Full Length Research Paper

ABSTRACT
National health policies that take into cognizance the interventions against the menace of students’ ill health in Nigeria are limited. This study investigated the health status of students in tertiary institutions in Bayelsa State. A descriptive study design was adopted to randomly select four tertiary institutions out of six. Two hundred students were randomly selected from the four schools; fifty from each school. Structured questionnaires containing symptoms-specific ill health were distributed to the selected students. One hundred and fifty-five questionnaires used for the analyses were retrieved. Thirty six specific health symptoms perceived by the students were classified following WHO standard. Out of 561 students-symptoms, 35.6% were mental health while 34.6% were infectious. More female (66.53%) than male (60.14%) showed mental health symptoms. The differences were not significant (P>0.05). Students who had lived in urban location had more mental than those that resided in rural location. The differences were significant (P<0.05). The symptoms decreases as age increased. 60.1% of the students developed these health challenges as they got admitted into schools while 39.9% of the students had the problem at home before admitted to the school. The symptoms of the student’s mental health increased as parents’ income improved. The implication of these results is a cause for prompt public health intervention.
Key words: Mental health, infectious health, students, tertiary institutions, Bayelsa State.
INTRODUCTION
Tertiary institution students represent higher percentages of adolescent, which is the period that marks transition from youthful age to adulthood (World Youth Report (WYR), 2003).Tertiary education represents a transitional period of a new independence life from their parents and a dependent life at school. The period is characterized by rapid interrelated changes both of body,mind and social relationship (National School Climate Council (NSCC), 2007).
Health, according to World Health Organization is the state of complete physical, mental and social well-being and not merely the absence of diseases and infirmity (WHO, 2002). University students are more vulnerable to various kinds of health problems, ranging from increased stresses to unhealthy lifestyle (Adewuya, 2006; Nerdrum et al., 2006; Ovuga et al., 2006; Stewart-Brown et al., 2000). The major health challenges identified among students in the tertiary institution are mental health, psychological problem, infectious diseases and emotional disorder (Tomoda et al., 2000). However, mental health has been more associated with adolescent. It accounted for 11.5% of the global disease burden (World Health Organisation (WHO), 2007). Over 450 million people worldwide are estimated to be suffering from some form of brain or mental disorder. In Nigeria alone, the prevalence of mental illness is reported at 20% (Shekihar, 2006).
Mental health is a major public health challenge, yet suffers institutional neglect. Over 30% of countries lack good mental health policy. Although in Nigeria Mental Health Policy was formulated in 1991 at Lagos, yet the implementation was not readily available (Mental Health Leadership and Advocacy Programme (MHLAP), 2012). The impact of lack of mental health policy implementation has created high rates of neglect, stigmatization, and streets roaming of the sufferers. The mental ill health has also impacted negatively on the educational outcomes among university students (Brackney and Karabenick, 1995). Despite these problems, the National health policies that take into cognizance interventions against the menace of students’ mental ill health in Nigeria is lacking.The early Identification of the mental related health conditions of students in the tertiary institutions is a pre requisite to providing a long lasting solution to students’ ill health. This information is lacking among students in the tertiary institutions in Bayelsa State, Nigeria. The aim of this study was to investigate the health status of students in tertiary institutions in Bayelsa State.
MATERIALS AND METHODS
Study area
This study was conducted in four of the six tertiary institutions in Bayelsa State, viz; Niger Delta University, Amassoma in Southern Ijaw Local Government Area (6°15′N and 6°14′E); Isaac Jasper Boro College of Education, Sagbama, Sagbama LGA (5°9′N and 16°14′E); Bayelsa State School of Nursing, Tombia, Yenagoa Local Government Area (4°53′N and 5°17′E) and Bayelsa State School of Health Technology, Otuogidi, Ogbia LGA (4°36′N and 5°45′E). These institutions were selected based on accessibility at the time of the study. Also the institutions were selected on local government basis. Southern Ijaw and Yenagoa LGAs had two tertiary institutions each. The most accessible was purposefully selected.
Study design
The study adopted a cross sectional study to determine the health status among students attending tertiary institutions in Bayelsa State, from January-March, 2016.
Sampling technique and data collection
The study population comprised all six tertiary institutions in Bayelsa State. These are; Niger Delta University, Amassoma, Federal University, Otuoke, Federal Polytechnics, Ekewe, Isaac Jasper Boro College of Education, Sagbama, Bayelsa State School of Nursing, Tombia and Bayelsa State School of Health Technology, Otuogidi. Four institutions were purposefully selected based on accessibility at the prevailing time. The samples include all the students in the selected schools. The study included only the new intakes students and those who were in their 3rd Year. The 3rd Year students were used because apart from Niger Delta University, every other institution runs a three-year program; hence the 3rd year is an equivalent of the final year in a four-year program. Although the total population of the schools was not known at the time of study, since the new intake were still undertaking registration process, the proportion of new intakes and third year students was in a ratio of 2:1 across the schools. For these reasons, fifty students from each institution were randomly selected based on willingness to supply data. From each institution, forty new intakes and twenty 3rd Year students were engaged after showing their willingness. Thirty-five new intakes and fifteen Year Three students from each institution who satisfy the inclusion conclusion were randomly selected, making up a total sample size of two hundred (200) students.
Research instrument
200 self-reporting questionnaires tagged: “The health status of students in tertiary institution (HSOSTS) in Bayelsa State” containing 40 items modified by World Health Organization (WHO) were distributed to the randomly selected students in the four institutions (fifty questionnaires for each institution) by a practicing doctor. Each questionnaire comprise two sections; A and B. Section A contained demographic information of students and parents while Section B contains items that elicit the response of the students on their perceived health challenges. The personal information included in the questionnaire was the sex, age, and residential location, year of study and occupation of parents of the students. Other information includes sets of mental and infectious health related symptoms supplied by a practicing doctor.
Ethical consideration
Prior to the distribution of questionnaires, ethical clearance (in the form of a verbal consent) was obtained during a pre meeting with the institutional heads and participating students to seek their consent. This was granted after the purpose and benefits of the study was properly explained to the institution’s head. The self-designed questionnaire was administered to randomly selected students to fill; thereafter, 145 duly filled questionnaires were retrieved from the respondents. The remaining fifty questionnaires were retrieved unfilled; hence, excluded in the data analyses. Only data retrieved were used for all the analyses.
Method of data analyses
Data were cleaned up and cross-checked for correctness before analysis. These were thereafter entered to Microsoft Office Excel 2007 and then exported to SPSS version 16.0 for analysis. Both descriptive and analytical statistical procedures were utilized. Descriptive statistics like percent mean and standard deviation were used for the presentation of demographic data and classification of health challenges. Significant differences of the mental health, infectious health of students of various sexes, age group and parental background across institutions were determined in ANOVAs at a confident level of 0.05.
RESULTS AND ANALYSIS
Demographic information
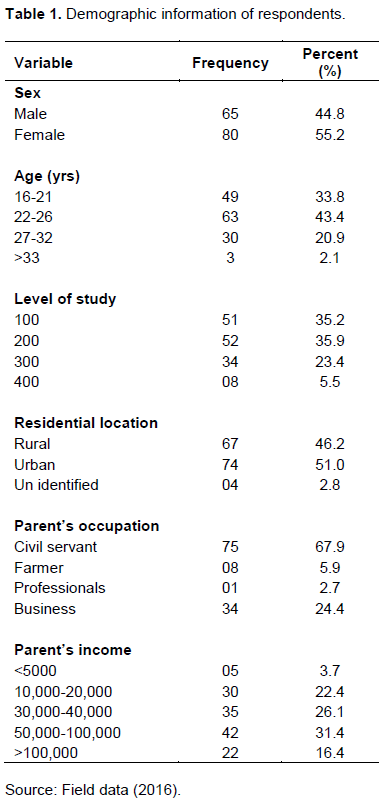
Out of the one hundred and forty-five (145) questionnaires retrieved, male respondent accounted for 44.8% while female accounted for 55.2%. 46.2% of the total respondents reside in rural area, 51.0% lives in urban area while 2.8% did not indicate residential area. The respondents of the students according to their year of studies are; 100 level (35.2%), 200 level (35.9%), 300 level (23.4%) and 400 level (5.5%).
The parent’s characteristics were also described by their occupation and income level. Higher percentage of the student’s parents were civil servant (67.9%), followed by business (24.4%). The differences were statistically significant (χ2 =26.62; df= 5; p< 0.05). The income level (naira) in the increasing order are; <5000 (3.7%), > 100,000 (16.4%), 10,000-20,000 (22.4%), 30,000-40,000 (26.1%), 50,000-100,000 (31.3%). Details are shown Table 1.
Perceived health status of students in tertiary institution in Bayelsa State during January to December, 2016
Thirty-six (36) health specific-symptoms classified by WHO were presented to students in the study institutions. Out of the 36 symptoms presented, 15 symptoms representing 41, 66% were significantly accepted across the institutions (F= 426.528; df= 1; p-value=0.000; p<0.05) (Table 2). Twenty-four (24) symptoms representing 66.7% were mental health while 12(33.3%) were infectious health.
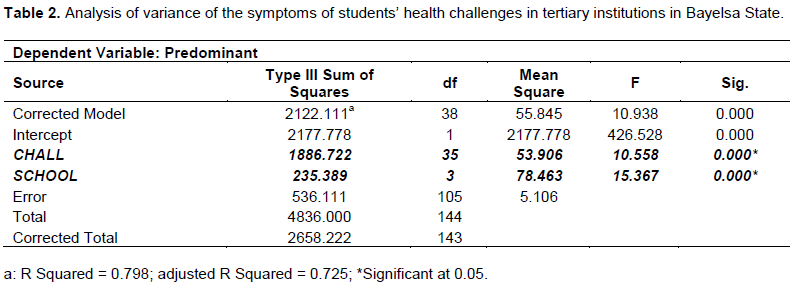
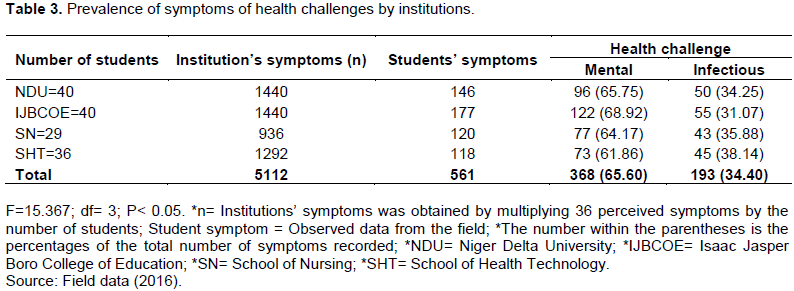
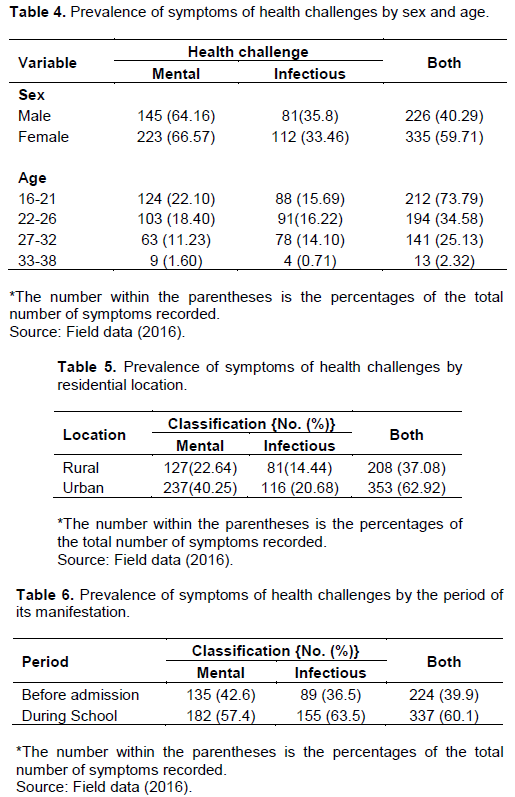
Five hundred and sixty one (561) students’ symptoms were pooled across the institutions. 65.6% had mental health while 34.6% had infectious health. The differences in students’ health status were significant (F=10.558; df=35; p<0.05). The similar trend was recorded across institutions (F=15.364; df=3; P< 0.05) (Table 3). Prevalence of the students-symptoms status showed sex differences. Symptoms of mental health were higher in female (66.53%) than in male (60.14%). Male showed more symptoms of infectious health (35.45%) than the female (33.45%). The differences were not statistically significant (χ2 =0.77; df= 3; P > 0.05). The symptoms of both mental and infectious health decreases as the age of the student increased (Table 4). Variations also exist in the symptoms of the ill health across students’ residential locations. Students that reside in the urban areas manifest more symptoms of mental and infectious health (mental- 70.25%; infectious- 20.65%) than those that reside in the rural location (mental- 20.68%; infectious- 14.44%). The differences were significant (χ2=24.46; df=1; p< 0.05) (Table 5). The health challenges of students were acquired at different period; some were acquired before gaining admission to the tertiary institution while some develop after gaining admission. From the result, 60.1% of the symptoms were developed after gaining admission while 39.9% were acquired before gaining admission into the school. The trends in the manifestation of the symptoms were similar for both mental and infectious health challenges (Table 6).
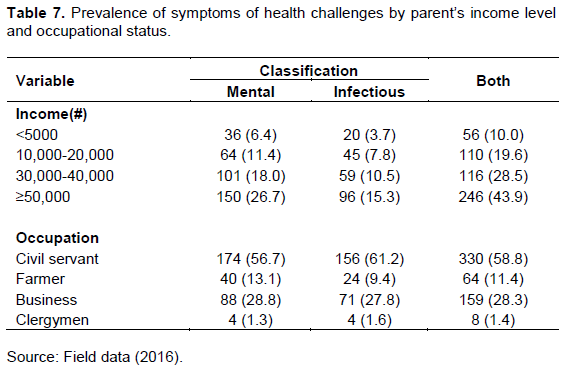
Prevalence of student symptoms health status by parent’s socio-economic status
Disparity exist between parents income level and students health challenges. The symptoms of students’ mental and infectious health increased as the parents’ income level increases. The disparity was not statistically significant. More so, students whose parents were civil servant showed more symptoms of both mental and infectious health while lower symptoms were observed among students whose parents were clergymen. The differences were statistically significant (χ2 = 2.18, df= 3; p> 0.05) (Table 7).
DISCUSSION
The health status of tertiary school students in Bayelsa State was more of mental illness (65.6%) than infectious illness (34.6%). This highlighted the fact that students are more vulnerable to psychological illness than communicable diseases. This observation is consistent with the report of Benton et al. (2003) and Eisenberg et al. (2007). Both acknowledged that students are more vulnerable to mental health problems than the general population. The vulnerability of students to mental health had been attributed to stress of academic pressures, adjustment to meet up with the challenges of adulthood, the demands of practical life and maintaining relationships with others (Rodgers and Tennison, 2009). The prevalence of mental health symptom in this present study was higher than the report elsewhere. Redhwan and Dhekra (2012) reported a prevalence of 48.3% of emotional disorders from among 338 students’ in Malaysian university. Berihun et al. (2015) reported 40.9% prevalence of mental distress among undergraduate students of University of Gondar, Northwest Ethiopia. Sadia and Zahid (2013) reported 31% severe mental health and 16% very severe mental health with 1850 students in six public sector universities of Lahore, Pakistan. The observed prevalence of severe and moderate depression (7.0 and 25.2%) among tertiary institution students in western Nigeria, as revealed in this study is a call for urgent public health intervention (Karl et al., 2013).
The prevalence of mental health was sex-specific. Higher prevalence in female than in male has been reported (Adewuya, 2006; Sadia and Zahid, 2013). The differences is an indication that female lack competence in managing their health challenges (Chew-Graham et al., 2003), or may show more proneness to anxiety (Eisenberg et al., 2007).
Mental health symptoms decreases as the age of the student increased. This observation has also been reported by (Tosevski et al., 2010). Variations of the symptoms by age may be connected with the ability to cope with anxiety and stress. In the present study, higher percentage of mental health symptoms was between 16 to 21 years. These subjects are within teenage age and slightly within adolescent age. The reduced ability to cope with anxiety and stress has been reported among similar age bracket elsewhere (Bostanci et al., 2005). Other reports (Wong et al., 2006; Stallman, 2010) have attributed the high percentage to the inability of students within this age bracket to openly discuss their psychological problems with friends.
Residential locations also affect the manifestation of ill health among students. In this study, students who resided in urban areas experienced more health challenges than students that had resided in rural areas; an observation that contrasted the report of Redhwan and Dhekra (2012) who reported that emotional disorder was less among urban students than rural students.
However, similar reports by Muhammad (1993) attributed the differences to the lifestyle and family background of students in these different locations.
The variation in the manifestation of mental and infectious health in students at different stages of their school life agrees with Fisher et al. (2003). Higher percentages of the students manifested the symptoms after they had been admitted to school. Gately (2005) asserted that the onset of mental illness often occurs during early childhood or adolescence, but it became more compounded when such individual struggle to cope with the stress and anxiety at school.
Parents’ income level had shown significant impact on the health conditions of students (Ovuga et al., 2006). Students in this study whose parents earn higher income experienced higher symptoms of both mental and infectious ill health; an observation that contrasted the report of Eisenberg et al. (2007). The occupation of students’ parents showed significant relationship.
However, the reasons why students whose parents are civil servants showed higher prevalence of mental symptoms than students whose parents are clergymen lacks explanation within the scope of this present study.
CONCLUSION AND RECOMMENDATION
The prevalence of mental and infectious distress among students in tertiary institution in Bayelsa State was found to be high. The prevalence was relatively high among female students than in male and decrease as age increases. Students that live in urban areas showed more vulnerability to ill health than those that live in rural areas. Most students manifest symptoms of ill health at the time they had admission into higher institution. Parents’ income level and occupation included factors associated with mental and infectious health challenges of students in the tertiary institution. It is recommended therefore that adequate attention be given to students as regards recognizing their health status as early as possible. Policy makers, college officials, non-governmental organizations, and parents, should show more concern to the health status of students. Programs aimed at preventing mental distress need to be introduced in schools so as to identify factors leading of mental distress at the early stage. Also, Counseling Unit should be established in each institution.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adewuya AO (2006). Prevalence of major depressive disorder in Nigerian College students with alcohol-related problems, General Hospital Psychiatry 28:169-173. |
|
|
Benton SA, Robertson JM, Tseng W, Newton FB, Benton SL (2003). Changes in counseling center client problems across 13 years professional psychology, research and practice 34:66-72. |
|
|
Brackney BE, Karabenick SA (1995). Psychopathology and academic performance: The role of motivation and learning strategies. Journal of Counseling Psychology 42(4):456. |
|
|
Bostanci M, Ozdel O, Oguzhanoglu NK, Ozdel L, Ergin A, Ergin N, Atesci F, Karadag F (2005). Depressive symptomatology among university students in Denizli, Turkey: prevalence and socio demographic correlates. Croatian Medical Journal 46(1):96-100. |
|
|
Chew-Graham CA, Rogers A, Yassin N (2003). 'I wouldn't want it on my CVor their records':medical students' experiences of help-seeking for mentalhealth problems. Medical Education Journal 37:873-880. |
|
|
Eisenberg D, Gollust SE, Golberstein E, Hefner JL (2007.). Prevalence and correlates of depression, anxiety, and suicidality among university students, American Journal of Orthopsychiatry 77(4):534-542. |
|
|
Fisher WA, Fisher JD, Harman J (2003). The information-motivation-behavioral skills model: a general social psychological approach to understanding and promoting health behavior. In: Suls J, Wallston KA, editors. Social psychological foundations of health and illness. Oxford: Wiley-Blackwell pp. 82-106. |
|
|
Gately G (2005). Colleges target mental health campus: Groups, courses, online services help reduce the stigma of treatment. |
|
|
Karl P, Limpopo T, Supa P (2013). Depression and Associated Factors among University Students in Western Nigeria. Journal of Psychology in Africa 23(3):459-466. |
|
|
Mental Health Leadership and Advocacy Programme (MHLAP) (2012). Mental Health Situation Analysis In Nigeria.The report of Mental Health Leadership and Advocacy Programme of the department of Psychiatry, University of Ibadan in collaboration with WHO centre for research and training in mental health, Neurosciences and drug and Alcohol abuse, |
|
|
Mohammad A (1993). Adolescent girls and their rights: health of adolescent girls, with special emphasis on reproductive and sexual health and nutrition", a paper prepared for the United Nations Expert Group Meeting on Adolescent girls and their Rights, Addis Ababa pp. 13-17. |
|
|
National School Climate Council (NSCC) (2007).The school climate challenge Narrowing the gap between school climate research and climate policy, practice guideline and teacher education policy. |
|
|
Nerdrum P, Rustoen T, Ronnestad M (2006). Student psychological distress:a psychometric study of 1750 Norwegian 1st-year undergraduate students. Scandinavian Journal of Educational Research 50:95-109. |
|
|
Ovuga E, Boardman J, Wasserman D (2006). Undergraduate student mental Health at Makerere University, Uganda. World Psychiatry 5(1):51-52. |
|
|
Redhwan AA, Dhekra HA (2012). Prevalence and Associated Factors of Emotional Disorder among Malaysian University Students. International Journal of Collaborative Research on Internal Medicine and Public Health 4:1401-1411 |
|
|
Rodgers LS, Tennison LR (2009). A preliminary assessment of adjustment disorder among First-Year College Students. Archives of Psychiatric Nursing 23(3):220-230. |
|
|
Sadia S, Zahid M (2013). Mental Health Problems in University Students: A Prevalence Study. FWU Journal of Social Sciences 7(2). |
|
|
Shekihar S, Gureje O (2006).WHO-AIMS Report on Mental Health System in Nigeria, WHO and Ministry of Health Ibadan, Nigeria P 15. |
|
|
Stewart-Brown S, Evans J, Patterson J, Petersen S, Doll H, Balding J, Regis D (2000).The health of students in institutes of higher education: an important and neglected public health problem? Journal of Public Health Medicine 22(4):492-499. |
|
|
Stallman HM (2010). Psychological distress in university students: a comparison with general population data Australian Psychologist 45(45):249-257. |
|
|
Tosevski DL, Milovancevic MP, Gajic SD (2010). Personalityand psychopathology of university students Current opinion in psychiatry 23(1):48-52. |
|
|
Tomoda A, Mori K, Kimura M, Takahashi T, Kitamura T (2000). One-year prevalence and incidence of depression among first-year university students in Japan: a preliminary study. Psychiatry and Clinical Neurosciences 54(5):583-588. |
|
|
World Youth Report (WYR) (2003).Youth and Health Issues, P 102. |
|
|
World Health Organisation (WHO) (2002). Health Environments for Children: Initiating an alliance for Action. Geneva. |
|
|
World Health Organisation (WHO) (2007). World Health Statistics (Geneva: WHO, 2007) 68. |
|
|
Wong JGWS, Cheung EPT, Chan KKC, Ma KKM, Tang SW (2006). Web-based survey of depression, anxiety and stress in first-year tertiary education students in Hong Kong. Australian and New Zealand Journal of Psychiatry 40(9):777-782. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


