Review

ABSTRACT
Most developments in biotechnology during the last few decades focused on the potential applications of human health, vaccination being the most prominent invention to date. Disease prevention is the most convenient and highly effective approach to promoting human health and prolonging life. Vaccinations have prevented millions of deaths worldwide every year and diseases that used to kill, disable or debilitate millions of people are either gone or seen very rarely. Prevention is the first essential step that needs to be taken before a preventive medicine or vaccine is developed and public health pays a prominent role in this respect. This is, actually, what is happening currently with the Corona Virus (Covid-19) pandemic, although recently vaccines are being administered in different parts of the world. This paper reviews the traditional inoculation methods that were practiced in several societies around the world for the last several hundreds of years, before the advent of the modern vaccination techniques. The paper was compiled using literature review of various publications consultations of the customary laws, and interviews of knowledgeable people on the subject matter. The paper emphasizes how the traditional inoculation practices have laid down the foundation for the advent of the modern vaccination techniques. The principle of isolating infected people leading to the modern practice of quarantine.
Key words: Inoculation, immunization, smallpox, traditional biotechnology, vaccination, vaccine, variolation.
INTRODUCTION
The term ‘Biotechnology’ was first coined by a Hungarian engineer, Karl Ereky in 1919 who defined it as “all lines of work by which products are produced from raw materials with the aid of living things”. Article 2 of the UN or any technological application that uses biological systems, living organisms, or derivatives thereof, to make or modify products or processes for specific use” (CBD, or any technological application that uses biological systems, living organisms, or derivatives thereof, to make or modify products or processes for specific use” (CBD, 2001). Although the term biotechnology is of recent origin, the discipline itself is very old. It is nearly as old as humanity itself and has ever since maintained a close relationship with society. Man began employing microorganisms as early as 5,000 BC for making wine, vinegar, curd, leavening bread, etc. (Singh, 1998). The beginning of agricultural revolution, using artificial selection for crops, livestock, and other domesticated animals as well as fermentation processes involved in converting one source of food into another are all the outcomes of biotechnology. Although the process of fermentation was not fully understood until the work of Louis Pasteur in 1857, it is the first use of biotechnology. All these processes of traditional biotechnology were practiced in Mesopotamia, Egypt, China and India since the Neolithic age (Stone age).
The invention of the world’s first vaccine (smallpox vaccine) by Edward Jenner (1798), and the discovery of the world’s first antibiotic, penicillin, from the mold, Penicillium notatum, by Alexander Fleming (1930) also harnessed the power of biotechnology. Vaccination is the administration of a vaccine (an antigen), in order to stimulate an individual’s immune system so that it can develop adaptive (acquired) immunity to a pathogen. A vaccine, therefore, is a biological preparation that provides active acquired immunity to a particular disease. Vaccines teach our immune system how to create antibodies that protect us from diseases. It's much safer for our immune system to learn this through vaccination than by catching the diseases and treating them. Once our immune system knows how to fight a disease, it can often protect us for many years or even for life, in some cases. Edward Jenner, an English physician and scientist, developed, for the first time, a smallpox vaccine in 1798, the world’s first vaccine ever (Riedel, 2005). As a result, Jenner is often called the father of immunology and his work is said to have saved more lives than the work of any other human (Derrick, 1999; BBC, 2006). When Edward Jenner introduced smallpox vaccine, it was initially called cowpox inoculation or vaccine inoculation. To avoid confusion with other inoculation or vaccination practices, smallpox inoculation continued to be referred to as variolation (from variola = smallpox) and cowpox inoculation was referred to as vaccination, derived from the virus, Variolae vaccinae that causes smallpox of the cow (Latin: vacca means cow).
Currently, the availability of gene cloning has enabled researchers to consider various novel strategies for vaccine development. The advent of genomics, proteomics, and biotechnology as well as the increased understanding of pathogenesis and immune responses to various pathogens has led to the development of safer, means of creating a new generation of vaccines that can overcome the drawbacks of traditional vaccines, which include purification of macromolecules with undesired contaminants and the complexity involved in obtaining sufficient quantities of purified antigenic components. The use of recombinant proteins allows the targeting of immune responses focused against few protective antigens. Since these vaccines use only specific pieces of the germ, they give a very strong immune response that is targeted to key parts of the germ. They can also be used on almost everyone who needs them, including people with weakened immune systems and long-term health problems (Okafor and Okeke, 2018). It is also important to realize that the challenges of vaccine development are not limited to the discovery of safe and effective antigens and delivery systems. The balance between cost, benefits and risk should certainly be evaluated before translating a vaccine candidate to the clinic. Millions of children worldwide die from infectious diseases, despite currently available vaccines. Thus, social, political and economic policies are also important issues and should be addressed appropriately.
The terms vaccination, inoculation and immunization are often used synonymously to refer to artificial induction of immunity against various infectious diseases. Vaccination has been found to be the most effective method of preventing infectious diseases. The immunity that develops in the body as a result of vaccination is actually responsible for the worldwide eradication of smallpox and the elimination of diseases such as polio, measles, diphtheria, tetanus, etc., from much of the world. Vaccination is one of the most cost-effective ways of avoiding disease – it currently prevents 2-3 million deaths a year and a further 1.5 million could be avoided if global coverage of vaccinations improved. Many diseases, which were causing great havoc to the world population, have been reduced by up to 99.9%, since their vaccines were introduced. However, if people stop having vaccines, it's possible for infectious diseases to quickly spread again (USCDCP, 2011). According to Glick et al. (2010), in recent years, a small but vocal minority of individuals, in some developed countries, have refused to have their children vaccinated, because these individuals argue that many of the previously common illnesses have been defeated, and they fear the potential side effects of the vaccinations more than the disease itself.
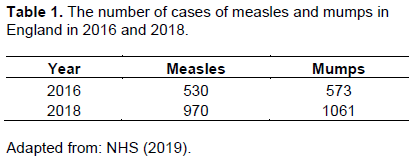
The World Health Organization (WHO) recently listed vaccine hesitancy as one of their top ten biggest threats to global health. Vaccine hesitancy is where people with access to vaccines delay or refuse vaccination. Vaccine hesitancy – the reluctance or refusal to vaccinate despite the availability of vaccines – threatens to reverse progress made in tackling vaccine-preventable diseases. Measles, for example, has seen a 30% increase in cases decades, recombinant DNA technology has provided a more effective, and cheaper vaccines. Within the last 2 globally. The reasons for this rise are complex, and not all of these cases are due to vaccine hesitancy. However, some countries that were close to eliminating the disease have seen resurgence (WHO, 2020). This can best be verified by the fact that measles and mumps are starting to appear again in England, even though the MMR (Measles, Mumps and Rubella) vaccine is safe and protect against both diseases. Recurrence of measles in the USA was reported recently on CNN news. Table 1 shows the resurgence of measles and mumps in England in 2016 and 2018.
Vaccine hesitancy is thus, a serious problem as diseases like measles can lead to life-threatening complications; and meningitis and mumps can cause hearing loss. Although scientists, at the moment, are working relentlessly to come up with a vaccination for the Corona Virus pandemic that is killing hundreds of thousands of people worldwide, CNN polls show that many people in the US are reluctant to take the vaccine even if it is released soon (CNN, 2020). Before the invention of antibiotics and vaccines, people in different parts of the world have been using various traditional practices of inoculation to prevent infectious diseases like smallpox, measles, etc., from spreading and killing people. All such processes, which are based on the natural capabilities of microorganisms, are commonly considered as old or traditional biotechnology. Moreover, customary laws and traditional practices in different parts of the world enlighten us that people contracting infectious diseases within a community were isolated by village leaders to prevent the spread of the disease to the community, a practice nowadays referred to as ‘Quarantine’. The paper shall, therefore, try to review the various traditional inoculation methods that were being practiced to prevent diseases in different parts of the world. It will also underscore how traditional societies have been handling infectious diseases; through the customary laws they have developed, by isolating infected persons and/or villages to prevent the spread of the disease to other villages and communities. Emphasis will be made to the customary laws and traditional practices of handling and treating infectious diseases in Eritrea, which have been confirmed through interviews conducted in the various regions of the country. Finally, it will try to address how such traditional practices have laid down grounds to the invention and development of modern vaccination techniques.
METHODOLOGY
The methodology employed to compile this paper includes:
(i) Review of literature: a general literature review was conducted on the subject matter from various publications including the Internet, and the most relevant information was selected.
(ii) Consultations on the Eritrean Customary Laws: there are 9 customary or traditional laws in Eritrea that were formulated several hundreds of years ago which were later published when the country was colonized by the Italians in 1890. These customary laws, which are comprehensive in their contents, were drafted by elderly people pooled from different villages and endorsed by majority of the people in the region. These laws currently constitute the basic components of the modern legal system in Eritrea.
(iii) Interviews: Elderly and knowledgeable people from the six regions of Eritrea were interviewed between 2017 and 2019, on the customary laws, in general and on the practices of handling infectious diseases in their communities. Ten to twelve representative villages were selected from each region depending on their sizes and 15 people from both sexes were interviewed from each village, constituting between 150 to 180 people in each region. The interviews were then analysed and a preliminary report was compiled (Tadesse, 2019). The review only addresses few regions of the world and by no means is comprehensive.
TRADITIONAL INOCULATION PRACTICES
Before the advent of the modern vaccination practices, traditional societies in different parts of the world have been applying their own methods of preventing infectious diseases before causing serious damage to their societies. The general principles of such traditional inoculation practices when compared with the modern techniques of vaccination are very similar and apply the same scientific justification; although people at that time were not able to explain the practice scientifically. The following sections shall therefore review the various traditional methods of inoculation that were being practiced in different regions of the world, to prevent diseases, before modern vaccination came into practice. Review of such traditional inoculation practices in various parts of the world shall, therefore, hopefully help us to justifiably conclude that they have, in a variety of ways, led and contributed to the invention of the modern techniques of vaccination being practiced nowadays.
Asia: India
According to Chandrakant (2014), inoculation practices have ancient origins and the technique was known in India and China, among others. Several historians have suggested that variolation may have started in India before the 18th century. Historical evidence for this assertion is lacking, except the 1767 account by J. Z. Holwell, which explains that variolation is documented in India from the 18th century (Holowell, 1767). Some details explained by Halowell suggest that sniffing was one of the inoculation methods practiced by the Indians. However, this was later found out to be a Chinese practice.
China
The earliest hints of the practice of inoculation for smallpox in China came during the 10th century. One of the Song Dynasty Chancellors of China lost his eldest son to smallpox and started seeking a means of sparing the rest of his family from the disease. He organized a meeting of physicians, wise men, and magicians from all across the empire to convene at the capital in Keifeng and share ideas on how to cure patients of smallpox. Then a divine man, from among the participants, carried out inoculation that spared the lives of the Chancellor’s family and many other people in the area (Needham, 2000). According to Needham (2000), the first clear and credible reference to smallpox inoculation in China comes from Wan Quan’s report of 1549; however, his report did not give details on the techniques of inoculation. Needham quotes an account from Zhang Yan’s new book on smallpox inoculation written in 1741, which explains the refined method of inoculation. In this new method, scabs are taken from an infected person, wrapped carefully in paper and put in a small bottle container. The bottle is corked tightly to prevent dissipation, labelled with the date the scabs were collected from the patient and stored in a cool, dark place. Then, after about 30 to 40 days, the powder is inoculated to the subjects by blowing into the nostrils of the subjects. Two such reports on the Chinese inoculation practice were received by the Royal Society in London in 1700, but no action was taken (Silverstein, 2009).
Circassia (North Caucasus)
According to Voltaire (1742), the Turks imparted their inoculation practices to their neighbour Circassia. The Circassian women have, from time immemorial, communicated the smallpox to their children when they are below six months old by making an incision in the arm and by putting into this incision pustules, taken carefully from the body of another child. This pustule produces the same effect in the arm it is put as yeast in a piece of dough; it ferments and diffuses through the whole mass of blood, developing immunity to the disease. This practice of immunization in Circassia is believed to have been derived from the Turks during early 18th century (Timoni, 1714).
America (USA)
According to Gross et al. (1998), in 1706, a Sudanese slave named Onesimus explained the procedures of inoculation to his master, a Boston Minister, Cotton Mather. Onesimus told his master that he had learned the knowledge of inoculation from Africa, particularly from West Africa. However, although Mather heard about the practice of inoculation from his Sudanese slave and later from Timoni’s report to the Royal Society, he was unable to convince local physicians to carry out the procedure (Kenneth, 1984). The practice of inoculation is documented in America as early as 1721, when Zabdiel Boylston, at the request of Cotton Mather, successfully inoculated two slaves and his own son. After this initial success, Boylston began performing inoculations throughout Boston, although there was a lot of controversy among the people and at least one attempt upon his life. However people started to be convinced slowly when the effectiveness of Boylston’s inoculation was proven to be successful. During the outbreak of smallpox, the mortality rate of people who contracted the disease naturally was one in six (about 17%), whereas out of the three hundred people inoculated by Boylston only six (2%) died (Dickson, 1896). Boylston travelled to London in 1724, where he published his results and he was elected to the Royal Society in 1726.
Europe: England
John Woodward received a letter from Emmanuel Timonius from Constantinople (the current Turkey), the contents of which were published in the Philosophical Transactions of the Royal Society of London in 1714 (Timoni, 1714). The letter emphasized that inoculation was a proven method of controlling the gravity of the smallpox disease. The practice of inoculation was first introduced to England by Lady Mary Wortley Montagu.
The husband of Lady Montagu, Edward Wortley Montagu, was serving as the British Ambassador to the then Ottoman Empire from 1716 to 1718. During her stay in the Ottoman Empire with her husband, Lady Montagu was able to witness, first-hand, the practices of inoculation by the Turks, in Istanbul, and she was greatly impressed by the practice (Hopkins, 1983; The Independent, 2008). Earlier, Lady Montagu actually lost a brother to smallpox and bore facial scars herself from the disease. In 1718, Lady Montagu had already started writing about inoculation to various influential persons in England and sent essays to several magazines.
England was ruthlessly threatened by smallpox epidemic in 1721 and Lady Montagu was back in England with her husband by then. Lady Montague had already inoculated one of her children in Turkey, before she returned back to England, despite opposition from religious leaders and medical personnel. However, because she had a prior knowledge about inoculation from Istanbul, Lady Montague called on her physician, Charles Maitland, to inoculate her daughter. To witness the inoculation process, she invited her friends, including Sir Hans Sloane, who was the physician of King George I of Great Britain, who reigned in the kingdom from 1714 to 1727. This occasion rose great interest among people and government of the kingdom and as a result Maitland was given permission to inoculate prisoners at Newgate Prison. Six prisoners who were sentenced to be hanged were selected for this purpose in exchange for their freedom (David, 2006). Maitland performed the inoculation to the prisoners, and the practice was witnessed by many notable doctors. After receiving the inoculation, all the prisoners survived and were released from prison. Following this successful practice, the daughters of the Prince of Wales received inoculations a year later in 1722 (Paul, 2005). After this historical event, the practice of inoculation slowly spread amongst the royal families of Europe and people started embracing the practice stage by stage.
France
Although the practice of inoculation started to gain popularity in England and some other parts of Europe, its introduction to France faced considerable opposition and was later banned by ruling of the parliament. Voltaire, a renowned French writer, historian and philosopher of the time, adamantly opposed the banning of inoculation in France. In his ‘Lettres Philosophiques’ he wrote criticism of his countrymen for being opposed to inoculation and having so little regard for the welfare of their children. He, in fact, concluded his letter by stating that “… had inoculation been practiced in France, it would have saved the lives of thousands” (Voltaire, 1742). In general, however, the popularity of inoculation grew in Europe through the 18th century and many parents were convinced that the benefits of inoculation outweighed the risks and thus started inoculating their children (Cohn, 2004).
Africa
The knowledge of inoculation against smallpox was known to West Africans, particularly the Akan ethnic groups which belong to Ghana, Benin and Ivory Coast. A Sudanese slave, Onesimus, had explained the inoculation procedure to his master, Cotton Mather, during the 18th century, and explained to him that he got the knowledge from Africa, particularly from west Africa (Waldstreicher, 2004).
Eritrea
The knowledge of inoculating people against smallpox seems to have been known to Africans during early 18th century. Although documented accounts are not available regarding traditional vaccinations or inoculations in Eritrea, it has been confirmed that some sort of inoculations were being practiced to prevent common diseases like measles and smallpox, since time im-memorial. This fact has been established through various interviews conducted with elderly and knowledgeable men and women in the various regions of Eritrea. The interviews were conducted in selected villages around all six regions of the country between 2017 and 2019, and a report compiled (Tadesse, 2019). Preliminary findings of the survey, especially the procedures of quarantining people contracting infectious diseases, were published in the local newspaper in Tigrigna, one of the local Eritrean languages (Hadas, 2019). Moreover, some of the customary laws and regulations that were being applied to govern communities, which were later on published in the form of books, mention about the practice of isolating infected people in a village/community to prevent the spread of contagious diseases.
Through the interviews conducted, it was established that many villages were practicing their own methods of preventing the spread of contagious diseases, before the advent of modern vaccination practices. Whenever it is confirmed that a person, a family or several people within a village or a community have contracted a communicable disease, the village chief (‘Chiqa Adi’) orders isolation of the infected person(s) in a separate part of the village and assigns a female to provide them with food, water and other necessities without having direct contact with them. The practice of isolating infected people is known as ‘wusheba’ in Tigrigna (one of the Eritrean languages), which is equivalent to the modern ‘quarantining’ practice.
In the case of measles, a different treatment was practiced. After confirming that some children in a particular community or a village have contracted measles, the village chief (‘Chiqa Adi’) orders the family of such children to strictly keep them isolated in their respective residences and prevent them from contacting other children in the village until their pustules are fully mature and start to burst. When the pustules are fully mature, all the people in the community, including children, gather and the bodies of the infected children with mature and bursting pustules are washed with water and the body-wash is collected in containers. Then, all the children above a specific age within the community gather and they are made to take a sip each, using a small cup, of the body wash from the children who have developed full blown measles. Within few days, the children who drank a limited amount of the body washes contract the disease in a mild form and start to slowly develop resistance/immunity to the disease.
Although these elderly people in the community cannot scientifically explain the practice they were undertaking, they know, through experience, that after such an exercise all children within the community will develop immunity to the disease and will never contract measles again. The principle here is that, when the bodies of the children with mature and bursting pustules are washed with water, the viruses causing measles are being washed from the pustules and abundantly diluted. Thus, when the rest of the children in the community are made to take a sip from such body washes, the viruses causing measles are introduced into their blood stream in a weak form (because they are abundantly diluted) and trigger their immune system to develop antibodies that start to fight and destroy the antigens. The antibodies formed against measles remain within the bodies of the children throughout and they become resistant to the disease for life.
Customary Laws and ‘Wusheba’ (Quarantine)
Before the advent of modern laws in Eritrea, several communities had developed their own customary laws and regulations to govern their people. Such laws were drafted by a group of selected elderly and knowledgeable people in the community and finally approved by all the people living in the community. Such customary laws were hand written and kept in churches and monasteries and through time they were either destroyed during the various wars fought or misplaced for various reasons. However, people in these communities took initiatives to revive and revitalize their customary laws and about nine such laws have now been published in Eritrea in the form of books and are made accessible for people to read them. These customary laws, by the way, have served as the basis of or foundation for the laws in the modern legal system of Eritrea.
One of the nine customary laws in Eritrea, the Law of Logo Chiwa (Ser’At Logo Chiwa), which was formulated in 1484 and revised 4 times thereafter (in 1650, in 1892, in 1935 and in 1938) mentions about how people contracting infectious diseases within a village/community should be treated. Article 55 of the law, although it does not explicitly state the inoculation methods that were being practiced at that time, it clearly explains the important steps that need to be taken by the community leaders (Chiqa Adi and Mslene) whenever a contagious disease spreads within a village/community (The Law of Logo Chiwa, 1938). People affected by any contagious disease, such as smallpox, syphilis, etc., are isolated by order of the village/community chief in order to prevent the spread of the disease. A woman from the village is assigned to prepare and supply food, water and all other necessities for the isolated people, and the necessary supplies, like fire wood, water, etc., are provided by few young people assigned by the village chief until the situation of the disease is improved. If the situation worsens, the village is completely prevented from making any sort of contact with the neighbouring villages and nobody is allowed to come in or go out of the village. The infected people will then receive inoculation by people knowledgeable about the practice and will be released if their conditions improve. If the situation of such infected people does not improve and if people start to die, then their bodies are burned wherever they are.
The Tygrigna equivalent for quarantine, ‘wusheba’, is a word coined to denote the practice of isolating an infected person or a group of persons to prevent the spread of a contagious disease within a community. The traditional practice of ‘wusheba’ is equivalent to the modern quarantine practices, which are now forming the basic tenet of the World Health Organization (WHO) whenever an epidemic or a pandemic disease, like the current Corona Virus (Covid-19) pandemic, infects a locality or the whole world. The WHO was officially established in 1948 (Michael, 2002) but the traditional quarantine practices, like wusheba, were being practiced before the establishment of the world body.
Ethiopia
The first European to report the practice of traditional inoculation or variolation by the Amhara and Tigray peoples in Ethiopia was Nathaniel Pearce.In 1831,Pearce travelled to Ethiopia and noted that inoculation practices were performed by a ‘debtera’ (a learned person in a church or monastery) in the traditional communities of Amhara and Tigray. The ‘debtera’ collects “a quantity of matter” from a person who has contracted smallpox and who has developed the most sores/pustules from the disease. He then “cuts a small cross with a razor in the arm” of his subject and put “a little of the matter” into the cut, which was afterwards bound up with a bandage. The cross, in this particular case, has a religious connotation, because majority of the people inhabiting the highlands of the Amhara and Tigray regions of Ethiopia are Christians. Later, the French Scientific Mission of 1839-1841 to Ethiopia, which included W.C. Harris and Dr. Petit, also described the inoculation practices that were being exercised in Ethiopia (Punkhurst, 1999).
CONCLUSION
Traditional inoculation, which started to be practiced in China as of the 10th century, expanded throughout the world, employing different methods, until modern vaccination techniques were discovered by Edward Jenner, in 1798. Traditional inoculation was thus being practiced in different parts of the world for over 80 years to prevent death and debilitations that may have been caused by various diseases. It is, therefore, obvious that the various methods of inoculation practiced in different regions of the world have immensely contributed to and laid down the foundation for the development of modern techniques of vaccination towards the end of the 18th century and beyond. The basic principles of the traditional inoculation methods and the modern vaccination practices are basically the same. They both introduce the disease-causing microorganisms to their subjects in a weakened form so that the individuals receiving these microorganisms would be able to develop immunity against the particular disease. The traditional inoculation practices do this by either adequately diluting the microorganisms in the case of washing the full-blown pustules or by inoculating their subjects with weakened forms of pathogens. Moreover, the traditional practice of isolating infected persons (wusheba) and the modern quarantine practices are basically similar and employ the same scientific knowledge, although the traditional people at that time were not able to scientifically explain them as they are being done now. From the above discussions, therefore, it would be imperative to conclude that modern vaccination techniques have their roots in and lent the principles of the inoculation methods that were being practiced by traditional societies around the world. Moreover, isolation of infected persons in a society was a common practice in traditional societies before the WHO declared quarantining of infected persons.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
BBC (2006). British Broadcasting Corporation: History - Edward Jenner (1749-1823). Retrieved June 2019. |
|
|
Convention on Biological Diversity (CBD) (2001). Hand Book of the Convention on Biological Diversity. Secretariat of the Convention on Biological Diversity. Earth Scan Publications Ltd., London. |
|
|
Chandrakant L (2014). A brief history of vaccines and vaccination in India. Indian Journal of Medical Research. |
|
|
CNN (2020). Cable News Network (CNN): News Session (July 2020). |
|
|
David W (2006). Bad Medicine: Doctors Doing Harm Since Hippocrates. Oxford University Press, England P 153. |
|
|
Cohn DV (2004). "Lady Montagu". Founders of Science. |
|
|
Derrick B (1999). Edward Jenner's Inquiry; a bicentenary analysis. Vaccine 17(4):301-307. |
|
|
Dickson WA (1896). A History of the Warfare of Science with Theology in Christendom. 2. New York: D. Appleton and Company P 57. e, accessed July, 2020. |
|
|
Glick BR, Pasternak JJ, Patten CL (2010). Molecular Biotechnology: Principles and Applications of Recombinant DNA. 4th Ed., ASM Press, Washington DC, USA. |
|
|
Gross C, Sepkowitz P, Kent A (1998). The Myth of the Medical Breakthrough: Smallpox, Vaccination, and Jenner Reconsidered". International Journal of Infectious Diseases 3(1):54-60. |
|
|
Hadas E (2019). Local Newspaper in Eritrea (Tigrigna), 28th year No. 181, 2019. |
|
|
Holowell JZ (1767). An Account of the Manner of Inoculating for the Smallpox in East Indies with Observations on the Mode of Treating that Disease in those parts. London: T. Becket & P.A. de Hondt. |
|
|
Hopkins DR (1983). Princess and Peasants: Smallpox in History, University of Chicago Press. |
|
|
Jenner E (1798). An Inquiry into Causes and Effects of Variolae Vaccinae, a Disease. Discovered in some of the Western Counties of England, particularly Gloucestershire, and Know by the Name of Cow Pox, printed for the author by Sampson Low, London. |
|
|
Kenneth S (1984). The Life and Times of Cotton Mather. Harper & Row, New York P 339. |
|
|
Michael M (2002). A brief history of the World Health Organization. The Lancet 360:1111-1112. |
|
|
Needham J (2000). Science and Civilization in China. Volume 6, Biology and Biological Technology, Part 6, Medicine. Cambridge University Press P 154. |
|
|
NHS (2019). Why Vaccines are Important. NHS Website, 2019. Accessed August 2020. |
|
|
Okafor N, Okeke BC (2018). Modern Industrial Microbiology and Biotechnology, 2nd Edition. CRC Press. |
|
|
Paul S (2005). A Brief History of Medicine. London: Robinson P 179. |
|
|
Punkhurst R (1999). An Introduction to the Medical History of Ethiopia. Trenton: Red Sea Press. |
|
|
Riedel S (2005). Edward Jenner and the history of smallpox and vaccination. Proceedings: Baylor University Medical Center 18(1):21-25. |
|
|
Silverstein AM (2009).A History of Immunology (2nd ed.). Academic Press P 293. |
|
|
Singh BD (1998). Biotechnology, BSc Edition. Kalyani Publishers, New Delhi, India. |
|
|
Tadesse M (2019). Report on the preliminary findings of the survey/interview conducted in the six regions of Eritrea between 2017 and 2019. |
|
|
The Independent (2008). How Islamic inventors changed the world. The Independent, London, 11 March 2008. |
|
|
The Law of Logo Chiwa (1938). Ser'At Logo Chiwa - The Law of Logo Chiwa, reprinted for the 4th time, Petros Sila Printing Press, Asmara. |
|
|
Timoni E (1714).An account of procuring Smallpox by incision or inoculation, as it is practiced in Constantinople. Philosophical Transactions of the Royal Society 29(338-350):72-82. |
|
|
United States Centers for Disease Control and Prevention (USCDCP) (2011). A CDC framework for preventing infectious diseases, accessed September 2019. |
|
|
Voltaire (1742). Lettres Philosophiques, English translation on-line. |
|
|
Waldstreicher D (2004). Runaway America: Benjamin Franklin, Slavery and the American Revolution. Hill and Wang 315 p. |
|
|
World Health Organization (WHO) (2020). Ten Threats to Global Health in 2019. WHO Websit. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


