Full Length Research Paper

ABSTRACT
Toxoplasma gondii is an obligatory intracellular parasite that causes a zoonotic disease capable of infecting nearly all warm-blooded hosts, including humans. However, reports on the molecular prevalence of T. gondii in humans are rare in Gabon. The present study aimed to evaluate the serological and molecular prevalence of T. gondii among apparently healthy rural populations in four regions of Gabon. This study included six hundred blood samples from the Interdisciplinary Center for Medical Research (CIRMF) bank, including 300 women and 300 men living in 111 villages. Blood samples were screened using enzyme-linked fluorescent assay (ELFA), while buffy coat samples were analyzed using PCR analyses. Of the 600 samples screened, 548 (91.3%) showed IgG antibodies against T. gondii; 11 (2%) had both IgG and IgM. Among the 548 positive samples, 155 (28%) had higher IgG titers (>300 UI/ml), and 49 of them (31.6%) were detected with T. gondii DNA. The present findings on human toxoplasmosis in Gabon suggest that at an older age, reactivation of old infections seems more frequent than new infections, as indicated by the presence of T. gondii using PCR among elevated IgG subjects without IgM. Further studies should be performed to identify the genotypes of T. gondii that infect humans in Gabon.
Key words: Toxoplasma gondii, humans, DNA, Gabon.
INTRODUCTION
Toxoplasma gondii is an obligatory intracellular parasite capable of infecting nearly all warm-blooded hosts, including humans (Howe and Sibley, 1995). Toxoplasmosis is distributed worldwide and infects up to one-third of the human population. Its prevalence varies among different geographical regions. In humans, the disease is transmitted through the ingestion of inadequately cooked or raw meat containing tissue cysts (bradyzoites) or by consuming fruits, vegetables, or water contaminated with oocysts (“spores”) (Dubey, 1998; Pleyer et al., 2019). Moreover, congenital transmission during pregnancy from mother to child is essential in its transmission. Non-specific or no symptoms in immunocompetent persons characterize toxoplasmosis. However, among immune-compromised patients (for example, HIV+/AIDS patients), it may cause severe consequences and even death (Tenter et al., 2000).
Detecting T. gondii is crucial for diagnosis and treatment and for characterizing epidemiological patterns and prevention. Diagnosis of toxoplasmosis infection is usually based on serological screening through the detection of anti-toxoplasmosis antibodies (IgG & IgM) using the Enzyme?linked Immunosorbent Assay (ELISA) approach (Botein et al., 2019; Ebrahimzadeh et al., 2018). Recently, molecular methods have been widely used to diagnose toxoplasmosis because of their high sensitivity (Alfonso et al., 2009; Nimri et al., 2004). Molecular diagnostics of toxoplasmosis generally target specific DNA loci (35-repeated B1 gene, 529 bp repetitive element, 18S rDNA, and ITS1) (de Wit et al., 2020; Farhadi et al., 2017; Homan et al., 2000).
Many studies on human toxoplasmosis in Gabon have been based on serological screening. These studies mainly focused on pregnant women (Nabias et al., 1998), and few deal with the general population (Duong et al., 1992a, b; Bisvigou et al., 2009)without any reports on the molecular detection of T. gondii. The only known study that used molecular methods to detect T. gondii was focused on genotyping different strains from animals after bioassays using swiss mice (Mercier et al., 2010). In the present study, we attempted to assess the toxoplasmosis situation in rural populations in four regions of Gabon based on serological and molecular detection. Blood samples collected from apparently healthy rural people between 18 and 70 years old were examined to determine the serological and molecular prevalence of T. gondii.
MATERIALS AND METHODS
Study site
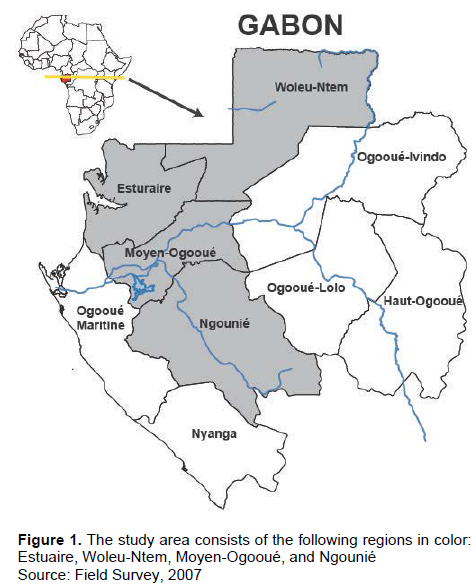
The study was conducted using samples from four regions of Gabon: Estuaire, Woleu-Ntem, Moyen-Ogooué, and Ngounié (Figure 1). The northwestern region of Estuaire has a very cosmopolitan rural population of diverse origins. It is open to the rest of the world through the Atlantic Ocean, mainly through the Owendo port and the Libreville airport. The Woleu-Ntem region, located in the forest zone in the far north, borders Cameroon and the Equatorial Guinea Republic, through which it connects with the rest of the continent. The Moyen-ogooué region, located almost in the center of Gabon, spans the equator. It is a forest area crossed by the Ogooué River with a predominantly indigenous population. The savannah region of Ngounié has a mixed indigenous population. Study sites were put into two groups based on their level of exchange with the outside world: a high exchange group (Estuaire and Woleu-Ntem) vs. a low exchange group (Moyen-Ogooué and Ngounié). Rural areas (villages) were selected because of the close relationship between the populations living there and the forest.
Study population and ethical consideration
The study involved people aged 18 to 70 over the four regions mentioned earlier, including one hundred and eleven villages. In the absence of a sampling frame and due to logistical limitations, we adopted random sampling and a multistage sampling approach. An agreement was obtained for implementing this study as a public health exercise under the Ministry of Health control. The written information and the study’s objectives have been approved following their presentation to the health and administrative authorities and the chiefs of each village that was visited in each region. In each town, individuals were counted, and their households were numbered. The villages were randomly and blindly chosen by drawing a paper with the number of studied families. Only people aged between 18 and 70 years were recruited after signing an informed consent form.
Blood collection
After acceptance, the selected individuals were given a questionnaire. Whole blood was collected into two 7 ml Vacutainer tubes containing EDTA by venipuncture at the elbow level. A laboratory unit was set up in each village’s healthcare facility. The samples were then processed according to a predefined protocol, including centrifugation at 1800 rpm for 10 min and transfer into Nunc cryotubes as follows: 5 aliquots of 1.5 ml of plasma, 1 aliquot of buffy coat, 1 aliquot of total blood pellet. These aliquots were preserved in a -20°C freezer.
At the end of each blood collection session, all the samples were transported in ice packs, then stored in a -80°C freezer at CIRMF until the analyses.
Measurement of specific IgG and IgM against T. gondii
The assay principle associates the immunoenzymatic method by immunocapture with a final fluorescence detection. IgG antibody titer was measured from 100 µl of plasma or serum using the ELFA-TOXO IgG II operated on an immunoanalyser (VIDASR) according to the manufacturer’s instructions (BiomerieuxR). Samples with titer ≥ 8 IU/ml were considered positive. Those with IgG concentration ≥ 300 IU/ml were assayed again after dilution to ¼ in a negative serum (vidas test kit).
For I gM, 10 µl of plasma or serum was used in an ELFA-TOXO IgM technique, which used an immunocomplex of T. gondii antigen coupled to a monoclonal antibody (vidas test kit). The reagents were used according to the manufacturer’s instructions (BiomerieuxR). Samples were considered positive when the value of the titer was ≥ 0.65 IU/ml.
DNA extraction and polymerase chain reaction
The genomic DNA was extracted from the buffy coats of the samples having an IgG titer ≥ 300 IU/ml (Brenier-Pinchart et al., 2015). Briefly, buffy coats were digested at equal volumes in a lysis buffer containing 0.3 mg/ml of proteinase K. After 3 h of incubation at 65°C, the DNA was extracted with phenol-chloroform. The aqueous phase of the extract was precipitated in two volumes of 100% ethanol and 3 M sodium acetate (0.1 volume) at -20°C for 1 h. The DNA pellet was then washed with 70% ethanol to remove salts. The DNA pellet was dried at room temperature, taken up in PPI water, and kept at -20°C until use.
From the extracted DNA, PCR was performed using the forward B22 (AAC GGG CGA GTA GCA CCT GAG GAG A) and the reverse B23 (TGG GTC TAC GTC GAT GGC ATG ACA AC) primers (Bretagne et al., 1993)targeting a fragment of 115 bp of B1 gene of T. gondii. The conventional PCR reaction was carried out in a final volume of 50 μl containing 0.5 μl of Taq Polymerase, 1 μl of each primer, 2.5 μl of each dNTP, 2.5 μl of PCR buffer (Buffer 10X), 5 μl of template DNA and 30 μl of ddH2O. For the PCR, the reaction consisted of initial denaturation of 95°C for 5 min, followed by 45 cycles of 95°C for 1 min, 55°C for 2 min, and 72°C for 2 min, and a final elongation at 72°C for 10 min. T. gondii DNA, as the positive control, and double-distilled water (DDW) instead of template DNA, as the negative control, were included in each experiment run. After staining with GelRed nucleic acid gel stain, PCR products were electrophoresed on a 3% agarose gel. The amplicons were visualized under UV illumination (Biorad).
Statistical analysis
Statistical analysis was performed using the Minitab program (Minitab Inc., State College, PA, USA) for Pearson’s Chi-squared test with Yates’ continuity correction. The differences between the two groups of samples were analyzed statistically using the Chi-square test. A p-value of ≤0.05 was considered significant.
RESULTS
Socio-demographic characteristics
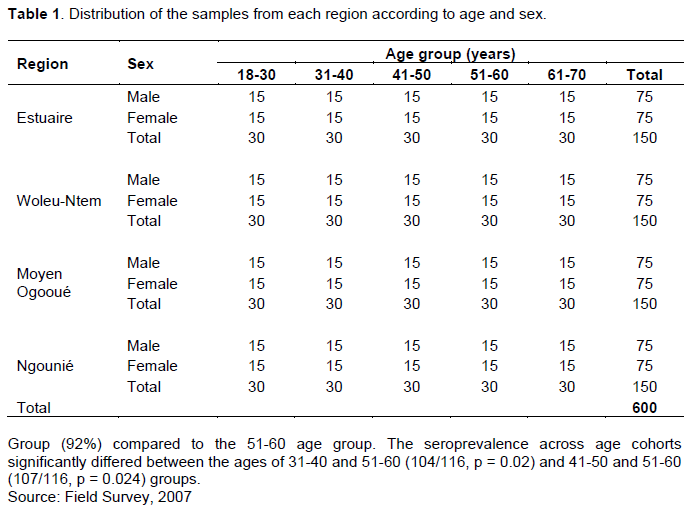
The socio-demographic characteristics of the study population are presented in Table 1. In total, 600 individuals from 18 to 70 years were recruited from 111 villages. This population included 300 women and 300 men.
Overall anti-T. gondii IgG and IgM seroprevalence
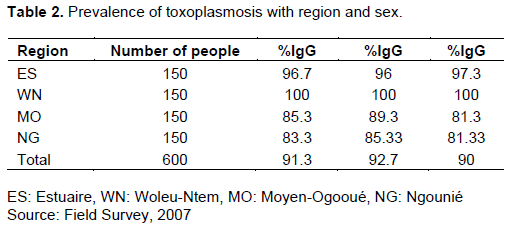
Serological tests revealed the presence of T. gondii-specific antibodies (IgG) in 91.3% of individuals (548/600). Among these individuals, 2% had anti-toxoplasmic IgM antibodies. The anti-T. gondii IgG seroprevalence was higher in men (92.7%) than in women (90%) (Table 2), but this difference was not statistically significant (p = 0.175).
Effect of geographic area and sex
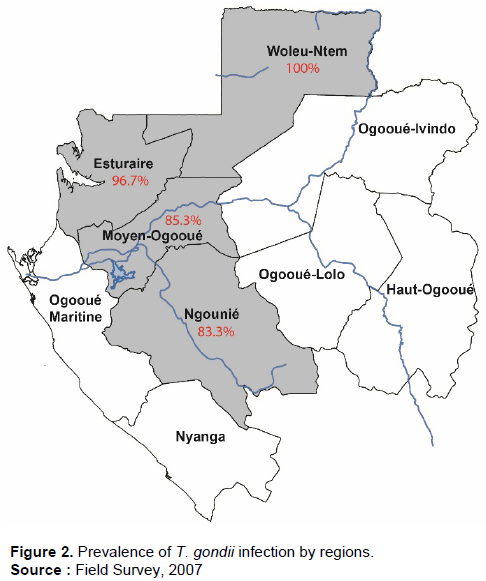
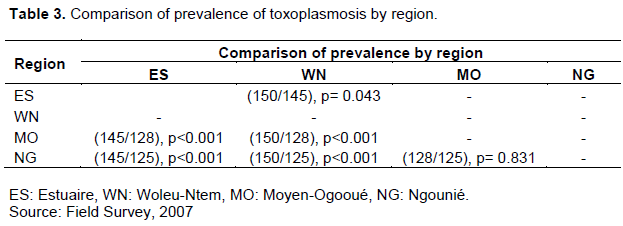
The overall prevalence within the geographic areas is presented in Figure 2. The Woleu-Ntem region recorded a higher seroprevalence than the other three regions, followed by the Estuaire region. A seroprevalence of 100% was recorded in Woleu-Ntem, 96.7% in Estuaire, 89.3% in Moyen-Ogooué, and 81.3% in Ngounié. As presented in Table 3, comparisons show a higher prevalence in Woleu-Ntem than in the three other regions (Estuaire, Moyen-Ogooué, Ngounié) (p=0.043, p<0.001, p<0.001, respectively), also between Estuaire and the two different regions (Moyen-Ogooué and Ngounié) (p<0.001, p<0.001, respectively). But there was no significant difference between Moyen-Ogooué and Ngounié regions (p=0.831). The observed differences were not linked to sex, regardless of the region.
Effect of age
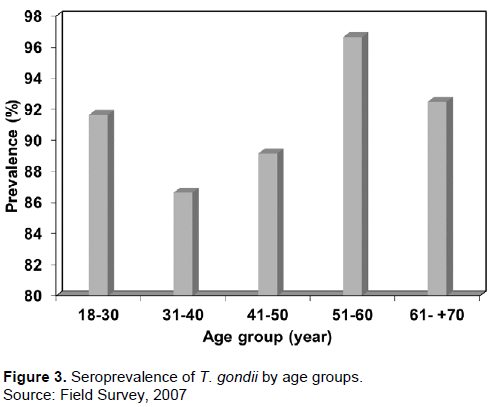
The study population was grouped without regard to sex and divided into increasing age groups of 10 years (Figure 3). The seroprevalences observed within these age groups were compared with each other. It was high between 18 and 30 years old (91%). It decreased slightly in the 31 to 40 years (86%) and 41 to 50 (89%) age groups. It was very high in the 51-60 age group, with 96%. It decreased again in the 61-70 age group (92%) compared to the 51-60 age group. The seroprevalence across age cohorts significantly differed between the ages of 31-40 and 51-60 (104/116, p = 0.02) and 41-50 and 51-60 (107/116, p = 0.024) groups.
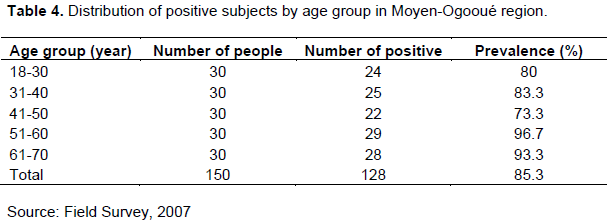
These differences were insignificant when the population was grouped according to geographic area and age group in Estuaire, Woleu-Ntem, and Ngounié regions. On the other hand, we observed significant differences with age in the Moyen-Ogooué, with an increase in seroprevalence up to the 51-60 age group followed by a plateau at 61-70 years. In the Moyen-Ogooué (Table 4), there was a significant difference between the age groups of 18-30 and 41-50 years (24/22; p = 0.044), between 41-50 and 51-60 (22/29; p = 0.011), and between 41-50 and 61-70 (22/28; p=0.013), irrespective of the sex.
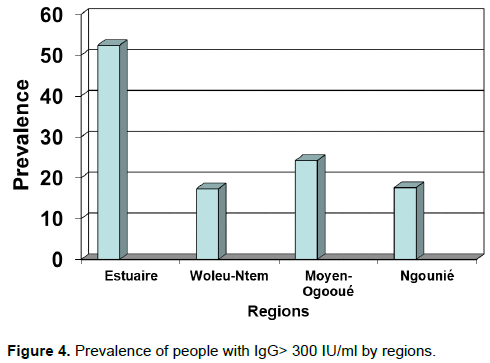
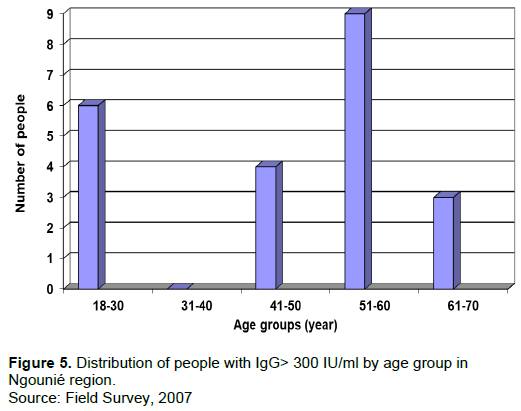
Distribution of high IgG titer
In the present study, individuals with IgG titers≥ 300 IU/ml were considered to have a very high titer. Such individuals were detected in the present study population. It appeared that out of the 548 positive individuals for IgG anti-T. gondii, 155 had a high IgG titer (28%). The distribution of these individuals according to geographic areas (Figure 4) shows that their number was higher in the Estuaire region, followed by the Moyen-Ogooué region. Thus, there were 76 individuals in Estuaire, 31 in Moyen-Ogooué, 26 in Woleu-Ntem, and 22 in Ngounié. These differences in IgG titer between regions were statistically higher in Estuaire (the coastal area) compared to Woleu-Ntem (p <0.001), Moyen-Ogooué (p <0.001), and Ngounié (p <0.001). No statistically significant difference was recorded between the three other regions, Woleu-Ntem, Moyen-Ogooué, and Ngounié.
Sex and age did not influence the rise in IgG titer, except in the ??Ngounié region (Figure 5). In this region, there were statistically significant differences in IgG titer with age in individuals between 18-30 and 31-40 (p = 0.021), 31-40 and 41-50 (p = 0.050), and 31-40 and 51-60 (p = 0.003). When the data was split by sex, there were no statistically significant differences according to age group in males. However, there were statistically significant differences among age cohorts in females: 18-30 and 51-60 (p = 0.039) and 31-40 and 51-60 (p = 0.004).
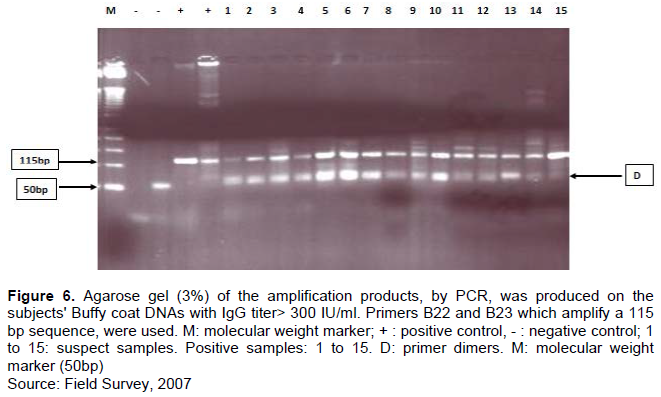
Molecular detection of parasitic DNA by PCR
The high level of IgG titer in the absence of IgM poses the problem of the presence or absence of the parasite in individuals diagnosed serologically. For molecular detection, only samples from individuals with IgG titers> 300 IU/ml were used to study the high IgG titer in the absence of IgM in specific individuals. The analysis showed that out of the 73 individuals tested for molecular detection, 49 were positive and characterized by an amplicon of 115 bp typical of the PCR product of the B1 gene of T. gondii (67.1%) (Figure 6).
DISCUSSION
T. gondii is a ubiquitous parasite. Its medical importance is increasing in Gabon because of the increase in at-risk populations (pregnant women and immunocompromised subjects) (Caron et al., 2008; Liégeois et al., 2012; Mintsa-Ndong et al., 2009).
Previous studies on toxoplasmosis in Gabon have shown the high prevalence of this parasite. Beauvais (1978) found a seroprevalence of 52.6% in the south-east of the country, and another study in the country’s urban centers showed a prevalence of 63% (Duong et al., 1992b). Studies dating from 1998 showed a prevalence of 71.2% among pregnant women (Nabias et al., 1998). In contrast, a recent study found a prevalence of 80.41% in pregnant women attending health centers in Koula-Moutou, east-central of Gabon (Ndong Mba et al., 2022). Since then, the only known study which assessed the toxoplasmosis situation in the general population living in rural areas is the work conducted by Bisvigou et al. (2009) in a rural population in south-east Gabon, which found a seroprevalence of 75.5% (Bisvigou et al., 2009).
However, all these studies were only serological, without any molecular aspect concerning the strains circulating within human populations. It is known that clinical murine toxoplasmosis manifestation is related to the strain. Although the type II genotype has been generally detected in humans, not all circulating strains and their relationship to clinical expression are known in humans (Dardé et al., 1992). This justifies our study based on the rural population and the use of molecular detection of T. gondii in human peripheral blood.
In Gabon, no study on the molecular aspect has been conducted in human populations, hence the lack of knowledge on the strains that affect local people. To initiate such an approach, we selected the study sites covering the regions of Estuaire on the coast, Woleu-Ntem in the north, Moyen-Ogooué in the center, and Ngounié in the south. Estuaire region is in contact with the West and the other continents, mainly via the port of Owendo and Libreville international airport, creating possibilities for the exchange or transfer of T. gondii’s strains. This also applies to the northern part of the country, where people trade with the rest of the continent. It should be added that the populations mix indigenous and foreign in these two regions. On the other hand, in the other two regions (Moyen-Ogooué and Ngounié), the population is poorly mixed but living in different environments; the forest for the central and the savannah for the southern parts of Gabon. The present study's environmental and socio-demographic aspects helped strengthen the analyses.
The choice of our method consists of studying the prevalence of toxoplasmosis in the rural human population and trying to understand the meaning of high levels of IgG titer in the absence of IgM in apparently healthy individuals to determine what relationship exists between this serological status and the presence or absence of the parasite in peripheral blood. However, studies in Gabon focused on humans, primarily pregnant women, were only based on IgG/IgM serology and found a high prevalence of T. gondii. Also, the strains circulating have never been studied in humans. Serological techniques have been used, without revealing the presence of the parasite but rather the contact between the parasite and humans. We used PCR to identify the parasite by looking for its DNA. It has been reported that using PCR in immunocompromised individuals and animals has made it possible to isolate DNA to characterize strains of T. gondii by using the PCR-RFLP technique (Ajzenberg et al., 2004; Dong et al., 2019; Dubey et al., 2003).
Toxoplasmosis is highly prevalent in Gabon. As in previous studies on pregnant women or the general population, we found a very high prevalence: 91.3%. This prevalence rate is higher than those previously found. The difference observed could be explained by the type of target population (rural population) and the choice of serological screening techniques.
The results of the present study show variation in prevalence depending on the geographic area. For Woleu-Ntem, the results are similar to those obtained 20 years ago by Duong et al. (1992a). On the other hand, the comparison remains challenging with the rest of the regions insofar as the urban centers were mainly examined by previous studies, unlike this study. It also appears that seroprevalence is higher in Woleu-Ntem (north) than in the other regions, followed by Estuaire (the coastal area). Sex does not seem to influence this distribution. Infection prevalence is almost the same for both sexes: 92.7% in men and 90% in women (p= 0.175). This observation is similar to that of Duong et al. (1992a).
Serological prevalence differed across the age cohorts of the study population. It was observed that regardless of sex, the seroprevalence was higher in individuals between 51 and 60 years than in the other age groups. This age difference in seroprevalence could be related to socio-cultural habits linked to age. Indeed, between 31 and 50 years old, high mobility reduces exposure to the parasite. Conversely, between 50 and 70 years, there is a decrease in mobility, with people returning to the countryside, reduced hygiene, and a sustained rate of fieldwork in these individuals that predispose them to infections. The other reason for this situation could be socio-cultural activities related to sex. Indeed, cooking, cultivating, and picking are part of the current activities of women, hence more frequent contact with the soil and perhaps higher exposure to the parasite. On the other hand, hunting and cutting trees are occupations done by men, resulting in less exposure. This could explain the isolated fluctuations in seroprevalence, which seem to be linked to age or sex.
Large numbers of people with toxoplasmic antibodies are evidence of immunity in over 90% of the rural population. However, we identified a category of people with a high titer of specific IgG and, in most cases, without IgM, which could indicate an active infection. Some regions, such as Estuaire (coastal area), recorded more individuals with a high titer than others. This suggests a phenomenon related to the environment.
The existence of individuals with high anti-toxoplasmic IgG levels without IgM has been reported in other studies (Furtado et al., 2016; Morvan et al., 1999; Teixeira et al., 2013). Various explanations have been given for this phenomenon, with some saying that it is due to the reactivation of old toxoplasmosis, and others say it is due to reinfestation or serological rebound (Holliman, 1994; James et al., 1996; Morvan et al., 1999; Nigro et al., 2003; Nimri et al., 2004). All these explanations assume the presence of the parasite in the peripheral blood, but very few have shown the parasite’s existence in these individuals, and even then, only in immunosuppressed individuals (Alfonso et al., 2009; Gashout et al., 2016).
In the present study, we tried to highlight the parasite’s existence in the blood by using the buffy coat of individuals with high IgG levels. Experience has shown that 67.12% of these individuals have circulating parasitic DNA. Although the detection of T. gondii DNA using PCR has been reported several times in blood (Ho-Yen et al., 1992; Johnson et al., 1990), it should be noted that this detection is more frequent in immunocompromised subjects (Alfonso et al., 2009; Gashout et al., 2016)and those with acute toxoplasmosis (Nimri et al., 2004). This work is undoubtedly one of the first to detect as much T. gondii in the peripheral blood of asymptomatic and assumed immunocompetent subjects as in immunosuppressed individuals. However, we have no data on the health status of these individuals to exclude cases of co-infection with diseases that can lead to immunosuppression.
In all cases, the existence of T. gondii DNA in the blood of asymptomatic individuals opens the possibility of characterizing the genotypes that infect humans.
Mouse inoculation is the gold standard technique for diagnosing T. gondii parasitemia. However, it poses a logistics problem and needs to be within reach of all laboratories. Some authors have compared three methods: mouse inoculation, cell culture, and PCR (Dupouy-Camet et al., 1992; James et al., 1996). They found that mouse inoculation and PCR were more sensitive than cell culture. However, for the mouse inoculation approach to be effective, samples containing living T. gondii are required. In contrast, PCR does not require a living organism; therefore, samples conserved under field conditions are still suitable for PCR. Thus, PCR has an advantage over mice inoculation. Our samples consisted of peripheral blood, less invasive than amniotic fluid, cerebrospinal fluid, and commonly better accepted for clinical diagnosis and field studies.
It is known that T. gondii-immunocompetent individuals harbor parasite cysts in their tissue. The rupture of these cysts during immunosuppression could have fatal clinical consequences in 91% of adults with antitoxoplasmic IgG in the current context, characterized by the increase in HIV seropositive individuals. Therefore, it is necessary to impose systematic surveillance of T. gondii in this population and pregnant women through molecular diagnosis using multiple copy genes such as the B1 gene and 529 bp (Homan et al., 2000). Even in some people with HIV, the standard serological diagnosis can be negative. A complementary PCR test would allow them to rule out the possibility of toxoplasmosis.
The establishment of molecular diagnosis by PCR (conventional, nested, or qPCR) on peripheral blood combined with a meticulous selection of the specific markers of the three existing genotypes will enable the characterization of the strains of T. gondii involved in toxoplasmosis in an African setting compared to other methods that need massive logistical supports such as mouse inoculations, cell cultures, microsatellites, MRIs and scanners.
CONCLUSION
T. gondii is highly prevalent in Gabon, sometimes reaching 100% in some areas of the country. With the increase in at-risk populations, new or reinforced prevention and diagnostic measures must be considered. These measures must be feasible and practical for developing countries instead of the cumbersome, expensive, and slow methods currently recommended (MRI, CT scan in the case of cerebral toxoplasmosis, inoculation in mice with several weeks delay before the result). These methods slow down the rapid management of severe toxoplasmosis. In this sense, the results show a high prevalence of T. gondii in immunocompetent people through molecular biology (PCR) and indicate that PCR could be a feasible alternative for developing countries.
It was proposed to define specific genomic markers, use restriction enzymes and the cloning of PCR products to face the limits of our work, and further characterize the strains circulating in our country after having determined the general prevalence in the whole rural population.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors thank populations all over the four regions of Gabon who consented to participate in the study, staff of the hospitals around the study sites, who provided logistical support for the team during the fieldwork, and the government of Gabon and Total Gabon sponsors Centre Interdisciplinaire de Recherches Médicales de Franceville.
REFERENCES
|
Ajzenberg D, Bañuls AL, Su C, Dumètre A, Demar M, Carme B, Dardé ML (2004). Genetic diversity, clonality and sexuality in Toxoplasma gondii. International Journal for Parasitology 34(10):1185-1196. |
|
|
Alfonso Y, Fraga J, Fonseca C, Jiménez N, Pinillos T, Dorta-Contreras AJ, Cox R, Capó V, Pomier O, Bandera F, Ginorio D (2009). Molecular diagnosis of Toxoplasma gondii infection in cerebrospinal fluid from AIDS patients. Cerebrospinal Fluid Research 6:1-6. |
|
|
Beauvais B (1978). La toxoplasmose au Gabon oriental. Résultats d'une enquête sérologique. Le Bulletin de la Société de Pathologie Exotique 71:172-181. |
|
|
Bisvigou U, Mickoto B, Ngoubangoye B, Mayi Tsonga S, Akue JP, Nkoghe D (2009). Séroprévalence de la toxoplasmose dans une population rurale du sud-est du Gabon. Parasite 16(3):240-242. |
|
|
Botein EF, Darwish A, El-Tantawy NL, EL-baz R, Eid MI, Shaltot AM (2019). Serological and molecular screening of umbilical cord blood for Toxoplasma gondii infection. Transplant Infectious Disease 21(4):e13117. |
|
|
Brenier-Pinchart MP, Capderou E, Bertini RL, Bailly S, Fricker-Hidalgo H, Varlet-Marie E, Murat JB, Sterkers Y, Touafek F, Bastien P, Pelloux H (2015). Molecular diagnosis of toxoplasmosis: Value of the buffy coat for the detection of circulating Toxoplasma gondii. Diagnostic Microbiology and Infectious Disease 82(4):289-91. |
|
|
Bretagne S, Costa JM, Vidaud M, Nhieu JT, Van Feith JF, Costa JM, Vidaud M (1993). Detection of Toxoplasma gondii by Competitive DNA Amplification of Bronchoalveolar Lavage Samples. Journal of Infectious Diseases 168(6):1585-1588. |
|
|
Caron M, Makuwa M, Souquière S, Descamps D, Brun-Vézinet F, Kazanji M (2008). Human immunodeficiency virus type 1 seroprevalence and antiretroviral drug resistance-associated mutations in miners in Gabon, central Africa. AIDS Research and Human Retroviruses 24(9):1225-8. |
|
|
Dardé ML, Bouteille B, Pestre-Alexandre M, Darde ML (1992). Isoenzyme Analysis of 35 Toxoplasma gondii Isolates and the Biological and Epidemiological Implications. The Journal of Parasitology pp. 786-794. |
|
|
de Wit LA, Kilpatrick AM, VanWormer E, Croll DA, Tershy BR, Kim M, Shapiro K (2020). Seasonal and spatial variation in Toxoplasma gondii contamination in soil in urban public spaces in California, United States. Zoonoses Public Health 67:70-78. |
|
|
Dong H, Su R, Li T, Su C, Zhang L, Yang Y (2019). Isolation, genotyping and pathogenicity of a Toxoplasma gondii strain isolated from a Serval (Leptailurus serval) in China. Transboundary and Emerging Diseases 66(4):1796-802. |
|
|
Dubey JP (1998). Advances in the life cycle of Toxoplasma gondii. International Journal for Parasitology 28(7):1019-1024. |
|
|
Dubey JP, Graham DH, Dahl E, Hilali M, El-Ghaysh A, Sreekumar C, Kwok OCH, Shen SK, Lehmann T (2003). Isolation and molecular characterization of Toxoplasma gondii from chickens and ducks from Egypt. Veterinary Parasitology 114(2):89-95. |
|
|
Duong TH, Martz M, Rondi ML, Richard-Lenoble D, Kombila M (1992a). Toxoplasmose au Gabon: résultats d'une enquête séro-épidémiologique. Bulletin de la Société de pathologie exotique 85(5):368-373. |
|
|
Duong TH, Dufillot D, Martz M, Richard-Lenoble D, Kombila M (1992b). Etude Séro-épidémiologique de la toxoplasmose à Libreville, Gabon. InAnnales de la Societe Belge de Medecine Tropicale 72(4):289-293. |
|
|
Dupouy-Camet J, Bougnoux ME, Lavareda de Souza S, Thulliez P, Dommergues M, Mandelbrot L, Ancelle T, Tourte-Schaefer C, Benarous R (1992). Comparative value of polymerase chain reaction and conventional biological tests for the prenatal diagnosis of congenital toxoplasmosis. Annales de Biologie Clinique (Paris). |
|
|
Ebrahimzadeh A, Shahraki MK, Mohammadi A (2018). Serological and molecular diagnosis of Toxoplasma gondii in patients with schizophrenia. Journal of Parasitic Diseases 42(2):177-181. |
|
|
Farhadi A, Haniloo A, Fazaeli A, Moradian S, Farhadi M (2017). PCR-based diagnosis of Toxoplasma parasite in ocular infections having clinical indications of toxoplasmosis. Iranian Journal of Parasitology 12(1):56. |
|
|
Furtado JM, Toscano M, Castro V, Rodrigues MW (2016). Roth Spots in Ocular Toxoplasmosis. Ocular Immunology and Inflammation 24(5):568-570. |
|
|
Gashout A, Amro A, Erhuma M, Al-Dwibe H. Elmaihub E, Babba H, Nattah N, Abudher A (2016). Molecular diagnosis of Toxoplasma gondii infection in Libya. BMC Infectious Diseases 16:1-8. |
|
|
Ho-Yen DO, Joss AWL, Balfour AH, Smyth ETM, Baird D, Chatterton JMW (1992). Use of the polymerase chain reaction to detect Toxoplasma gondii in human blood samples. Journal of Clinical Pathology 45(10):910-913. |
|
|
Holliman R (1994). Recent developments in the diagnosis of toxoplasmosis. Serodiagn. Immunother. infectious Diseases 6(1):5-16. |
|
|
Homan WL, Vercammen M, De Braekeleer J, Verschueren H (2000). Identification of a 200- to 300-fold repetitive 529 bp DNA fragment in Toxoplasma gondii, and its use for diagnostic and quantitative PCR. International Journal for Parasitology 30(1):69-75. |
|
|
Howe DK, Sibley LD (1995). Toxoplasma gondii comprises three clonal lineages: Correlation of parasite genotype with human disease. The Journal of Infectious Diseases 172(6):1561-1566. |
|
|
James GS, Sintchenko VG, Dickeson DJ, Gilbert GL (1996). Comparison of cell culture, mouse inoculation, and PCR for detection of Toxoplasma gondii: Effects of storage conditions on sensitivity. Journal of Clinical Microbiology 34(6):1572-1575. |
|
|
Johnson JD, Holliman R., SAVV D (1990). Detection of Toxoplasma gondii using the polymerase chain reaction 18:989. |
|
|
Liégeois F, Vella C, Eymard-Duvernay S, Sica J, Makosso L, Mouinga-Ondémé A, Mongo AD, Boué V, Butel C, Peeters M, Gonzalez JP, Delaporte E, Rouet F (2012). Virological failure rates and HIV-1 drug resistance patterns in patients on first-line antiretroviral treatment in semirural and rural Gabon. Journal of the International AIDS Society 15(2):17985. |
|
|
Mercier A, Devillard S, Ngoubangoye B, Bonnabau H, Bañuls AL, Durand P, Salle B, Ajzenberg D, Dardé ML (2010). Additional haplogroups of Toxoplasma gondii out of Africa: Population structure and mouse-virulence of strains from Gabon. PLoS Neglected Tropical Diseases 4(11):e876. |
|
|
Mintsa-Ndong A, Caron M, Plantier JC, Makuwa M, Le Hello S, Courgnaud V, Roques P, Kazanji M (2009). High HIV type 1 prevalence and wide genetic diversity with dominance of recombinant strains but low level of antiretroviral drug-resistance mutations in untreated patients in northeast gabon, Central Africa. AIDS Research and Human Retroviruses 25(4):411-418. |
|
|
Morvan JM, Mambely R, Selekon B, C.-MM (1999). La toxoplasmose à l'Institut Pasteur de Bangui, République centrafricaine (1996-1998):données sérologiques. Le Bulletin de la Société de Pathologie Exotique 92:157-60. |
|
|
Nabias R, Ngouamizokou A, Migot-Nabias F, Mbou-Moutsimbi RA, Lansoud-Soukate J (1998). Enquête sérologique sur la toxoplasmose chez les consultantes du Centre de Prévention Maternelle et Infantile (PMI) de Franceville. Le Bulletin de la Société de Pathologie Exotique 91(4):318-320. |
|
|
Ndong MT, Mongo DA, Moudounga KH, Pambo-Pambo AB, Ibouanga BA, Sima OC, Mickala P. Seroprevalence and risks factors predicting Toxoplasma gondii (Toxoplasmosis) infection in pregnant women inKoula-Moutou and surronding departments in central eastern Gabon. Ethics, Medicine and Public health 24:100841. |
|
|
Nigro M, Gutierrez A, Hoffer AM, Clemente M, Kaufer F, Carral L, Martin V, Guarnera EA, Angel SO (2003). Evaluation of Toxoplasma gondii recombinant proteins for the diagnosis of recently acquired toxoplasmosis by an immunoglobulin G analysis. Diagnostic Microbiology and Infectious Disease 47(4):609-613. |
|
|
Nimri L, Pelloux H, Elkhatib L (2004). Detection of Toxoplasma gondii DNA and specific antibodies in high-risk pregnant women. The American Journal of Tropical Medicine and Hygiene 71(6):831-835. |
|
|
Pleyer U, Groß U, Schlüter D, Wilking H, Seeber F (2019). Toxoplasmosis in Germany-epidemiology, diagnosis, risk factors, and treatment. Deutsches Ärzteblatt International 116(25):435. |
|
|
Teixeira LE, Kanunfre KA, Shimokawa PT, Targa LS, Rodrigues JC, Domingues W, Yamamoto L, Okay TS (2013). The performance of four molecular methods for the laboratory diagnosis of congenital toxoplasmosis in amniotic fluid samples. Revista da Sociedade Brasileira de Medicina Tropical 46:584-588. |
|
|
Tenter AM, Heckeroth AR, Weiss LM (2000). Toxoplasma gondii: From animals to humans. International Journal for Parasitology 30(12-13):1217-1258. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


