ABSTRACT
The Ebola Virus Disease (EVD) outbreak in West Africa in 2014 resulted in cases spreading to other parts of the world, such as the United States of America (USA). A survey was carried out among Meharry Medical College residents to ascertain their knowledge of Center of Disease Control and Prevention (CDC) guidelines on prevention and management of EVD. A structured questionnaire was administered to a cross-section of residents at Meharry Medical College between December 2014 and January 2015. A total of 60 residents participated in the survey. Of these, 11 (18.3%) were psychiatry residents, 5 (8.3%) each were preventive and occupational medicine residents, while 13 (21.7%) and 26 (43.4%) were family and internal medicine residents, respectively. Compared to other specialties, resident physicians in occupational medicine had higher knowledge of the first step in the management of Ebola virus (EBOV) (p=0.042). On whether use of personal protective equipment (PPE) was required for individuals driving or riding in a vehicle carrying human remains of EBOV patients, only 10 respondents (16.7%) answered correctly, with preventive medicine residents performing significantly better than other physicians (p<0.0001). In conclusion, this study identified that resident physicians have a low level of knowledge regarding the presentation, prevention and management of EVD, including handling post-mortem remains. This study highlights the importance of educational interventions to improve knowledge on EVD prevention and management.
Key words: Ebola virus disease, Ebola hemorrhagic fever, infectious disease, awareness, Knowledge, attitude and perception (KAP), medical residents, knowledge, attitudes, Ebola epidemic.
Ebola virus (EBOV) outbreaks have a devastating impact on the health care system, especially in sub-Saharan African countries with a health care system that is sub-par. An outbreak presents major challenges to these countries and their public health systems. EBOV was first discovered near the Ebola River in Zaire, now Democratic Republic of Congo in 1976 (CDC, 2015). Transmission of this virus occurs by direct contact through broken skin or mucous membranes; blood or body fluids of an infected Ebola patient, contaminated objects, or through infected fruit bats or primates (CDC, 2015). There have been approximately 20 outbreaks of Ebola virus in Africa with a reported fatality rate of 25 to 90% (WHO, 2015).
Previous outbreaks have been reported in the Democratic Republic of Congo (2008 to 2009, 2012, 2014), Gabon (2002), Republic of Congo (2002 to 2003), and Uganda (2007 to 2008, 2012) (Blaize et al., 2014). Ebola virus is known to be endemic in sub-Saharan Africa. The Ebola outbreak which began in March 2014 affected Sierra Leone, Liberia, Nigeria, Guinea, Mali, Spain, Senegal, and USA. Zaire Ebola virus species, which is the most active of the Ebola Virus Disease (EVDs), was reported to be the etiologic agent of the EVD in Africa (CDC, 2014). The 2014 Ebola outbreak was reported to be the largest and worst in history to date with a case fatality rate of 60 to 87% in the first few months of the outbreak (Sarwar et al., 2015). By August and October 2014, EBOV had crossed international boundaries to spread to countries in Europe and the USA respectively.
Majority of the people who had been infected with Ebola virus in the USA were those who had gone to provide supportive care for Ebola patients in Africa. The onset of reported cases of transmission in the USA resulted in the Center of Disease Control and Prevention (CDC) issuing recommendations to prevent further spread of the virus amongst USA healthcare institutions and the general public. Little is known about the knowledge, attitudes and practices of physicians in the USA and for purposes of this study in the southeast region of the USA, particularly residents who are always the first point of contact for patients that may be admitted into the hospital with EVD. This study assessed the knowledge of CDC recommendations for the prevention and management of EVD amongst resident physicians at Meharry medical college.
Setting
The study was conducted at Meharry Medical College located in Nashville Tennessee, USA.
Study subjects
Subjects were Meharry medical resident physicians. A total of 60 resident physicians participated in the survey comprising 63.13% of the resident population (n=95). Five specialties were represented: Family medicine, internal medicine, psychiatry, occupational medicine, and preventive medicine.
Survey design and distribution
A cross sectional survey was conducted between December 2014 and January 2015. The survey questionnaire was developed based on a literature review of EVD, specifically from the CDC recommendations on the prevention and management of EVD. The study questionnaire was self-administered during a noon conference or morning report of each residency program, and the questionnaires were collected at the end of the noon conference or morning report. The first section of the survey was demographic information. The subsequent parts of the survey were testing the resident’s knowledge on signs and symptoms of EVD, prevention, transmission, treatment, and handling of deceased Ebola patient. A total of 30 items developed from the literature search were tested. The survey was anonymous. The Intuitional Review Board of Meharry Medical College approved the survey after review by the Ethics Committee. There was a disclaimer reinforcing the fact that the survey was voluntary and that no identifying information will be collected to connect them to their responses.
Statistical analysis
The statistical package for social sciences (SPSS) 22.0 (SPSS Inc., Chicago, IL) was used for analysis of the data. The data from the survey were coded using appropriate data library and entered into SPSS 22.0. The data for age was grouped and entered as numerical data while the results from the study was coded using 1 for yes, 2 for no and 0 for omission. Descriptive statistics were reported in terms of percentages. Chi-square test was performed to compare answers between the residencies. P<0.05 was set as the statistically significant value.
A total of 60 residents participated in the survey. Of these, 53.3% were male, 46.7% were female, 58.3% were international medical graduates, 41.7% were American Medical Graduates and 43.3% have graduated from medical school within 5 to 10 yrs. with the remaining 56.7% graduated from medical school more than 10 yrs. (Table 1). Majority of the residents (95%) were between 25-49 years of age, with 5% that were older than 50 years of age. Post-graduate year one residents constituted 25%, post graduate year two residents 38.3%, post graduate year three residents 31.7% and post graduate year four residents 5% (Table 1).
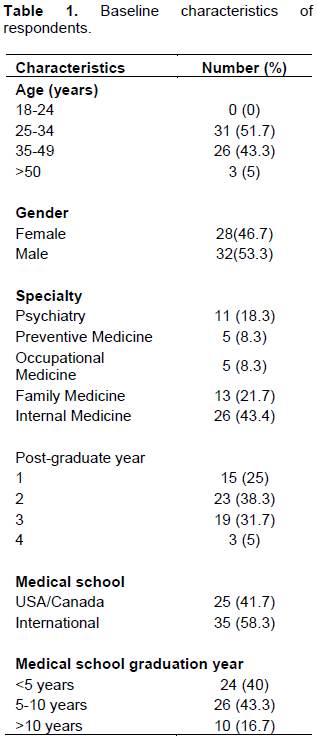
In terms of specialty, internal medicine residents were 43.4%, family medicine residents 21.7%, psychiatry residents 18.3%, occupational and preventive medicine residents were each 8.3%. Only 6.7% of the residents correctly identified all the symptoms of EVD. A total of 58.3% of the residents believed washing hands with water or non-alcohol based hand sanitizer is a good hygiene practice. In terms of transmission, 23.7% of the residents believed that EVD could be transmitted through inhalation. With regards to management of EVD, 55% of the residents recognized isolation as the first step in the management of EVD. On whether personal protective equipment (PPE) was required for individuals driving or riding in a vehicle carrying human remains of EVD deceased patient, only 16.7% answered correctly.
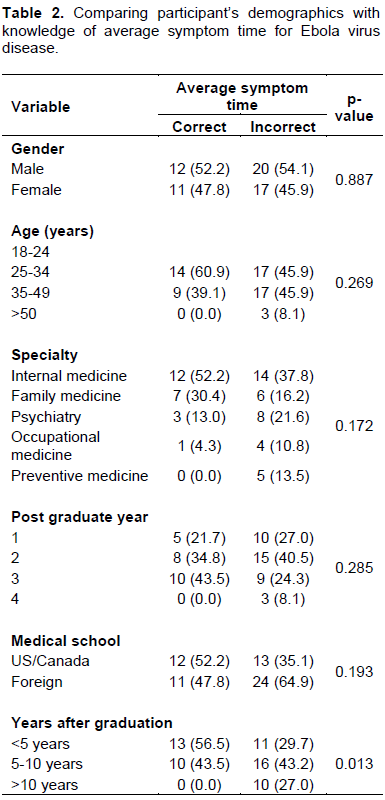
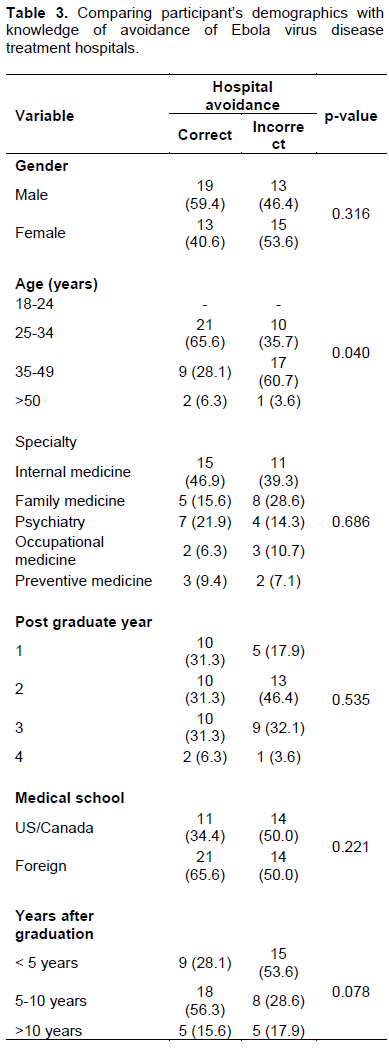
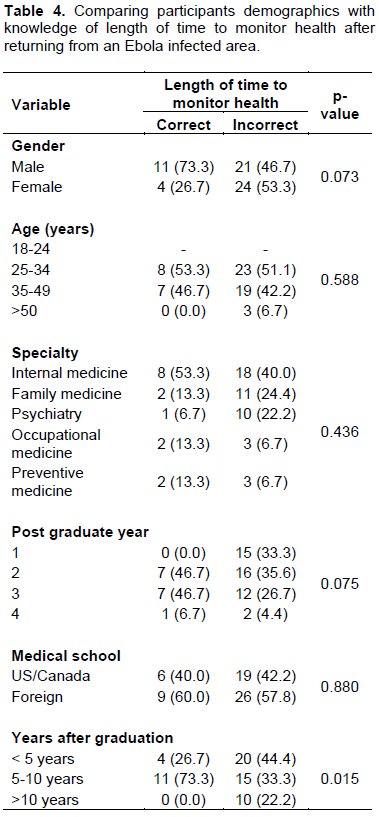
There were some demographic differences that were noted such as when assessing knowledge of average symptoms time of EVD (Table 2), recent graduates did better than older graduates (P=0.013). When assessing resident’s knowledge of the length of time to monitor health after returning from an EVD infected area (Table 3), recent graduates did better than older graduates (P=0.015). When assessing knowledge of avoiding EVD treatment hospitals or centers (Table 4), younger residents did better than older residents (P=0.040).
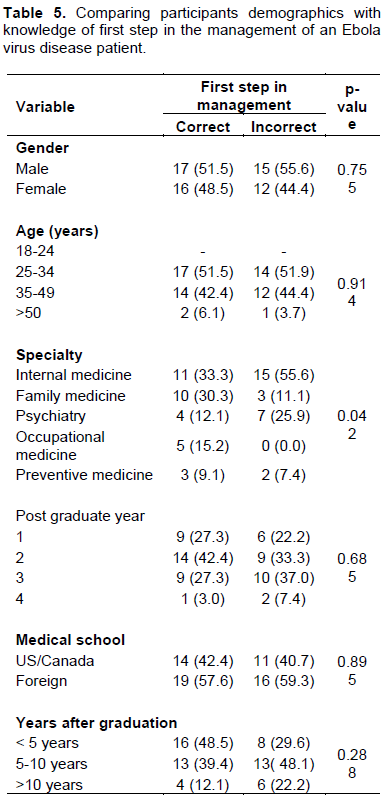
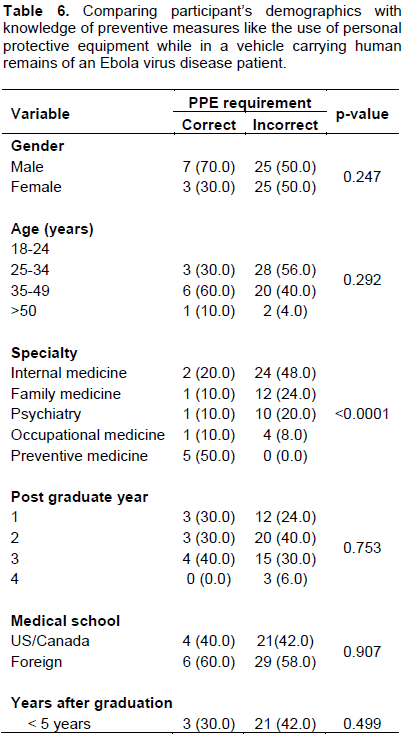
When comparing resident’s knowledge of first step in the management of EVD patients (Table 5), occupational medicine residents did better than the other groups of residents (P=0.042). When comparing knowledge of preventive measures in handling human remains of EVD patients (Table 6), preventive medicine residents did better than the other residents (P<0.0001). Occupational Medicine and Preventive Medicine residents did better on the knowledge of the first step of management of EVD, and on handling of human remains of deceased EVD patients respectively. Younger residents did better on knowledge of avoiding EVD treatment centers. There was no difference in knowledge of EVD with regards to EVD and the type of medical school (International Medical Graduates vs. American Medical Graduates) that the resident attended. There was no significant difference in postgraduate year levels knowledge of EVD
Resident physicians are usually the first to see patients in most teaching institutions, and should protect themselves against infectious agents. Their knowledge of infectious agents and disease process is critical. Knowledge of EVD is not only important to residents, but to the general public as a whole.
Although, the 2014 West African Ebola epidemic was prevalent in the news, only 6.7% of the residents at Meharry Medical College identified all of the early symptoms of EVD. Residents exhibited poor knowledge of good hygiene practices; with 58.3% believing washing hands with water or non-alcohol, based sanitizer is a good hygiene practice.
Knowledge of any disease or condition is important. Slightly more than half (55%) of the residents recognized isolation as the first step in the management of EVD, and only 16.7% answered correctly on whether PPE was required for individuals driving or riding in a car carrying human remains of EVD deceased patient.
The results indicated that recent graduates from medical school did better on knowledge of average symptoms time of EVD and length of time to monitor health after returning from an EVD infected area. A possible explanation in the difference of knowledge between recent and older graduate could be attributed to the time lapse since the recent graduates received formal instructions on EVD versus the older graduates.
According to the authors’ best knowledge, no study has directly addressed the knowledge of EVD among resident physicians in the USA, limiting comparison with an existing study. However, there have been various other studies where authors have attempted to access the knowledge of EVD among healthcare workers. Some of these studies include the work of Abebe et al. (2016) of Gondar University Hospital in Northwest Ethiopia and Narasimhulu et al. (2015) in New York City (2015).
In the first study by Abebe et al. (2016), the authors stratified Healthcare Professionals (HCP) into two groups, physicians and allied health professionals. In that study, they found poor knowledge and negative incorrect beliefs among doctors and allied health professionals (Abebe et al., 2016). The latter study by Narasimhulu et al. (2015) analyzed Healthcare Workers (HCW) attitude towards care of patients with EVD.
In this study, the authors stratified HCWs by attending physicians, resident physicians, nurses and other. The majority of participants in this study (41.2%) were nurses. This study found that there was a linkage between HCWs beliefs about EVD and their willingness to provide care to patients with EVD although this linkage was not a mirror image of their beliefs regarding whether it would be ethical to refuse care for these patients (Narasimhulu et al., 2015). The studies cited previously can add value to the results obtained in this analysis, it demonstrates that at a minimum there is limited knowledge amongst HCWs about EVD and that more training is needed for HCWs.
The data from this study indicates that recent and younger graduates had significantly better knowledge of EVD. Recent graduates are likely to be more current on evolving diseases of epidemic. They are up to date with new treatments and are more likely to apply them. A systematic review evaluating the relationship between clinical experience and quality of health care showed that in terms of current standards of care and of clinical developments, younger physicians were more up to date (Chouldhry et al., 2005).
There was no significant finding between residents who graduated from medical school outside the U.S with those that graduated in the USA/Canada. We found no significant difference between these two groups of graduates. This was an expected finding since the 2014 West African Ebola epidemic was limited to, West Africa and previous outbreaks have been limited to Central Africa. As with the American Medical Graduates it is possible that the majority of the International Medical Graduates had not previously managed an EVD patient.
Occupational medicine and preventive medicine residents did better on the knowledge of the first step of management of EVD, and on handling of human remains of deceased EVD patients respectively. At Meharry Medical College, the occupational medicine and preventive medicine residents attend the same weekly didactic sessions. Residents are taught preventive measures and global health topics that are included in the American Board of Preventive Medicine Certification Exams. Exposure to these topics at didactics in an effort to meet the Core Competencies for the American Board of Preventive Medicine Certification Exams could possibly explain why the residents in occupational medicine and preventive medicine performed significantly better than other specialties in this aspect. It was interesting to note that the occupational medicine and preventive medicine residents at Meharry Medical College did not outperform residents in other specialties on the remaining questions. The core competencies for the American Board of Preventive Medicine is that every Occupational Medicine and Preventive Medicine resident should be proficient in achieving success in the American Board of Preventive Medicine Certification Exams which should have sufficiently equipped these residents with greater knowledge to outperform their fellow residents of other specialties.
EVD is a public health problem. The most recent epidemic has ended but from previous trend will most likely not be the last EVD epidemic in the world. It is prudent therefore for physicians to be knowledgeable about EVD and emerging diseases that have the potential to overwhelm our public health systems.
The sample size of this study was small, which might limit generalizations. In addition, since it was performed at a single institution, generalization is limited. These findings may not actually reflect the knowledge of the residents because of their busy schedule or possible lack of interest. These results should be an impetus for further research in the knowledge of EVD and emerging diseases that are of public health concern. Intervention programs such as lecture series might improve the knowledge base of residents.
Resident physicians have a low level of knowledge regarding the presentation, prevention and management of EVD, including handling post-mortem remains. This study highlights the importance of educational interventions to improve knowledge, attitude and practices of resident physicians in regards to management and prevention of EVD.
The authors have not declared any conflict of interests.
REFERENCES
|
Abebe TB, Bhagavathula AS, Tefera, YG, Ahmad A, Khan MU, Belachew SA, Abegaz TM (2016). Healthcare Professionals' Awareness, Knowledge, Attitudes, Perceptions and Beliefs about Ebola at Gondar University Hospital, Northwest Ethiopia: A Cross-sectional Study. J. Public Health Afr. 7(2):570.
|
|
|
|
Blaize S, Pannetier D, Oester eich L, Rieger T, Koiyogui L, Magassouba N, Soropoqui B, Sow MS, Keita S, De Clerck H, Tiffany A, Dominguez G, Loua M, Traoré A, Kolié M, Malano ER, Heleze E, Bocquin A, Mély S, Raoul H, Caro V, Cadar D, Gabriel M, Pahlmann M, Tappe D, Schmidt-Ghanasit J, Imouma B, Diallo AK, Formenty P, Herp MV, Gunther S (2014). Emergence of Ebola Virus Disease in Guinea. N Engl. J. Med. 371:1418-1425.
|
|
|
|
|
Centers for Disease Control and Prevention (CDC) (2014). Ebola Virus Disease Ebola Outbreak in West Africa. Accessed March 8, 2015. Available at:
View.
|
|
|
|
|
Centers for Disease Control and Prevention (CDC) (2015). Ebola Virus Disease (EVD). About Ebola Virus Disease. Accessed March 8, 2015. Available at:
View.
|
|
|
|
|
Centers for Disease Control and Prevention (CDC) (2015). Ebola Virus Disease (EVD). Transmission. Accessed March 8, 2015. Available at:
View.
|
|
|
|
|
Chouldhry NK, Fletcher RH, Soumerai SB (2005). Systematic Review: The Relationship between Clinical Experience and Quality of Health Care. Ann. Int. Med. 142:260-262.
|
|
|
|
|
Narasimhulu DM, Edwards V, Chazotte C, Bhatt D, Weedon J, Minkoff H (2015). Healthcare Workers' Attitudes toward Patients with Ebola Virus Disease in the United States. Open Forum Infectious Diseases. Accessed September 8, 2017. Available at:
View.
|
|
|
|
|
Sarwar UN, Costner P, Enama ME, Berkowitz N, Hu Z, Hendel CS, Sitar S, Plummer S, Mulangu S, Bailer RT, Koup RA, Mascola JR, Nabel GJ, Sullivan NJ, Graham BS, Ledgerwood JE (2015). Safety and Immunogenicity of DNA Vaccines Encoding Ebolavirus and Marburgvirus Wild-Type Glycoproteins in a Phase I Clinical Trial. J. Infect Dis. 211(4):549-557
Crossref
|
|
|
|
|
World Health Organization (WHO) (2015). Ebola Virus Disease. Accessed March 8, 2015. Available at:
View.
|
|