Full Length Research Paper

ABSTRACT
Heart failure is a complex, clinical syndrome of signs and symptoms that are caused by defects in cardiac structure, function, or both, resulting in impairment of peripheral circulation and organ oxygenation. It is a staggering clinical and public health problem and the study of the epidemiology on heart failure demonstrated that heart failure is associated with significant mortality, morbidity, and health care expenditures. It is a disorder in which the heart pumps blood inadequately which lead to reduced blood flow, congestion of blood in the veins and lungs, and other changes that may further weaken the heart. The aim of this study is to assess the relative contribution of the various causes of heart failure and its prevalence over time which helps policy makers as a tool for decision making in allocating resources and to analysis the association of heart failure with related factors. To a chive this objective of the study a retrospective cohort study based on data from the heart failure patients at Felege Hiwot referral hospital from 2013 to 2017. The analysis revealed that the prevalence of heart failure was decreased over time when we compared patient who had taken treatment with patients who does not take any treatment. Hypertension, diabetes mellitus, anemia, and infection were highly correlated with heart failure and had significant effect on heart failure (p<0.05) and treatments are the basic way to manage heart failure and to recover from this disease. About 71% of patients who died from heart failure were died within four years of diagnosis.
Key words: Assessment, heart failure, management and pharmacologic.
INTRODUCTION
Heart failure (HF) is a complex, clinical syndrome of signs and symptoms that are caused by defects in cardiac structure, function, or both, resulting in impairment of peripheral circulation and organ oxygenation in which more than 6 million people in the United States older than 20 years have heart failure, approximately 800,000 new cases are diagnosed each year (Katz, 2013). Heart failure is a major public health problem associated with high morbidity and mortality among individuals 65 years and older (Sochalski et al., 2009). It is the most common principal discharge diagnosis among medicare beneficiaries and the third highest for hospital reimbursements (Home Health Agency center, 2017). This disease is the leading causes of death in all developing regions of the world with the exception of sub-Saharan Africa, where the first phase of the epidemiologic transition is still dominant, although with a shifting trend towards a double burden of infectious and non-communicable diseases (Boutayeb, 2006). Epidemiological studies and data from clinical trials have shown that the early time period after a hospitalization for HF is a particularly vulnerable interval. Although survival rates for all patients with HF have improved during the past several decades, the greatest gains have been made in the treatment of patients with heart failure with reduced heart failure (Gurwitz et al., 2013).
Evidence from clinical trials supports the use of digoxin to improve symptoms and reduce hospitalization in patients with HF with reduced left ventricular ejection fraction particularly in patients with more advanced symptoms that contributes to digoxin’s as well as neurohumoral and it acts by inhibiting the Na-K-ATPase pump, thus reducing the transport of sodium from the intracellular space in myocytes (Ambrosy et al., 2014). An observational study, including propensity analysis (Cleland, 2013), report that aspirin 75 mg/d, given to 828 outpatients with chronic heart failure, was associated with a 30% reduction in hospitalizations for heart failure and a 42% reduction in mortality compared either with 503 patients not taking aspirin or 64 patients taking higher doses of aspirin.
Based on a research done on the prevalence and etiology of heart failure in patients seen at a teaching hospital in Ghana, the result shows that among the 524 patients involved in the study, 398 of the patients had heart failure according to the modified framingham criteria for the diagnosis of heart failure; giving rise to a prevalence of 76%. Duration of heart failure symptoms is an important factor affecting survival in patients who receive mechanical circulatory support. Patients with heart failure who received mechanical circulatory support have an overall better survival and higher frequency of transplantation and myocardial recovery, despite being sicker at the time of implantation.
In developing countries including Ethiopia, there are many unsettled issues and even controversies among physicians regarding the pharmacologic preferences, indications and contra indications to start a drug and when to hold. In the study done by Belete and Fessahaye (2010) in Jimma University specialized hospital during a five year period, they found that among 781 cardiac cases, Rheumatic heart disease was more common 256 (32.8%) followed by hypertensive heart disease and cardiomyopathy accounting for 189 (24.2%) and 158 (20.2%) of cases, respectively. There were no study done on incidence or prevalence of heart failure in the adult population in Ethiopia. However, there are indicators that heart failure will be a significant burden in the country, and typically affects middle-aged adults. The aim of this study is to assess the relative contribution of the various causes of heart failure and its prevalence over time which help policy makers as a tool for decision making in allocating resources. Additionally it can be used as a baseline data for community based epidemiological studies to see burden of heart failure diseases in the public setting and to identify the significant factors which causes heart failure.
MATERIALS AND METHODS
Study design and eligibility for the study
A retrospective record review was conducted to collect data registered from September, 2013 to August, 2017. The target populations of this study are all heart failure patients who attend Felege Hiwot referral hospital and have been active in follow-up for their Heart failure. During the 4 year period from September 2013 to August 2017, a total of 1681 cardiac patients were admitted, 936 patients to the medical ward and 745 patients to intensive care units (ICU). Among these 384 cases that had follow up and newly diagnose patients who were enrolled to the follow up and had complete card record were taken as study subjects. And hence, 384 patients were considered to collect the data of heart failure which was evaluated at fixed time points. During the data collection time each incomplete chart of the patient was excluded to overcome the problem of data missing, even though there were missing handling mechanisms.
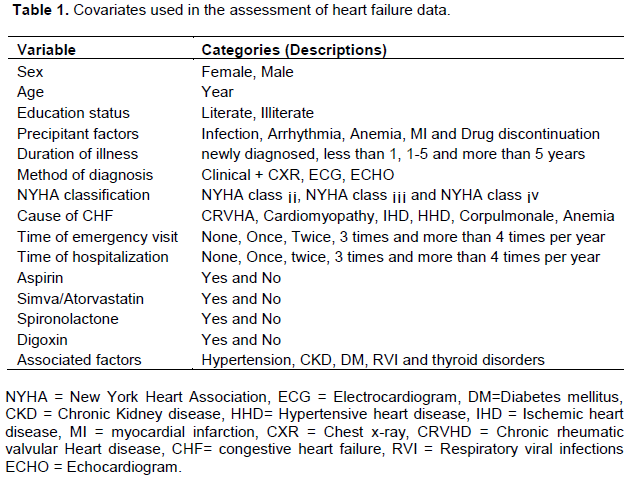
One aim is to ensure horizontal equity in the analyses and comparison on the effect of factor affecting heart failure. The relevant inpatient data were extracted with the study variables on sex, age, precipitating factor, duration of illness, method of diagnosis, associated factors, drug combination, cause of congestive heart failure, frequency of emergency visit, frequency of hospitalization, Spironolactone, digoxin, aspirin, final assessment, New York heart classification and Simva or atrovastatin. Previous studies have reported a proportion among patients with heart failure widely varying from 13 to 74% (Vasan et al., 1995). The different study populations and differences in study design and diagnostic criteria used for heart failure in general are probably responsible for these discordant epidemiological data (McAlister et al., 1999). A recent retrospective community study conducted in patients hospitalized for heart failure over a period of 15 years showed an decrease over time in the average prevalence of heart failure after they starts the treatment as compared with heart failure who had not start their drugs which could be one explanation for the variable proportion of patients with heart failure in various studies. Studies including younger patients show a lower frequency of heart failure (Cohn and Johnson , 1990). Multivariable analysis identified older age, stroke, diabetes, cancer, hyponatraemia, and low glomerular filtration rate as predictors of 5 year mortality in heart failure. In a recent study including hospitalized patients with newonset heart failure, 1 year predictors of mortality in patients with preserved heart failure were age, systolic blood pressure, hyponatraemia, anemia, renal dysfunction, and co-morbidities (Owan et al., 2006). An exploratory analysis was conducted to obtain descriptive statistics of the study variables to obtain percentages and to analyses the relationship between the degree of heart failure and the health failure related factors, a univariate analysis was performed using the chiâ€square test. Continuous variables were expressed as mean ±standard deviation while the categorical variables were summarized by per cents and analyzed with Chi-square test. Associations of heart failure with age, sex and others factors were sought using chi-square. P value ≤ 0.05 was considered statistically significant. In this study several potential explanatory variables were considered in this study (Table 1).
RESULTS AND DISCUSSION
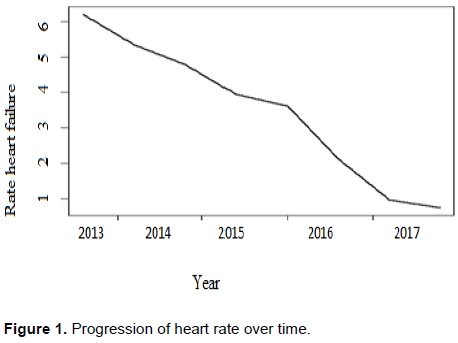
In this study 384 patients were considered to collect the heart failure which was evaluated at fixed time points. Based on graph of Figure 1, this study had shown that after the patient starts their medication, the rate of heart failure was changed over time. The notion is that because heart rates may increase or decrease over time in response to changes in a person's condition or response to a treatment. From the graph we understand that, when the patients start their follow up like taking of treatments (aspirin, digoxin, Spironolactone) the prevalence of heart failure was decreased over time as compared to the patient who does not take any treatment.
Based on the result of Table 2, the demographic characteristics result, states that the mean age was 48.36 years with a standard deviation of ±19. 043 which shows that heart failure was affect the middle age group as well as the older age group and age had a significant effect on heart failure (p = 0.0001). This result also has similarity with the study of Hunt (2005) who conclude that the overall prevalence of heart failure in the adult population in developed countries is 2% and its prevalence increases with age. Among the total study subjects 53.6% (206 cases) were females that indicates females were more exposed for heart failure than males, sex was also one significant factor for the cases of heart failure (p=0.002) which is in line with the study result of Isaac and Yaw (2013) and the study by Scantlebury and Borlaug (2011), which states the etiology of heart failure has been shown to have significant differences by sex.
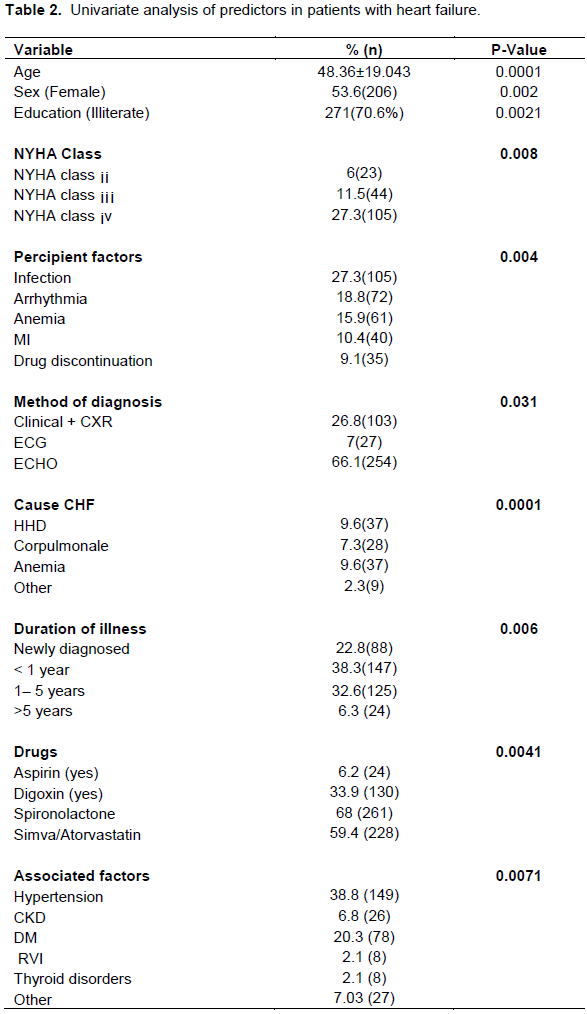
Similarly, on the result of education status most of the patients were, 271(70.6%) were illiterate (p=0.0021). This result is an indicator about the inverse relationship between education and management of heart failure disease for an individual which is similar to the study of Harper et al. (2011) were conclude developed nations, education has been shown to be inversely associated with coronary heart disease. This relation has great importance to many health professionals and policy makers (Commision on Social Determinants of Health, 2008).
Different associated factors had a significant effect on heart failure (p = 0.0071). Among those factors hypertension was a cause in 149 (38.8%) of the patients, 26 (6.8%) patients had chronic kidney disease, 78(20.3%) patients had diabetes mellitus (DM), 8 (2.1%) patients had retroviral infection and another 8 (2.1%) had thyroid disorder as a comorbidity. 27 (7.03%) patients had other associated factors like smoking, family history and obesity while the remaining 88 (22.9%) of patients had no documented associated factor which share similar findings with the study of Owan et al. (2006). From this result, hypertension and diabetes mellitus were contributing the highest percentage for cause of the heart disease. When we consider the variable of NYHA class had its own effect on heart failure (p=0.008). Based on the NYHA class, 317 (82.6%) of patients had NYHA class ¡v, 44 (11.5%) had NYHA class ¡¡¡ and 23 (6%) of the cases had NYHA class ¡¡, this reflects NYHA class ¡v takes the highest portion for the cause of heart failure as compared to the other NYHA class. This result is different from Ahmed et al. (2006), however, because the NYHA classification involves doctors' subjective judgment of symptoms and clinical data, wide interobserver variability has been reported. Once the patients went to medication they had diagnosed in different mechanisms, since method of diagnosis had an effect on the type of treatment they had taken (p =0.031). According to this study result about 254(66.1%) of the study subjects were diagnoses in Echocardiogram (ECHO) method and 103(28.6%), 27(7%) were diagnoses by Clinical + CXR and ECG respectively.
After identifying patients that has heart failure, appropriate drug were given for each patients which were the more significant factor in the management of heart failure (p= 0.0041). Among those patients, 261(68%) used spironolactone, 228 (59.4%) used simva/ atorvastatin and 130(33.9%), 24(6.2%) used digoxin and aspirin respectively. From our observe spironolactone takes the highest percentage for controlling heart failure disease. This is because spironolactone used to treat heart failure by reduces blood pressure, also prevent body from absorbing too much salt which had effect on heart failure. Similarity, simva/atorvastatin helps to control associated factors like DM, hypertension even if aspirin contribute the smallest portion, it is used to lower risk of heart failure in patients with coronary artery disease such as patients with history of heart attack. Drugs reduced heart failure hospitalizations and the combined events of heart failure death or heart failure hospitalization in patients.
In the same case 105 (27.3%) of cases with CHF were precipitated by infection and pneumonia which was the commonest infection accounting for 45 cases (42%) of all infections, arrhythmia was found to be the precipitant in 72 (18.8%) of cases, 61 (15.9%) had anemia as a precipitating factor and 40 (10.4%) had myocardial infarction which was highly related with heart failure and 35(9.1%) of patients had drug discontinuation as a precipitant. And based on duration of illness about 88 (22.9%) of cases were newly diagnosed patient, 147 (38.3%) were diagnosed on follow up for less than 1 year, 125 (32.6%) of cases had follow up between 1- 5 years and 24 (6.3%) were on follow up for > 5 years.
CONCLUSION
Heart failure (HF) is an increasingly common problem and is associated with high morbidity and mortality. The associated factors were the most and common causes for heart failure (p=<0.05). Anemia is concomitant factor and a significant cause of heart failure which shows that risk factors of anemia especially infection like malaria and hookworm infestations are very common in this catchment areas of the study and this is a readily preventable cause by taking preventive measures. Treatments (drugs) are the basic way to manage heart failure and to recover from this disease (p= 0.0041). About 71% of patients who died from heart failure were dead within four years of diagnosis, and all the patients who died from heart failure were New York heart association class IV patients which shows the functional status is an important predictor of outcome.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
ACKNOWLEDGEMENTS
The author is grateful to the Editor of Journal of Public Health and Epidemiology and anonymous Reviewer’s for their helpful comments and suggestions on the earlier version of this article and for Felege Hiwot referral Hospital for allowing to use heart failure data.
REFERENCES
|
Ambrosy AP, Butler J, Ahmed A, Vaduganathan M, Van Veldhuisen DJ, Colucci WS, Gheorghiade M (2014).The use of digoxin in patients with worsening chronic heart failure: reconsidering an old drug to reduce hospital admissions. Journal of the American College of Cardiology 63(18):1823-1832. |
|
|
Amed A, Aronow WS, Fleg JL (2006). Higher New York Heart Association classes and increased mortality and hospitalization in patients with heart failure and preserved left ventricular function. American Heart Journal 151(2):444-450. |
|
|
Boutayeb A (2006).The double burden of communicable and non-communicable diseases in developing countries. Transactions of the Royal society of Tropical Medicine and Hygiene 100(3):191-199. |
|
|
Cleland JG (2013). Is aspirin useful in primary prevention?. European heart Journal 34(44):3412-3418. |
|
|
Cohn JN, Johnson G (1990).Heart failure with normal ejection fraction. The V-HeFT Study. Veterans Administration Cooperative Study Group.Circulation 81:48-53. |
|
|
Commision on Social Determinants of Health (2008). Closing the gap in a generation: health equityhrough action on the social determinants of health. Final Report of the Commission on Socia Determinants of Health. World Health Organization; Geneva. |
|
|
Gurwitz JH, Magid DJ, Smith DH, Goldberg RJ, McManus DD, Allen LA, Saczynski JS, Thorp ML, Hsu G, Sung SH, Go AS (2013). Contemporary prevalence and correlates of incident heart failure with preserved ejection fraction. CrossRefPubMedGoogle. |
|
|
Habte B, Alemseged F, Tesfaye D (2010) The pattern of cardiac diseases at the cardiac clinic of Jimma University specialised hospital, south West Ethiopia. Ethiopian journal of health sciences 20(2). |
|
|
Harper S, Lynch J, Smith GD (2011). Social determinants and the decline of cardiovascular diseases: understanding the links. Annual review of public health 32:39-69. |
|
|
Home health agency center (2017). CMS website. |
|
|
Hunt S (2005). Focused update incorporated into the ACC/AHA 2009 Guidelines for the Diagnosis and Management of Heart Failure in Adults. |
|
|
Isaac KO, Yaw AB (2013). Epartment of Medicine Prevalence and Etiology of Heart Failure in Patients Seen at a Teaching Hospital in Ghana. |
|
|
Katz S (2013). Warlow C, Dennis MS, van Gijn J, Hankey GJ, Sandercock PA, Bamford JM, Wardlaw JM (2002).Stroke: a practical guide to management. Blackwell Science. |
|
|
McAlister FA, Teo KK, Taher M, Montague TJ, Humen D, Cheung L, Kiaii M, Yim R, Armstrong PW (1999).Insights into the contemporary epidemiology and outpatient management of congestive heart failure. American heart Journal 138(1):87-94. |
|
|
Owan TE, Hodge DO, Herges RM, Jacobsen SJ, Roger VL, Redfield MM (2006).Trends in prevalence and outcome of heart failure with preserved ejection fraction.New England Journal of Medicine 355(3):251-259. |
|
|
Scantlebury DC, Borlaug BA (2011).Why are women more likely than men to develop heart failure with preserved ejection fraction?. Current opinion in cardiology 26(6):562-568. |
|
|
Sochalski J, Jaarsma T, Krumholz HM, Laramee A, McMurray JJ, Naylor MD, Rich MW, Riegel B, Stewart S (2009).What works in chronic care management: the case of heart failure. Health Affairs 28(1):179-189. |
|
|
Vasan RS, Benjamin EJ, Levy D (1995). Prevalence, clinical features and prognosis of diastolic heart failure: an epidemiologic perspective. Journal of the American College of Cardiology 26(7):1565-1574. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


