49.9 (49.1-50.8) and Haussa 34.7 (33.8-35.5). It should be noted that from the country’s general statistics, the main ethnic groups in Niger are Hausa (54.0%) and Djerma/Sonrai (22.2%). We also have Tuareg (10.0%), Fulani (Peuhl) 6.5%, Kanuri 5.9%, other small groups include Gourmantchés, Arab and Tubu. Niamey is populated by many different ethnic groups, although Djerma and Haussa are the majority.
The overall pooled average cancer patient’s age is 44.7 (44.4-45) years. The average age of male patients is 45.0 years (44.4-45.5) while the average age of female patients is 44.4 years (44.1-44.8).
Breast cancer patients
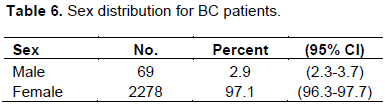
The average age of BC patients is 46.0 years (45.4 - 46.5). For male patients it is 54.7 years (51.1 - 58.2) while the average age for female patients is 45.7 (45.1-46.2) years. Reported mortality for BC is 9.7%, that is, the proportion of cancer patients that have died since the startup of the cancer registry. It should be noted that not all death cases are systematically reported, and follow up of death cases remains a challenge, depending on patients’ trajectory and information availability. 97.1% of breast cancer burden are female cases.
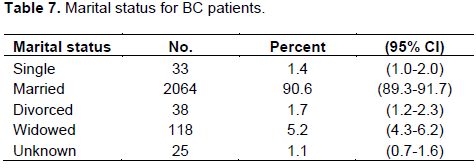
The two main ethnics groups of Djerma-Sonrai and Hausa are the majority. This reflects the main ethnic groups in Niger.
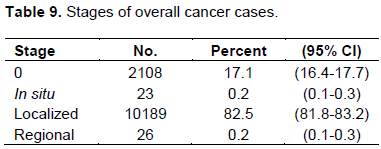
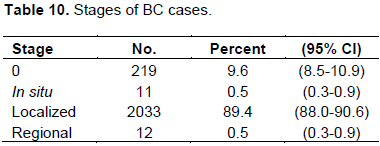
Stage of cancer cases
As for all cancers, diagnosis method for breast cancers is mainly clinical, then histological and cytological as explained earlier.
Trend analysis
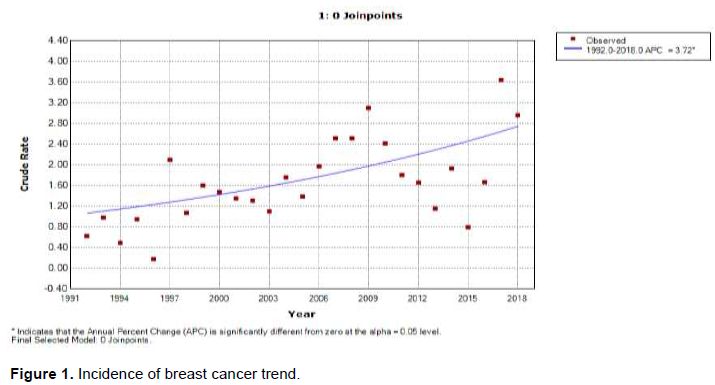
Breast cancer incidence grew in Niger from 1992 to 2018 with a significant annual percentage change (APC) of 3.7 (1.5-6) from 1992 to 2018. Despite a slow startup, cancer data registration saw an increase from 2000 to 2010 with a boost in 2003. Recently, with the help of the National Center for the Fight Against Cancer, Ministry of Health teams started supporting data collection within the country for a wider coverage, which is why there is an increase from 2016 (Figure 1).
Survival analysis, modeling of factors associated with BC survival
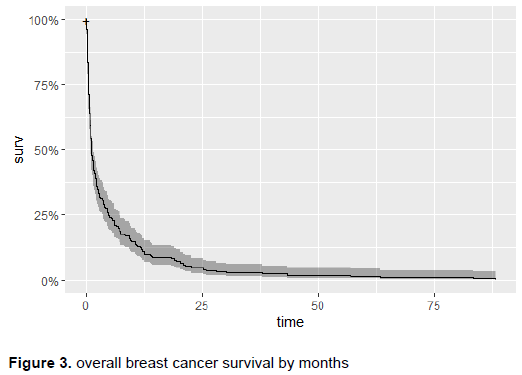
Overall BC survival was found to be low; it turned out to be 13% at 12 months. Both univariate and multivariate Cox proportional hazards models were fitted with age, sex, diagnosis method and marital status as covariates. Results are shown in Table 1 to12.
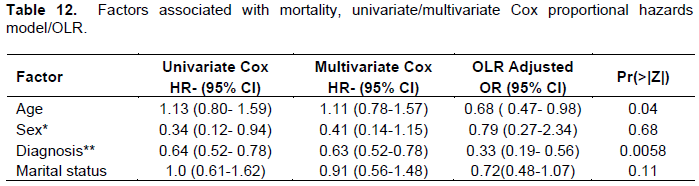
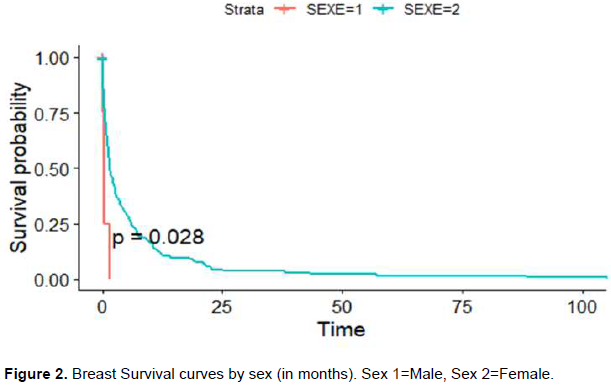
On univariate analysis, sex and diagnosis method (histological) were associated with BC survival. Patients diagnosed with histological conformation had a lower hazard of dying. With multivariate analysis, a lower death risk was found also for patients with histological confirmation. Most of the time, patients with histological confirmation were undergoing treatment, mainly surgical. Many patients were diagnosed clinically and these include most liver cancer cases (Figure 2).
DISCUSSION
The current study demonstrated that breast cancer is the most common cancer followed by gynecological cancers (cervical and ovarian) in Niger; this is in line with findings from Salamatou et al. (2013) who explored 17 years of cancer registry data in Niger (from 1992 to 2009). They reported that BC is the most frequent female cancer (27.4%) followed by cervical cancer (13.4%) and ovarian cancer (8.83%). Cancer affects more women than men in Niger. For BC, the majority of cases occur in women. The unbalanced sample size between the two sexes will not allow us to focus on comparison (Figure 3).
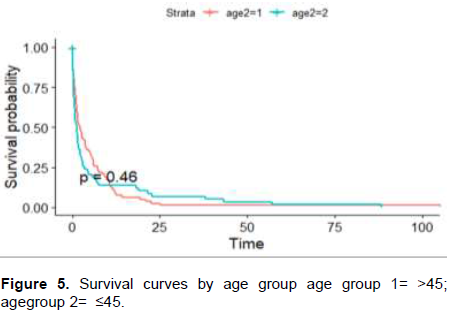
In this study, an overall average cancer patient’s age of 44.7 (44.4-45) years and an average age for BC patients of 46.0 years (45.4 - 46.5) was found. Nayama et al. (2006) reported an average age of 36.5 years for cancer patients. Zaki et al. (2013) reported an average age of 44.1 years in BC women patients. Cancer patients’ age is documented to be low generally in Africa as compared to other parts of the world (Joko?Fru et al., 2020b; Dickens et al., 2014; Ibrahim and Oludara, 2012), as is also the case for Niger (Figure 5).
This study found an increasing BC incidence trend in Niger over the 27 years of cancer registry. Many recent studies reported a continuously increasing BC incidence in sub-Saharan Africa (Azubuike et al., 2018; Brinton et al., 2014). Reporting on the GLOBOCAN 2018, Bray et al. (2018) estimated the age standardized BC incidence to be 37.3/100,000). In Western Africa, Sighoko et al. (2013) have analyzed trends of BC over two different periods in two population-based cancer registries, in Mali (1987-1997; 1998-2009) and in The Gambia (1988-1997; 1998-2006). They found that BC incidence rates have increased by 20% (incidence rate ratio (IRR)) 1.20 (1.07-1.35) in Bamako (Mali), with an annual percentage change of 2.0% (0.4-3.6). Moreover, they found a similar pattern in The Gambia for women under 50 years, IRR 1.47 (1.07-2.01). In the Niger context, the opening of some small-scale centers where cancer diagnosis is done, a cancer screening campaign from a non- governmental organization (SOS Cancer Niger), and the creation of the new national center for the Fight Against Cancer, have all contributed to the wider cancer screening scope and growing incidence.
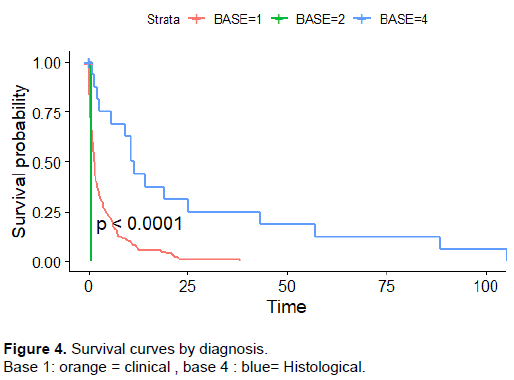
Overall BC survival was found to be low. First of all, the reader should be cautioned that the Niger Cancer Registry is located in Niamey and patients coming from the 7 other regions of the country are not easily traceable for mortality information. Patient results are very often censored, incomplete information is available about the survival time and it is not absolutely clear whether death is due to cancer or other causes. In short, follow up remains a recognized challenge in the country, given the available resources of the cancer registry network. On univariate analysis, sex and diagnosis method (histological) were associated with BC survival. With multivariate analysis, we found only a higher hazard for patients with histological confirmation. Patients clinically diagnosed are mainly those that attend health centers at advanced stages, hence their higher mortality (Figure 4).
Surgery or other treatments could only be palliative.
The Breast Cancer Survival and Survival Gap Apportionment in sub-Saharan Africa (ABC-DO) prospective cohort study by McCormack et al. (2013) was conducted at eight hospitals across five sub-Saharan African countries (Namibia, Nigeria, South Africa, Uganda, and Zambia). It reported about 50% (48-53), 3-year overall survival globally. Nevertheless, they observed significant variations between different countries (44% in Uganda, 47% in Zambia vs 36% in Nigeria which is closer to Niger). From this data, less than 10% of Niger patients have 3-year survival. In a recent study by (Joko?Fru WY, 2020a) entitled “Breast cancer survival in sub?Saharan Africa by age, stage at diagnosis and human development index: A population?based registry study’’, age at diagnosis was found to be associated with increased mortality risk after adjusting for the effect of stage and country-level Human Development Index (HDI). They analyzed 2,588 BC cases, diagnosed in 2008-2015 from 14 population-based cancer registries in 12 countries: Benin, Cote d'Ivoire, Ethiopia, Kenya, Mali, Mauritius, Mozambique, Namibia, Seychelles, South Africa, Uganda and Zimbabwe. (Allemani et al., 2015) found that five-year relative survival estimates range from 12% in parts of Africa to almost 90% in the United States, Australia and Canada. In Saudi Arabia, the relative survival probabilities at one, three and five years from the incidence data were 96, 83 and 65%, respectively, with the differential linked to a combination of early detection, access to treatment services and cultural barriers.
CONCLUSION
Cancer incidence and mortality are growing in Niger, and overall BC survival remains low. The prominence of breast and gynecological cancers explained the majority of female cancers. This study should contribute to setting out milestones for further research. Given the scarcity of epidemiological research on BC in Niger, there is need to conduct more studies, especially on cancer trends and survival.
RECOMMENDATIONS
Based on the findings of this, study, it could be recommended to strengthen screening and report to the cancer registry for a wider coverage. More human resources are needed to analyze laboratory samples. Main hospitals (at least the university teaching hospital and national reference hospital) should be equipped with mammography equipment.
LIMITATIONS
The limitations of this study include the coverage of the Niger cancer registry, especially in the first year of its creation, when the registry reported cancer cases in Niamey and the surroundings before expanding to inner regions of the country. Moreover, lack of proper information on some patient’s follow-up can influence the survival of patients.
The study was approved by the Faculty of Health Sciences, Abdou Moumouni University, Niamey, Niger and the Head of the Laboratory of Pathological Anatomy and Cytology (reference number: 0331/10-03-2020).
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adeloye D, Sowunmi OY, Jacobs W, David RA, Adeosun AA, Amuta AO, Misra S, Gadanya M, Auta A, Harhay MO, Chan KYEstimating the incidence of breast cancer in Africa: A systematic review and meta-analysis. Journal of Global Health 8(1). |
|
|
Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang XS.CONCORD Working Group. (2015). Global surveillance of cancer survival 1995-2009: analysis of individual data for 25 676 887 patients from 279 population-based registries in 67 countries (CONCORD-2). The Lancet 385(9972):977-1010. |
|
|
Azubuike, Samuel O., Colin Muirhead, Louise Hayes, and Richard McNally (2018). Rising global burden of breast cancer: the case of sub-Saharan Africa (with emphasis on Nigeria) and implications for regional development: a review. World Journal of Surgical Oncology 16(1):1-13. |
|
|
Black E, Richmond R (2019). Improving early detection of breast cancer in sub-Saharan Africa: why mammography may not be the way forward. Globalization and health 15(1):1-11. |
|
|
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a Cancer Journal for Clinicians 68(6):394-424. |
|
|
Brinton LA, Figueroa JD, Awuah B, Yarney J, Wiafe S, Wood SN, Clegg-Lamptey JN (2014). Breast cancer in Sub-Saharan Africa: opportunities for prevention. Breast cancer research and treatment 144(3):467-478. |
|
|
Dickens C, Joffe M, Jacobson J, Venter F, Schüz J, Cubasch H, McCormack V (2014). Stage at breast cancer diagnosis and distance from diagnostic hospital in a periurban setting: a South African public hospital case series of over 1,000 women. International Journal of Cancer 135(9):2173-2182. |
|
|
Salamatou G, Zaki HM, Arfaoui A, Hami H, Soulaymani A, Nouhou H, Quyou A (2013). Épidémiologie des cancers au Niger, 1992 à 2009. Bulletin du cancer 100(2):127-133 |
|
|
Ibrahim NA, Oludara MA (2012). Socio-demographic factors and reasons associated with delay in breast cancer presentation: a study in Nigerian women. The Breast 21(3):416-418. |
|
|
Joko?Fru WY, Jedy?Agba E, Korir A, Ogunbiyi O, Dzamalala CP, Chokunonga E, Parkin DM (2020b). The evolving epidemic of breast cancer in sub?Saharan Africa: Results from the African Cancer Registry Network. International Journal of Cancer 147(8):2131-2141. |
|
|
Joko?Fru WY, Miranda?Filho A, Soerjomataram I, Egue M, Akele?Akpo MT, N'da G, Parkin DM (2020a). Breast cancer survival in sub?Saharan Africa by age, stage at diagnosis and human development index: A population?based registry study. International Journal of Cancer 146(5):1208-1218. |
|
|
Mamoudou SG, Hami H, Mahamadou HZ (2013). Profil épidémiologique et anatomopathologique du cancer du sein au Niger'',Journal Africain du Cancer/African Journal of Cancer 5(4):185-191. |
|
|
McCormack V, McKenzie F, Foerster M, Zietsman A, Galukande M, Adisa C, dos-Santos-Silva I (2020). Breast cancer survival and survival gap apportionment in sub-Saharan Africa (ABC-DO): a prospective cohort study. The Lancet Global Health 8(9):e1203-e1212. |
|
|
Mohammed SI, Harford JB (2014). Sorting reality from what we think we know about breast cancer in Africa. PLoS medicine 11(9):e1001721. |
|
|
Nayama M, Nouhou H, Souna-Madougou K, Idi N, Garba M, Tahirou A, Touré A (2006). Cancers gynecologiques et mammaires: aspects epidemiologiques et histologiques dans le service d'anatomie et cytologie pathologique de la Faculte des Sciences et de la Sante de Niamey Niger 21(3):43-49. French. PMID: 19435008. |
|
|
Sighoko D, Kamate B, Traore C, Malle B, Coulibaly B, Karidiatou A, Hainaut P (2013). Breast cancer in pre-menopausal women in West Africa: analysis of temporal trends and evaluation of risk factors associated with reproductive life. The Breast 22(5):828-835. |
|
|
UNICEF and UNESCO. |
|
|
WHO Cancer Country profiles (2020). |
|
|
Youlden DR, Cramb SM, Dunn NA, Muller JM, Pyke CM, Baade PD (2012).The descriptive epidemiology of female breast cancer: an international comparison of screening, incidence, survival and mortality. Cancer Epidemiology 36(3):237-248. |
|
|
Zouladeny H, Dille I, Wehbi NK, Kim J, Soliman AS (2015). Epidemiologic and clinical profiles of breast diseases in Niger. International journal of cancer and oncology 2(2):1-6. |
|
|
Zaki HM, Garba-Bouda O, Garba SM, Nouhou H (2013). Profil épidémiologique et anatomopathologique du cancer du sein au Niger. Journal Africain du Cancer/African Journal of Cancer 5(4):185-191. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


