Full Length Research Paper

ABSTRACT
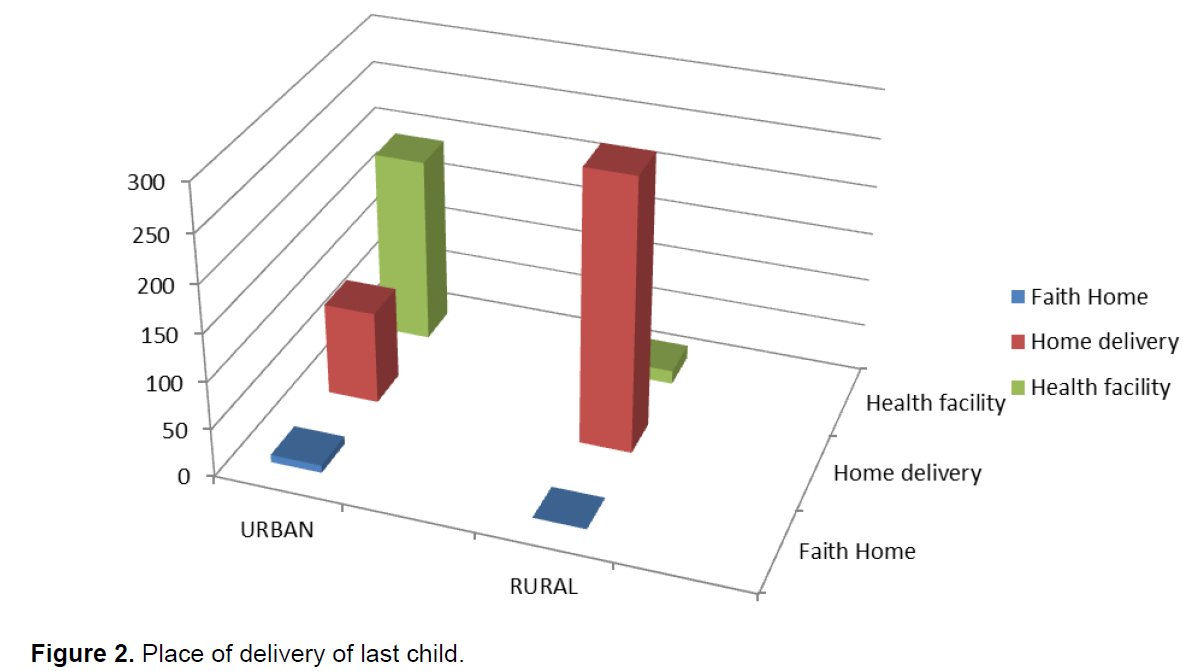
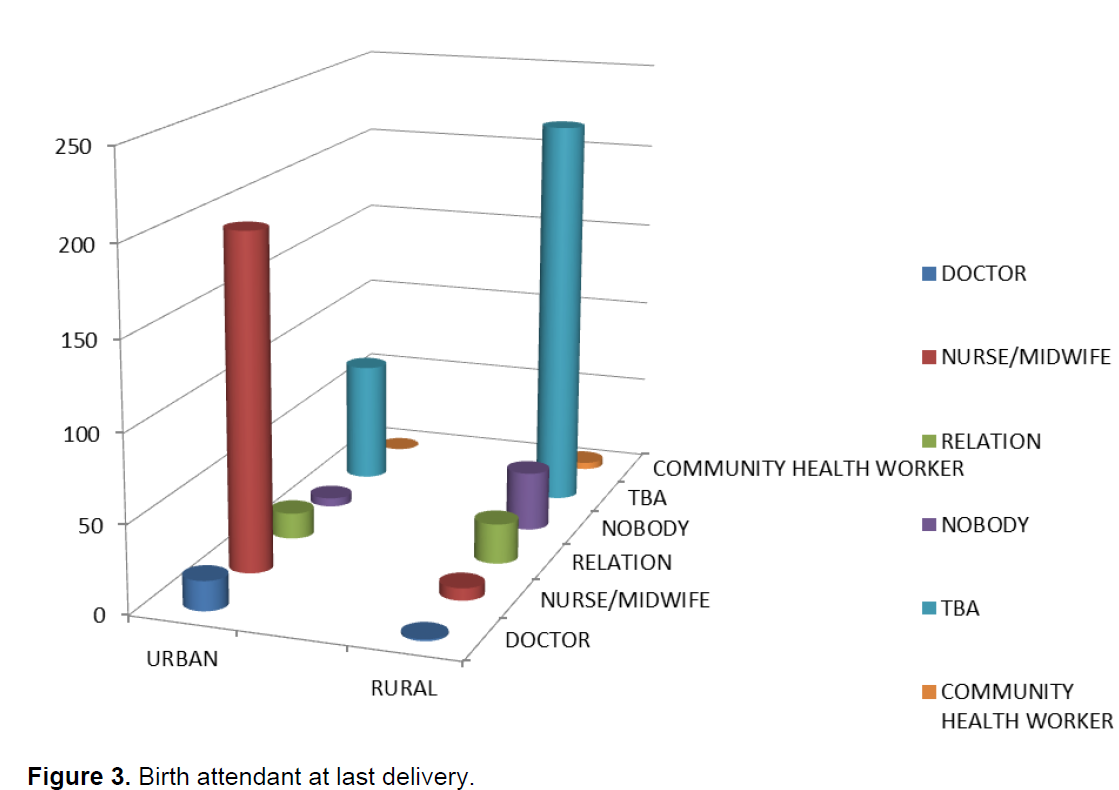
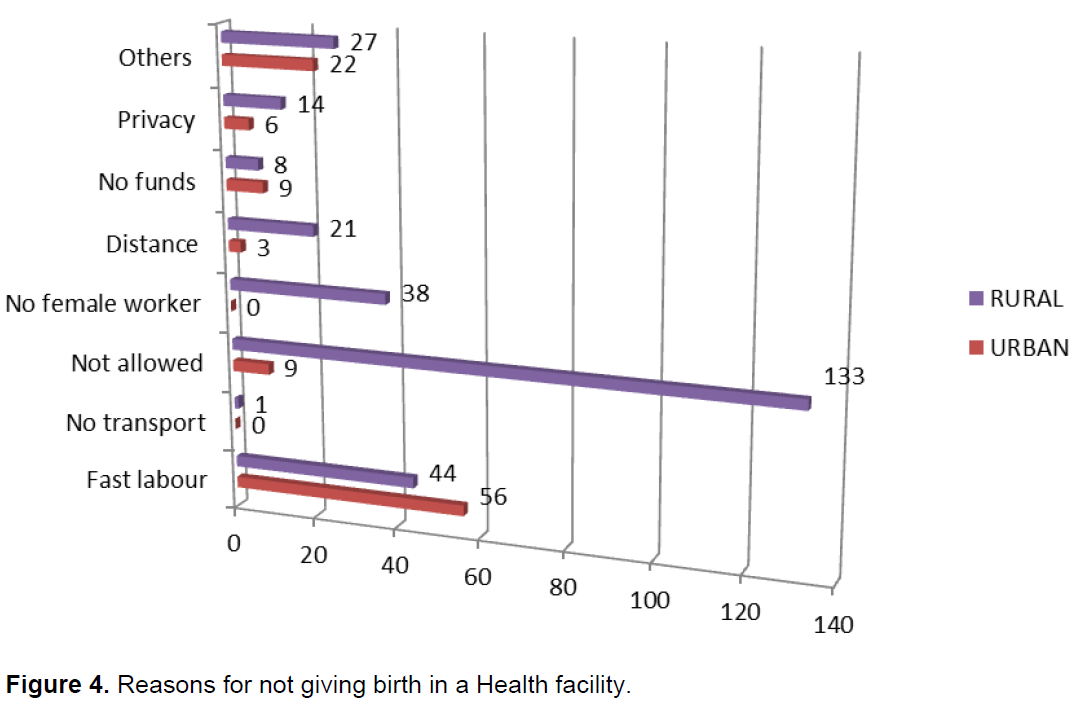
Child-birth is a risk producing event that requires timely and adequate medical intervention for women who experience obstetric complications. The provision of a health worker with midwifery skills at every birth, plus access to emergency hospital obstetric care, is the option to mitigate this risk. However, in sub Saharan Africa, most births take place outside health facilities and without skilled attendants. This study aimed to determine and compare the factors which influence the choice of place of delivery among women in an urban and a rural community in Sokoto. It was a cross-sectional comparative study of 600 randomly selected women of reproductive age, in Sokoto South and Gwadabawa Local Government Areas of Sokoto State, Nigeria using semi-structured interviewer administered questionnaires. The proportion of women who delivered in health facilities was 65.0 and 4.7% in the urban and rural groups, respectively; whereas the proportion that had skilled attendants at delivery was 70 and 4.3% in the urban and rural groups, respectively. Lack of consent from husband, no privacy in health facilities, distance to the health facility and non-availability of delivery wards were the reasons for home deliveries in the rural study group, while the emergency nature of labour was the reason in the urban group. Women residing in rural areas need health promotion interventions in order to meet the International Conference on Population and Development + target of achieving 90% births attended by skilled attendants by 2015.
Key words: Determinants, place of delivery, skilled attendant, urban and rural, Sokoto.
INTRODUCTION
In Africa, about 50% of births were attended by a skilled health worker (WHO, 2014) despite an increase from 55 to 66% between 1990 and 2011 in all developing regions as indicated by the 2013 Millennium Development Goals Report (The MDG Report, 2013). These figures are far lower than the global target for this indicator which aimed to ensure that at least 90% of births worldwide be attended by skilled health personnel by 2015 (UNFPA, 2011). Though about 85% of women do not experience major problems during childbirth (WHO, 2013), complications that do occur can be sudden and unpredictable, requiring immediate action. Maternal and perinatal outcomes in such cases are greatly improved when such complications occur in the presence of a skilled attendant. Thus, the provision of a health worker with midwifery skills at every birth, plus access to emergency hospital obstetric care, is considered the most crucial intervention for safe motherhood (UNFPA, 2011).
In Nigeria, estimates of maternal mortality ratio vary from 300 to 400 per 100,000 live births in parts of Southwest Nigeria to as high as 1,800 per 100,000 live births in Northwest and Northeast of Nigeria (FMOH, 2011). The number of maternal deaths in Nigeria going by the WHO, UNFPA and UNICEF estimates of maternal mortality in 2010 was 57,000; giving a maternal mortality ratio of 867 per 100,000 live births; range from 673 to 1,130 per 100,000 live births. According to the 2013 Nigerian Demographic and Health Survey (NDHS, 2013), 11.5% of women of the Northwest region of Nigeria delivered at a health facility, while 19.5 and 45.7% of women of the Northeast and Northcentral regions, respectively delivered at a health facility. This was in sharp contrast to the 78.1 and 75.0% of women in the Southeast and Southwest region of the country who delivered at a health facility. In another baseline survey by UNFPA of UNFPA Assisted States in Nigeria, the proportion of women who delivered in a health facility was found to be high in Anambra (87.9%), Abia (82.8%), Osun (76.4%) and Ogun (74.2%) states, while in Sokoto (5.7%), Kebbi (8.2%) and Katsina (7.5%) states, the proportions were extremely low (UNFPA, 2010). Furthermore, a cross-sectional study carried out among women in a semi-urban settlement in Giwa, Northwestern Nigeria revealed that majority (76%) of the women had their deliveries at home and were not supervised by skilled personnel (Idris et al., 2013), while another study of women attending antenatal care at the Usmanu Danfodiyo University Teaching Hospital Sokoto showed that despite the fact that these women received antenatal care at the Tertiary Institution, 31.5% delivered elsewhere and majority (15.3%) of the deliveries elsewhere took place at the woman’s home (Ekele and Tunau, 2007).
Previous studies have reported that factors that determine place of delivery include cultural, socioeconomic, demographic and service accessibility factors. Rural residence, low socioeconomic status, young maternal age, low maternal or paternal educational attainment and high birth-order have been observed to be associated with high probabilities of delivery outside a health facility (Envuladu et al., 2013; Yegezu and Kitila, 2014; Nanang and Atabila, 2014; Kruger et al., 2011). In a study in Aba, Southeastern Nigeria which aimed to identify determinants of choice of non-institutional birth places and reasons for such, the major factors found included cost, friendly staff and perceived experience of birth attendant (Nduka and Nduka, 2014), while educational attainment was found to be the most consistent determinant of both ANC attendance and skilled assistance in delivery in Kaduna State of Nigeria (Oguntunde et al., 2010).
The high level of maternal mortality in developing countries has been attributed partly to the non-availability of maternal and child health services and partly to the poor-utilization of these services where they exist. Access to quality care during pregnancy and especially at delivery has been observed to be the crucial factor in explaining the disparity in maternal mortality and morbidity between the developing and the industrialized countries (Silal et al., 2012). An estimated 90% of maternal deaths would be avoided if adequate care was provided during the intrapartum period (Crowe, 2012). Appropriate delivery care is important for both maternal and perinatal health, especially in cases where delivery complications arise. As such providing skilled care at birth not only reduces maternal mortality but has been found to also reduce infant mortality (Ekirapa-Kiracho et al., 2011).
Thus, the knowledge of possible factors that determine the choice of place of delivery among pregnant mothers will enable us to design appropriate interventions to meet the maternal health care needs of this sub-population. This has not been explored among the rural population of Sokoto as most quoted studies were health-facility based.
This aims of this study was to determine and compare the factors that influence the choice of place of delivery among women in an urban and a rural community in Sokoto, Northwest Nigeria, with a view to making recommendations that will improve deliveries by skilled birth attendants in the short term and hopefully, also reduce the high maternal mortality and improve other maternal health indicators in the area in the long term.
MATERIALS AND METHODS
Sokoto State in its present form came into being in October 1996 when Zamfara State was carved out. With a land area of 28,232.37 km2, the state is located between longitudes 11° 30" to 13° 50" East and latitude 4° to 6° North. It is bordered in the North by Niger Republic, Zamfara State to the East and Kebbi State to the South and West. According to the provisional figures of the 2006 National Population Census, Sokoto State has population of 3,696,999 people made up principally of two major groups, namely, Hausa and Fulani. Culturally, the state is homogenous. The people of the state are Muslims and Islamic religion provides them with a code of conduct and behaviour.
Women of child bearing age constitute about 20% of the total population and are therefore a major consumer of health care services. Women die mainly from complications during pregnancy and delivery due to hemorrhage, sepsis, preeclampsia/eclampsia, anemia, and malaria resulting largely due to inadequate maternal healthcare (Shamaki et al., 2013). The population that largely reside in the rural areas are poor and uneducated. The state has 23 LGAS, 120 health districts and 244 political wards. Presently, there are 538 health facilities within the three tiers of health care delivery system. Among these are two tertiary health facilities owned by the Federal Government, namely, the Usmanu Danfodiyo University Teaching Hospital (UDUTH) and the Federal Neuro-psychiatric Center at Kware. The state government has a specialist hospital in Sokoto and 18 general hospitals fairly distributed within the 23 LGAs. The remaining are Primary Health Centres, Clinics and dispensaries run by the LGA councils. Free medical care was restricted to leprosy, tuberculosis and HIV/AIDS, but has recently been extended to include children under five years and pregnant women.
Gwadabawa is a LGA in Sokoto State. Its headquarters are in the town of Gwadabawa on the A1 highway. It has an area of 991 km² and a population of 231,358 as per the 2006 census. Its coordinates are 13°22′11″N 5°13′48″E13.36972°N 5.23°E. It is mainly a rural area and the population are mainly farmers and artisans.
Sokoto South is also a LGA in Sokoto State, Nigeria. Its headquarters are in Shiyar Sarkin Zamfara. It has an area of 41 km² and a population of 194,914 at the 2006 census. Its coordinates are 13°03′N 5°13′E13.05°N 5.217°E. It is situated in the Sokoto metropolis which is highly urbanised. Traders form a greater percentage of the population, while the rest are civil servants, artisans and people of other occupations (Imam, 2006).
Study design
The study was a cross-sectional comparative study conducted in Sokoto South (urban) and Gwadabawa (rural) LGAs of Sokoto, Sokoto State, Nigeria, in August 2010. Quantitative research methods were employed and involved interviews to a random sample of 600 women, aged 15 to 49 years, who gave birth within two years prior to the study. The time restriction was to aid recall of reasons for choice of place of delivery. The minimum sample size in this cross-sectional study design was determined by using the formula:
n = z² pq/d² (the study population was more than 10,000)
where n = minimum sample size required, z = standard normal deviate at 95% confidence level =1.96, p = estimated proportion of variable of interest in the population =78%, that is, 0.78 (Idris et al., 2006), d = tolerable alpha error or precision = 0.05, q = complementary probability of p (q = 1 – p), n = was therefore estimated at 263.69, approximately 264 subjects.
To accommodate for non-response and rejection of participation, the estimated sample size, n, was divided by 0.9 (with the anticipation of a 90% response rate, R). Thus, ns = n/R = 263.69/0.9 = 292.98 approximately 300 subjects, in each of the two study areas. They were selected by a multistage sampling method.
Stage 1: A random selection of one rural LGA and one urban LGA in Sokoto State, using balloting (rolled and picked papers) procedure was done. Gwadabawa and Sokoto South LGAs were picked respectively.
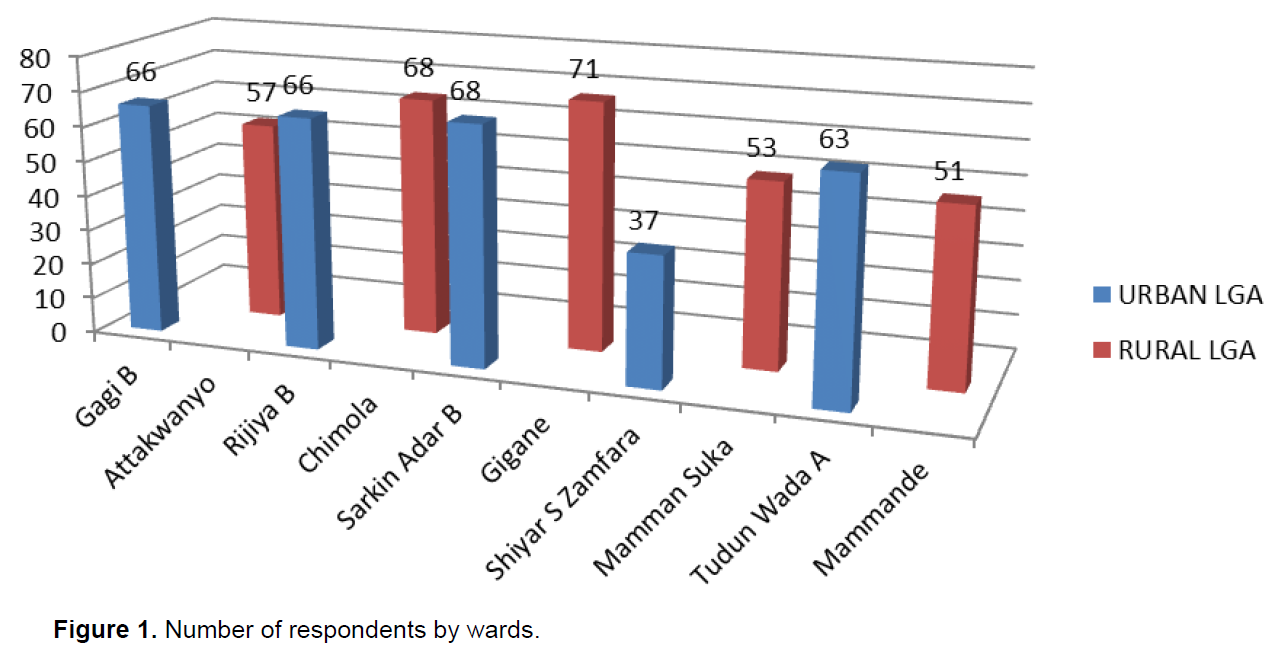
Stage 2: Then stratification of each randomly selected LGA by ward and random selection of five wards from each LGA using balloting (rolled and picked papers) procedure was done. Chimola, Gigane, Mammande, Mamman Suka and Attakwanyo wards were picked from Gwadabawa LGA while Sarkin Adar B, Shiyar Sarkin Zamfara A, Gagi B, Tudun Wada A and Rijiya B wards were picked from Sokoto South LGA.
Stage 3: Proportionate allocation of respondents to the 5 randomly selected wards was done based on the population of women of childbearing age. Sampling interval was determined using the proportionate allocation and the population of women of childbearing age in the selected wards.
Stage 4: House numbering and listing was then carried out to determine the number of houses in each of the selected wards. The calculated sampling interval was used to select the houses in the wards to be included in the study. To determine which integer to be used, simple random sampling by balloting was done. It was assumed that each house had a woman with a child of 2 years old or less. However, in an event that more than one woman in a house is qualified, balloting was done to select who was studied. On the other hand, where there was no woman that qualified in the selected house, the next house was used.
The houses were visited between 9am to 2pm each day except weekends until the study was completed. The starting point was the first house nearest to the well in the east and by simple random sampling every third house was selected for the study. Sampling occurred until the sample size was reached. All the women who agreed to participate were interviewed.
The method of data collection was by the use of questionnaires. An instrument, a semi-structured interviewer administered questionnaire with closed and open-ended questions was used. The questionnaire included: sociodemographic characteristics of the subjects, obstetric history of the subjects, availability and accessibility of maternity services to the subjects, antenatal attendance or otherwise in the last pregnancy, place of delivery of last child and reason for the choice, postnatal attendance and practise of family planning or otherwise in last pregnancy.
Questionnaires were sorted out manually for accuracy and completeness. Data processing was done using the Epi-info version 3.4.1, Microsoft Excel and Graph pad Instat, Computer Statistical Software Packages. The data is presented using graphs and tables for frequencies and percentages of the variables. The Chi-square test was used to compare differences between proportions, while the student t-test was used for comparison of mean differences. All statistical analysis was at 5% level of significance, p≤ 0.05 (that is, 95% confidence interval).
Twenty female students of School of Midwifery, UDUTH, Sokoto who spoke the Hausa language fluently were recruited to serve as research assistants and a day training was organized to intimate them with the objectives and the various aspects of the study. They were trained specifically on the general principles and conduct of survey research, manner of entry and interaction with the community, use of survey instruments and the entire conduct of the study procedure.
Approval to carry out the study was obtained from the ethics committee of the Usmanu Danfodiyo University Teaching Hospital, Sokoto. Permission to carry out the study was also obtained from the Health Department of the LGAs selected for the study. Advocacy visit was done to establish rapport with the village head of the rural local government area chosen. Informed consent was obtained from the women; the purpose of the study was explained to them. Strict compliance was made to Helsinki declaration on the use of human subject for studies (Helsinki, 1996).
RESULTS
DISCUSSION
LIMITATION
CONCLUSION
The analysis of place of delivery in this study examined delivery care in terms of "home" deliveries versus health facility deliveries. Factors influencing place of delivery are very similar to factors associated with childbirth attendant, which is not surprising, given the high correlation between the two.
In the rural study area, few pregnant women sought antenatal care, few delivered in health facilities and fewer still had deliveries attended by skilled personnel. Therefore, women residing in rural areas need urgent and intensive health promotion interventions in order to meet the International Conference on Population and Development + target of achieving 90% births attended by skilled attendants by 2015.
On the other hand, the findings in the urban study area were more encouraging. However, more still needs to be put in place to tackle the reasons/factors shown from this study that affected choice of place of delivery.
RECOMMENDATIONS
CONFLICT OF INTERESTS
REFERENCES
|
Adekoya JA, Aluko-Arowolo SO (2012). Pregnancy duration and choice of ante-natal and delivery care in selected rural and mixed urban areas of Ijebu, South Western Nigeria. Gender Behaviour. 10(1):4370. |
|
|
Adekunle OO, Similoluwa AO (2012). Determinants of place of delivery among booked patients in a tertiary institution. Ann. Afr. Med. 11:192-3 |
|
|
Ashimi AO, Amole TG (2015). Prevalence, reasons and predictors for home births among pregnant women attending antenatal care in Birnin Kudu, North-west Nigeria. Sexual Reproductive Healthcare 6(3):119-125. |
|
|
Awoyemi TT, Obayelu OA, Opaluwa HI (2011). Effect of distance on utilization of health care services in rural Kogi State, Nigeria. J. Hum. Ecol. 35(1):1-9. |
|
|
Berhan Y, Berhan A (2014). Antenatal Care as a Means of Increasing Birth in the Health Facility and Reducing Maternal Mortality: A Systematic Review. Ethiopian J. Health Sci. 24(0 Suppl):93-104. |
|
|
Choe S-A, Kim J, Kim S, Park Y, Kullaya SM, Kim C (2016). Do antenatal care visits always contribute to facility-based delivery in Tanzania? A study of repeated cross-sectional data. Health Policy and Planning 31(3):277-284. |
|
|
Crowe S, Utley M, Costello A, Pagel C (2012). How many births in sub-Saharan Africa and South Asia will not be attended by a skilled birth attendant between 2011 and 2015? BMC Pregnancy Childbirth, 17(12):4. |
|
|
Doss C (2013). Intrahousehold bargaining and resource allocation in developing countries. The World Bank Res. Observer 28(1):52-78. |
|
|
Ekele BA, Tunau KA (2007). Place of delivery among women who had antenatal care in a teaching hospital. Acta Obstet. Gynecol. Scand. 86(5):627-630. |
|
|
Ekirapa-Kiracho E, Waiswa P, Rahman MH, Makumbi F, Kiwanuka N, Okui O, Rutebemberwa E, Bua J, Mutebi A, Nalwadda G, Serwadda D (2011). Increasing access to institutional deliveries using demand and supply side incentives: early results from a quasi-experimental study. BMC international health and human rights 11(1):1. |
|
|
Envuladu EA, Agbo HA, Lassa S, Kigbu JH, Zoakah AI (2013). Factors determining the choice of a place of delivery among pregnant women in Russia village of Jos North, Nigeria achieving the MDGs 4 and 5. Int. J. Med. Biomed. Res. 2(1):23-27. |
|
|
Federal Ministry of Health (2011) Concept Note on Health System Strengthening Initiative: Consensus Strategy for Mortality Estimation . Abuja, Nigeria: Federal Ministry of Health. |
|
|
Gabrysch S, Cousens S, Cox J, Campbell O (2011). Distance and quality of care strongly influence choice of delivery place in rural Zambia: A study linking national data in a Geographic Information System. J. Epidemiol. Community Health 65:A42-A42. |
|
|
Helsinki Declaration (1996). Provide the title British Medical Journal. 313:1148-1149. |
|
|
Idris SH, Gwarzo UM, Shehu AU (2006). Determinants of place of delivery among women in a semi-urban settlement in Zaria, Northern Nigeria. Ann. Afr. Med. 5:68-72. |
|
|
Idris SH, Sambo MN, Ibrahim MS (2013). Barriers to utilization of maternal health care services in a semi-urban community in northern Nigeria: The client's perspective. Niger Med. J. 54:27-32. |
|
|
Imam A (2006) Prevalence of coliform bacteria on environmental surface in day care centres and nursery schools in Sokoto metropolis. MPH Dissertation, Usmanu Danfodiyo University, Sokoto. |
|
|
Kitui J, Lewis S, Davey G (2013). Factors influencing place of delivery for women in Kenya: an analysis of the Kenya demographic and health survey, 2008/2009. BMC Pregnancy and Childbirth 13:40. |
|
|
Kruger CC, Olsen OE, Mighay E, Ali M (2011). Where do women give birth in rural Tanzania? Rural Remote Health 11(3):1791. |
|
|
Lwelamira J, Safari J (2012). Choice of Place for Childbirth: Prevalence and Determinants of Health Facility Delivery Among Women in Bahi District, Central Tanzania Asian J. Med. Sci. 4(3):105-112. |
|
|
Nekesa JM, Mbugua S, Mukthar V (2013). Male Involvement in Maternal Health Care as a Determinant of Utilization of Skilled Birth Attendants in Kenya Demographic and health surveys Vol. 93. |
|
|
Nanang ML, Atabila A (2014). Factors predicting home delivery among women in Bosomtwe-Atwima-Kwanwoma district of Ghana: A case control study. Int. J. Med. Public Health 4:287-291. |
|
|
Nduka I, Nduka EC (2014). Determinants of noninstitutional deliveries in an urban community in Nigeria. J. Med. Investigations Practice, 9(3):102. |
|
|
Oguntunde O, Aina O, Ibrahim MS, Umar HS, Passano P (2010). Antenatal care and skilled birth attendance in three communities in kaduna state, Nigeria. Afr. J. Reprod. Health 14(3):89-96. |
|
|
Onta S, Choulagai B, Shrestha B, Subedi N, Bhandari GP, Krettek A (2014). Perceptions of users and providers on barriers to utilizing skilled birth care in mid- and far-western Nepal: a qualitative study. Global Health Action, 7, 10.3402/gha.v7.24580. |
|
|
Pervin J, Moran A, Rahman M, Razzaque A, Sibley L, Streatfield PK, Reichenbach LJ, Koblinsky M, Hruschka D, Rahman A (2012). Association of antenatal care with facility delivery and perinatal survival - a population-based study in Bangladesh. BMC Pregnancy Childbirth 16(12):111. |
|
|
Ravi RP, Ravishankar AK (2014). "Does Socio-demographic Factors Influence Women's Choice of Place of Delivery in Rural Areas of Tamilnadu State in India." Am. J. Public Health Res. 2(3):75-80. |
|
|
Silal SP, Penn-Kekana L, Harris B, Birch S, McIntyre D (2012) Exploring inequalities in access to and use of maternal health services in South Africa. BMC Health Serv. Res. 12:120. |
|
|
Singh A, Kumar A, Pranjali P (2014). Utilization of maternal healthcare among adolescent mothers in urban India: evidence from DLHS-3. PeerJ, 2:e592. |
|
|
Shamaki MA, Rostam K, Adamu YM (2013). Targeting poverty to improve maternal health in Sokoto State, Nigeria. Malaysian J. Society and Space 3:38-46. |
|
|
Shimamoto K, Gipson JD (2015). The relationship of women's status and empowerment with skilled birth attendant use in Senegal and Tanzania. BMC Pregnancy and Childbirth, 15:154. |
|
|
Some TD, Sombie I, Meda N (2011). Women's perceptions of homebirths in two rural medical districts in Burkina Faso: a qualitative study. Reproductive health 8(3):1-7. |
|
|
Shah R, Bélanger D (2011). Socioeconomic correlates of utilization of maternal health services by tribal women in India. Can. Stud. Popul. 38(1-2):83-98. |
|
|
The Millennium Development Goals Report (2013). New York; United Nations, 2013. |
|
|
Tukur D, Oche MO (2015). Determinants of antenatal care, institutional delivery and postnatal care services utilization in Nigeria. The Pan Afr. Med. J. 21:321. |
|
|
UNFPA (United Nation Population Funds) (2010). "Healthcare Services in UNFPA Assisted States of Nigeria" Sokoto State Report, prepared by UNFPA Nigeria Country Office, November 2010 |
|
|
UNFPA (2011). Main Report State of the World's Midwifery 2011. UNFPA. |
|
|
WHO World Health Organisation, UNICEF, UNFPA, The World Bank (2014). Trends in maternal mortality: 1990 to 2013. WHO, UNICEF, UNFPA and The World Bank estimates. Geneva: World Health Organisation. |
|
|
WHO (World Health Organization) (2013). Maternal mortality, Millennium Development Goal (MDG) 5. |
|
|
Yar'zever I, Said IY (2013). Knowledge and barriers in utilization of maternal health care services in Kano State, Northern Nigeria. Eur. J. Biol. Med. Sci. Res. 1(1):1-14. |
|
|
Yegezu RT, Kitila SB (2014). Assessment of factors affecting choice of delivery place among pregnant women in Jimma Zone, South West Ethiopia: Cross Sectional Study. J. Women's Health Care 4:211. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


