Full Length Research Paper

ABSTRACT
This study was conducted to study the correlating factors between personal nutritional awareness and consumption behavior of the elderly in Samutprakarn Province, Thailand. Members of the elderly society of Samutprakarn Province were interviewed with a rating scale questionnaire to know about their personal data, nutritional awareness and the factors that influence their food consumption behaviors. 400 elderlies participated in the study. Their ages range is between 60 and 84 years old (±0.79); with average age of 67.20 years. There were 156 males (38.90%) and 244 females (61.1%). Factors that influence nutritional awareness showed reliability statistic between 0.25 and 0.46 and food consumption behavior was 0.34. Moreover, result shows emotional awareness (r=0.43, p-value < 0.05), accurate self-assessment (r=0.13, p-value < 0.05), and self-confidence (r=0.16, p-value < 0.05) were positively and significantly correlated with food consumption behaviors. It can be concluded that the 3 personal awareness factors were positively correlated with food consumption behaviors. With a high rating, personal awareness can impact proper food consumption behaviors.
Key word: Elderly, food consumption behavior, nutritional awareness, personal factor.
INTRODUCTION
Our global population is getting older (U.S. Census Buereau, n.d.). In 2017, there was a total population of 7.4 billon people and more than 962 million were 60 years old and above, accounting for 13% of the global population. The growing rate of the elderly has increased by 3% resulting in an inevitable change in our population structures. European countries are the first to expect the change with the lowest (16%) of the population being considered children and 21% being over 65 years of age. Meanwhile, African countries have the highest population growth rate as the children population accounts for 42% and only 5% are elders. Thailand and other countries in Asia like Singapore and Japan are rapidly becoming aged society since 2005, meaning that the population f over 60 years of age accounts for more than 10% of the total population. Thailand’s National Statistical Office announced that 10.7% of the nation’s population is in their elderly stage. More than half of this number (58.8%) is early-aged, 31.7% are mid-aged and 9.5% are more than 80 years of age (National Statistical Office of Thailand, 2007). Suboptimal diet is an important preventable risk factor for non-communicable diseases (NCDs); however, its impact on the burden of NCDs has not been systematically evaluated. This study aimed to evaluate the consumption of major foods and nutrients across 195 countries and to quantify the impact of their suboptimal intake on NCD mortality and morbidity (GBD, 2017; Diet Collaborators, 2019). There have been studies in Ethiopia (Abate et al., 2020), South Africa (Naidoo et al., 2015), Sir Lanka (Damayanthi et al., 2018)and Brazil (Boscatto et al., 2013)stating that high proportion of older adults are malnourished and socio-economic characteristics and depression are significantly associated with malnutrition.
Moreover, Benjamas (2008)’s study reveals that the common elderly meals in Thailand are negatively related to numbers of health problems; heart and coronary arteries diseases. Most seniors will eventually have to experience changes physically, mentally and even socially. The common diseases found in aged people are diabetes, blood pressure abnormality, heart and coronary arteries diseases, gout and cancers. Because the important factor for these diseases is their food consumption behavior; they and their caregivers must be able to determine or provide appropriate nutrition for them. Moreover, with organs deterioration that comes with age, there is a higher risk for nutrition imbalance condition which leads to numerous chronic diseases; obesity, diabetes, and high blood pressure. Mazengo et al. (1996)’s study revealed the relationship between diet and dental caries by assessing 24 h food intake in 273 subjects aged 12, between 35-44 and 65-74. Their study found that the mean number of decayed teeth (DT) increased significantly with age. Wang et al. (2014)declared that more than 31,588 people above 50 years old have died due to coronary arteries disease and diabetes. Gunsam and Murden (2016) also reported factors influencing food choices in the elderly, which reflected in their eating behaviors and health (Gunsam and Murden, 2016).
MATERIALS AND METHODS
The purpose of this cross-sectional study is to study and analyze how personal factors (age, gender, education, income, and family-existence) affect the elderly people’s food consumption behaviors. Our subjects for this study were people above 60 years old, both male and female, who were fully aware and could fully communicate. The study subjects were members of Samutprakarn’s Senior Club. The main tools used in this study were interviews and questionnaires. The acquired data were analyzed to study the relationship between the consumption behavior of the elderly and their nutritional awareness.
Research population
There are 17,920 people aged over 60 years in Samutprakarn who lived with family and/or a caregiver. The sample size was calculated using Taro Yamane’s formula as follows:
n = N/(1+N(e)2)
where n = sample size, N = population under study, and e = acceptable sampling errors (=0.05).
From the total of 221,543 Samutprakarn’s senior citizens based on Samutprakarn’s Statistical Office’s data and the acceptable sampling errors of 0.05, the sample size was calculated to be 400 people.
Simple random sampling was performed on 400 people from 3 districts in Samutprakarn Province. The questions in the interviews and questionnaires were adapted from Goleman (1995)’s self-awareness theory and the 9 nutrition guidelines for the elderly. The questions were tested and reviewed in a small group of people aged between 50 and 59 prior to the actual study.
Inclusion criteria
(1) People aged 60 or above.
(2) Residents who had been living in Samutprakarn for at least 6 months
(3) People in their full conscious, with no sign of dementia and could communicate perfectly without hearing problem.
(4) People who were able to eat without any health concerns limitation.
(5) People in no need of assistance, physically or mentally.
(6) Having four natural posterior teeth (2 opposing teeth) or having functional denture
Exclusion criteria
(1) People who could not freely choose their own meal e.g., members of senior housing.
(2) People with dietary restrictions.
(3) Having no teeth or not wearing denture
Data were collected by interviewing the sample group. The interview was done with the help of village health volunteers and dental nurses in the area. Inter-examiner calibration was done. Each subject was interviewed directly by the researchers individually for approximately 10 min. The questions included their personal information, nutrition awareness, and consumption behavior. The details are as follows:
(1) Personal information: Sex, age, highest education, income, family and living conditions
(2) Nutrition awareness: Questions asked in the section were based on Goleman’s (1995)Mixed Model of Emotional Intelligence Theory, Healthy Diet for the Elderly: Guideline for food consumption (Healthy Diet for the Elderly, 2017). It was adapted from sakoolnamarka et al. (2021)’s research questions. The main topics were emotional awareness, accurate self-assessment and self-confidence ratings.
(3) Consumption behavior: Here, the interviewees were to answer questions regarding their consumption behavior. Questions here were adapted from Kitkamolsawet’s (2017)“Food consumption behavior and its risk/benefits to the health of the elderly in Nakorn Nayok”. The questions were mainly about the frequency of the elderly food consumption in a certain period of time.
The data obtained were then analyzed and interpreted by scoring with the criteria as follows:
Emotional Awareness: For positive behavior, 5 = very agreed, 4 = agreed, 3 = neither agreed nor disagreed, 2 = disagreed, 1 = totally disagreed. Reverse scoring was applied for negative behavior, as 5 = Totally Disagreed and 1 = Very Agreed.
Consumption Behavior: The scoring was based on the frequency of their healthy/unhealthy food consumption. For healthy consumption/behavior, 5 = Everyday, 4 = Almost everyday, 3 = Every other day, 2 = Once a week, 1 = Rare, and 0 = Not once. Reverse scoring was applied for unhealthy behavior, as 5 for Not once and 0 for Every day.
Then, the average scores were calculated in each topic to represent the behavior of the sample group. Reliability test was done using Cronbach’ alpha method. The data calculated were then analyzed to find the factors that influence older adults' consumption behaviors using independent t-test, One-way ANOVA and Pearson correlation coefficient. In this test, the confidence level was set at 0.95. Normality tests were done to determine if the obtained data set, including nutrition awareness and consumption behavior, were well-modeled by a normal distribution. The result from the Skewness and kurtosis test was between –1.00 and +1.00 which was in an acceptable range. Therefore, the data were considered normally distributed.
The questionnaires’ internal consistency reliability was tested by three professionals to determine:
(1) The content validity and appropriateness of the language used. Index of Item-Objective Congruence (IOC) all came back above 0.5.
(2) Reliability: The reliability test was done by interviewing a similar sample group with the exact same questions before the actual interview. Cronbach 'alpha reliability coefficient was between 0.78 and 0.83.
RESULTS
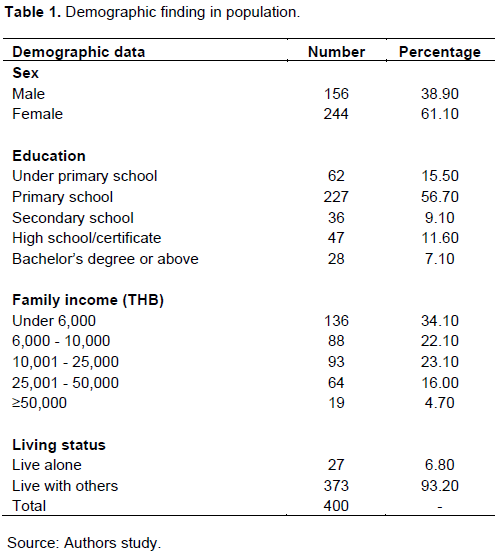
From the total of 400 old adults, 156 (38.90%) were males and 244 (61.10%) were females. Their age range is from 60 to 84 years old (±0.79) and the average age was 67.20 years old. 227 (56.70%) had the highest education level (primary school education). Thirty-four percent of the subjects had an income of less than 6,000 Baht per month. Most of the subjects (93.20%) stayed with their family. Table 1 shows the demographic profiles of the population.
The demographic data were analyzed together with the consumption behavioral data obtained using independent t-test and one-way ANOVA. The result of the overall test showed Education level and Family income had statistically and significant effect on the consumption behavior of the elderly (p=0.00).
Individual nutritional awareness
The data obtained were calculated to find the sample group’s representative value, the average for the individual nutritional awareness. The calculated scores were then interpreted as follows: 0.00-2.50 = Very Low, 2.51-3.00 = Low, 3.01-3.00 = Fair, 3.51-4.00 = High and Very High for more than 4.01.
Emotional awareness
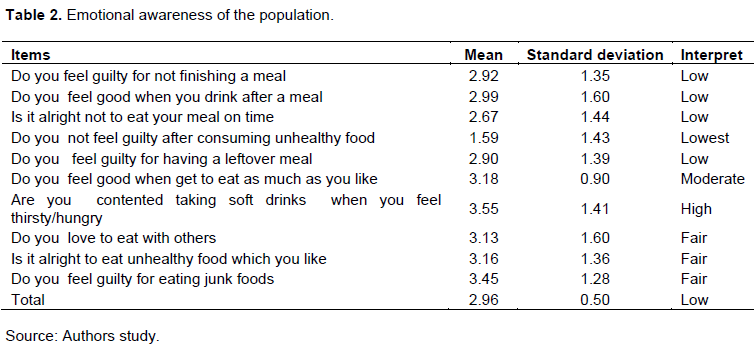
The result shows that the subjects are highly aware that taking soft drinks makes them feel satisfied when they are thirsty/hungry (Average of 3.55). The subjects do not feel guilty for eating junk foods (Average of 3.45). They feel good when they get to eat as much as they like (Average of 3.18). It is alright for them to eat unhealthy food which they like (Average of 3.16). They love to eat with their family (Average of 3.13) and they are alright not to eat their meal on time. However, they tend to feel good when they drink after a meal; they do not feel guilty for not finishing a meal and for having a leftover meal (average of 2.99, 2.92 and 2.90, respectively). They do not feeling guilty after consuming restricted food (1.5). The results are shown in Table 2.
Accurate self-assessment
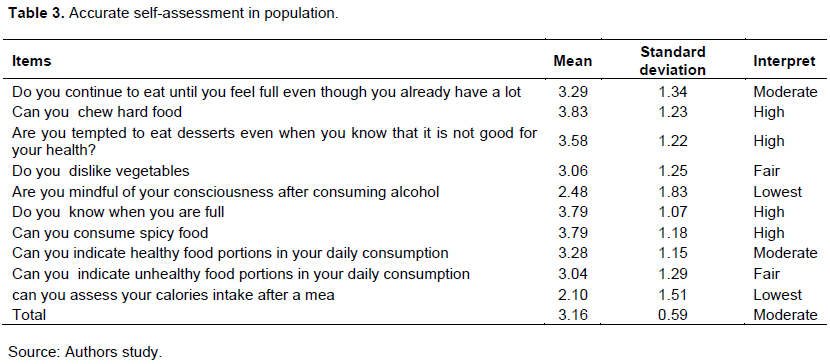
The results from the accurate self-assessment test are as follows. The samples were able to accurately assess themselves high for these questions: “Can you chew hard food” (3.83)? “Do you know when you are full” and “Can you consume spicy food” (3.79)? “Are you tempted to eat desserts even when you know that it is not good for your health” (3.58)?
For the following questions, the samples assessed themselves at the intermediate level (3.29, 3.28 and 3.04, respectively): “Do you continue to eat until you feel full even though you already have a lot” and “can you indicate healthy and unhealthy food portions in your daily consumption”? However, the samples were able to assess themselves poorly for the following questions (2.48 and 2.01): “Are you mindful of your consciousness after consuming alcohol” and “can you assess your calories intake after a meal”? The results are shown in Table 3.
Self-confidence
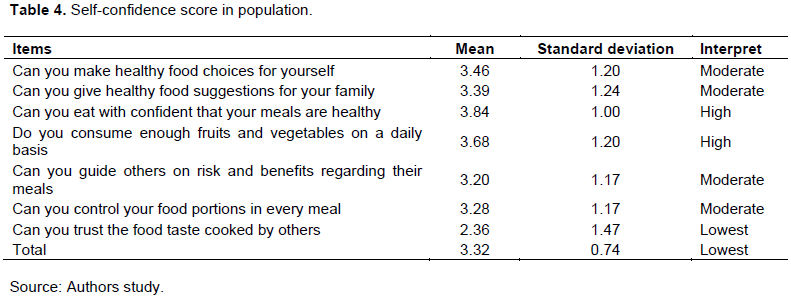
The results from the self-confidence test show that the samples were highly confident that their meals were healthy and that they consume enough fruits and vegetables on a daily basis (average of 3.84 and 3.68, respectively). However, the results reveal that the samples were only moderately confident of their food choice and their ability to make healthy food choices for themselves and their family at the average of 3.46 and 3.39. Similarly, the confidence levels of their own ability to control food portions and to guide others on risk and benefits of their meals were at mid-way (average of 3.28 and 3.20). Lastly, their confidence levels were lowest (2.36) for not trusting the food taste cooked by others. The results are depicted in Table 4.
Consumption behavior
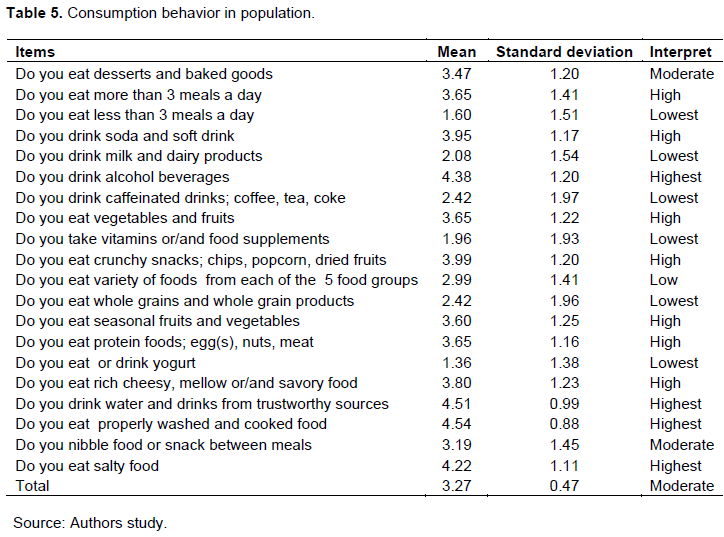
The consumption behavioral data show the highest consumption of properly washed and cooked food (3.54), water and drinks from trustworthy sources (3.51), alcohol beverages (3.48) and high sodium food (4.22) (Table 5).
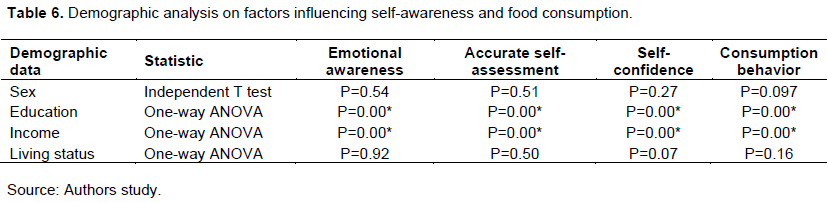
Afterwards, the personal data gathered were analyzed together with the average awareness scores including emotional awareness, accurate self-sssessment, self-confidence and consumption behavior using Independent T-test and One way ANOVA technique. The results show that education and family income had the highest effect on all 3 awareness topics shown in Table 6.
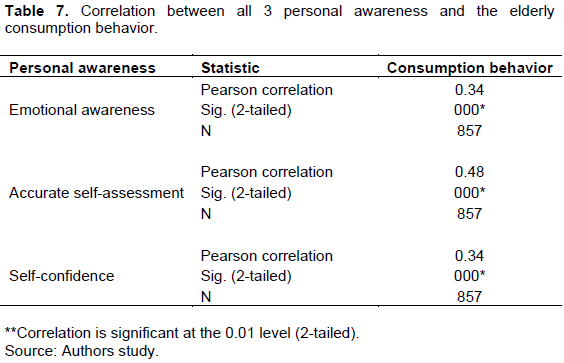
There is statistical significance and positive relationship between all 3 personal awareness and the elderly eating behavior, with significant levels at 0.00 (Table 7).
After the educational background and family income data were tested and confirmed, they were significant in statistical variance (F). Sheffe’s method was applied to compare the mean difference between the two factors and the sample’s food consumption behavior. The test result revealed that educational levels and family income both significantly had influences on how people consume food and their awareness. The average data are shown in Tables 7 to 8.
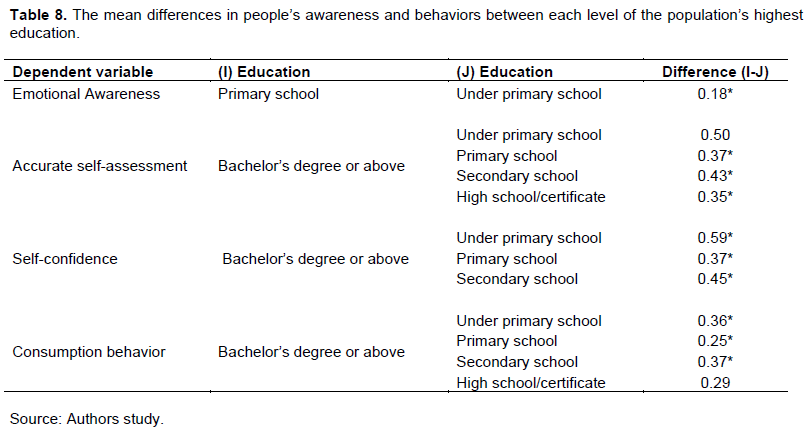
When comparing the elderly’s emotional awareness, the ones with highest education level (below elementary) had a significantly 0.18 lower mean value than the ones at elementary level. People with Bachelor’s degree or higher tend to have the highest ability to accurately assess themselves than the other groups (below primary school, primary school, secondary school, and high school or equivalent at significantly 0.50, 0.37, 0.43 and 0.35 sequentially). Similarly, people with Bachelor’s degree or higher had higher self-confidence levels (at significantly 0.59, 0.37, and 0.49 respectively) than the others (below primary school, primary school, secondary school). Likewise, food consumption behavior scores were significantly higher in Bachelor’s degree or higher group than the rest (0.36, 0.25, 0.37 and 0.29) (Table 8).
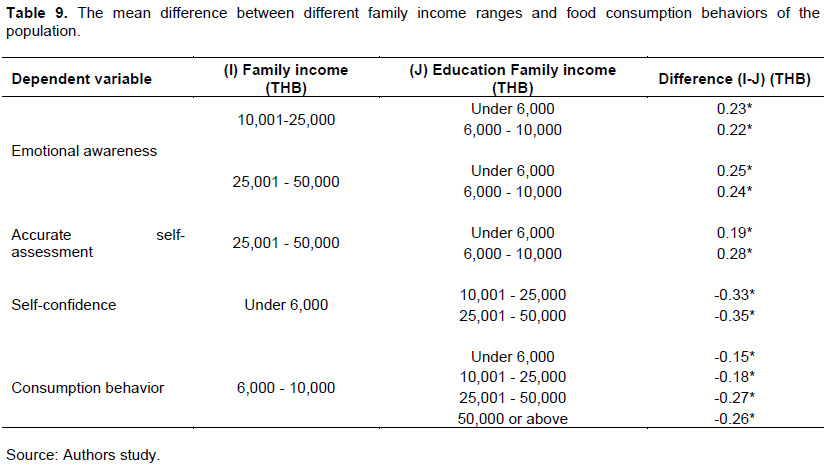
Elders with average family income in the range of 10,001 to 25,000 Baht per month had a higher emotional awareness (month (significantly 0.23 and 0.22, respectively) than those with 6,000 Baht and 6,000-10,000 Baht per.
Regarding accurate self-assessment, the elderly with average family income in the range of 25,001 to 50,000 Baht per month had a significantly higher mean scores (at significantly 0.23 and 0.24, respectively) than the ones with their income lower than 6,000 Baht and 6,000-10,000 Baht per month.
Similarly, the group with the least monthly income (less than 6,000 Baht per month) had the lowest self-confidence compared to the ones with average family income in the range of 10,001 to 25,000 Baht and 25,001 to 50,000 Baht per month. The mean differences were significantly 0.33 and 0.35.
However, when comparing the elderly with average family income in the range of 6,000-10,000 Baht to the other groups, their food consumption behaviors were scored at the lowest. The mean differences in comparison with the less than 6,000 Baht/month, 10,001-25,000, 25,001-50,000 and over 50,000 Baht per month were significantly 0.15, 0.18, 0.26, and 0.26 accordingly (Table 9).
DISCUSSION
An interesting finding in the research paper is that the elders personal factors are associated with their food consumption behaviors. This creates a further understanding of how internal and external factors could influence the elderly's dietary behaviors. The results from this research are that personal factors including the highest educational level and average family income do have a direct influence on one's consumption behavior. Likewise, elders’ emotional awareness as well as their self-assessment and confidence also have a positive relationship with their food consumption behavior.
The demographic data have an effect on the elders’ eating behaviors in this research, conforming to sakoolnamarka et al. (2021) who studied the Correlation between Nutritional Awareness and Food Consumption Behaviors of The Elderly in Nakhon Nayok Province in all 3 aspects. sakoolnamarka et al. (2021) concluded that the highest educational level and the elderly’s nutritional awareness are directly related. Also, family income influenced how elders accurately assess themselves.
The result regarding the positive relationship between the elderly’s family income and their diets correspond to the work of Myres and Kroetsch (1978)on “The Influence of Family Income on Food Consumption Patterns and Nutrient In take in Canada”. They stated that “Mean intake of nutrients increased with increase in income in all physiological groups”. Moreover, Ren et al. (2019), in studying “Family income and nutrition-related health: Evidence from food consumption in China’’, had similar result. Income-BMI gradients tend to increase along with income percentiles, and income has a significantly positive impact on BMI and overweight for the male sample; but it has no significant impact on the female sample.
Worsley et al. (2004)discovered in their “The relationship between education and food consumption in the 1995 Australian National Nutrition Survey” study that higher education is associated with the regular consumption of a wider variety of foods. Our study also gives out a matching result. A person with a higher education tends to do better with his diet.
Emotional awareness along with accurate self-assessment and self-confidence are also positively related to the elders’ consumption behavior. The results corresponded with Sakoolnamarka et al. (2021)study on ‘Correlation Between Nutritional Awareness and Food Consumption Behaviors of the Elderly in Nakhon Nayok Province’. Sakoolnamarka stated in her study that “The emotional awareness, accurate self-assessment, and self-confidence were positively correlated with food consumption behaviors.” In addition, the study of Rabiei et al. (2013) on “Understanding the relationship between nutritional knowledge, self-efficacy, and self-concept of high-school students suffering from overweight” also revealed there is direct relationship between nutritional knowledge, self-concept, and self-efficacy.
To focus on the relationship between emotional awareness and consumption behavior, Magnus (2016)reported the influence of emotional awareness on behaviors and abilities. He stated that a person’s emotional awareness has a direct impact on the ability to improve one’s behavior in every aspect. Likewise, Shouse and Nilsson (2011), in their study on “Self-Silencing, Emotional Awareness, and Eating Behaviors in College Women”, discovered that emotional awareness moderated the relationships between self-silencing and disordered eating and intuitive eating.
Many researches have proved similar results for accurate self-assessment factor. Schroder et al. (2013)reported “Habitual self-control: A brief measure of persistent goal pursuit.” Junger and van Kampen (2010)studied “Cognitive ability and self-control in relation to dietary habits, physical activity and bodyweight in adolescents” and Kennett and Nisbet (1998)studied “The influence of body mass index and learned resourcefulness skills on body image and lifestyle practices”. These studies have shown that self-regulation of eating is likely to interact with biologically-mediated variation in appetite, and as a consequence, general self-regulation questionnaires show only modest associations with healthy eating behaviors and weight control.
The self-confidence factor also corresponds to previous studies. Berman (2006)studied the relationship between eating self-efficacy and eating disorder symptoms in a non-clinical sample; it is concluded it has relationship with eating behaviors and weight-loss in clinical samples. Sawdon et al. (2007)studied “The relationship between self-discrepancies, eating disorder and depressive symptoms in women”; they disclosed that eating disorder and depressive symptoms were correlated with a number of self-discrepancies. Neha (2017)studied "The Role of Body Image, Dieting, Self-Esteem and Binge Eating in Health Behaviors" and found that the relationship between body image and dieting was mediated by self-esteem. Furthermore, the relationship between dieting and self-esteem was mediated by binge eating.
In this study, the demographic data which are the educational level, family income and awareness focused in this study, are statistically and significantly related to elders’ eating behavior.
The results that the elders who graduated with bachelor degrees or higher had the best consumption behavior indicate that educational level is highly involved in a person’s diets. Therefore, promoting adequate education in communities would improve the population’s dietary behavior. The current young adults would become better and educated elders with better health and knowledge.
However, the financial factor came out unexpectedly in this study. Elders with higher income did not show any significantly higher scores in both awareness and eating behavior aspects. There have been numerous studies regarding the influence of money on people’s lifestyles. Even though people with no financial restrictions are able to determine and weigh the advantages and disadvantages of their diets, their decisions are still disagreeable. The spread of the novel COIVD-19 virus is one of the obvious examples. The number of infected people was continuously high in the area with high-income people who did not agree that the vaccines are safe (Wellcome Trust, 2018).
Now that we have learned how personal awareness affects dietary behavior, we should encourage the society to help the elderly create more nutritional awareness by not only educating them with nutritional knowledge, but also arranging an entertaining activity that would bring self-awareness, accurate self-assessment and self-confidence.
The result from this study helps us understand the relating coefficients regarding the elderly in a small city.
CONCLUSION
(1) There is a significant correlation between awareness factors (emotional awareness, accurate self-assessment and self-confidence) and food consumption behavior (p=0.00).
(2) Personal factors (highest education level and family income) have a positive influence on food consumption behavior with significance (p=0.00).
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abate T, Mengistu B, Atnafu A, Derso T (2020). Malnutrition and its determinants among older adults people in Addis Ababa, Ethiopia. BMC Geriatrics 20(1):498. |
|
|
Benjamas N. (2008). Psycho-social factors related to self-care behavior and happiness of the senior citizen club members in the hospitals under medical service department, Bangkok metropolis. Bangkok: Srinakharinwirot University, Graduate School. |
|
|
Berman ES (2006). The relationship between eating self-efficacy and eating disorder symptoms in a non-clinical sample. Eating Behaviors 7(1):79-90. |
|
|
Boscatto EC, Duarte Mde F, Coqueiro RS, Barbosa AR. (2013). Nutritional status in the oldest elderly and associated factors. Revista da Associação Médica Brasileira 59(1):40-47. |
|
|
Damayanthi H, Moy FM, Abdullah KL, Dharmaratne SD. (2018). Health related quality of life and its associated factors among community-dwelling older people in Sri Lanka: A cross-sectional study. Archives of Gerontology and Geriatrics 76:215-220. |
|
|
GBD 2017 Diet Collaborators (2019). Health effects of dietary risks in 195 countries, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet 393:1958-1972. |
|
|
Goleman D (1995). Emotional intelligence. New York: Bantam Books Publishing. |
|
|
Gunsam PP, Murden SW (2016). Factors Influencing Food Choice in the Elderly Mauritian Population. University of Mauritius Research Journal 13:179-191. |
|
|
Healthy Diet for Elderly (2017). Guideline for food consumption to make good health in Thai Elderly. |
|
|
Junger M, van Kampen M. (2010). Cognitive ability and self-control in relation to dietary habits, physical activity and bodyweight in adolescents. International Journal of Behavioral Nutrition and Physical Activity 7(1):22. |
|
|
Kennett DJ, Nisbet C (1998). The influence of body mass index and learned resourcefulness skills on body image and lifestyle practises. Patient Education and Counseling 33(1):1-12. |
|
|
Kitkamolsawet G (2017). Factors influencing food consumption behavior beneficial and damaging to dental health in elderly in Muang District, Nakhon Nayok. (senior project). Bangkok: Srinakharinwirot University. |
|
|
Magnus OI (2016). Emotional Self Awareness and Information Literacy Competence as Correlates of Task Performance of Academic Library Personnel. Library Philosophy and Practice (e-journal) 1370:1-22. |
|
|
Mazengo MC, Tenovuo J, Hausen H (1996). Dental caries in relation to diet, saliva and cariogenic microorganisms in Tanzanians of selected age groups. Community Dentistry and Oral Epidemiology 24(3):169-174. |
|
|
Myres AW, Kroetsch D. (1978). The Influence of Family Income on Food Consumption Patterns and Nutrient Intake in Canada. Canadian Journal of Public Health / Revue Canadienne de Sante'e Publique 69(3):208-221. |
|
|
Naidoo I, Charlton KE, Esterhuizen TM, Cassim B (2015). High risk of malnutrition associated with depressive symptoms in older South Africans living in KwaZulu-Natal, South Africa: a cross-sectional survey. Journal of Health, Population and Nutrition 33:19. |
|
|
National Statistical Office of Thailand. (2007). Statistic of Elderly in 2007. |
|
|
Neha MT. (2017). The Role of Body Image, Dieting, Self-Esteem and Binge Eating in Health Behaviors. (Master of Arts (MA)). Eastern Illinois University, USA. |
|
|
Rabiei L, Sharifirad GR, Azadbakht L, Hassanzadeh A (2013). Understanding the relationship between nutritional knowledge, self-efficacy, and self-concept of high-school students suffering from overweight. Journal of Education and Health Promotion 2:39. |
|
|
Ren Y, Li H, Wang X (2019). Family income and nutrition-related health: Evidence from food consumption in China. Social Science and Medicine 232:58-76. |
|
|
Sawdon AM, Cooper M, Seabrook R (2007). The relationship between self-discrepancies, eating disorder and depressive symptoms in women. European Eating Disorders Review: The Professional Journal of the Eating Disorders Association 15(3):207-212. |
|
|
Schroder KEE, Ollis CL, Davies S (2013). abitual Self-Control: A Brief Measure of Persistent Goal Pursuit. European Journal of Personality 27(1):82-95. |
|
|
Sakoolnamarka S, Lawprasert K, Larpjitkusol S, Srikan T, Chuayboon S, Rungsitanont S (2021). Correlation between Nutritional Awareness and Food Consumption Behaviors of the Elderly in Nakhon Nayok Province. Srinakharinwirot University Dental Journal 14(1):64-79. |
|
|
Shouse SH, Nilsson J (2011). Self-Silencing, Emotional Awareness, and Eating Behaviors in College Women. Psychology of Women Quarterly 35(3):451-457. |
|
|
U.S. Census Bureau (n.d.). Population Division. |
|
|
Wang X, Ouyang Y, Liu J, Zhu M, Zhao G, Bao W, Hu FB (2014). Fruit and vegetable consumption and mortality from all causes, cardiovascular disease, and cancer: systematic review and dose-response meta-analysis of prospective cohort studies. BMJ: British Medical Journal 349:4490. |
|
|
Wellcome Trust (2018). Wellcome Global Monitor (2nd ed.): UK Data Service. SN: 8466, |
|
|
Worsley A, Blasche R, Ball K, Crawford D. (2004). The relationship between education and food consumption in the 1995 Australian National Nutrition Survey. Public Health Nutrition 7(5):649-663. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


