Full Length Research Paper

ABSTRACT
Youths are facing different sexual and reproductive health problems. Most health services for youth are designed for adults and do not always have favorable conditions to meet the special needs of youths. As well, youths have been characterized by low sexual and reproductive health service utilization. Identifying and integrating young people preferences and needs regarding health facility helps better to serve the youth. Sexual and reproductive health needs and service utilization among youths in West Badewacho Woreda, Hadiya Zone, South Ethiopia was assess. A cross sectional study was conducted from 1 to 30 March, 2014 in West Badewacho Woreda, Hadiya Zone, South Ethiopia. A simple random sampling technique was used and total sample size was 658 youths. Data were entered into epi data 3.1 and exported to Statistical Package for the Social Sciences (SPSS) version 20. Descriptive statics for age and family size, proportion for categorical variables, bivarate and multivariate logistic regression analysis were performed. Total of 640 subjects participated in the study and yielded 97.3% response rate. Out of total participants, 25.8% ever had sex. From the total respondents, 76.3% need at least one component of sexual and reproductive health services. During multivariate analysis sex, age, knowledge about reproductive health, participation in peer education, youth educational status and ever had sex were predictors to have reproductive health service need. Out of the total participants, only 29.4% youths utilized reproductive health services in the last one year. In multivariate analysis, ever had sex (Aor3.080, 95%ci [1.918 to 4.944]), ever heard about sexual and reproductive health (Aor=2.016, 95%ci [1.308 to 3.106]) and had need to reproductive health services (Aor= 8.564, 95% [4.080 to 17.977]) were predictors to sexual and reproductive health service utilization. Youths have imprecise sexual and reproductive health knowledge. In contrast to the huge sexual and reproductive health needs, the services provided by the nearby health facility are far from addressing the needs even if the services were available its unfriendliness to youths resulted in less utilization of the available services.
Key word: Youths, adolescent, sexual, reproductive health, service utilization.
INTRODUCTION
Globally, there are 1.8 billion young people aged 10 to 24 years, representing 33% of the world’s population , with over 85% living in developing countries. Recent estimates (in 2013) indicate that 17.0% of the global population, 20.0% of Sub-Saharan Africa and 20.3% of Ethiopian population are composed of youth aged 15 to 24 years in which 4/5th live in rural parts (Worled Health Organization 2011).
Worldwide, the young ones are facing different sexual and reproductive health problems like unwanted pregnancy, unsafe abortion, sexual transmitted infections (STI) including the human immunodeficiency virus (HIV) and substance abuse, but people who are young are usually mistakenly perceived to be healthy and not in need of special health services (Roudi-fahimi and El Feki S 2008; Alliance A youth 2005). In the developing world, unmarried people in the past were nearly expected to need reproductive health services. Viewing youths as a specific group with their own reproductive health service needs is a relatively recent practice (Regmi et al., 2010; Ethiopia Minister of Health 2006). Health services for youth are not designed as needed and do not always have favorable conditions to meet the special needs of youths this is because, youths’ accesses to the services are not clearly understood by themselves and service providers. Attracting the youth to the clinical services has remained a challenge and that there is need to create demand and improve health-seeking behavior of the youth (African youth alliance 2012; Alliance/pathfinder 2005).
Ethiopia adapted International Conference on Population and Development (ICPD) agreement and take measures that have been commenced to alleviate the problem which includes the development of the national adolescent and youth reproductive health strategy, youth policy, standards on youth friendly reproductive health (RH) services, and youth sector development plan (Chicago university 2013). In spite of this, most of the existing services are still adult-centered, non-youth friendly, undertaken in small scale and not well organized to meet the RH service needs of this section of the population. But despite these initiatives, reproductive health service utilization among the youth still faces a lot of challenges related to the sensitive nature of youth sex and sexuality (Center UkH development 2011). There is no youth center and stand alone youth friendly facility at West BADEWACHO Woreda while youth reproductive health services are offered using the integrated model of service delivery in health facilities. There is limited information about such programs operation and barriers for utilization in health facilities at the study area even at county level. In Ethiopia, there is no clear evidence about youth sexual and Reproductive Health (SRH) need and as well gaps. This study aim to investigate youth’s reproductive health needs, service utilization and facility service operational barriers for youth friendly services at public health facilities. This study had also identified areas for service quality improvements aim to adjust and organize reproductive health services of public health facilities. It is also important for health planners and policy makers to design a strategy for improve youth/adolescent reproductive health center. This research is also expected to fill gaps in this area of research and add to the existing body of knowledge.
MATERIALS AND METHODS
The study was conducted from 1 to 30 March, 2014 in West Badewacho Woreda, Hadiya Zone, South Ethiopia. West Badewacho is located at 348 km from Addis Ababa to the south and 114km from Hawasa to the west and 100 km from Hosanna town. Community based cross-sectional study by employing both quantitative and qualitative techniques were conducted.
Quantitative part
A total sample size of 658 youths were used in this study, using the following assumptions p=18.8% taken from rural youth reproductive health service utilization study at North West Ethiopia, Mechakel District 2013, 95% ci, 5% marginal error and 10% non-response rate and design effect 2.
Qualitative study
Purposive sampling technique was used for qualitative study from four health centers in the Woreda and four health posts were selected randomly. Six service providers and two health centers heads were selected purposively and participated in the study from health facilities, then in-depth interview of health facility heads and service providers with facility observation was conducted by principal investigator using interview guide and observation checklists.
Sampling procedure
Multi stage sampling technique was used from 22 kebeles (administration unit) in the district, 7 kebeles were selected by simple random sampling technique then sampling frame of youth’s age 15 to 24 years old was prepared from health post house hold family folder at each selected kebeles; proportional allocation to size of youths was used. After that, we selected proportional number of youths by simple random sampling technique from each selected kebeles. When more than one youth was found per household one youth was selected by a lottery method to avoid Household collinearity effect. When a youth was not found at home three consecutive visits was made before considering them as non-respondent. A questionnaire was adapted by reviewing different literatures and customized based on the study objectives and study area. After translation to amharic and hadiyssa by language expert’s, face-to-face interview was conducted by trained data collectors who speak both languages and translated back to English. Ten data collectors who completed college diploma nurses and two Bsc clinical nurse supervisors were recruited and underwent one day training. The questionnaire was Pre tested on 33 youths in Jarso Mazoria kebele before data collection to check consistency and corrections were taken. Anonymity was kept during data collection. Interviews were conducted in a private place and confidentiality was kept and respondents were assured that the information will not be accessible to others. After completing each interview, data collectors checked for completeness of questionnaire. Data was checked for completeness, consistency and entered to EPI data 3.1 then exported to SPSS version 20 for analysis. Descriptive statics for age, family size and age at first sex, proportion for categorical variables, bivarate and multivariate logistic regressions with 95%CI analysis were performed. Candidate variables with P-value less than 0.25 in the bivarate analysis were included in the multivariate logistic regression analysis to develop model. Then variables P-value of less than 0.05 in multivariate analysis were taken as significance and included in the final model. Results were organized using tables, charts and statement. Qualitative data was analysed thematically in narrative way and triangulated with quantitative findings.
Ethical consideration
In order to maintain confidentiality, the sitting arrangement of the participants was considered: all the selected youths were called and made to sit in prior arranged rooms. Each youth took a single seat with sparse arrangement of chairs and desks. No names or identifiers were included on the questionnaire. For the qualitative part, we obtained verbal consent from the participants. Then the data collectors made the interview by using semi-structured interview guide. The interview was entirely tape recorded and field notes were taken.
RESULTS
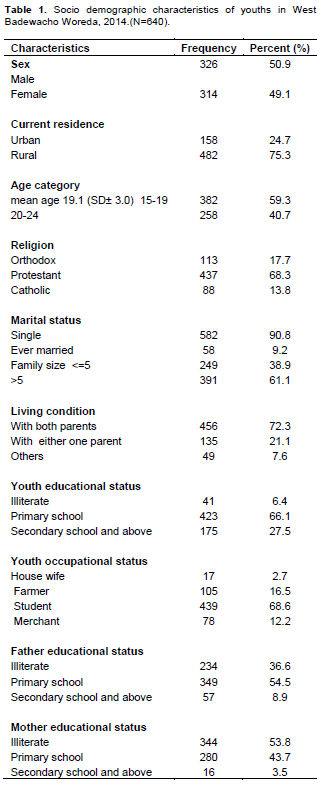
Socio demographic characteristics
Out of the total participants, 165 (25.8%) ever had sex and among those 134 (81.2%) have had sexual intercourse in the last 12 months. The mean age to start sexual intercourse was 16.9 (SD±2.8). Major reasons for sexual debut were personal desire 63 (38.2%), peer pressure 53 (32.1%), marriage 38 (23%) and others (6.7%). The study shows that 74 (55.2%) of the sexually active youths had more than one sexual partner in the past one year. Education (Table 2).
Knowledge on sexually transmitted infections
From all respondents 335 (52.3%) heard about sexually transmitted infections. The most common types of STI mentioned to be known were gonorrhea 282 (44.1%), syphilis 212 (33.1%), cancroids 106 (16.6%) and Lymphogranuloma venereum (LGV) 61(9.5%). Common STI symptoms mentioned by youths were burning during urination 213 (33.1%), genital ulcers 140 (21.9%) and genital discharge 168 (26.3%). Out of sexually active participants 28 (20.8%) had experienced either one of STI symptom. But from these, only 11 (39.2%) sought medical treatment. Some youths had misconceptions on the mode of transmission of STIs. More than half of the respondents 382 (59.7%) said STIs are transmitted through unprotected sex and 40.3% had misconception like urinating on a hot stone 110 (17.2%), urinating when moon raise (11.9) and sitting on hot stone 71 (11.1%).
Knowledge on fertility and family planning
The fertility awareness of youths was assessed by asking the period that a woman can get pregnant if she has unprotected sex. Out of these, 91 (40.4%) males and 134 (59.6%) were females. The most frequently mentioned family planning methods were pills 415 (64.8%), injectables 305 (47.7%) and condoms 260 (40.6%). The most common utilized contraceptives were condom (52.5%), pills (31.1%), injectable (26.2%), implanon (9.8%), intrauterine contraceptive device (IUCD) (6.5%) and others (4.9%).
Knowledge on HIV/AIDS
Some youths had misconception about HIV/AIDS transmission. Three hundred and forty (53.1 %%) respondents had misconceptions on the mode of transmission of HIV such as, body contact, mosquito bite and sharing of meal with an HIV infected person. The most commonly mentioned HIV/AIDS prevention methods include, sexual abstinence 415 (64.8%), having one uninfected faithful partner 458 (71.6%), using condoms correctly and consistently 407 (63.6%) and avoiding sharing of sharp materials 206 (32.2%).
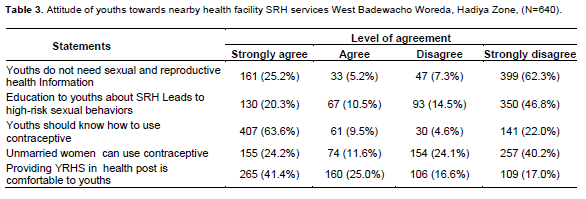
Attitude of youths towards nearby Health facility SRH services
As indicated below in Table 3, most youths 446 (69.6%) had favorable attitude towards reproductive health information to youths. More than half (66.4%) agreed with the idea of availing reproductive health services in health post is comfortable to youths. Although the proportion of youths that agreed on the need for youths to know contraception usage was high 468 (73.1%), the proportion of youths counteracting the idea of unmarried women who have sexual practice to use contraceptive was also high 411(64.3%) (Table 3).
STI/HIV/AIDS risk perception of youths
Of the 640 respondents, 256 (40.0%) stated that their level of risk to acquiring STI/HIV/AIDS was low while 141 (22.0%) perceived that their level of risk was high as illustrated in the pie chart. The major reasons for low or no risk perception by the respondents was abstinence or sexual inactivity, having a single sexual partner while few alluded it to the use of condoms during sex. Those that felt to be at a higher risk reasoned multiple sexual partnerships, inconsistent condom use and no condom use at all as the reasons for their higher STI/HIV infection risk.
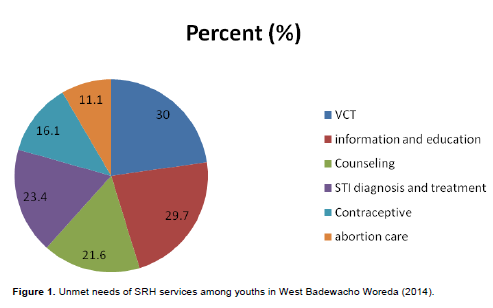
Unmet needs of SRH services among youths
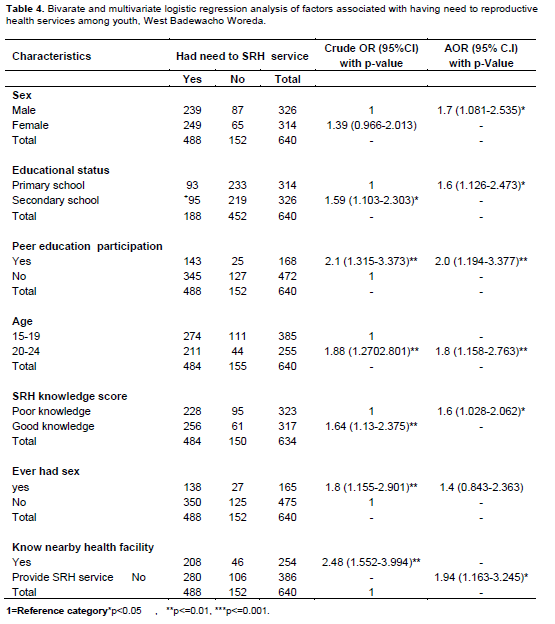
In response to questions regarding sexual and reproductive health service provision modalities; the youth stated that they would prefer a room within the health center that is separate from other services (33.0%) followed by in health post (25.8%) and out of health facility within their own center (22.3%) Figure 1. During bivarate analysis educational status, age, knowledge about SRH, participation in peer education, ever had sex, and know nearby health facility provide SRH service were associated with sexual and reproductive health service need among youths. After controlling for potential confounding variables through logistic regression sex, educational status, age, knowledge about SRH, participation in peer education, and know nearby health facility provide SRH service are predictors to have need to SRH services.
Female youths (all of them didn’t have any experience of having child) were about 69% (AOR = 1.693 CI: [1.081 to 2.535]) they were more likely to have need for SRH service than the males. The odds of having need to SRH services was about 1.6 times (AOR = 1.6, 95%CI [1.126 to 2.473]) higher for secondary school and above educated youths than primary school educational status youths. Youths aged 20 to 24 years were 80% (AOR = 1.8, 95%CI [1.158-2.763]) more likely to have a need for SRH services than those 15 to 19 years old. Participants’ have had good knowledge (above mean knowledgeable and below mean didn’t know) about sexual and reproductive health service need was 60% (AOR= 1.6, 95%CI [1.028-2.062]) higher than those who had poor knowledge. The odds of having need for SRH services was 2 times (AOR=2.0, 95%CI [1.194 to 3.377]) higher for youths who participated in peer-to-peer SRH education than those who did not participate. The odds of needing sexual and reproductive health services among youths who knew about the availability of a health facility providing sexual and reproductive health service was 2 times (AOR=1.94, 95%CI [1.163 to 3.245]) higher than those who did not about the availability (Table 4).
From qualitative study according to the informants, both health centers and catchment health posts provide reproductive health services to youths. The range of services provided by both health centers were voluntary counselling and testing (VCT), family planning, counseling, STI diagnosis and treatment and abortion. The health posts provide family planning and information, education and communication about reproductive health. Based on their experience, most key informant participants mentioned that most youths would like to get to a health facility for contraception, condom and abortion services. The service provider said:
“Some youths ask contraceptive, condom and we give them. When we place condom out of Health post room no condom when we back from lunch. This shows even if they fear many youths have needed to utilize SRH services”.
Most key informants mentioned youth reproductive health services are given together with other services in adult outpatient department (OPD) and delivery case team in both health centers. The waiting area was together with adult patients/clients. All of the informants agreed on the non comfortable of waiting area and service provision room to youths.
“From my experience when youths came to health center they do not know where the service is given and fear to tell what they want to get. Most of them came and stand on the corner of health center don’t ask any thing. But when I ask their need they tell me if they want VCT I provide the service and take them to delivery case team for other SRH services. They never sit and wait services at waiting area with adult clients/patients” service provider key informant.
According to service providers for the issue of service utilization, the service unit aim to provide reproductive health services which are not comfortable to youths with the possibility of hearing others conversations and sometimes there is interruption while delivering services. Since a single provider is expected to deliver family planning (FP), VCT and other sexual and reproductive health services at same time, use of separate rooms for different services were difficult. According to key informants, most sexual and reproductive health services were free to youths except sexually transmitted infection case treatment and HCG pregnancy test that are provided with fee.
Concerning approach of service provider who visited the service said that, 144 (66.4%) youths were comfortable and welcoming while 73 (33.6%) youths were not comfortable and welcoming. On the other hand, the proportion of youths that were satisfied with the service they got from the nearby health facility were 140 (64.5%). All Key informants mentioned that generally, FP provision, abortion cares and prevention of mother-to-child transmission of HIV (PMTCT) training were provided to service providers but no specific training on youth reproductive health service.
The observation finding shows that in all studied health facilities, no signs announcing the presence of RH services together with the list of services and working hours at the gate. The waiting area was in front of the card room on the corridor of adult OPD and delivery room. The service unit at the adult OPD had not been screened to examination bed and it was easy to hear client conversation from outside. From training inventory review, no staff was trained about counseling, STI diagnosis and treatment, youth sexual and reproductive health services. Even if not specific to youths, there were posters about family planning, HIV/AIDS and antenatal clinic (ANC).
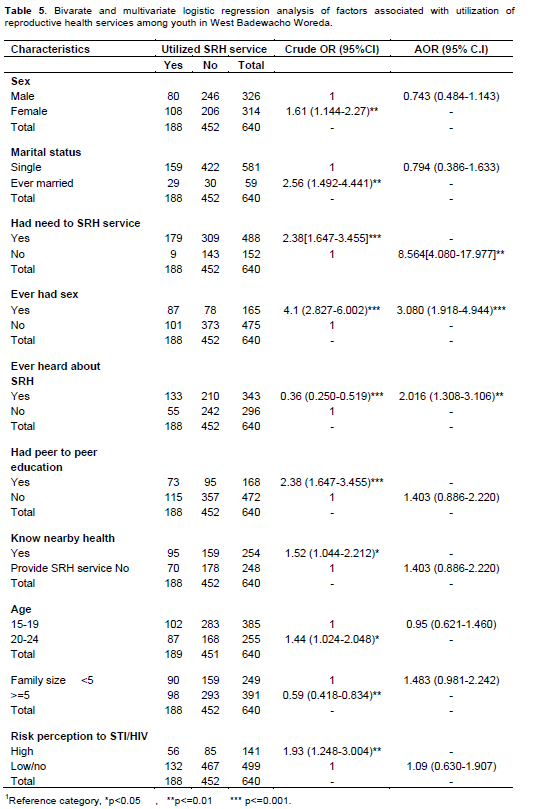
The bivarate analysis showed that utilization of the nearby health facility for sexual and reproductive health services is positively associated with being female (COR 1.61,95%CI 1.144 to 2.272), married (COR 2.56, 95%CI 1.492 to 4.441), had need to SRH services (COR 9.2, 95%CI 4.579 to 18.503), ever had sex (COR 4.1, 95% CI 2.827 to 6.002), participation in peer education (COR 2.38, 95% CI 1.647 to 3.455), Know nearby health facility provide SRH service (COR 1.52, 95%CI 1.044 to 2.212), age 20 to 24years old (COR 1.44, 95%CI 1.024 to 2.048) and high risk perception to STI/HIV/AIDS (COR 1.93, 95%CI 1.248 to 3.004). Results of multivariate analysis dedicated that have need to sexual and reproductive health services, ever had sex and ever heard about SRH are the main predictors of sexual and reproductive health service utilization. The odds of sexual and reproductive health service utilization was 8 times (AOR= 8.56, 95% [4.080 to 17.977]) higher for youths who had need to SRH services than those who did not need the services. Reproductive health service utilization among youths who heard about SRH was 2 times (AOR=2.02, 95%CI (1.308-3.106)] higher than never heard about it. The odds of reproductive health service utilization to ever had sex youths was 3 times (AOR 3.08, 95%CI [1.918 to 4.944]) higher than abstainers (Table 5).
DISCUSSION
Youths in West Badewacho Woreda have huge sexual and reproductive health need while the services available are far from addressing these needs. Moreover, the study gives an insight into the gap in youths knowledge on sexual and reproductive health and their poor service utilization despite the fact that there are risky sexual practices among youths.
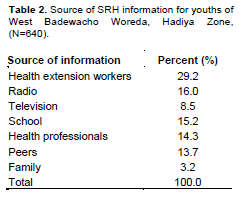
More than half of the respondents heard about sexual and reproductive health. This is lesser than the study conducted in Addis Ababa University students (Regmi et al., 2010). This discrepancy explained is due to less information sources and weak peer education programs in the study area. The major sources of information were health extension workers followed by radio and television. This is consistent with the previous studies of Mechekel and Gondar (Ethiopia Minister of Health 2006; African youth alliance 2012). More than half of the respondents had experienced either one of STI symptom. This is higher than the study conducted in Nigeria (Alliance/pathfinder 2005). The difference may be that, consistent condom utilization is low and misconception about mode of transmission is high in the study area.
More than half of the respondents did not know fertile time in a woman’s menstrual cycle. When we see the proportion of females and male, it is better than the findings of the recent Ethiopian demographic health survey of women and men of all ages in the community knowing the unsafe period of a woman (Roudi-fahimi and El Feki 2008; Regmi et al., 2010). Still the observed proportion is not adequate to say youths are knowledgeable on this issue. This study dedicated that out of sexually active youths in the last one year use contraceptive. This is comparable with the study conducted in Chicago university (Chicago university 2013). The major services needed by youths were VCT, information and education, counseling, contraceptive, abortion car and condom distribution. This study finding is lower than the studies done in Addis Ababa University (Center UkH development 2011). The possible reason for the discrepancy is lack of information and low awareness about sexual and reproductive health in the study area. The current study indicates that around 30% youths visited health facilities for sexual and reproductive health services in the past one year. This result is higher than previous studies done in Nepal among youth (Chicago university 2013). This may be due to difference in infrastructure and socio cultural background in two countries. The most frequent visited health facilities were health center followed by health post and private clinic for sexual and reproductive health services which is consistent with the study conducted in Gondar and Mechekel (USAID 2007; Mengistu and Melku 2013).
With the approach of service provider, more than half of the youths who visited the service said they were comfortable and felt they were welcomed. This study result is lower than that of previous studies in India and Botswana (Center UkH development 2011; Mengistu and Melku 2013). The possible explanation for the discrepancy may be service providers at the study area were not trained about counseling and youth friendly services. This is supported by qualitative findings. The major reasons for not welcoming were that service provider see and fear when they get to meet new person’s and the case of not having money, this is comparable with previous studies conducted in Dessie mechekel and kenya (Mengistu and Melku 2013; Guttmacher Institute, International Planned Parenthood Federation 2010; Okereke 2011).
Concerning accessibility of health facility to utilize sexual and reproductive health services, only 10.5% youths take more than two hours to reach the nearby health facility on foot from their home. This is less than the study conducted in Guttmacher Institute, International Planned Parenthood Federation (Guttmacher Institute, International Planned Parenthood Federation 2010). This discrepancy may be difference in health care system and infrastructure of the two countries. Consistent with different studies in the current study, old youths were more likely to utilize sexual and reproductive health services than young youths Nepal and Kenya (Okereke 2011). A substantial number of studies identified that youths with secondary education and above were more likely to utilize sexual and reproductive health service than primary. This study also supported the above claim. Female youths were more likely to utilize sexual and reproductive health services as compared to male youths kenya (Okereke 2011). This finding is different from that of a study conducted in mechekel and rural Ethiopia (Molla et al., 2009) and Nigeria. A possible explanation can be that most participants in peer education were females that can lead to open discussion and increase awareness.
CONCLUSION
Consistent with other study, youths who participated in peer to peer education were more likely to utilize sexual and reproductive health services than not participated ones Rural Ethiopia (ICOMP 2009; Molla et al., 2009). This can be justified by the fact that discussion of services with peer categories allows youths to create more opportunities to exchange information and experiences to get awareness about services. Consistent with other studies, youths with high risk perception to acquire STI/HIV/AIDS were more likely to utilize sexual and reproductive health services than those who had low risk perception Gondar (Okereke 2011). Unlike other studies, knowledge about sexual and reproductive health (Mengistu and Melku 2013; Okereke 2011; Molla et al., 2009) and residence are not associated with sexual and reproductive health service utilization. The possible explanation is that the current study conducted in rural district where the towns are small do not have significant difference in many aspects with that of the nearby rural kebeles.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
| African youth alliance (2012). Reproductive Health White Paper World Youth Alliance.18(4): 1–15. | ||||
| Alliance A youth (2005). R esearch Utilization Developing and Scaling Up a Counseling Tool to Promote Integrated Services for Youth 8(3):18-38. | ||||
| Alliance/pathfinder. Integrating Youth-Friendly Sexual and Reproductive Health Services in Public Health Facilities(2005). A Success Story and Lessons Learned in Tanzania November 8(5):1–17. | ||||
| Center UkH development(2011). Helpdesk Report: Adolescent Reproductive Health in Ethiopia 13(2): 1–21. | ||||
| Chicago university (2013). Policy Brief School-based Health Centers: Implications for Adolescent Reproductive Health 9(2):1–8. | ||||
| Ethiopia Minister of Health(2006). National Adolescent and Youth Reproductive Health Strategy 12(6):4–68. | ||||
| Guttmacher Institute, International Planned Parenthood Federation(2010). Facts on the sexual and reproductive health of adolescent women in the developing world. April. Available at: www.guttmacher.org/pubs/FB Adolescents-SRH. | ||||
| ICOMP IC(2009) . Linked Response to Reproductive Health and HIV / AIDS 8(1):7–38. | ||||
|
Mengistu TS, Melku AT(2013). Sexual and reproductive health problems and service needs of university students in south east Ethiopia a Exploratory qualitative study. Sci. J. Public Heal. 1(4):184–8. |
||||
|
Molla M, Emmelin M, Berhane Y, Lindtjørn B (2009). Readiness of youth in rural Ethiopia to seek health services for sexually transmited infections. African J. AIDS Res. 8(2):135–46. Crossref |
||||
| Okereke CI (2011). Unmet Reproductive Health Needs and Health-Seeking Behaviour of Adolescents in Owerri.Nigeria. Afr. J. Reprod. Health 14(1):43–54. | ||||
| Regmi PR, Teijlingen E Van, Simkhada P, Acharya DR (2010). Barriers to Sexual Health Services for Young People in Nepal. ©INTERNATIONAL Cent. DIARRHOEAL Dis. Res. 28(6):1–9. | ||||
| Roudi-fahimi F, El Feki S (2008). Facts of life Youth Sexuality and Reproductive Health. Midle East North Africa 9(6):1–78. | ||||
| USAID (2007). Integrating Family Planning and HIV / AIDS Services for Young People : Tools for Programming 11(3):2–25. | ||||
| Worled Health Organization (2011). Young People Today . Time to Act now 4(2):1–117. | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


