Full Length Research Paper

ABSTRACT
Knowledge and practices in preventing malaria infection were assessed in a cross-sectional study in Morogoro Municipal. Malaria is a life-threatening parasitic disease transmitted caused by plasmodial species which are plasmodium falciparum, plasmodium vivax, plasmodium ovale, and plasmodium malariae. With most of the cases of malaria being due to Plasmodium falciparum accounting for more than 95% of infections. A total of sixty families were randomly selected from five study areas (Chamwino, Mafiga, Kichangani, Misufini and Manzese) to participate in the study. The questionnaire consisting of closed and open-ended questions was administered. The results indicated that knowledge on malaria transmission and prevention was reasonable as the respondents declared to have a significant knowledge (85%) on malaria transmission and prevention, though there was a knowledge gap among respondents. Breeding sites were also assessed and the results showed that 26.7% reported dark places as breeding sites, 40% mentioned the edges of ponds and stagnant water, 26.7% tagged dirty areas as breeding sites, 1.7% mentioned cattle sheds, and 5% were not aware at all. Methods used for management of malaria in their homes indicate that most of the respondents (73.3%) agreed with indoor residual spraying (IRS) while (26.7%) did not agree with IRS. Most respondents commented on the effectiveness of Home Management of Malaria (HMM) to be somehow helpful in reducing malaria infection cases, while 31.7% strongly agreed that HMM has been effective in reducing malaria infection cases. Therefore, there is a need to improve the emphasis of HMM to ensure that the effectiveness of HMM is being achieved at a great level.
Key words: Knowledge, mosquito, indoor residual spraying, home management of malaria.
INTRODUCTION
Malaria is a life-threatening parasitic disease transmitted through the bite of an infected female anopheles mosquito. It is caused by plasmodial species which are plasmodium falciparum, plasmodium vivax, plasmodium ovale and plasmodium malariae. Approximately 93% of the continental people live in areas where malaria is spread for at least 1 month per year. Though Tanzania has been promoting the use of long-lasting insecticide-treated nets (LLINs), there are still between 60,000 and 80,000 malaria attributable deaths per year, primarily children under the age of 5 years and pregnant women (Ministry of Health, 2015). The extent of the disease is deeper where knowledge and awareness of malaria and its vectors, health infrastructure, and human resources for health are poor (Measure DHS Project, 2011; Mboera et al., 2015). Most of the cases of malaria are due to Plasmodium falciparum accounting for more than 95% of infectious and this species is responsible for the severe form of the disease that may lead to death (Killeen et al., 2013). According to Chukwuocha et al. (2009), malaria is among the cause of childhood mortality in most countries. The infections for malaria can be either symptomatic or asymptomatic as an individual can be suspected to have been infected with malaria but without showing symptoms, thus effective management for malaria should be accompanied by several diagnostic tests. Home Management of Malaria (HMM) is one of the key strategies to reduce the burden of malaria in Morogoro Municipal. HMM is a national policy that is being implemented throughout the country, including the Morogoro region (Daniel and Sigsbert, 2017).
Vector control is the main component of the global strategy for malaria control which targets averting parasite transmission mainly through interventions targeting adult Anopheles mosquitoes by protecting individuals who sleep or rest indoors (Killeen et al., 2013). Pyrethroids in LLINs and indoor residual spray (IRS) use have improved dramatically and turned into being the cornerstone of malaria control programs (Moonen et al., 2010). Presently, the Ministry of Health and Social Welfare highlights a scale-up of insecticide-treated net dissemination programs under the Roll Back Malaria initiative (Partnership Roll Back Malaria, 2005). To accomplish this, the country embarked on nationwide free distribution of LLINs to ensure that every household owned treated bed nets (Partnership Roll Back Malaria, 2005 and Moonen et al., 2010). HMM was selected to be done on these areas because there are standing water bodies created by rainfall which provide breeding grounds for malaria-carrying mosquitoes. HMM is a key strategy to reduce the burden of malaria for vulnerable populations in endemic cities (WHO, 2005), and it has been adopted by the WHO as a cornerstone of malaria control. Moreover, most of the people who have been affected are those staying in families who do not take preventive measures. The strategy for HMM also aims to improve the ineffective self-medication practices that is very common among most people in their families.
The HMM strategy empowers communities to respond to malaria using effective, good-quality antimalarial medicines through community involvement (WHO, 2009).
The Roll Back malaria has defined the HMM as an integral part of an overall malaria case management strategy aiming to improve access to treatment for malaria in areas with limited access to health facilities. As in Morogoro Municipal, some areas are quietly difficult to access competent health services as a result the practices for home management of some diseases including malaria is necessary. So far HMM is being promoted with artemisinin-based combination therapy (ACT). Conrad and Rosenthal (2019) indicated that based on different studies conducted in Africa ACT has shown excellent treatment efficacy. The need to reduce malaria morbidity and mortality through the improvement of home management for malaria is thus of crucial importance as it will lead to a number of community-based initiatives including training of mothers, community health workers, and appropriate anti-malarial use (Oreagba et al., 2004). Since preventive measures for malaria are never 100% effective in most families, this has made the transmission of malaria persist for several years in cities.
This study intends to assess public knowledge on malaria together with the practice on home management of malaria among selected families in Morogoro Municipality. Understanding the knowledge and practice of malaria will assist communities in fighting against malaria.
MATERIALS AND METHODS
A random sampling procedure was used to select the areas and 60 families were selected for this study. The areas selected were Chamwino, Mafiga, Kichangani, Misufini and Manzese. These areas were selected because there are standing water bodies created by rainfall which provide breeding grounds for malaria-carrying mosquitoes. Data were collected using a structured, questionnaire which was in Kiswahili translated from the English version. The questionnaire consisted of closed and open-ended questions. For each selected household, the head or second-in-charge was selected to fill out the questionnaire. The questionnaire was divided into two parts which were knowledge and practices. The questionnaires contained multiple-choice questions, and some consisted of two optional answers “yes” or “no”. The questionnaires were developed on the basis of guidelines and in regard to adaptations from previous literature studies.
Data processing and analysis
Data collected were coded and entered into Excel, then plugged into Epi Info 7 ready for data analysis. All questions on knowledge of mosquitoes and malaria and awareness of changed biting behavior of mosquito were scored with one mark for the correct answer, so as to categorize participants with ‘good knowledge’ zero was given for incorrect answers, and those participants giving incorrect answers were categorized as having ‘poor knowledge’.
Ethical consideration
Ethical clearance for the studies was granted by the Sokoine University of Agriculture (SUA).
RESULTS
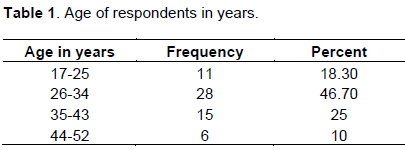
A total of 60 participants were involved in the study in which 21/60 (35%) were males and 39/60 (65%) were females. Out of this, 86% were married; while the rest (14%) were not married. Table 1 shows the range of ages of respondents who were involved in the study. As 18.3% ranged in age, between 17 and 25, 46.7% ranged in years between 26 and 34, 25% were in the age between 35 and 43 and 10% ranged in years between 44 and 52.
Perception about the concept of malaria
About 20% had good knowledge about malaria, 53.3% had medium knowledge, 16.7% had poor knowledge and 10% had very poor knowledge of malaria at all. The respondents of the age between 17 and 25 seemed to have more knowledge followed by the age between 26 and 34. This is perhaps because most of the respondents in these two age groups were students and some were current graduates from school. On the course of Malaria, 85% had a right perception that malaria is an illness caused by mosquito bites, while about 8.3% perceived that malaria is an illness due to spiritual problems, and the remaining 6.7%, knew nothing about the cause of Malaria.
Response on the breeding factors of mosquitoes
The 26.7% mentioned dark places as the breeding sites for mosquitoes, 40% recognized the breeding sites of mosquitoes to be on the edges of ponds and stagnant water, 26.7% mentioned dirty areas while 1.7% tagged the cattle sheds to accelerate the breeding of mosquitoes and 5% were not aware of the breeding sites of mosquitoes (Table 2).

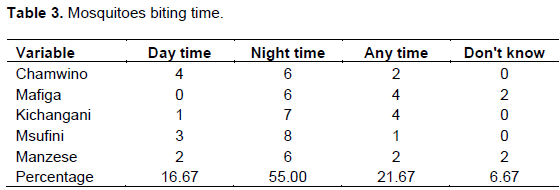
Recognition on when do mosquitoes bite
Table 3 shows how the respondents in each study area responded to the time of mosquito bites. The respondents had four options to select, of these options 16.7% selected daytime, 55% mentioned that mosquitoes do bite at night, 21.67% selected mosquitoes can bite at any time and 6.67% did not know when do mosquitoes bite.
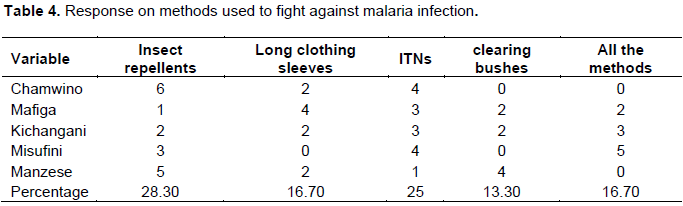
Measures are taken to control malaria
Of the five selected study areas, 28.3% chose the use of insect repellents as the method they use at their homes to manage malaria, 16.7% mentioned wearing long sleeves clothing at night, 25% used insecticidal treated nets (ITNs) as a measure to prevent a malaria infection, 13.3% reported clearing of bushes and 16.7% reported that they use all of given optional methods (Table 4).
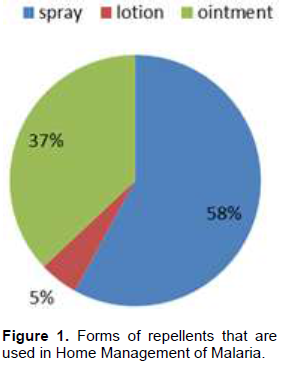
Recognition of the forms of repellents that are used in Home management of malaria
Respondents who mentioned the use of repellents were asked about the forms of repellents they use in managing malaria at their homes. Fifty-eight percent (58%) reported that they use sprays and the common spray repellent that was mentioned is Rungu. Thirty-seven percent (37%) mentioned ointment as the form of repellents they use and 5% (Figure 1) used repellents in lotion form, thus they are applied on the skin surface.
Frequency of the use of repellents on home management of malaria
The respondents were then asked to what extent they use repellents in controlling malaria, 15% reported that they use the repellents frequently, meaning more than thrice per week, 30% reported that they use once per week and 55% reported that they use the repellents in very rare cases.
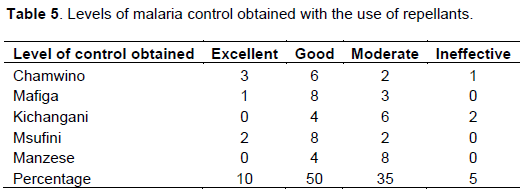
Recognition on the impression of the level of control obtained with the use of repellants
Table 5 summarizes the impression on the level of control obtained with the use of repellents. 10% of respondents noted the use of repellents to be excellent in managing malaria, 50% perceived the use of repellents as good in controlling malaria, 35% reported as moderate and 5% perceived the use of repellents as ineffective.
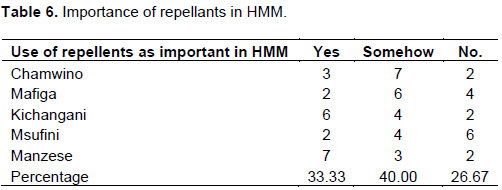
Response on the importance of the use of repellents in home management of malaria
The respondents were then asked to suggest if the use of repellents in accompany other methods is important in managing Malaria. Thirty-three (33.33%) noted that it is important, 40% reported it as somehow and 26.67% said it is not important (Table 6).
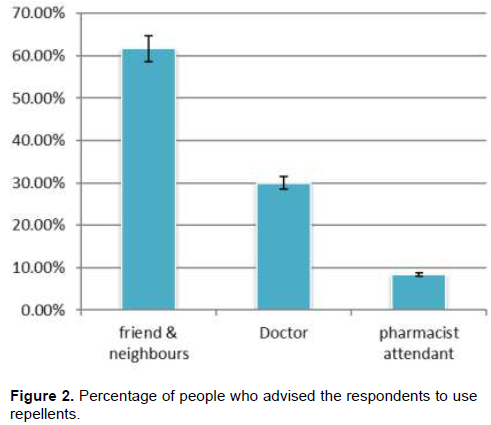
Assessment on who advised on the use of repellents to respondents
The participants were asked who recommended them to use the repellents in controlling Malaria at their homes. They were asked if they its friends, neighbors, doctors, or pharmacist attendants. Thirty-seven (37) participants (61.7%) mentioned that their friends and neighbors recommended them to use repellents, 18/60 (30%) were recommended by doctors and 5/60 (8.3%) were recommended by pharmacists attendant (Figure 2).
Indoor residual spraying
The participants were asked to comment on the issue of indoor residual spraying (IRS). Most participants (73.3%) agreed with indoor residual spraying while 26.7% of the participants denied on IRS program claiming that it is the source of other insects like bed bugs in their houses and the insecticides have a bad smell.
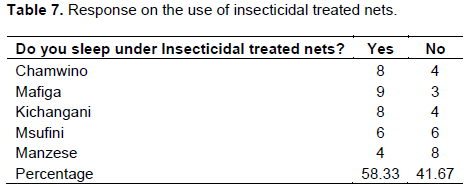
Recognition of the use of insecticidal treated nets (ITNs)
Participants in each study area were asked if they use ITNs as one of the measures to control Malaria at their homes. The 58.33% noted the use of ITNs at their homes while 41.67% do not have a tendency of using ITNs as a measure to prevent Malaria infection (Table 7).
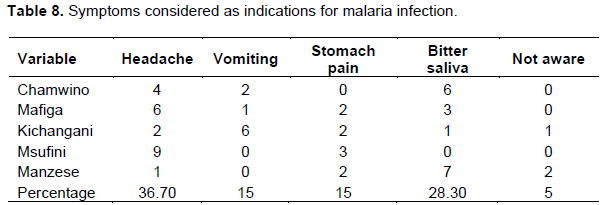
Primary symptoms are considered as indicators for malaria infection
The respondents were given five optional choices (headache, vomiting, stomach pain, bitter saliva, and not aware) to choose as symptoms they consider in Malaria infection. The 36.675 noticed headache as a symptom of malaria infection, 15% reported vomiting, 15% noticed stomach pain, and 28.3% mentioned bitter saliva and 5% were not aware of any of the indicators for Malaria infection. Table 8 summarizes the response to symptoms.
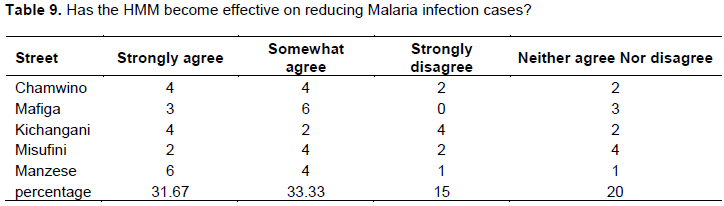
Perception on the effectiveness of home management of malaria in reducing malaria infection cases
Table 9 depicts the response to the recommendations on the effectiveness of HMM in reducing infection cases. As 31.7% strongly agreed that HMM has been effective in reducing malaria infection cases, 33.33% noticed the effectiveness to be somehow, 15% strongly disagreed that HMM has not been effective anymore in reducing Malaria infection cases and 20% neither agreed nor disagreed.
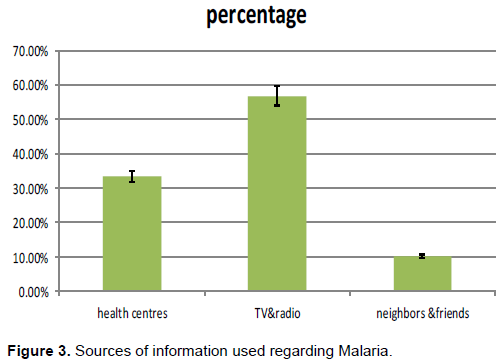
Recognition of the sources of information used regarding malaria
Different sources of information were tagged by respondents being used as ways of acquiring different information about malaria. Most mentioned Televisions and radio (56.7%) as the media for obtaining information, 33.3% mentioned health centers as their sources of information, and 10% used to obtain information from their neighbors and friends (Figure 3).
Factors hindering proper Home management of malaria
About 40% of the respondents noticed poverty as a factor that hindered proper home management of malaria. Some of the respondents (33.3%) perceived that illiteracy/ignorance is a hindering factor. However, 10% reported improper use of insecticide-treated nets as hindering factor and 15% agreed that an unclean environment and over or under dosage of drugs were factors that hindered proper Home Management of Malaria.
DISCUSSION
The areas selected were based on the fact there is standing water created by rainfall and also the community itself which provide breeding grounds for malaria-carrying mosquitoes. In this study, it was revealed that most people in the selected areas are somehow aware of malaria as they demonstrated a better understanding of malaria causes, symptoms, and preventive measures. These findings conform to previous studies by Mabaso et al. (2012). The majority of the respondents mentioned the correct route for malaria transmission (through the bite of a mosquito). A few respondents demonstrated having poor knowledge of the malaria transmission route as some believed it is a spiritual problem. The same results were also similar to the results which were reported by Hopkins et al. (2007) and Govella and Ferguson (2012). The study communities reported identifying malaria mainly on the basis of symptoms of headache or high fever and vomiting. Despite good knowledge of symptoms to the majority of respondents, some of the respondents were not aware of the symptoms of malaria at all. Thus, lack of clear knowledge among the respondents could lead to delay in seeking appropriate care from health facilities.
Insect repellents and the use of Insecticidal Treated Nets (ITNs) were highly recognized as methods for protection against malaria, most of the studies have also reported the benefits of ITNs. The majority reported having a tendency to sleep under bed nets, though the respondents mentioned the affordability to purchase a net was the barrier to owning a net. This was an encouraging observation and can be used by the malaria control program to increase the number of ITNs to help to combat malaria cases in families. Malaria control based on indoor residual spraying depended on the acceptance of the respondents, though the majority of respondents (73.3%) agreed with the issue of IRS, other respondents did not accept it. And the causes of refusal of IRS were the bad smell of the insecticides, poisoning to their domestic animals, and may accelerate the occurrence of other insects like bedbugs. Previous studies by Ajay et al. (2008) also noticed this. Thus, there is a significant relationship between people’s knowledge of the cause of malaria and preventive measures against it.
Despite a better understanding of malaria transmission risks, signs and symptoms, the study respondents demonstrated a knowledge gap on mosquito breeding sites by stating cattle sheds, dirty areas, dark places and edges of ponds, and stagnant water to be the most breeding sites for malaria vector. In the current study, participants demonstrated better knowledge of malaria breeding sites. This study is contrary to the study conducted by Mathania et al. (2016) and Madne et al. (2014) whereby garbage and long grasses were potential breeding sites for malaria vectors. Most respondents reported their friends and neighbors to be their most common source of information, whereas most adults utilized health centers as areas for seeking health information whereas respondents of the mid-age pointed to radio and television as the source of information. The findings correlate with the study done by Edson and Kayombo (2007). Time spent at home for the mid ages could explain the reason for their choice. This study has realized that the mid ages group had better knowledge on malaria transmission is by mosquito bites when compared to adults. Perhaps this is because the mid-age respondents were currently from school thus this suggests that malaria intervention officers should involve school teachers in malaria intervention programs.
On the other the case of use of repellents, most participants mentioned the use of sprays though they had a claim on the highest cost of the repellents thus due to cost the HMM in most of the families is not achieved effectively. Most participants (43.3%) noticed the use of repellents only once per week to save the repellent in a way that lasts for a long time. Many studies have reported insecticidal pressure as a response to prevent malaria (Emidi et al., 2015), but this was in response to indoor interventions thus does not consider the people working in outdoor activities thus leaving a high chance of being exposed to malaria.
This study has found that the majority of participants were not aware that mosquitoes can bite in the early evening and are capable of transmitting malaria. This could be due to constant messages pointing to malaria as a disease transmitted by midnight-biting mosquitoes. Similar findings were reported by Russell et al. (2011). Thus, most participants (28.3%) noticed the use of repellents, and (25%) reported the use of insecticidal treated nets as methods to prevent malaria compared to other methods. Thus, the healthy community should impart knowledge to the community about the changed feeding behavior of mosquitoes responsible for malaria infection so that people can protect themselves against early mosquito bites.
CONCLUSION AND RECOMMENDATIONS
The findings of this study have shown that the communities have knowledge of malaria transmission, symptoms, and prevention measures. The use of repellents is widespread among respondents which makes it intensive in malaria control. The high use of repellents is an advantage for the malaria control programs. There is a need for future studies to evaluate more the effectiveness of Home Management of Malaria so that to enhance the community perception of the overall program of preventing Malaria. Lastly, there is a great need for collaboration between the government and non-government sectors on malaria control.
CONFLICT OF INTERESTS
The authors have not declared any conflict of inter
ACKNOWLEDGMENTS
The authors are grateful to Dr. Mshamu Shabani for his valuable comments on statistical analysis and all households who participated in the study.
REFERENCES
|
Ajay LO, Falade CO, Bamgboye EA, Oduala AMJ, Kale OO (2008). Assessment of treatment guidelines to improve home treatment of Malaria in children in rural southwest Nigeria. Malaria Journal 7:24 |
|
|
Chukwuocha UM, Osuagwu AE, Dozie INS, Nwoke, BEB (2009). The clinical pattern and complications of severe malaria in parts of the Imo river basin of Nigeria. Nigerian Hospital Practice 3(6):4314-4321. |
|
|
Conrad MD, RosenthaI PJ (2019). Antimalarial drug resistance in Africa: the calm before the storm? Lancet Infectious Diseases 19(10):e338-e351. |
|
|
Daniel M, Sigsbert PM (2017). The malaria testing and treatment landscape in mainland Tanzania. Malaria Journal 16(1):1-15. |
|
|
Edson F, Kayombo EJ (2007) Knowledge on Malaria Transmission and Its Prevention among Schoolchildren in Kyela District, South-Western Tanzania. Tanzania Health Research Bulletin 9(3):207-210. |
|
|
Hopkins H, Talisuma A, Whitty CJM, Staedke SG (2007). Impact of home-based management of malaria on health outcomes in Africa: a systematic review of the evidence. Malaria Journal 6(1):1-10. |
|
|
Emidi B, Kabula B, Tungu P, Massaga J, Kisinza W (2015). Insecticide resistance testing in malaria vectors in Tanzania: Challenges in mosquito sampling and rearing under field conditions. Rwanda Journal 2(1):60-64. |
|
|
Govella NC, Ferguson H (2012). Why Use of Interventions Targeting Outdoor Biting Mosquitoes will be Necessary to Achieve Malaria Elimination. Front Physiology 3:199. |
|
|
Killeen GF, Seyoum A, Sikaala C, Zomboko AS, Gimnig JE, Govella NJ (2013). Eliminating malaria vectors. Parasit Vectors 6(1):172. |
|
|
Mabaso M, Ndlovu NC (2012). Critical review of research literature on climate-driven malaria epidemics in sub-Saharan Africa. Public Health 126(11):909-919. |
|
|
Madne G, Jindal AK, Patel BB, Sharma R, Kant R (2014). Knowledge and practices concerning malaria in rural community of Pune district. Medical Journal of Dr. DY Patil University 7(4):450. |
|
|
Mathania MM, Kimera SI, Silayo RS (2016). Knowledge and awareness of malaria and mosquito biting behaviour in selected sites within Morogoro and Dodoma regions Tanzania. Malaria Journal 15(1):1-9. |
|
|
Mboera LE, Ipuge Y, Kumalija CJ, Rubona J, Perera S, Masanja H (2015). Midterm review of national health plans: an example from the United Republic of Tanzania. Bull World Health Organ 93:271-278. |
|
|
Measure DHS Project (2011). Tanzania HIV/AIDS and malaria indicator survey 2011-12: Key findings. Dar es Salaam, Tanzania Commission for AIDS, National Bureau of Statistics, ICF International. |
|
|
Ministry of Health (2015). Midterm analytical review of the performance of the health sector strategic plan III 2009-2015. |
|
|
Moonen B, Cohen JM, Snow RW, Slutsker L, Drakeley C, Smith DL (2010). Operational strategies to achieve and maintain malaria elimination. The Lancet 376(9752):1592-1603. |
|
|
Oreagba AF, Onajole AT, Olayemi SA (2004). Knowledge of malaria among caregivers of young children of rural and urban communities. Tropical Journal of Pharmaceutical Research 3(1):299-304. |
|
|
Partnership Roll Back Malaria (2005). Scaling up insecticide-treated netting programs in Africa: a strategic framework for coordinated national action. Geneva: World Health Organization P 26. |
|
|
Russell TL, Govella NJ, Azizi S, Drakeley CJ, Kachur SP, Killeen GF (2011). Increased proportions of outdoor feeding among residual malaria vector populations following increased use of insecticide-treated nets in rural Tanzania. Malaria Journal 10(1):1-10. |
|
|
World Health Organization (WHO) (2005). Report of the expert committee on malaria, 2005. |
|
|
World Health Organization (WHO) (2009). World Malaria report 2009. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


