Full Length Research Paper

ABSTRACT
This study examined knowledge and awareness regarding HIV and AIDS among pregnant women in Butwal, Nepal. Pregnant women were selected using a systematic random sampling method from the antenatal care registry at every 5th and 10th interval. Although 80% of women mentioned unprotected sexual contact as the major route of HIV transmission, only 36.7% women knew that HIV can be transmitted from the infected mothers to their babies. Approximately half of the women (53.0%) mentioned foreign employees as a vulnerable group for HIV infection, followed by multiple sexual partners (41.0%), intravenous drug users (40.0%), commercial sex workers (35.0%), and labor migrants (25.0%). Although 71.7% women knew that proper use of a condom could easily prevent HIV transmission, few women knew other preventive ways (such as use of disposable syringes). Implementation of effective health education programs on HIV infection is needed for pregnant women in the study area.
Key words: Education, awareness, HIV and AIDS, pregnant women.
INTRODUCTION
Human Immunodeficiency Virus (HIV) infection or Acquired Immunodeficiency Syndrome (AIDS), which has a high rate of case fatality and lacks curative treatment, is one of the most serious global public health challenges. The first case of HIV and AIDS was reported in the United States of America in 1981 (Global Factsheet HIV/AIDS, 2014). According to UNAIDS factsheet, in 2018 there were 37.9 million people living with HIV infection (36.2 million adults and 1.7 million children) worldwide. Among them, 8.1 million did not know they have HIV infection. In the case of women, approximately 6000 young women age between 15 and 24 years of age became infected with HIV every week. Young women aged 15-24 years are twice as likely to be living with HIV infection compared to men at the same age group (Global Factsheet HIV/AIDS, 2019). Similarly, around 770,000 people died globally from AIDS related illness in 2018. Most of the risk behaviors are attributable to HIV infections in adults; however, a child becomes infected from their mother most of the time (Karir et al., 2019). Women are not only in high risk group to acquire HIV infection; they have the unique role of transferring the infection to child.
The presence of HIV infection in reproductive age requires special attention as HIV transmission from mother to child during pregnancy, labor, and delivery, or breastfeeding (known as perinatal transmission) is the most common route of HIV infection in children (Nduati et al., 2000). The perinatal transmission is responsible for as many as 90% of HIV infections among children (Nduati et al., 2000). Furthermore, HIV and AIDS is linked to high rates of adverse pregnancy outcomes, such as intrauterine growth restriction, preterm delivery, eclampsia, other sexually transmitted diseases, and infections (Patil et al., 2011). HIV and AIDS do not only affect the health of an individual, it also impacts on households, communities, and economic growth of the nations. The largest number of people with HIV/AIDS resides in low- and middle-income countries. In 2018, 70% (25.6 million) were in African countries, 16% (5.9 million) in Asia and Pacific regions and 6% (2.2 million) in Western and central Europe and North America (Global factsheet, 2018).
Nepal is a landlocked country of South Asia which boarders three sides (East, West and South) with India and North with People’s Republic of China. It is a developing country with human development index of 0.548 and life expectancy of 69.9 years having approximately 28 million populations (CBS, 2015; UNDP, 2015).
There are many factors that increase the national vulnerability to HIV infection in Nepal amongst which poverty, unemployment, low literacy, internal and cross boarder migration, gender inequality, injecting drug use, commercial sex work and sex trafficking, stigma related to sex and sexuality (Bam et al., 2013) are few of them.
In Nepal, the first case of HIV and AIDS was officially reported in 1988 (National Center for AIDS and STD Control, 2013) and the number of cases with HIV and AIDS was in an increasing trend for 20 years (Patil et al., 2011; NCASC, 2013). In 1988, the number of people infected with HIV were 4 (National Center of AIDS and STD Control, Kathmandu 2013), which reached 70,000 in 2007 (DHS, 2013). However, numbers appear to be decreasing currently as the estimated number of people living with HIV was 31,020 and 304 were pregnant women in 2017 (NCASC, 2014). However, given the limitations of Nepal’s public health surveillance system, the actual number of infections is thought to be much higher. In developing countries like Nepal, HIV and AIDS transmission is becoming a great public health problem due to the lack of information about HIV and AIDS prevention (Global FactSheets HIV/AIDS, 2014; WHO/UNAIDS, 2019). In a place like Rupandehi district, this is specifically a problem, due to the proximity to the border site of India, high circular and seasonal migration pattern, unsafe sexual practices among sexual workers during out migration period, lack of knowledge about prevention of mother to child transmission (PMTCT) program and unavailability of sexually transmitted infections treatment facilities in rural areas (Poudel et al.,
2004; Paudel et al., 2016; World Bank, 2019). Since HIV infection is preventable, HIV and AIDS awareness remains of great importance and necessity. It has been observed that most of the women in the community do not have knowledge and awareness about HIV/AIDS as well as its prevention and management.
Women’s adequate knowledge and awareness on HIV infection has a crucial role on prevention of HIV transmission, specifically in socially and economically disadvantaged communities (Sama et al., 2012; Karim et al., 2010). Women’s awareness about HIV and AIDS can empower them in changing their sexual behaviors and in utilizing preventive measures of HIV and AIDS leading to prevention of mother to child transmission (MTCT) of HIV (Sama et al., 2012). Thus, this research aims to examine knowledge and awareness regarding HIV and AIDS among pregnant women in Butwal, Rupandehi district, Nepal.
MATERIALS AND METHODS
This is a descriptive study using primary data sources. The study was conducted in two hospitals: Lumbini Zonal hospital (a Government hospital) and Siddhartha Children and Women hospital (a private hospital) in Butwal Municipality at Rupandehi district, Nepal. Rupandehi district is one of the seventy-seven districts of Nepal, which belongs to Lumbini Zone. Butwal is a big town in the Southern part of Nepal in Rupandehi district, in Lumbini zone, which is 240 km west of Kathmandu and 22 km north of Bhairahawa at the northern ridges of Terai region. Rupandehi district, specifically Butwal has highway connections to the Indian border and it is also a hub for migrant workers from the Western Nepal.
Systematic random sampling technique was used for the selection of study sample. Newly registered pregnant women attending antenatal clinic (ANC) aged between 15 to 35 years, during the study period between April 15 and 30, 2014 were identified. Then, every 5th and 10th registered pregnant women were selected. Out of the total 455 pregnant women identified, a total sample of 60, that is, 30 sample from each of the two hospitals, were selected. Structured interview questionnaires were developed, piloted, and finalized to collect necessary information related to demographic information, socioeconomic characteristics, educational level, occupational information and information of knowledge and awareness of HIV and AIDS of pregnant women. The questionnaire included information on sources, causative agents, modes of transmission, signs and symptoms, and preventive measures of HIV and AIDS and vulnerable groups for HIV and AIDS. The structured questionnaire was administered by means of face to face interview after consent was obtained. Pregnant women were asked about their knowledge and awareness of HIV and AIDS during pregnancy with the help of female health professionals working in the same clinic. The study was approved by the Research Ethics Committee of Tribhuvan University, Lumbini Zonal Hospital, and Siddhartha Children and Women Hospital. A descriptive statistical analysis was performed to interpret the data. Data are presented as frequency and percentage in table.
RESULTS
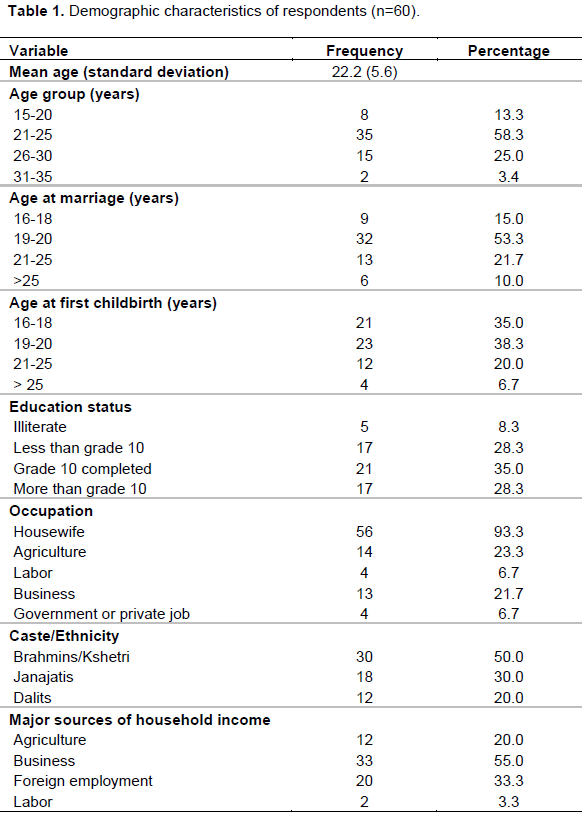
As shown in Table 1, mean age of pregnant women was 22.2 years (±5.6), with maximum (58.3%) of the pregnant women (5 belonging to the age group between 21 and 25 years). More than half (53.3%) of the women got married at the age of 19-20 years and the majority (38.3%) of women had their first baby at 19-20 years of age followed by (35.0%) at the age of 16-18 years and (20.0%) at the age of 21-25 years of age. Also, 8.3% were illiterate (that is, unable to read and write). Most (93.3%) of the pregnant women were housewives, followed by agriculture (23.5%), business (21.7%), government and private job (6.7%) and labor (6.7%). Brahmin/Kshetri were the main ethnic group, which represented half (50%) of the total population of the study area. The majority (55.0%) of the pregnant women’s source of household income was business, followed by (33.3%) foreign employment, and (20%) agriculture.
As shown in Table 2, most of the respondents (80.0%) have heard about HIV/AIDS. The highest proportion (63.3%) of respondents said that they got information about HIV and AIDS from teachers when they were at school. The second major source of information on HIV and AIDS was friends (46.7%) and the third source was radio (43.3%), followed by television (31.7%), newspapers (28.3%) and family members (23.3%), respectively.
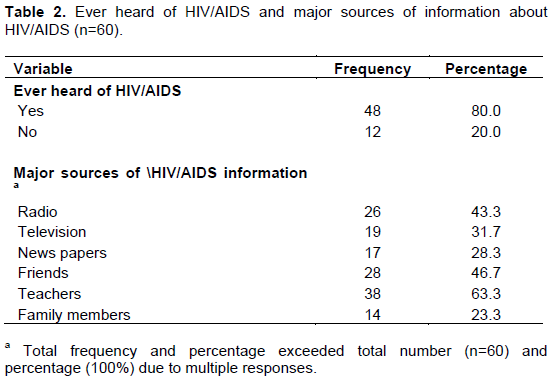
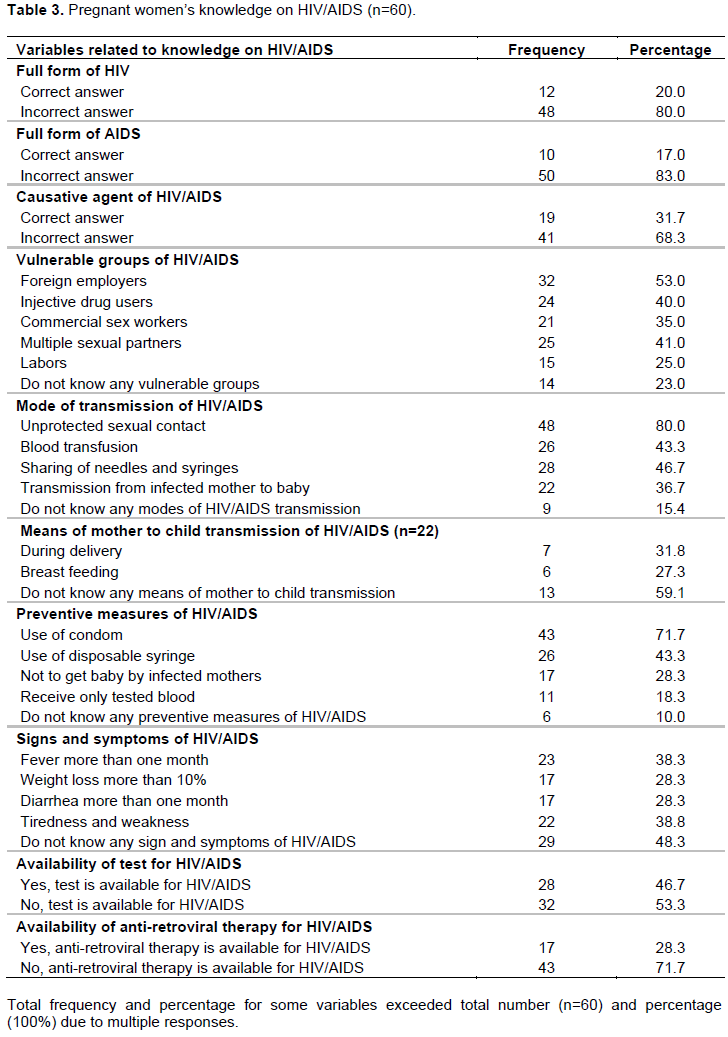
Table 3 illustrates respondents’ knowledge on HIV and AIDS. Four out of five (80.0%) of pregnant women were unable to tell the full form of HIV and AIDS. The majority (68.3%) of the pregnant women were unable to tell the causative agent of the HIV and AIDS. More than a half (53.0%) of the respondents mentioned that foreign employees are the most vulnerable groups for HIV and AIDS, followed by 41.0% who believed it was multiple sexual partners, 40.0% opined intravenous drug user, 35.0% claimed commercial sex workers and 23.0% said labor migrants. Similarly, the majority (80%) of the respondents mentioned unprotected sexual contact as a mode of HIV and AIDS transmission, followed by (46.7%) sharing needles (43.3%) blood transfusion, and (36.7%) from infected mothers to babies as modes of HIV and AIDS transmission. Approximately half (48.3%) of the respondents did not know any signs and symptoms of HIV and AIDS. More than two-third (71.7%) of respondents mentioned the use of condom as a way to prevent HIV and AIDS followed by (65.0%) awareness program, (43.3%) use of disposable syringe, (28.8%) not getting baby from infected mother, but a few were aware of other preventive measures such as receiving only tested blood.
DISCUSSION
Main finding
This study examined knowledge and awareness on HIV and AIDS among the pregnant women in Butwal, Rupandehi district, utilizing the primary data collected from these women. Most of the pregnant women were young, married at a young age, and were housewives. Business was the main source of household income, whereas, foreign employment ranks the second source of household income for pregnant women. Most of the pregnant women got information from teacher during their school time. Importantly, this was a hospital-based study and none of the pregnant women mentioned health workers as a source of information about HIV and AIDS. Many pregnant women did not know the signs and symptoms of HIV and AIDS. Approximately, half of all the pregnant women knew foreign employees as a vulnerable group of HIV and AIDS, and the percentage of women who knew other vulnerable groups of HIV and AIDS (such as commercial sex worker, multiple sexual partner, and injective drug user) was even lower. Significant percentage of women mentioned unprotected sexual contact as a major mode of transmission of HIV and AIDS, but very few pregnant women mentioned infected mother to baby (that is, MTCT) as a mode of transmission of HIV and AIDS. There were significant percentage of women who knew condom use during sexual activities as a way to prevent from HIV and AIDS. Nevertheless, few women knew other preventive ways for HIV and AIDS transmission (such as the use of disposable syringes and receiving only tested blood).
The highest proportions of pregnant women heard about HIV and AIDS from the teacher during their high school time. This indicates that school education is the most reliable and easy source of gaining information about HIV and AIDS for the young pregnant women. Revision of school curriculum and incorporating sexual health including HIV, AIDS, and sexually transmitted diseases (STDs) and health-related topics in high school level may be a first step to improving knowledge and awareness on HIV and AIDS. Similarly, information about HIV and AIDS may easily be transmitted through peers and friend groups. Women can maintain friendly trustworthy relationship among peers; thus, they can share their knowledge and private matters among peers. The government’s health service providers and private organizations who are working on HIV and AIDS programs can also empower women through the health education. Similarly, local and national Radio and Television channels can play a huge role in disseminating knowledge about HIV and AIDS to the general population.
This study showed that there is lack of education of pregnant women from ANC clinic as none mentioned they got information from health care workers. So, it is crucial to start health education on HIV and AIDS at the ANC clinic to provide basic knowledge about HIV and AIDS that encourages pregnant women for laboratory tests related to this infection as well as prevention and management of HIV/AIDS While some of our study findings are similar with other studies, some of our study findings are different or show lower percentage of pregnant women who have knowledge of HIV and AIDS than in other studies conducted in Nepal (Pandey, 2013; Acharya et al., 2017). Similar to our study, these two studies also found that none of the women mentioned health professionals as a source of information of HIV and AIDS (Pandey, 2013; Acharya et al., 2017). The major sources of information of HIV and AIDS in these studies were Radio, Television, and Newspapers (Pandey, 2013; Acharya et al., 2017). Similar to our study, the majority of women in both studies said that HIV and AIDS is transmitted from unprotected sexual contact (Pandey, 2013; Acharya et al., 2017). However, the percentage of pregnant women who mentioned HIV and AIDS is transmitted from unprotected sexual contact with infected person was different across studies [88.9% in a study conducted by Pandey (2013); 100% in a study conducted by Acharya et al. (2017); and 80.0% in our study]. Similarly, the percentage of women who mentioned transmission of HIV and AIDS from infected mother to child (that is, MTCT) was higher in a previous study (70.4%) compared to ours (36.7%) (Pandey, 2013). Additionally, the percentages of women who mentioned the vulnerable groups and preventive measures for HIV and AIDS in a previous study were different compared to our study. In a previous study, 83.3% of pregnant women said that commercial sex workers and having multiple sex partners are high-risk groups for HIV and AIDS, and 77.8% of pregnant women said that HIV and AIDS can be prevented by avoiding multiple sex partners (Pandey, 2013). The part of these differences might have been related to the fact that these studies used a different study method (that is, non-probability purposive sampling technique) than ours (systematic random sampling technique) (Pandey, 2013; Acharya et al., 2017). Furthermore, part of these differences might have been related to the different study locations and different hospitals. Although these studies were also conducted in hospital-based ANC clinics, these studies were conducted in tertiary level government hospitals in Kathmandu: Bir Hospital and at Paropakar Maternity and Women’s Hospital. It is also important to note that women who knew HIV can be transmitted from mothers to babies in our study sample (36.7%) was lower than in the National Demographic Health Survey 2016 (47.0% of general women and 51.0% of men) (Ministry of Health Nepal, 2017), indicating the excess risk in our pregnant sample.
Our study findings are similar to the studies conducted in other countries, such as China and India (Maimaiti and Andersson, 2008; Jahan et al., 2017). In these studies, the majority of pregnant women mentioned sexual contact and injection as routes of transmission, whereas MTCT was mentioned as a least route of transmission (Maimaiti and Andersson, 2008; Jahan et al., 2017). Similarly, the use of condoms was mentioned as a major preventive measure (Jahan et al., 2017). The percentage of women knowing the signs and symptoms of HIV and AIDS was low in the study conducted in China, similar to our study finding (Maimaiti and Andersson, 2008).
A study carried out by Narayani et al. (2013) in Mangalore India concluded that the awareness and knowledge on HIV/AIDS among pregnant women attending ANC checkup is superficial, which is equivalent to our study.
A study on pregnant mother seeking ANC in Vimsar Burla in India conducted by Karir et al. (2019) concluded that only 30.7% women said that AIDS can be treated; majority (60.7%) did not know if there is treatment, and 54% of respondents did not know about mother to child transmission. In our study, 36.7% pregnant mother knew that AIDS can be transmitted by infected mother to baby (Karir et al., 2019).
Our study found few women who knew that HIV and AIDS could be transmitted from infected mothers to babies. Although our study did not assess details of knowledge on MTCT and its preventive measures, the observed study findings are important as the literature shows that compared to pregnant women who do not have sufficient knowledge on HIV and AIDS, those who have sufficient knowledge on HIV and AIDS are 3 times more likely to have better knowledge on MTCT of HIV (Abtew et al., 2016). PMTCT and reducing the new HIV infection depends on accurate and up-to-date knowledge of childbearing women including pregnant women about HIV and AIDS including the modes of HIV transmission, vulnerable groups, and preventive measures, and depends on their preventive practices (Sama et al., 2012; Karim et al., 2010). Women with lack of awareness on HIV and AIDS such as modes of transmission, vulnerable groups, and preventive measures indicate that these women are more susceptible in getting HIV infection from their husband or sex partners (with HIV infection) and they are also a high-risk group in transmitting HIV infection to their babies (that is, MTCT).
The observed limited knowledge of pregnant women on HIV and AIDS may suggest the ineffectiveness of efforts, such as counseling, health education, and health promotion services provided by ANC clinics, which informs us of an opportunity for taking appropriate interventions in the management of women during ANC visits so as to increase knowledge and awareness of pregnant women to promote primary prevention or PMTCT of HIV. Additionally, the observed limited knowledge would have been related to the fact that a significant number of women were young and are housewives, which might have minimized their access to information on HIV and AIDS (Yaya et al., 2016; Mahra et al., 2014). Another reason could be related to the culture of Nepal, where women have limited decision-making powers and are predominately discouraged to access or gain knowledge or to discuss the issues related to HIV and AIDS (Wasti et al., 2011). Specifically, women who are confined within the household chores are less empowered; thus, they are mostly affected by the sociocultural practices and beliefs (Carey and Maisto, 1997; Fisher, 1992).
This study attempted to gain an understanding of the knowledge and awareness of young pregnant women regarding HIV and AIDS. While the study in this area is important specifically in this population, given the importance of prevention of HIV infection on the health of mothers and babies, the findings of this study should be interpreted with caution. The research was carried out in two hospitals of Butwal municipality; therefore, the findings of this study cannot be generalized to the women who do not come for the ANC check-ups. The women attending ANC check-ups and who do not come for ANC check-ups are more likely to be different. In fact, women who do not come for ANC check-ups are more likely to be socio-economically disadvantaged and socio-economically disadvantageous women are associated with having less knowledge on HIV and AIDS than women who attend ANC check-up (Abtew et al., 2016; Yaya et al., 2016; Shrestha, 2013). This study could not examine whether HIV and AIDS awareness was different or affected by age, education, income, and occupation status of pregnant women due to small sample size (leading to small or no cell count in the cross tabulation). This study does not provide information about reasons for not having awareness about HIV and AIDS and ways to improve awareness about HIV and AIDS among young pregnant women. Future study is needed for this purpose. The understanding about the reasons for not having enough awareness about HIV and AIDS and the ways to improve the awareness may help to implement effective educational interventions to improve young pregnant women’s knowledge and awareness on HIV and AIDS.
Assessment of knowledge on MTCT of HIV and its prevention is an important aspect of the study that was conducted among pregnant women. While this study assessed whether pregnant women knew the different modes of transmission of HIV and AIDS, this study did not assess detailed knowledge on MTCT. The assessment of knowledge of MTCT may include: how and when MTCT could occur (during pregnancy, during delivery, during breast feeding), means to reduce or prevent the risk of MTCT (such as antiretroviral treatment drugs, safe delivery, breast feeding), and existing interventions to minimize or prevent MTCT (Abtew et al., 2016). Future studies addressing this knowledge gap may assist in strengthening the efforts to increase knowledge of pregnant women on MTCT of HIV and the PMTCT services.
CONCLUSION
Overall, the majority of pregnant women did not have knowledge regarding HIV and AIDS including different modes of transmission, high-risk groups, and preventive measures of HIV and AIDS. We recommend more efforts to be extended on improving women's knowledge on HIV and AIDS. Importantly, this study was conducted in ANC and none of the pregnant women studied mentioned health workers as a source of information about HIV and AIDS and very few women knew MTCT as a mode of transmission of HIV and AIDS. The findings indicate an important opportunity to improve the education program regarding HIV and AIDS for pregnant women in light of PMTCT. The study recommends future studies to assess pregnant women’s knowledge focusing on MTCT of HIV and AIDS, its preventive measures and the gaps in PMTCT services in ANC clinics. The findings will be helpful for identifying strategies for improving the knowledge on MTCT and for strengthening the PMTCT services.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abtew S, Awoke W, Asrat A (2016). Knowledge of pregnant women on mother-to-child transmission of HIV, its prevention, and associated factors in Assosa town, Northwest Ethiopia. HIV/AIDS-Research and Palliative Care 8:01-107. |
|
|
Acharya R, Acharya T, Devkota R (2017). Knowledge regarding prevention of mother to child transmission of HIV/AIDS among antenatal mothers in Nepal. Journal of College of Medical Sciences-Nepal 14(1):44-48. |
|
|
Bam K, Thapa R, Newman MS, Bhatt LP, Bhatta SK (2013) Sexual Behavior and Condom Use among Seasonal Dalit Migrant Laborers to India from Far West, Nepal: A Qualitative Study. PLoS ONE 8(9):e74903. |
|
|
Carey MP, Maisto SA (1997). Enhancing motivation to reduce the risk of HIV infection for economically disadvantaged urban women. Journal of Consulting and Clinical Psychology 65(4):531-541. |
|
|
Central Bureau of Statistics. Nepal in Figure. Government of Nepal. 2015. |
|
|
Department of Health Services, DHS (2013). HIV/AIDS and STD control: Annual Report (2010/2011). Department of Health Services, Ministry of Health and Population, Government of Nepal. |
|
|
Fisher JD (1992). Changing AIDS-risk behavior. Psychological Bulletin 111(3):455-474. |
|
|
Global HIV & AIDS Statistics (2019). Fact Sheet. Joint United Nations Programme on HIV/AIDS 2019. |
|
|
Global Fact Sheets HIV/AIDS (2014). |
|
|
Ministry of Health Nepal (2017). Country progress report Nepal: to contribute to global AIDS monitoring report 2017. Government of Nepal, Ministry of Health, National Centre for AIDS and STD Control. |
|
|
Jahan U, Verma K, Gupta S, Dwivedi S, Yadav A (2017). Awareness, knowledge and attitude of pregnant women towards HIV/AIDS in tertiary care hospital: A community-based study. International Journal of Advanced Research 5(8):494-500. |
|
|
Karim QA, Sibeko S, Baxter C (2010). Preventing HIV infection in women. A Global health imperative. Clinical Infectious Diseases 50(S3):S122-S129. |
|
|
Karir Shilpa, Smita Kumari Panda, Sadhu Charan Panda. Knowledge regarding HIV/AIDS and mother to child transmission issues among women seeking antenatal care in Vimsar, Burla. International Journal of Medical and Biomedical Studies 2019. Volume 3, Issue 5:117-224 |
|
|
Mahra B, Bhattar S, Bhalla P, Rawat D (2014). HIV/AIDS awareness among VCT clients. A cross-sectional study from Delhi, India. BioMed Research International. 1-7; |
|
|
Maimaiti R, Andersson R (2008). Awareness and attitudes about HIV among pregnant women in Aksu, Northwest China. The Open AIDS Journal 2:72-77. |
|
|
Ministry of Health (2017). Nepal; New ERA; and ICF. Nepal Demographic and Health Survey 2016. Ministry of Health, Nepal. |
|
|
Narayani B, Shakuntal H. Effectiveness of teaching programme on knowledge, attitude and practices regarding the HIV/AIDS among pregnant women in Lady Goshen Hospital, Mangalore Karnataka. Journal of Evolutional Medicine and Dental Science 2(25):4548-53 |
|
|
National Centre for AIDS and STD Control (2013). Control. Cumulative HIV/AIDS situation of Nepal Kathmandu: National Centre of AIDS and STD Control. |
|
|
NCASC (2014). NCfAaSC. Country progress report on HIV/AIDS Response. Nepal: Ministry of Health and Population, National Centre for AIDS and STD Control (NCASC); 2014. |
|
|
Nduati R, John G, Mbori-Ngacha D (2000). Effect of breastfeeding and formula feeding on transmission of HIV-1: a randomized clinicaltrial. Journal of the American Medical Association 283:1167-74. |
|
|
Pandey N (2013). Knowledge of pregnant women regarding HIV/AIDS. Journal of Chitwan Medical College-Nepal 3(5):18-21. |
|
|
Patil S, Bhosale R, Sambarey P, Gupta N, Suryavanshi N, Sastry J, Bollinger RC, Gupta A, Shankar A (2011). Impact of maternal human immunodeficiency virus infection on pregnancy and birth outcomes in Pune,India. AIDS Care 23(12):1562-9. |
|
|
Paudel T, Singh N, Banjara MR, Kafle SP, Gimire YC, Pokharel BR, Rawal BB, Badal K, Chaulagain M, Pendse R, Ghimire P (2016). Epidemiology of HIV, programmatic progress and gaps in last 10 years in Nepal. Journal of Virus Eradiation 2(4):35-40. |
|
|
Poudel KC, Jimba M, Okumura J, Joshi AB, Wakai S (2004). Migrants's risky sexual behaviors in India and at home in far western Nepal. Tropical Medicine and International Health 9(8):897-903. |
|
|
Sama CB, Feteh VF, Tindong M, Tanyi JT, Bihle NM, Angwafo FF, III. Prevalence of Maternal HIV infection and knowledge on mother-to-child transmission of HIV and its prevention among antenatal care attendees in a rural area in northwest Cameroon. PLoS ONE 12(2):e0172102. |
|
|
Shrestha G (2013). Factors related to utilization of antenatal care in Nepal: A generalized linear approach. Journal of Kathmandu Medical College 2(4):69-74. |
|
|
The World Bank (2019). HIV/AIDS in Nepal. |
|
|
Wasti SP, Randall J, Simkhada P, Teijlingen EV (2011). In what way do Nepalese cultural factors affect adherence to antiretroviral treatment in Nepal. Health Science Journal 5(1):37-47. |
|
|
WHO/UNAIDS (2019). HIV in pregnancy: A review. |
|
|
Yaya Sanni, Bishwajit Ghose, Danhoundo G, Shah V, Ekholuenetale M (2016). Trend and determinants of HIV/AIDS knowledge among women in Bangladesh. BMC 16:812. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


