Full Length Research Paper

ABSTRACT
Supplementary immunization activities campaigns provide children with an additional dose of vaccine and deliver other interventions. However, there is dearth of information on knowledge, attitude and perception of mothers of under-five towards vaccination during supplementary immunization activities. A descriptive cross-sectional study which employed multistage sampling technique was designed to fill this gap. Four wards were randomly selected from eleven wards in Ibadan North-West Local Government Area and houses were enumerated from the selected wards, systematic random sampling was used to select houses and then respondents. A semi-structured interviewer administered questionnaire was used to elicit information on three hundred and five respondents. Knowledge scores of ≤4, 5-8, and ≥ 9 were rated poor, fair and good, respectively. Attitude scores of ≤5 and >5 was rated negative and positive attitude, respectively while perception scores ≤4 and >4 were rated negative and positive perception, respectively. Data was analyzed with SPSS version 25 using descriptive statistics and Chi-square test at 5% level of significance. The mean age of respondents was 30.6±6.1years, the highest level of education for most (68.5%) was secondary school. Their mean parity and number of under-five were 2.5±1.4 and 1.2±0.4, respectively. Knowledge was generally poor, more than half (53.1%) had poor knowledge, majority (88.2%) have positive attitude while 84.6% have a positive perception. One-fourth (24.6%) and one-fifth are of the opinion that frequent vaccination will make the vaccine ineffective and overload immune system, respectively. There was generally poor knowledge of supplementary immunizations and mothers need to be educated on the importance.
Key words: Immunization, supplementary immunization activities, mothers of under-five, vaccination, Nigeria.
INTRODUCTION
Immunization is one of the most effective public health interventions available, which involves conferring increased resistance to an infectious disease by means other than experiencing the natural infection. According to the 2018 Nigeria Demographic and Health Survey, vaccination coverage in Nigeria has shown an upward shift over the past 10 years. The percentage of children aged 12-23 months who received all their basic vaccinations increased from 23% in 2008 to 31% in 2018, while the percentage of children who received none of the basic vaccinations declined from 29 to 19% during the same period. Recently, vaccines have reduced the child morbidity rate greatly and saved more lives (World Health Organization [WHO], 2006). Childhood immunization is an act of actuating invulnerability to a child by applying a vaccine that almost guarantees protection from many major diseases. Childhood vaccination is widely considered to be "overwhelmingly good" by the scientific community (Givs, 2005).
WHO initiated the Expanded Program on Immunization (EPI) in May 1974, intending to vaccinate children throughout the world (WHO, 1988). The fundamental techniques for infection prevention are to eliminate or diminish the number of infecting microorganisms from circulation, enhance the host immune response, and treat the infected host. Supplementary Immunization (Mass Immunization) was an integral part of early control efforts after which polio vaccines were used for routine immunization programs. The resolution in 1988 to eradicate polio globally led to the development of appropriate strategies to achieve this goal, including supplementary immunization campaigns (that is, national immunization days, sub-national immunization days, and mop-up activities), to ensure maximum coverage in the shortest possible time.
However, to reach the maximum coverage, it is important to have comprehensive planning, proper execution, and adequate monitoring. The standard of supplementary immunization activities was arrived at after different approaches which substantially reduced the incidence of polio. The low vaccination uptake during supplementary immunization has been credited to variables such as poor knowledge, no felt need, too many rounds, religious belief, political differences, maternal education, age, occupation, marital status, home, access to media, fear of side effects, family unit riches, and place of delivery (Tagbo et al., 2014). Vaccine-preventable diseases (VPDs) cause an estimated 2 million deaths or more annually, of which about 1.5 million deaths occur in children under five. Refusal of supplementary immunization campaigns is a significant challenge (Henderson, 1999). Studies showed that some parents believed that there was no other vaccine required outside the routine vaccination like immunization plus days and had little knowledge of the supplementary immunization schedule. Parents were ignorant of the number of doses of vaccines required. A significant proportion of respondents in all states incorrectly believed that giving a child more than four vaccine doses was harmful, while others believed that the vaccine should only be given once (Babalola, 2017). Immunization which has greatly reduced the burden of infectious diseases prevents illness, disability and death from vaccine-preventable diseases including measles, pertussis, diphtheria, polio, rubella and tetanus (Yousif et al., 2013).
Immunizing a child significantly reduces the cost of treating diseases, thus providing a healthy childhood and reducing poverty and suffering (Siddiqi et al., 2010). The study was to determine the knowledge, attitude, and perception of mothers of under-fives towards this campaign. It will help determine if there is any misconception or willingness to vaccinate their children, which will affect their immunization status.
MATERIALS AND METHODS
Study design
A descriptive cross-sectional design was used for this study with the aid of semi–structured interviewer-administered questionnaire to assess the knowledge, attitude and perception of mothers of under-five towards the vaccination during supplementary immunization campaign between 2019 and 2021.
Description of study area
This study was carried out at Ibadan North-West Local Government Area (IBNWLGA) which is one of the eleven LGAs that constitute Ibadan metropolitan area. Ibadan is the capital of Oyo State, one of the 36 states of the Federal Republic of Nigeria. The state is centrally situated in the southwestern part of the country and it is 128 km north-east of Lagos and 345 km south-west of Abuja, the federal capital territory.
Ibadan Northwest Local Government Area was created out from Ibadan North West 1991 as one of the functioning LGAs in Oyo State, Nigeria by the Military head of State, General Ibrahim Babangida. The administrative headquarters of this LGA is located in Onireke. It has an area of 26 km² and a population of 152,834 at the 2006 census. Ibadan North West Local Government is bounded in the North by Ido Local Government, in the West by Ibadan South West Local Government, in the East by Ibadan North East and in the South by Ibadan South East Local Government. Ibadan North West Local Government is a predominantly urban area with eleven wards which has within his jurisdiction Onireke, Ayeye, Dugbe, Inalende, Ologuneru to mention just a few. The Local Government can boast of markets like Ayeye, Dugbe, Agbeni and Eleyele. Its inhabitants include Yoruba, Hausa, Ibo and Other tribes who engage in trading, farming, artisanship and civil service (Ajayi et al., 2018).
Study population
The study population for this research was mothers of under-five children living within IBNWLGA.
Inclusion criterion
This include mothers of under-five children willing to participate in the study.
Exclusion Criteria
This include mothers of under-five children who had not been living in the study area or just visiting; mothers of under-five children who were too sick to participate; and mothers of under-five children who were not available at the time.
Sample size determination
The number of mothers of under-five interviewed in the study area was determined using Leslie Kish formula. It was established that the desired level of reliability should not exceed 0.05 with 95% confidence interval using percentage of under-five that did not receive all basic vaccination in Oyo State of 76.7% according to Nigeria Demographic and Heath Survey (NPC and ICF Macro, 2019).
n = Z2pq/d2
where n = Sample size, Z = Standard normal deviation; 1.96, p = Prevalence of mother of under-five, q = 1 – Prevalence, d = Precision; 0.05, z = 1.96; p. 76.7% that is, 76.7/100 = 0.
q = 1 – 0.268 = 0.732
d2 = 0.05 × 0.05 = 0.0025
= 1.96 × 1.96 × 0.767 × 0.233 / 0.0025 = 0.6865 / 0.0025 = 274.6
10% Non-response rate = 274.6 / (1-0.10) = 305 (approximately)
Three hundred and five respondents were therefore targeted to participate in the study. However, the figure was raised to three hundred and five to adjust for 10% attrition rate or non-response rate from two hundred and seventy-five.
Sampling procedure
A multi-stage sampling technique was employed for this study.
Stage 1: Four (4) wards were selected from the eleven (11) wards using simple random sampling.
Stage 2: Settlements were selected from each of the four (4) wards using simple random sampling.
Stage 3: Houses in the settlements were enumerated and simple random was used to select the houses.
Stage 4: Simple random sampling was used to select the participants in the households.
Instrument for data collection
A semi-structured interviewer administered questionnaire was used to obtain the necessary information from the respondents. The questionnaire was developed by the researcher based on literature reviewed. The questionnaire was used to gather information on the socio-demographic data of the respondents, knowledge, attitude and perception of mothers of under-five towards vaccination during supplementary immunization campaigns.
Procedure for data collection
The study was carried out with the assistance of three (3) trained Research Assistants (RAs). The RAs were recruited and trained to ensure adequate understanding of the content of the study instruments as well as the data collection process and management. The trained RAs were involved in the pretest and this was done to provide them with practical experiences. Respondents were identified, questionnaires were distributed which was replicated for the main data. Both the benefits and the possible harms that may arise as a result of participating in the study was explained to the research participants. The informed consent forms (attached to the questionnaires) was read to the potential participants after they were given adequate information about the study. Then, after the questionnaire had been filled, the researcher checked for completeness and errors before leaving the field.
Validity and reliability of the instrument
Validity refers to the accuracy of an instrument, that is, how well it measures what it is supposed to measure. In order to establish validity of the instrument, it was validated by comprehensive review of relevant literature and formulation of research objectives. The instrument was also subjected to peer review before it was administered. The instrument was pre-tested among similar population and a reliability co-efficient of 0.739 (Cronbach Alpha) was gotten and the instrument was considered reliable.
Data management and analysis
All completed questionnaires were checked for completeness and consistencies of variables. Cleaning, sorting, recording and coding of data for analysis were also done. A coding guide was developed to facilitate data entry and entered into the computer using the statistical software and analyzed. Knowledge scores of ≤4, 5-8, ≥ 9 were rated poor, fair and good, respectively. Attitude scores of ≤5 and >5 were rated negative and positive attitude, respectively while perception scores ≤4 and >4 were rated negative and positive perception, respectively. The result obtained from the Statistical Package for Social Sciences (SPSS version 25) analysis summarized and presented in prose, tables and charts. The data collected were subjected to descriptive and inferential statistics which include Chi-square analysis with p-value set at 0.05 level of significance.
Ethical considerations
Ethical approval was sought and obtained from the Oyo State Ministry of Health research ethics committee before going to the field for data collection with Reference number AD 13/479/1289. Also, informed consent was obtained from the respondents. To ensure confidentiality of research participants, identifiers such as names and other information that can reveal the identity of research participants was not included in the research instruments. The nature of the study, benefits and objectives were explained to the respondents and they were assured that the information given would be treated with utmost confidentiality. Respondents were also intimated about the opportunity to withdraw their consent freely at any point during the study. Confidentiality of each participant was maximally maintained during and after the collection of their information. Information gathered from the respondents were stored in the computer for analysis by the researcher while copies of the filled instruments were kept for maximum safety.
RESULTS
Socio-demographic characteristics
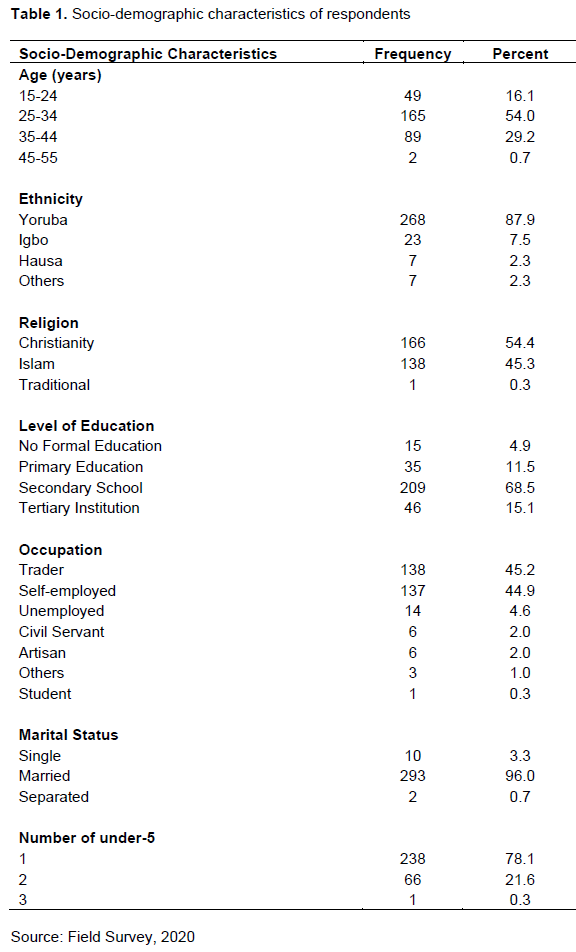
There were 305 respondents recruited for this study, which were women with under-five children. More than half of the respondents (54.1%) age ranged from 25 to 34 years old with mean age of 30.3±6.1, which 87.9% were of Yoruba ethnicity as expected due to the study area selected. More than half of the respondents (54.4%) are Christians, more than two-third (68.5%) had highest of education to be secondary school and the major occupation was trading with 45.2% of the respondents. Majority (95.7%) were married which is also expected and due to the nature of the study. Out of the married women, majority (91.5%) was in monogamous marriage, of which 78.0% had one child as under five (Table 1).
Knowledge on supplementary immunization campaign
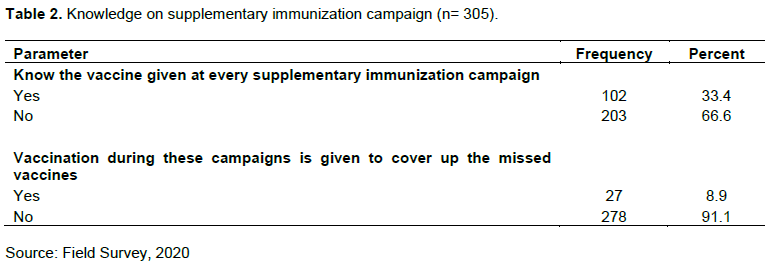
All the respondents have heard of supplementary immunization campaign with health worker being their most reliable source of information on supplementary immunization (38.0%). However, one-third (33.4%) knows the vaccine given at supplementary immunization (Table 2).
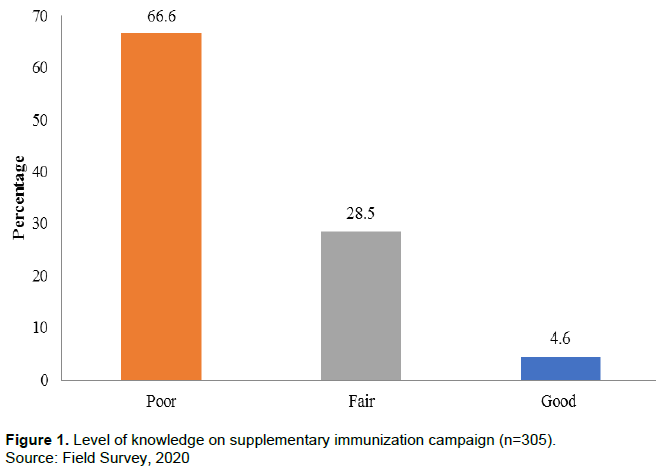
Respondents had a mean knowledge score of 3.2±1.8. The proportion of respondents’ level of knowledge was as follows: 66.6% had poor knowledge (0-3), 28.5% had fair knowledge (4-6) while 4.9% had a good knowledge (7-9) on supplementary immunization campaign (Figure 1).
Attitude on supplementary immunization campaign
Respondents mean attitude score was 13.7±2.9. The proportion of respondents’ level of perception was as follow: one tenth (11.8%) had a negative attitude, majority (88.2%) had positive attitude on supplementary immunization campaign. One-tenth (12.8%) see no need for immunization if the child is healthy, about one-tenth (11.8%) of the respondents agreed that it is better for their child to fall sick and develop immunity against the disease than to take immunization during this campaign, just few of the respondents (2.0%) agreed that authorities promote vaccination for financial gain and not for people’s health. However, majority of the respondents (92.5%) disagreed that proper information is given about the vaccine by the vaccinator, few (7.5%) sees no need for supplementary immunization after the routine immunization, majority (94.4%) agreed that most houses are always visited. Most of the respondents (88.0%) consider all the vaccine collected necessary for the child, majority (90.8%) trust the vaccinators during the supplementary immunization campaigns in vaccinating their children, almost one-tenth (12.8%) would not want to get their next child to be immunized during this period and more than half of the respondents (54.4%) will not allow their child to take the vaccine in their absence. However, about one-fifth (19.0%) of the respondents said political difference can affect their decision in allowing their child to be vaccinated and many (75.7%) can change their decision in allowing their child to be vaccinated by the influence of the religious leaders (Table 3).

Perception on supplementary immunization campaign
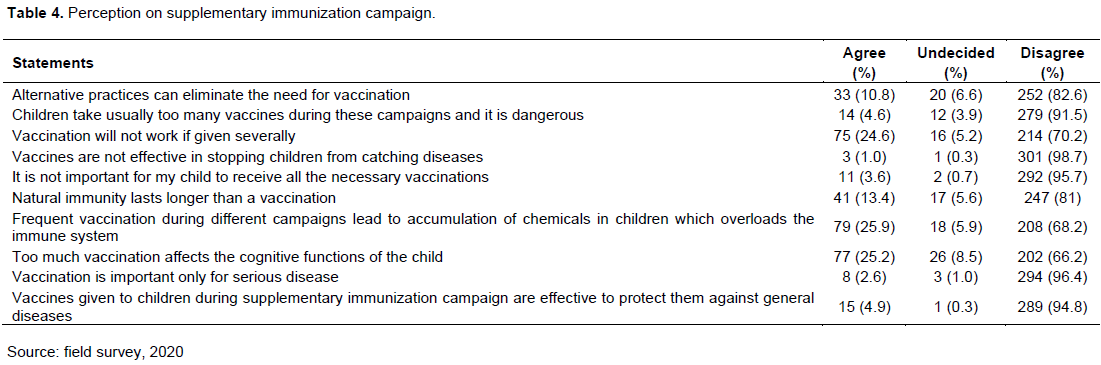
Respondents mean perception score was 8.4±2.0. The proportion of respondents’ level of perception was as follows; 15.4% had a negative attitude, 84.6% had positive attitude on supplementary immunization campaign. One-tenth (10.8%) of the respondents agreed that alternative practices can eliminate for the need of vaccination and majority (91.5%) disagreed that children usually take too many vaccines during these campaigns and it is dangerous. Also, one-fourth (24.6%) agreed that vaccination will not work if given severally, almost all the respondents (98.7%) disagreed that vaccines are not effective in stopping children from catching diseases. Only few (3.6%) perceived that it is not important for their child to receive all the necessary vaccinations, and about one-tenth (13.4%) agreed that natural immunity lasts longer than vaccination. One-fourth of the respondents are of the perception that frequent vaccination leads to accumulation of chemicals in children which overloads the immune system and too much vaccination affects the cognitive functions of the child, majority (96.4%) agreed that vaccination during this period is important only for serious disease and few (4.9%) are of the perception that vaccines given to children during supplementary immunization campaign are effective to protect them against general diseases (Table 4).
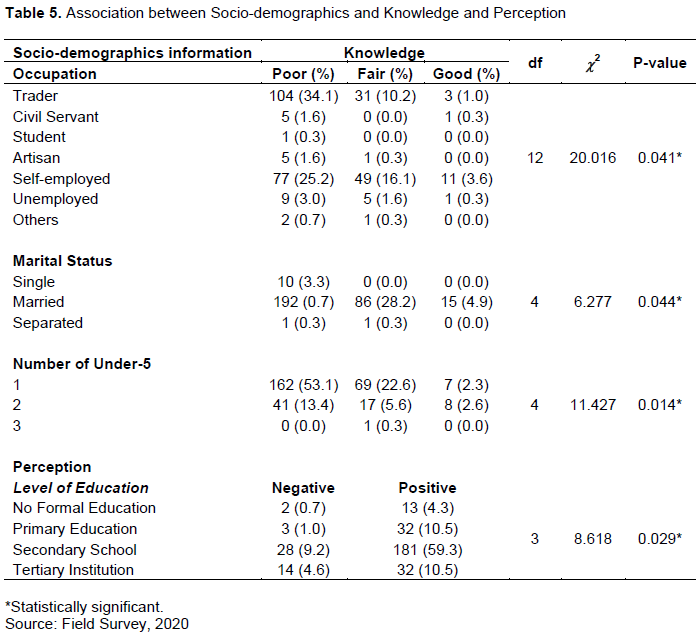
Association between socio-demographics and knowledge and perception
Fisher’s exact analysis revealed that there was a significant association between the occupation, marital status, number of under-five and the knowledge on supplementary immunization with a p-value of 0.04, 0.04 and 0.01, respectively. Also, there was a significant association between level of education and the perception on supplementary immunization with a p-value of 0.03 (Table 5).
DISCUSSION
The majority of the respondents’ age ranged from 25 to 34 years old, with a mean age of 30.3±6.1 similar to a study by Meleko et al. (2017). Many of the respondents had their highest level of education as being secondary school, which indicates that many of the respondents are literate. Trading was the major occupation of the respondents, which is a result of the nature of the community. However, a study by Abdulraheem et al. (2011) confirms the assertion by Marks et al. (1979) that educational level is associated with mothers and missed opportunities for vaccination. This implies that education cannot be overlooked when assessing factors influencing childhood immunization incompletion. All the respondents have heard of a supplementary immunization campaign similar to that studied by Kanma-Okafor et al. (2019). Few had good knowledge of supplementary immunization campaigns, lower than in a study by Hassan et al. (2019). The majority mentioned that it protects their children from diseases, which is the reason the majority had a positive perception and attitude towards the supplementary immunization campaign. One-third said that it promotes children’s growth, supported by Anekwe and Kumar (2015). Almost one-fifth of the respondents see acceptance of vaccines during this campaign as a way of increasing children’s survival. Some mentioned it reduces cases of disability, while a few agreed that it helps healthy adulthood, which is in contrast to the findings by Njidda et al. (2017), where most of the respondents agreed with it. This study revealed that the majority had a positive attitude similar to a study by Kalyani and Belsiyal (2016), which could be attributed to the general poor knowledge. This is a sharp contrast with the findings where only about half of the respondents had a positive attitude toward immunization (Birhanu et al., 2015). One-tenth did not consider the need for immunization if the child is healthy, higher than reports by Kanma-Okafor et al. (2019) and Odia et al. (2015). Few see no need for supplementary immunization after routine immunization, similar to a study by Khowaja et al. (2014). A majority of the respondents disagreed that proper information was given about the vaccine by the vaccinator and this contributed majorly to the poor knowledge of the majority. Few saw no need for house-to-house immunisation after the routine immunisation, similar to a study by Brown et al. (2015). Majority of the respondents considered all the vaccines collected necessary for the child, and almost one-tenth would not want to get their next child to be immunized during this period, which is higher than what was documented by Vonasek et al. (2016). Majority had a positive perception similar to a study by Hassan et al. (2019) on supplementary immunization campaigns. One-tenth of the respondents agreed that alternative practices can eliminate the need for vaccination, which was similar to a study by Taiwo et al. (2017) which documented that mothers give their children traditional concoctions in place of vaccines. Some agreed that children usually take too many vaccines during these campaigns and it is dangerous. This is also supported by Taiwo et al. (2017) where they mentioned that the fear of multiple vaccines overloading the immune system needs to be taken seriously to prevent obstacle to vaccine acceptance also because the knowledge about the number of times a child should receive vaccines is generally poor (Babalola, 2017). Furthermore, one-fourth agreed that vaccination will not work if given severally close to a study where mothers of children under the age of five incorrectly believed that administering more than four doses of vaccine is harmful to a child (Falade, 2014), and this is also because knowledge about how many times a child should receive vaccines is generally poor (Babalola, 2017). Almost all the respondents disagreed that vaccines are not effective in stopping children from catching diseases, similar to other studies where most believed that immunizing children was necessary for disease prevention (Angadi et al., 2013; Birhanu et al., 2015; Kanma-Okafor et al., 2019).
CONCLUSION AND RECOMMENDATIONS
This study revealed that all the respondents had heard about the immunization of under-five children, but the majority of the respondents had poor knowledge of supplementary immunization. The majority also had a positive attitude and perception towards the immunization of under-five children. There is a need for greater support for supplementary immunization campaigns, especially by educating mothers of children under five on their benefits, so as to achieve optimal nationwide immunization coverage. However, there should be a strong and persistent engagement of communities, particularly traditional and religious leaders, to improve acceptance of the vaccine; periodic education, including the need to create more jingles on air in the local dialects which the community can relate to promote acceptance of the supplementary immunization schedule; and vaccine providers need to be properly trained to strengthen the provider’s capacity for quality service.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abdulraheem IS, Onajole AT, Jimoh AAG, Oladipo AR (2011). Reasons for incomplete vaccination and factors for missed opportunities among rural Nigerian children 3(4):194-203. |
|
|
Ajayi TO, Moody JO, Anthony CS (2019). Ethnobotanical survey of plants used in the management of hypertension in Ibadan North Local Government Area of Oyo State, Nigeria. Nigerian Journal of Pharmaceutical Research 15(1):61-73 |
|
|
Anekwe TD, Kumar S (2012). The effect of a vaccination program on child anthropometry: evidence from India's Universal Immunization Program. Journal of Public Health 34(4):489-497. |
|
|
Angadi MM, Jose AP, Udgiri R, Masali KA, Sorganvi V (2013). A study of knowledge, attitude and practices on immunization of children in urban slums of bijapur city, karnataka, India. Journal of clinical and diagnostic research 7(12):2803-2806. |
|
|
Babalola S (2017). Maternal reasons for non-immunization and partial immunization in northern Nigeria. Journal of Pediatric and Child Health 47(5):276-81 |
|
|
Birhanu S, Anteneh A, Kibie Y, Jejaw A (2015). Knowledge, attitude and practice of mothers towards immunization of infants in health centres at Addis Ababa, Ethiopia. American Journal of Health Research 4(1):6-17. |
|
|
Brown VB, Oluwatosin A, Ogundeji MO (2015). Experiences, perceptions and preferences of mothers towards childhood immunisation reminder/recall in Ibadan, Nigeria: a cross-sectional study. Pan African Medical Journal 20 p. |
|
|
GIVS (2005). Global Immunization Vision and Strategy 2006-2015 Geneva: WHO/UNICEF; 2005. |
|
|
Falade BA (2014). Vaccination resistance, religion and attitudes to science in Nigeria. |
|
|
Hassan MR, Azman MA, Yong CL, Mardhiah T, Nazmi T (2019). Original article knowledge and perception towards supplementary immunization activities (sia) among mothers in cheras. kualalumpur 19(2):126-131. |
|
|
Henderson DA (1999). Lessons from the eradication campaigns. Vaccine 17:S53-S55. |
|
|
Kalyani V, Belsiyal X (2016). Knowledge, attitude and practice of mothers of under five children regarding immunization in a selected community, Rishikesh, Uttarakhand. International Journal of Recent Scientific Research 7:11301-11305. |
|
|
Kanma-Okafor O, Adefolalu O, Balogun M (2019). Maternal knowledge, attitude and compliance regarding immunization of under five children in Primary Health Care centres in Ikorodu Local Government Area, Lagos State. Journal of Clinical Sciences 16(1):7-14. |
|
|
Khowaja AR, Khan SA, Nizam N, Omer SB, Zaidi A (2012). Parental perceptions surrounding polio and self-reported non-participation in polio supplementary immunization activities in Karachi, Pakistan: a mixed methods study. Bulletin of the World Health Organization 90(11):822-830. |
|
|
Marks JS, Halpin TJ, Irvin JJ, Johnson DA, Keller JR (1979). Risk factors associated with failure to receive vaccinations. Pediatrics 64(3):304-309. |
|
|
Meleko A, Geremew M, Birhanu F (2017). Assessment of Child Immunization Coverage and Associated Factors with Full Vaccination among Children Aged 12-23 Months at Mizan Aman Town. Bench Maji Zone, Southwest Ethiopia. |
|
|
Njidda UM, Kever RT, Lola N, Dathini H, Mshelia A (2017). Assessment of parents' knowledge towards the benefits of child immunization in Maiduguri, Borno State, Nigeria. Nursing & Care Open Access Journal 3(2):226-239. |
|
|
Odia OJ, Okafor IP, Roberts AA (2015). Knowledge, Attitude and Practice of Childhood Immunization among Mothers of Under-Fives in Kosofe Local Council Development Area. Lagos State Journal of Community Medicine and Primary Health Care 27(1):55-63. |
|
|
Siddiqi N, Siddiqi A-E-A, Nisar N, Khan A (2010). Mothers' knowledge about EPI and its relation with age-appropriate vaccination of infants in peri-urban Karachi. Journal of the Pakistan Medical Association 60(11):940-944. |
|
|
Tagbo BN, Eke CB, Omolowo BI, Onwuasigwe CN, Onyeka EB, Mildred UO (2014). Vaccination Coverage and its Determinants in Children Aged 11-23 Months in an Urban District of Nigeria. World Journal of Vaccines 4(4):175-183. |
|
|
Taiwo L, Idris S, Abubakar A, Nguku P, Nsubuga P, Gidado S, Okeke L, Emiasegen S, Waziri E (2017). Factors affecting access to information on routine immunization among mothers of under 5 children in Kaduna State Nigeria, 2015. Pan African Medical Journal 27(1):186. |
|
|
Vonasek BJ, Bajunirwe F, Jacobson LE, Twesigye L, Dahm J, Grant MJ, Sethi AK, Conway JH (2016). Do maternal knowledge and attitudes towards childhood immunizations in rural Uganda correlate with complete childhood vaccination? PLoS One 11(2):e0150131. |
|
|
World Health Organization (WHO) (2006). Challenges in global immunization and the global immunization vision and strategy 2006-2015. Weekly Epidemiological Record= Relevé épidémiologique hebdomadaire 81(19):190-195. |
|
|
World Health Organization (WHO) (1988). Polio eradication by the year 2000. Resolutions of the 41th World Health Assembly. Geneva: World Health Organization, 1988 (WHA resolution no. 41.28) |
|
|
Yousif MA, Albarraq AA, Abdallah MA, Elbur AI (2013). Parents′ Knowledge and Attitudes on Childhood Immunization, Vaccines Vaccin Taif. Saudi Arabia J Vaccines Vaccin 5(215):2. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


