Full Length Research Paper

ABSTRACT
This study examined and identified the determinants of modern contraceptive use among fertile women in Debark district. In order to meet the objective descriptive, multiple logistic regression and multilevel logistic regression statistical techniques were used for data analysis. The results of multiple logistic regressions showed that health center, place of residence, marital status, access to media, environmental condition, frequency of modern contraceptive use, type of modern contraceptive and HIV test are significant determinant factors of modern contraceptive use in Debark districts. The results of multilevel logistic regression analysis showed that the random intercept and the fixed coefficient model provided the best fit for the data under consideration. The variance of the random component related to the intercept term was found to be statistically significant, implying differences in the distribution of modern contraceptive use in the health center. It also found that place of residence, marital status, environmental conditions, access of media, frequency of modern contraceptive use, type of modern contraceptive and HIV test were significant determinant factors of distribution of modern contraceptive among health center.
Key words: Determinants, modern contraceptive use, debark.
Abbreviation: AIC/BIC, Akaike/Bayesian information criterion; ACSA, Central Statistical Agency; E/DHS, Ethiopian/ Demographic and Health Survey; FGAE, Family Guidance Association of Ethiopia; FHD, Family Health Department, HIV/AIDS, human immune virus/acquired immune deficiency syndrome; ICC, intra class correlation coefficient; MDGs, millennium development goals; NGO, non-governmental organizations; SPSS, Statistical Package for Social Science; SSA, Sub-Saharan Africa; UNICEF, United Nation Children’s Fund; USAID, United States Agency for International Development; WHR, World Health Report; LAPMCs, long acting and permanent method contraceptive; DHS, Demographic Health Survey Agency; UNFPA, United Nations Family Planning Agency; DEPO, Depo-Provera; POP, progesterone only pill; COC, combined oral contraceptive.INTRODUCTION
In Eastern and Southern Africa, injections and implants are the most popular methods, accounting for over 40% of contraceptive (Giusti and Vignoli, 2016). Traditional methods, generally not recommended as contraceptives because of their lower effectiveness in preventing pregnancy, are still commonly used in Middle Africa, West Africa, Western Asia and Eastern Europe, where 65, 37, 35 and 32%, respectively, of women of reproductive age who are married or in union and are currently using a method of contraceptive rely on a traditional method (Oyedokun, 2004). In Azerbaijan, for instance, 64% of contraceptive users rely on withdrawal (Short and Kiros, 2002). The relatively high birth rate in Nigeria, which has been accompanied by steady declines in death rates has resulted in high rates of population growth. Within the last four decades, there have been increasing pressures towards family limitations in Nigeria. These are results of rapid growth of the large towns, very great extension of educational facilities, and among the elite, the far greater difficulty of securing top jobs that have come with independence (Ebigbola and Ogunjuyigbe, 1998). Unfortunately, this is almost impossible to achieve since all the available evidence indicates that the rate of growth of the economy has been lower than the rate of growth of the population. Standards of living tend to worsen when the rate of population growth exceeds the rate of economic growth (Feyisetan and Bamiwuye, 1998).
The continuing growth of the world population has become an urgent global problem. Ethiopia, like most countries in sub-Saharan Africa, is experiencing rapid population growth. Currently, the country’s population is growing at a rate of 3%, one of the highest rates in the world and if it continues unabated, the population will have doubled in 23 years, preventing any gain in the national development effort (Beekle and McCabe, 2006; Tizta et al., 2014).
Sexually active young women worldwide are at high risk of pregnancy, largely because they use ineffective methods or use contraceptive intermittently. Often those who use effective hormonal methods, the pill and the injectable as well as condoms, have high discontinuation rates (Pachauri and Santhya, 2003).
However, the implant, another hormonal method, which became available in the 1990s, has helped young women to use effective method successfully, contributing to recent declines in teenage pregnancy in the United States (Harper, 2004).
The use of modern contraceptive methods prevents unintended pregnancy, which is associated with many negative health consequences (White and Speizer, 2007). Everyday, more than 400,000 contraceptives hadtaken around the world, of which about half are deliberate, while the other half is unintentional (Preston and Sapienza, 1990). This high level of unwanted fertility leads to high fertility and population growth rate that remain a significant impediment to development. In many developing countries, increase in population size coupled with low technological development contributed to deforestation, soil degradation and species loss. In other words, to support more people more food should be produced. To produce more food, more resources are required in food production, which causes depletion of natural resources (Preston and Sapienza, 1990).
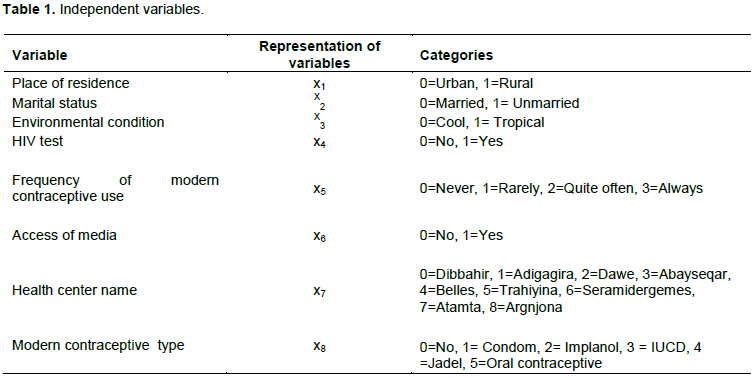
The general objective of this study was to identify determinants of modern contraceptive use among fertile women in Debark districts. While the specific objectives are (1) to identify socioeconomic, demographic and other proximate determinants of modern contraceptive use methods among fertile women in Debark districts and (2) to examine the extent of variation in contraceptive use within and between the health center and an environmental condition of Debark districts as shown in Table 1.
MATERIALS AND METHODS
Source of data
The data for this study was taken from the 2015 Debark district health office (secondary data) collected in North Gondar zone health office. The data were analyzed using SPSS and Stata.
Dependent variable
The response variable of this study is status of modern contraceptive use of fertile women in Debark districts in the health center. The response variable for the ith individual is represented by ![]() and it measures a type of modern contraceptive use and it is dichotomized with 0 women being short act modern contraceptive use (Pill or Oral contraceptive, Condom and injection) and 1 woman being long act modern contraceptive used (Implanol, IUCD, Jadel, etc.).
and it measures a type of modern contraceptive use and it is dichotomized with 0 women being short act modern contraceptive use (Pill or Oral contraceptive, Condom and injection) and 1 woman being long act modern contraceptive used (Implanol, IUCD, Jadel, etc.).
Independent variables
In this study, possible determinants of modern contraceptive use were grouped as demographic, socioeconomic, environmental and other related factors.
Experimental
In clinical situations, the status of a patient is assessed by the presence or absence of a disease. There are many factors to consider which may or may not correlate with the incidence of the disease. There has been numerous retrospective medical research studies published each year that review past medical records and charts of former patients to help determine some of the risk factors (or causing agents) of diseases that are of interest. Finding the determinants and the potential factors can help to know and prevent the attitudes of contraceptive users. All the diseases and nearly all of the risk factors considered are categorical variables (variables taking on two or more possible values) (Hosmer and Lemeshow, 1989).
Logistic regression is a statistical technique for predicting the probability of an event, given a set of predictor variables. The procedure is more sophisticated than the linear regression procedure. The binary logistic regression procedure empowers one to select the predictive model for dichotomous dependent variables. It describes the relationship between a dichotomous response variable and a set of explanatory variables. The explanatory variables may be continuous or discrete. The logistic model, as a non-linear regression model, is a special case of generalized linear model where the assumptions of normality and constant variance of residuals are not satisfied (Mccullagh and Nelder, 1989).
Generally, when the dependent variable is dichotomous (such as presence or absence, success or failure, etc.), binary logistic regression is used. The logistic regression is also preferred to multiple regression and discriminant analysis as it results in a meaningful interpretation, it is mathematically flexible and its distribution is easy to use and it requires fewer assumptions (Hosmer and Lemeshow, 1989).
The best approach to the analysis of multilevel data is an approach that represents within-group as well as between group relation within a single level analysis, where ‘group’ refers to the units at the higher levels of the nesting hierarchy (Snijders and Bosker, 1999).
RESULTS
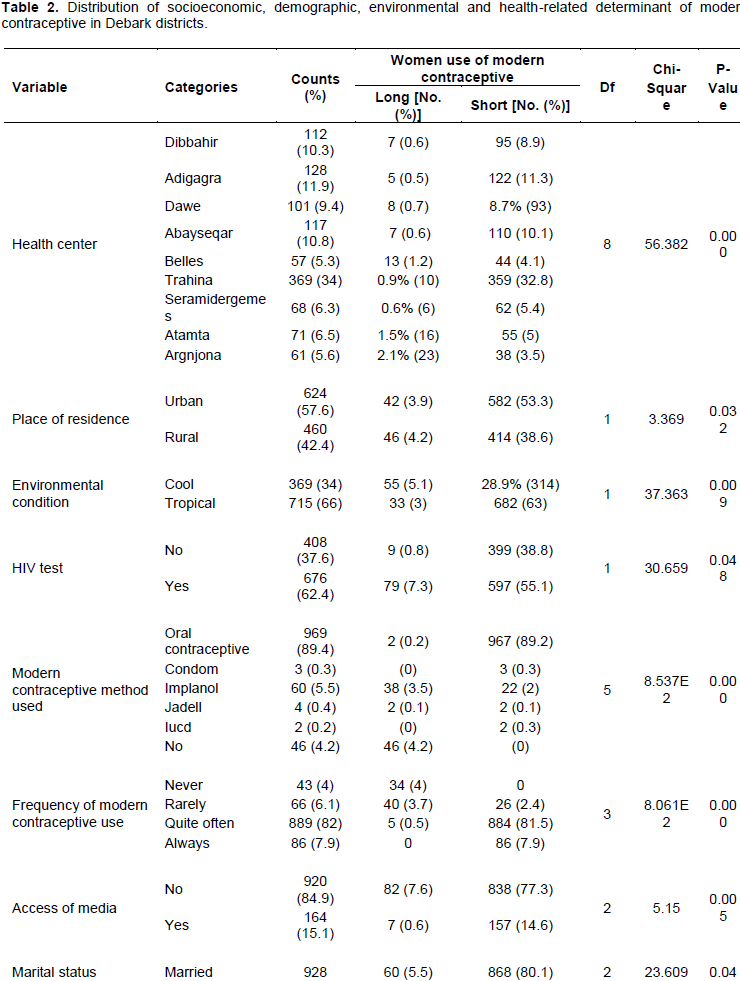
A total of 1084 fertile women were included in the study from Debark districts. The initial population consists of 26714 women who were modern contraceptive users on their background characteristics as well as reproductive health issues. Out of which 1084 women have complete measurements and were considered in this study and others were excluded due to the major socioeconomic and demographic background characteristics of the respondents are incomplete of data on the variables which are considered in the analysis shown in Table 2. Among 1084 fertile women, 57.6% reside in the urban area and 42.4% are residing in the rural area. Higher short-term modern contraceptive use occurred in a woman who resides in an urban area (53.3%) as compared to women who reside in rural areas (38.6%).
Table 2 also shows that, among the total respondents, 66% of them had lived in tropical environmental conditions and higher short-term modern contraceptive use was observed (63%), while 55.1% of women were short-term modern contraceptive users. The proportion of frequency of modern contraceptive use is also considerably higher for women (7.9%) in the short term as compared to those who are always in the long term. Furthermore, the proportion of women who have got the access to media about modern contraceptive use varied by media access. The majority of respondents, 84.9% of them had no media access well.
The majority of respondents (85.6%) were married. While only 80.1% married were short-term modern contraceptive user and 5.5% of the married women were long-term modern contraceptive users.
Likelihood-Ratio test
Under model summary in Table 3, it was observed that -2Log likelihood statistics were 49.133a. This statistic showed us how much improvement is needed before predictors provide the best possible prediction of the response variable, the smaller the statistics the better the model. The statistics for only intercept model is



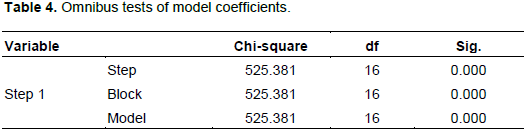
Another method of assessing the overall fit of the logistic regression model is an Omnibus test of model coefficients. Based on the results in Table 4, the null hypothesis shows that there is no difference between the model with only a constant and the model with independent variables was rejected.
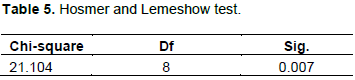
Hosmer and Lemeshow test
Since Table 5 shows the p-value as 0.007 which is less than 0.05, then we reject the null hypothesis that there is no difference between observed and model predicted values, implying that the model fitted the data well.
Two additional descriptive measures of goodness of fit presented in Table 3 are R2 indices defined by Cox and Snell (1989) and Nagelkerke (1991). These indices are variations of the R2 concept defined in the ordinary least square regression model. The Nagelkerke R2 was 93.9% indicating that the explanatory variables were useful in predicting the presence or absence of modern contraceptive in Debark district.
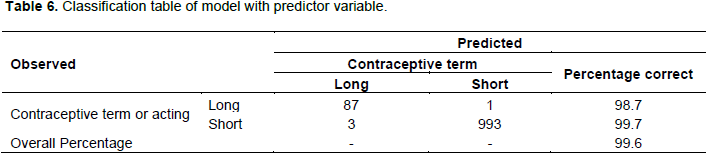
Classification table
The classification of Table 6 showed that 98.7% of the women in long-term modern contraceptive were correctly classified, whereas 99.7% of the women in short-term modern contraceptive user were correctly classified. The overall correct prediction was 99.6%, which is an improvement over the chance level.
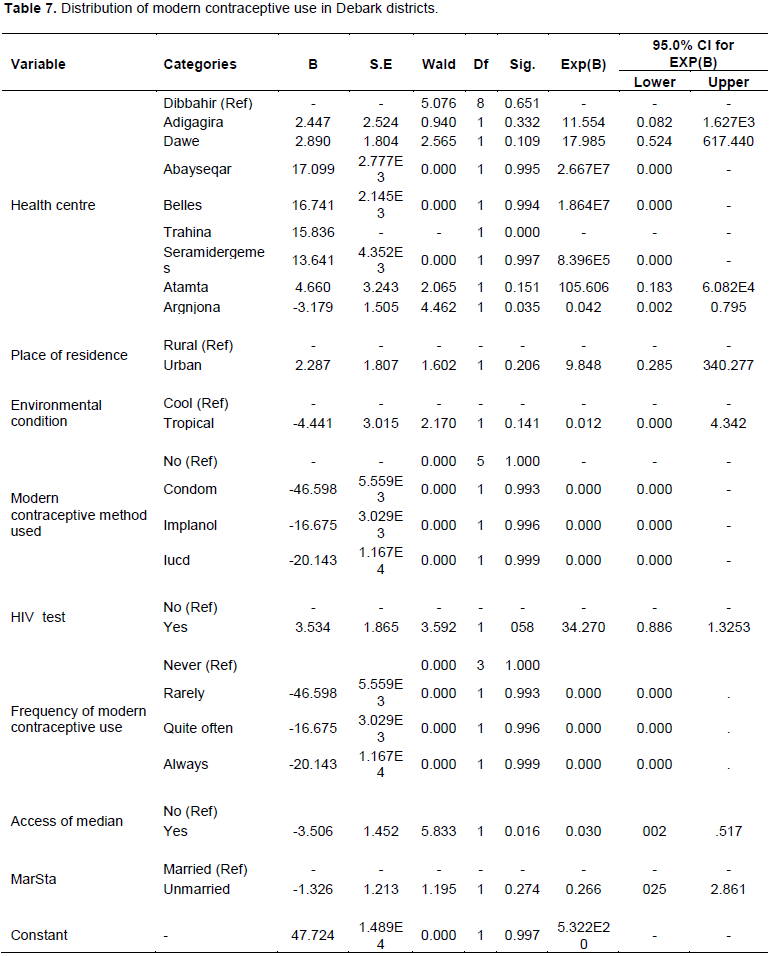
Multiple logistic regression analysis
Health center, place of residence, marital status, environmental condition, HIV test, the frequency of modern contraceptive use, access of media and the type of modern contraceptive use found to be significant predictors for the determinant of modern contraceptive use at 5% level of significance. Thus, the estimated model is given by:
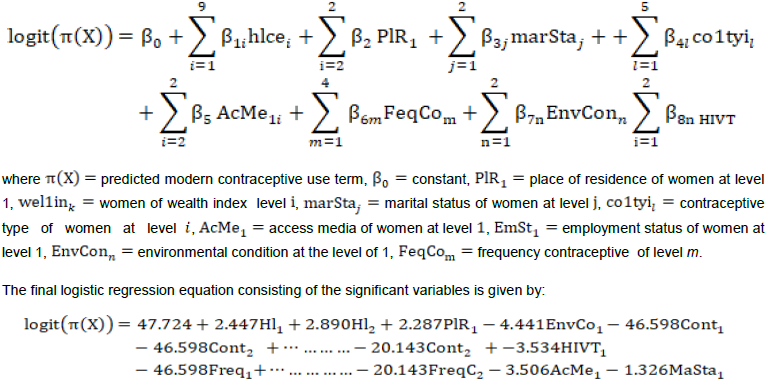
The logistic model showed that the likelihood of having determinant of modern contraceptive was significantly associated with the geographical health center. Women who live in the Atamta Health Center were 105.606 times more likely to have modern contraceptive use than Dibbahir Health Center controlling other variables in the model (OR=105.606; 95% CI: 0.183-6.082E4). Similarly, women who lived in the Dawe Health Center were 17.985 times more likely to have modern contraceptive use than Dibbahir Health Center controlling other variables in the model (OR=17.985; 95% CI: 0.524 - 617.440). Moreover, women who live in Trahina and Argnjona were more likely to have modern contraceptive use than Dibbahir Health Center. Unlike the odds of having modern contraceptive use among women who live in Adigagra, Abayseqar, Seramedergemes and Bellese, they are not significantly different from those of women who live in the Dibbahir Health Center.
Place of residence has a significant association with the determinant of modern contraceptive use. Women who reside in a rural area were 9.848 times less likely to have modern contraceptive than those who reside in urban area controlling for other variables in the model (OR=9.848; 95% CI: 0.285-346.277). Women who live in tropical environmental condition were 1.8% less likely to have modern contraceptive use than women who had a cool environmental condition (OR=0.012; 95% CI: 0.000-4.342).
Furthermore, access to media is also a significant factor associated with the determinant of modern contraceptive use. Women who get access of health center were 84.4% less likely not to access media as compared to women who cannot get access to media from their homes, controlling for other variables in the model (OR=5.833; CI: 0.016 - 0.300).
Multilevel logistic regression analysis
A Chi-square test statistic was applied to assess heterogeneity in the proportion of women who had determinants of modern contraceptive use among the nine health centers. The test yield c2 = 56.382, df = 8, P < 0.001. Thus, there is an evidence for heterogeneity with respect to the distribution of modern contraceptive use among health center.
Multilevel logistic regression model comparison
Table 7 shows the predicted probability of modern contraceptive use by health center with predictors, place of residence, environmental condition, wealth index, the frequency of modern contraceptive use, type of modern contraceptive use, marital status and access of media, and HIV test. Then the maximum health center varied for predicted probability range as observed among variables in the short term of modern contraceptive. These variables have high random effects on modern contraceptive as compared to the other predictor variables and they are also used in the random coefficient model.
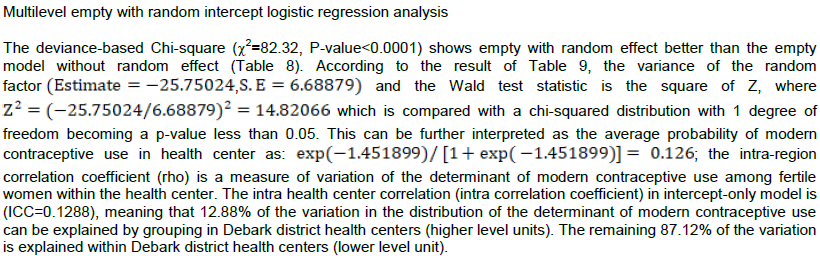
Multilevel random intercept logistic regression analysis
In multilevel random intercept logistic regression model, the probability of the determinant of modern contraceptive use was allowed to vary across health center, but assumed that the effects of explanatory variables are the same for each health center. That is, the random intercept varies across health center, but levels of explanatory variables are fixed across health center in predicting determinant of modern contraceptive use in Debark district health center (Table 10).
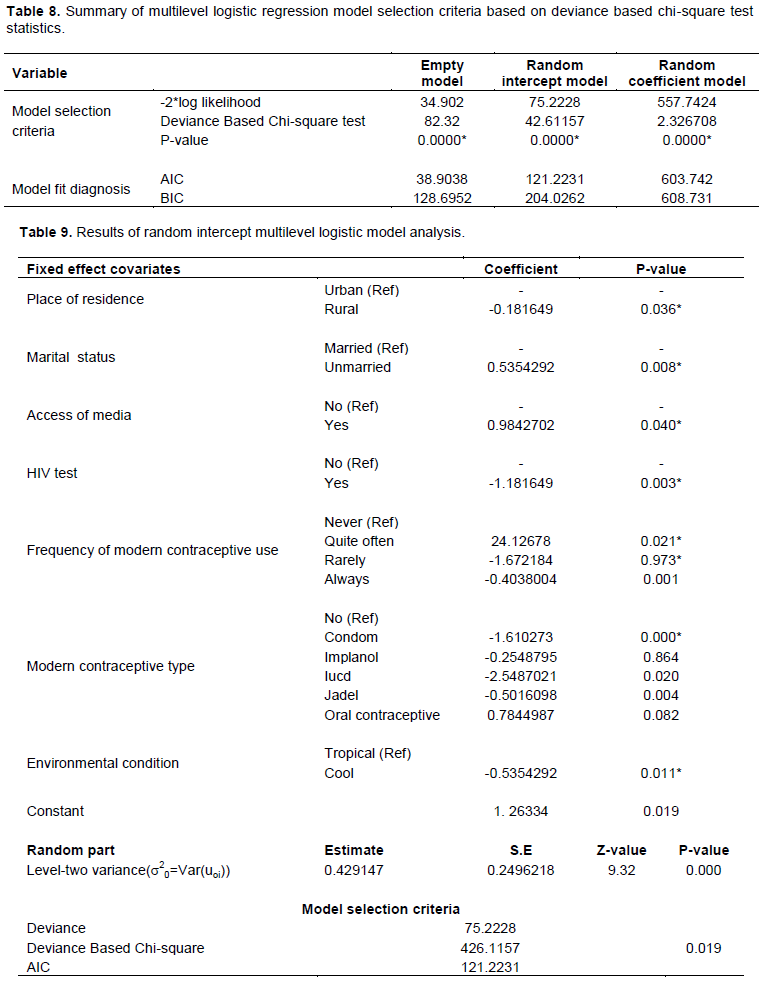
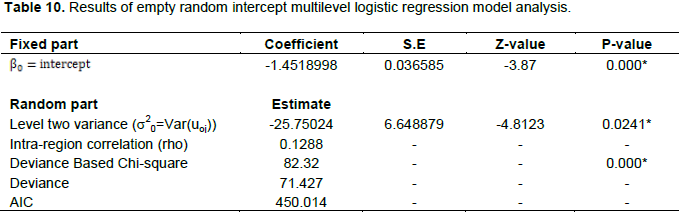
According to the result of the random intercept model, the fixed part showed that place of residence, marital status, environmental condition, access of media, frequency of modern contraceptive use, modern contraceptive type and HIV test were found to be significant determinants of variation in the determinant of modern contraceptive use among health centers. The random part of empty random intercept multilevel model showed that the intercept variance of the random effect is -25.75024, whereas the intercept variance of the random intercept model is 0.429247. The variance of random effect of the intercept multilevel model decreased as compared to the random effects of the intercept of the empty random intercept model. The reduction of the random effect of the intercept variance is due to the inclusion of fixed explanatory variables. That is, taking into account the fixed independent variables which can provide extra predictive value on the determinant of modern contraceptive in each health center.
DISCUSSION
This study aims to identify some determinants of modern contraceptive based on Debark district health office 2015 data. Accordingly, descriptive analysis, binary logistic regression, and multilevel logistic regression techniques were used. In general, the results from this study were a little consistent with most previous studies in terms of the determinants of modern contraceptive use among fertile women. The results which were obtained were discussed in the following. The descriptive analysis of this study shows that the distribution of modern contraceptive users was 95.8%. Based on the result of this study, a woman who lives in Dibbahir (10.3%), Abayseqar (10.8%), Dawe (9.4%), Tirahina (34%), and Adigagira (11.9%) health centers were more likely to have modern contraceptive than women who live in the Belles health center.
This study found that the determinant of modern contraceptive use among fertile women were significantly associated with marital status. Women whose marital status is married were 85.9% less likely to the determinant of modern contraceptive use than fertile women whose marital status is unmarried.
The finding also showed that place of residence was significantly associated with the determinant of modern contraceptive use among fertile women. This result is in agreement with Fengyu et al. (1999) who suggested that major determinant factors for modern contraceptive use were to prevent unwanted pregnancy. Similarly, the finding is consistent with Hasinur et al. (2011) who found that women had little or no access to modern contraceptive, the result revealed that the urban women were the mostly attended on regular modern contraceptive use.
The result of this study indicates that the determinant of modern contraceptive use among fertile women was significantly associated with access to media. Women who do not get the access of media were more likely to be determinant of modern contraceptive use than those who have access to media. This result is consistent with Abdurahman et al. (2014) who found that the major determinant of modern contraceptive was not getting access to media. Similarly, the findings show that women who do not have access to media were 84.6% times more affected by determinant of modern contraceptive among fertile women than those who have access to media for modern contraceptive use among fertile women.
The study showed that the likelihood of women who do not get access to media were 5.603 times more likely to affect modern contraceptive use than those women who have access to media.
The finding also shows that modern contraceptive types were significantly associated with the determinant of modern contraceptive use among fertile women. Women who use IUCD and condom were less likely than for those determinants of modern contraceptive use. This result is in agreement with 3 who suggested that major determinant factors for modern contraceptive use were to prevent unwanted pregnancy. This study found that IUCD and condom were significantly associated with the determinant of modern contraceptive use and the users of condom and IUCD were less likely to be fertile.
The model of this study revealed that the likelihood of having the determinant of modern contraceptive use among fertile women who had HIV test were 1.659 times more likely to have short-term modern contraceptive use than fertile women who had a long-term modern contraceptive use. This finding is consistent with a study done in Uganda (Saurabh et al., 2013) that revealed that the determinant of modern contraceptive use occurred in women who had an HIV test.
CONCLUSIONS
The study identified that demographic, socioeconomic, environmental and health-related variables have an important effect on determinants of modern contraceptive use in Debark district.
According to this study, multiple logistic regression showed that health center, place of residence, marital status, environmental condition, access to media, the frequency of modern contraceptive use, and modern contraceptive type were all important factors to determining the determinant of modern contraceptive use among fertile women in Debark districts.
From the results of multilevel logistic regression analysis among all the three models, the random intercept multilevel model provided the best fit for the data under consideration. It showed that the distribution was varied among health centers. Additionally, in empty with random intercept model and random intercept and fixed coefficient models, the overall variance of the constant term was found to be significant, which reflects the existence of differences in the distribution of modern contraceptive use among fertile women across health center. The significant determinant factors for the variations of distribution of modern contraceptive among health center were an environmental condition, place of residence, marital status, access of media, HIV test, the frequency of modern contraceptive use and modern contraceptive type.
RECOMMENDATIONS
Based on the findings of this study, the following recommendations are forwarded:
(1) Awareness has to be given to the society on the use of modern contraceptive.
(2) To improve the media access, awareness has to be given to the society in order to address the risk of unwanted pregnancy, the risk of abortion, use of modern contraceptive, type of modern contraceptive, the frequency of modern contraceptive, and the importance of family planning.
(3) Health officers should test the women on HIV/AIDS status before they give modern contraceptive drug because the drug has an adverse effect on those long-term users.
(4) Debark districts health office should be addressed the health centers for all kebeles because it is difficult for the user to move from one health center to another.
LIMITATIONS OF THE STUDY
The major limitations of the study are:
(1) The study is conducted based on secondary data which might have incomplete and biased information.
(2) Some important variables like discussion about modern contraceptive, weight or number of children were not included in the study due to missing values, non-response and absence of these variables in Debark district health office 2015 data.
(3) The data used in this study are from Debark district health office 2015 data. Thus, the results may not necessarily reflect the current situation of Debark district health centers because all the variables of the study were not available.
CONFLICT OF INTERESTS
The authors declare that there is no conflict of interest
REFERENCES
|
Abdurahman M, Desalegn W, Amsalu F, Berihun M (2014). Determinants of modern contraceptive utilization among married women of reproductive age group in North Shoa Zone, Amhara Region, Ethiopia. Reproductive Health. |
|
|
Beekle AT, McCabe C (2006). Awareness and determinants of family planning practice in Jimma, Ethiopia. International Nursing Review 53:269-276. |
|
|
Cox DR, Snell E1 (1989). Analysis of binary data (2nd ed.). Chapman and Hall. The journal of educational research 96(1). |
|
|
Ebigbola JA, Ogunjuyigbe PO (1998). Contraceptive Knowledge and Practice by women attending antenatal Clinic in Nigeria. Ife Social Sciences Review 15(1):20-29. |
|
|
Fengyu Z, Amy O, Tsui C, Suchindran, M (1999). The Determinants of Contraceptive Discontinuation in Northern India: A Multilevel Analysis of Calendar Data. |
|
|
Feyisetan BJ, Bamiwuye S (1998). Postpartum Counseling and Contraceptive Use in Nigeria. Social Science Research 15(1):30-41. |
|
|
Giusti C, Vignoli D (2006) Determinants of contraceptive use in Egypt: A multilevel approach. Statistical Methods and Applications 15:89-106. |
|
|
Harper SR (2004). The measure of a man: Conceptualizations of masculinity among high-achieving African American male college students. Berkeley Journal of Sociology 48(1):89-107. |
|
|
Hasinur RK, Ewart J, Shaw H (2011). Multilevel Logistic Regression Analysis Applied to Binary Contraceptive Prevalence Data. Journal of Data Science 9:93-110. |
|
|
Hosmer D, Lemeshow S (1989). Assessing the fit of the model, Noel A. C. Cressie, Nicholas I. Fisher, Iain M. Johnstone, J. Kadane, David W. et al Applied Logistic Regression. 2nd ed: New York, John Wiley and Sons, Inc.143-200. |
|
|
Mccullagh P, Nelder JA (1989). Binary data, Generalized Linear Models, Monographs on Statistics and Applied Probability, 2nd edn, Chapman and Hall, London, UK. 98-128. |
|
|
Nagelkerke NJD (1991). The analysis of binary data (2nd ed.). A note on a general definition of the coefficient of determination. Biometrika, 78:691-692. |
|
|
Oyedokun AO (2004). Domestic violence and contraceptive use in Ife-North Local Government area of Osun State, Nigeria. Unpublished M.Sc. thesis submitted to the department of Demography and Social Statistics, Obafemi Awolowo University, Ile-Ife, Nigeria. 169 p. |
|
|
Pachauri S, Santhya KG (2003). Contraceptive behaviors among adolescents in Asia: Issues and challenges. In S. Bott et al., eds. Towards Adulthood: Exploring the Sexual and Reproductive Health of Adolescents in South Asia, Geneva: World Health Organization, pp. 105-107. |
|
|
Preston LE, Sapienza HJ (1990). Stakeholder management and corporate performance. Journal of Behavioral Economics 19:361-75. |
|
|
Saurabh RS, Prateek SS, Jegadeesh R (2013). Unmet Need for Family Planning in Developing Countries: Challenges and Solutions. International Journal of Gynecological and Obstetrical Research 1(2):84-87. |
|
|
Short S, Kiros G (2002). Husbands, wives, sons, and daughters: Fertility preferences and the demand for contraception in Ethiopia. Population Research and Policy Review. 2002 ed. pp. 377-402. |
|
|
Snijders TAB, Bosker RJ (1999). Multilevel Analysis: An Introduction to Basic and Advanced Multilevel Modeling. Department of Statistics, University of Poone. 1st ed. London: Sage Publications P 266. |
|
|
Tizta T, Gily C, Stanley L, Wondwosen K, Els L, Marleen T, Olivier D (2014). Family Planning Knowledge, Attitude and Practice among Married Couples in Jimma Zone, Ethiopia. PLOS ONE. |
|
|
White J, Speizer I (2007). Can Family Planning outreach bridge the urban-rural divide in Zambia. BMC Health Services Research 7:143. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


