Full Length Research Paper

ABSTRACT
In 2013, in Togo, the Demographic and Health Survey III estimated the proportion of low birth weight at 10%. The objective of this study was to determine the factors associated with low birth weight in Togo. We conducted a case-control study on newborn records from Tchamba Hospital from 2014 to 2016. Cases were newborns with birth weight strictly below 2500 g whereas controls were those with a weight greater than or equal to 2500 g. There was one case for every two controls. Odd ratios were estimated using a multivariate logistic regression analysis. The sample consisted of 305 cases and 610 controls. Factors associated with low birth weight were gestational age less than 37 weeks (OR = 62.60, 95%CI [24.51 - 159.87], p ï‚£ 0.0001), maternal age below 18 years (OR = 2.41, 95%CI [1.11 - 5.22], p = 0.026), non-use of long-lasting treated mosquito nets (OR = 5.3, 95%CI [3.42 - 8.18], p ≤ 0,0001), and severe malaria during pregnancy (OR = 3.7, 95%CI [1.24 -11.04], p = 0.019). Almost all factors associated with low birth weight identified could be modified. We recommend raising awareness about the risk factors of low birth weight and malaria prevention.
Key words: Associated factors, low birth weight, newborn, Tchamba, Togo
INTRODUCTION
Low birth weight (LBW) is a major public health problem in both developing and developed countries. In Africa, between 1998 and 2008, the prevalence of LBW varied from 7 to 17% depending on the study areas and periods (Malaba et al., 2005; Roberfroid et al., 2008; Schmiegelow et al., 2012). In Togo, LBW in 2008 represented 6.8% of all live births, with a neonatal mortality rate of 4.5 times higher than the average rate (Ministère de la Santé du Togo, 2012). According to the Togo Demographic Health Survey (DHS III) of 2013, infant/child mortality and neonatal mortality were 8.9 and 2.7%, respectively. Newborns accounted for 32.3% of deaths of children under five; 11.6% of these deaths were due to premature births and low birth weight has consequences on the physical and mental growth of the child (Meda et al., 1995). LBW newborns are exposed to homeostasis disorders and complications such as hypothermia, hypoglycemia and hypocalcemia.
Low birth weight is a multifactorial health problem affecting a vulnerable population and can be prevented through targeted interventions that focus on modifiable factors that have been proven effective in several countries around the world (Rajaratnam et al., 2010; Oestergaard et al., 2011).
In rural Burkina Faso, the prevalence of LBW remained stable between 2004 and 2006 at between 17 and 16%. In Tanzania, prevalence increased from 10% in 1998 to 11% in 2008. Low age of mother, premature birth, and a history of severe malaria during pregnancy)are found to be associated with LBW (Institute of Medicine, 1985; Letaief et al., 2001; Balaka et al., 2002; March of Dimes, 2004; Mabiala-Babela et al., 2007; Beddek and Demmouche, 2013; Kangulu et al., 2014; Feresu et al., 2015). Togo DHS III report found a prevalence of LBW of 10% (Ministère de la Planification, du Développement et de l’Aménagement du Territoire du Togo, 2014). These figures were certainly underestimated, considering the fact that in many developing countries, there are still large numbers of home births that are not covered by national statistics.
Some studies have been conducted in Togo on this topic, but they have been essentially descriptive, carried out at the University Hospital Centers of Lomé and Kara (unpublished data).
In view of these observations, it appeared necessary to conduct an analytical study in the periphery of a district hospital to deepen and document the factors associated with LBW, in order to strengthen and better target health interventions based on the country context and to determine the factors associated with low birth weight at the Tchamba District Hospital (DH) in Togo from 2014 to 2016.
METHODS
Study area and design
The study area includes all live births registered at the maternity ward of the Tchamba District Hospital from January 1st, 2014 to December 31st, 2016 while the case-control study conducted comprised from February 1st to April 30th, 2017.
Sample size determination
One case was considered for two unmatched controls. The size of our sample was calculated using Open Epi software. For a bilateral confidence level of 95%, a power of 80% and a rib ratio of 1.5 were used according to Fleiss with continuity correction. The sample consisted of 305 cases and 610 controls.
Sampling techniques
Cases were recruited using systematic sampling at the MU of Tchamba DH by reviewing birth records that took place from January 1st, 2014 to December 31st, 2016 from a list of 337 cases. Controls were recruited from the same Tchamba DH birth register as the cases. These were the two newborns according to the case identified on the list in the birth register. In situation where two cases followed each other in the register, it was considered among the normal newborns according to the second case, the controls of these cases by taking them consecutively 2 by 2 for the first and second cases respectively.
Technical tools and data collection
The data collected included characteristics of the newborn and the socio-demographic, clinical and obstetrical characteristics of the child's mother. A literature review was conducted using birth registers, prenatal consultation registers, prenatal consultation cards and parturient files. An extraction sheet was developed and completed using data recorded in the case and control data sources.
Statistical analysis
In descriptive analysis, the proportions were estimated and tested using a chi-squared (χ²) test. Means and standard deviations were calculated to describe the sociodemographic characteristics of babies and the obstetric history of their mothers. A univariate logistic regression was used to select variables with a p-value of <0.20 for inclusion in the baseline model in multivariate analysis. In a top-down multivariate logistic regression model, we calculated the adjusted ORs (ORa) that were tested by the χ² test to identify factors associated with LBW at a 95% confidence interval (CI). We used the p < 0.05 as the significance threshold.
RESULTS
Socio-demographic and clinical characteristics of the sample
From January 2014 to December 2016, Tchamba District Hospital recorded a total of 337 LBW newborns out of 3151 deliveries. Female to Male (F/M) ratio for the entire sample was 0.9; this sex ratio was 1 for cases and 0.8 for controls (p = 0.02). For all newborns, the mean gestational age (GA) was 39.17 ± 2.26 weeks of Last Menstrual Period (WLMP) ranging from 25 to 40 WLMP, with 13% having had a GA strictly below 37 weeks. The mean gestational age was statistically different between cases and controls [37.6 ± 3.3 WLMP and 40 ± 0.5 WLMP (p=0.001)], respectively.
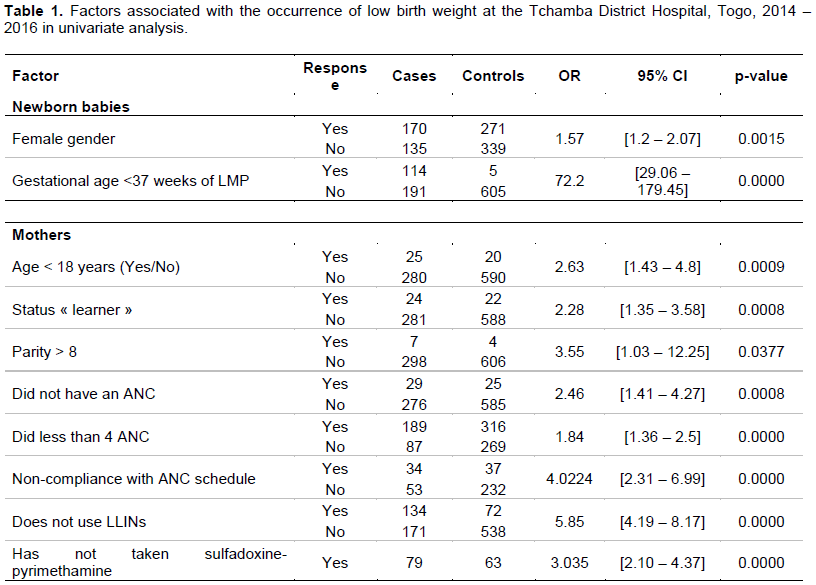
Factors associated with LBW at Tchamba District Hospital, Togo, 2014 - 2016 in bivariate analysis
In bivariate analysis (Table 1), statistically significant factors associated with LBW were gestational age < 37 weeks (OR = 72.2, 95%CI [29.06-179.45], p ≤ 0.000), female sex with (OR = 1.57, 95%CI [1.2-2.07], P = 0.001), non-use of long-lasting treated mosquito nets (LLINs) (OR=5.85, 95%CI [4.19 - 8.17], p≤ 0.001), non-compliance with the antenatal care (ANC) schedule (OR=4.02, 95%CI [2.31 - 6.99], p≤ 0.001), parity > 8 (OR=3.55, 95%CI [1.03 - 12.25], p=0.03), failure to take sulfadoxine-pyrimethamine during pregnancy (OR=3.035, 95%CI [2.10 - 4.37] and p≤ 0.001), age < 18 years with OR=2.63, 95%CI [1.43 - 4.8], p≤ 0.001, failure to use ANC with OR= 2.46, 95%CI [1.41 - 4.27], p = 0.0008, the "learner" status with OR=2.28, 95%CI [1.35 - 3.58], p=0.0008, the achievement of less than 4 CPN with OR = 1.84, 95%CI [1.36 - 2.5], p≤ 0.001.
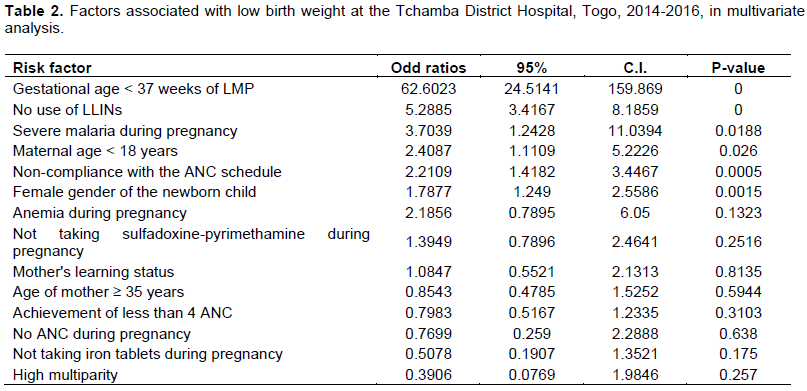
Factors associated with LBW at Tchamba District Hospital, Togo, 2014 - 2016 in multivariate analysis
In multivariate analysis (Table 2), statistically significant factors associated with LBW were gestational age < 37 weeks with OR= 62.6, 95%CI [24.51 - 159.87], p≤ 0.001, female sex of the newborn with OR=1.79, 95%CI [1.25 - 2.56], p=0.0015, non-use of LLINs with OR=5.29, 95%CI [3.41 - 8.18], p≤ 0.001, occurrence of severe malaria during pregnancy with OR=3.7, 95%CI [1.24 - 11.03], p=0.0188, age of mother < 18 years with OR=2.4, 95%CI [1.11 - 5.22], p=0.026, non-compliance with the ANC schedule with OR=2.21, 95%CI [1.42 - 3.44], p=0.0005
DISCUSSION
Gestational age < 37 weeks of LMP was associated with LBW. Similar observations had already been made in descriptive studies. Indeed, in Algeria, Fatima et al. (Beddek and Demmouche, 2013)found that the proportion of LBW infants is higher (50.90%) among mothers who had pregnancies with a gestational age of less than 37 weeks of LMP. While in the DRC, in Katanga, Ignace (Kangulu et al., 2014)found that 100% of the newborns born during pregnancy < 37 weeks of LMP were LBW. Therefore, low birth weight is thought to result either from premature birth (delivery before the 37th week of LMP) or from delayed fetal growth in children born at term (March of Dimes, 2004).
In our study, it was observed that LBW was associated with a mother age under 18 years during pregnancy. Similarly, in Togo, Balakahad already observed in 2002 that 26.5% of mothers of premature infants were under 20 years of age (Balaka et al., 2002). This result is comparable to that of Mabiala-Babela et al. (2007) in Congo Brazzaville, who concluded that the mother's age < 18 years was a factor in LBW. Similar factor was identified in Tunisia in the Monastir region with a relatively weaker association (OR=1.14) (Letaief et al., 2001); whereas it was 7.62 in Katanga in the DRC (Kangulu et al., 2014). These differences could be related to the difference in sampling technique, as the Tunisian study only considered newborns from single and normal pregnancies with matching of gestational age and date of birth.
Mothers under 18 years of age are still teenagers who have not yet completed their own growth, and are therefore more likely to give birth to low birth weight children than older mothers with the same nutritional status (Kurz and Johnson-Welch, 1994). Competition between pregnancy and growth has a particularly negative effect on the micronutrient status of adolescent girls (Scholl et al., 1990). These teenage mothers often have other factors that increase the risk of childbirth for low birth weight, black race, low socio-economic status, small height, low education, lack of or inadequate prenatal health care (Institute of Medicine, 1985). It seems increasingly clear that age is a social risk factor and not a biological factor, except in very young adolescent girls (Hediger et al., 1997).
According to our results, LBW was observed almost twice as much in female newborns. This finding is consistent with (Letaief et al., 2001)who found that female gender was significantly associated with the occurrence of low birth weight (Letaief et al., 2001). A history of mother severe malaria during pregnancy was associated with LBW. This observation was seen in Zimbabwe that malaria increased the risk of LBW by 1.89 times (Feresu et al., 2015). Malarial infection during pregnancy is a major public health problem occurring in all tropical and subtropical regions (Feresu et al., 2015).
Our results showed that LBW was associated with a non-use of LLINs during pregnancy. Indeed, sleeping under a long-lasting insecticide-treated mosquito net is one of the three recommended approaches to prevent malaria and reduce its incidence in pregnant women; the other two are intermittent preventive treatment and management of malaria cases in pregnant women. A study of a high transmission area in Kenya found that women who sleep under an insecticide-treated mosquito net every night during their first four pregnancies had four times fewer premature or low birth weight children (ter Kuile et al., 2003).
Non-compliance with the ANC schedule was found to be a factor associated with the occurrence of LBW. Twice as many LBW newborns were found among mothers who did not follow the LBW schedule as among those who did. In Togo, lower risk maternity guidelines require that pregnant women be followed for prenatal consultations at least 4 times before giving birth. At each consultation, an appointment is given to the women for the next consultation, in accordance with these different periods, but this schedule is not always respected by pregnant women.
Non-compliance with ANC schedule was also reported by several authors as being associated with the occurrence of LBW (Letaief et al., 2001; Rakotozanany et al., 2004; Kangulu et al., 2014). Letaief et al. (2001).noted the same level of association as our results, but not statistically significant (2.5 with p= 0.058). Ignace in the DRC, a stronger association was found (OR twice that measured in our study) (Kangulu et al., 2014). ANC is prenatal surveillance to prevent several diseases responsible for low birth weight (malaria, intestinal helminthiasis, anemia). Women who did not follow the ANC schedule may have insidiously allowed factors that would have caused weight deficit to develop and could have been detected and managed to prevent this weight deficit from occurring. This is true since it is estimated that in Africa, two thirds of low birth weight cases are attributable to intrauterine growth retardation (Ezeaka et al., 2003).
CONCLUSION
Factors associated with LBW identified are socio-demographic (gestational age < 37 weeks of LMP, maternal age < 18 years and female sex of the newborn), and clinical (non-use of LLINs, non-compliance with the ANC schedule and severe malaria during pregnancy), almost all of which could be modified. We recommend raising awareness about the risk factors of LBW and malaria prevention.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Balaka B, Baeta S, Agbéré AD, Boko K, Kessie K, Assimadi K (2002). Facteurs de risque associés à la prématurité au CHU de Lomé, Togo. Bulletin de la Société de Pathologie Exotique 95(4):280-283. |
|
|
Beddek F, Demmouche A (2013). Facteurs relatifs au faible poids de naissance à l'EHS En Gynécologie Obstétrique de Sidi Bel Abbes (Ouest de L'Algérie). Pan African Medical Journal 16: |
|
|
Ezeaka VC, Egri-Okwaji MT, Renner JK, Grange AO (2003). Anthropometric measurements in the detection of low birth weight infants in Lagos. The Nigerian Postgraduate Medical Journal 10(3):168-172. |
|
|
Feresu SA, Harlow SD, Woelk GB (2015). Risk Factors for Low Birthweight in Zimbabwean Women: A Secondary Data Analysis. PLoS ONE 10:e0129705. |
|
|
Hediger ML, Scholl TO, Schall JI, Krueger PM (1997). Young maternal age and preterm labor. Annals of Epidemiology 7(6)400-406. |
|
|
Institute of Medicine (1985). Preventing Low Birthweight. Washington, DC: The National Academies Press. |
|
|
Kangulu IB, Umba EKN, Nzaji MK, Kayamba PKM (2014). Facteurs de risque de faible poids de naissance en milieu semi-rural de Kamina, République Démocratique du Congo. The Pan African Medical Journal 17. |
|
|
Kurz KM, Johnson-Welch C (1994) The nutrition and lives of adolescents in developing countries: findings from the Nutrition of Adole ... | POPLINE.org. |
|
|
Letaief M, Soltani MS, Salem KB,Bchir MA (2001). Epidemiology of low birth weight in the Tunisian Sahel. Public Health 13(4):359-366. |
|
|
Mabiala-Babela JR, Matingou VC, Senga P (2007). Risk factors for low birth weight in Brazzaville, Congo. Journal De Gynecologie, Obstetrique Et Biologie De La Reproduction 36(8):795-798. |
|
|
Malaba LC, Iliff PJ, Nathoo KJ, Marinda E, Moulton L H, Zijenah LS,Humphrey JH (2005).Effect of postpartum maternal or neonatal vitamin A supplementation on infant mortality among infants born to HIV-negative mothers in Zimbabwe. The American Journal of Clinical Nutrition 81(2):454-460. |
|
|
March of Dimes (2004) Low birthweight. |
|
|
Meda N, Soula G, Dabis F, Cousens S, Some A, Mertens T, Salamon R (1995). Risk factors in prematurity and intrauterine growth retardation in Burkina Faso. Revue D'epidemiologie et de Sante Publique 43(3):215-224. |
|
|
Ministère de la Planification, du développement et de l'Aménagement du territoire du Togo (2014). Rapport de l'Enquête Démographique et de Santé Togo 2013. |
|
|
Ministère de la Santé du Togo (2012). Plan National De Developpement Sanitaire Du Togo 2012-2015 |
|
|
Oestergaard MZ, Inoue M, Yoshida S, Mahanani WR, Gore FM, Cousens S, Lawn JE, Mathers CD (2011). Neonatal mortality levels for 193 countries in 2009 with trends since 1990: A systematic analysis of progress, projections, and priorities. PLoS Medicine 8:e1001080. |
|
|
Rajaratnam JK, Marcus JR, Flaxman AD, Wang H, Levin-Rector A, Dwyer L, Murray CJ (2010). Neonatal postneonatal, childhood, and under-5 mortality for 187 countries, 1970-2010: a systematic analysis of progress towards Millennium Development Goal 4. The Lancet 375(9730):1988-2008. |
|
|
Rakotozanany LE, Rabarijaona LP, Rakotomanga JDM (2004) Facteurs relatifs au faible poids de naissance au CHUA gynécologie obstétrique de Befelatanana. In: Scribd. |
|
|
Roberfroid D, Huybregts L, Lanou H, Henry MC, Meda N, Menten J (2008).Effects of maternal multiple micronutrient supplementation on fetal growth: a double-blind randomized controlled trial in rural Burkina Faso. The American Journal of Clinical Nutrition 88(5):1330-1340. |
|
|
Schmiegelow C, Minja D, Oesterholt M, Pehrson C, Suhrs HE, Boström S, Theander TG (2012).Factors associated with and causes of perinatal mortality in northeastern Tanzania. Acta Obstetricia et Gynecologica Scandinavica 91(9):1061-1068. |
|
|
Scholl TO, Hediger ML, Ances IG, Belsky DH,Salmon RW (1990). Weight gain during pregnancy in adolescence: predictive ability of early weight gain. Obstetrics and Gynecology 75(6):948-953. |
|
|
ter Kuile FO, Terlouw DJ, Phillips-Howard PA, Hawley WA, Friedman JF, Kolczak MS, Nahlen BL(2003).Impact of permethrin-treated bed nets on malaria and all-cause morbidity in young children in an area of intense perennial malaria transmission in western Kenya: cross-sectional survey. The American Journal of Tropical Medicine and Hygiene 68(4_suppl):100-107. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


