Full Length Research Paper

ABSTRACT
The rampant practice of self-medication is indicative of very strong existing push and pulls factors. These factors could be economic, social or systemic. Despite having some beneficial effects, self-medication has life-threatening consequences. This study was aimed to determine the factors which push users to medicine sources or factors at the sources which pull users. A pre-validated questionnaire was administered to participants. Data were collected and analyzed using Microsoft Excel and the results expressed as frequencies and percentages. From the total of 650 respondents, poverty was found to be the major push factor for 360 participants (55.39%), followed by unprofessionalism, friends’ advice, previous use of medicine, lack of time, and poor price regulation as others. Low cost of medicines was found to pull 402 (61.8%) users to sources of medicines for self-medication. More than 300 of the respondents found easy access to medicine and advertising as strong pull factors. Other important pull factors include quick and time-saving, proliferation of medicine vendors, hospital crowds, and inadequate prescription checks at sources of medication. Poverty is a major push factor for self-medication, further compounded by quick access to illicit sources of medication. Consequently, users get pulled to cheaper sources, which unfortunately sell poor quality medicines, lack the expertise, or do not check prescription. Price control is required to ensure that quality medicines are accessible to users. Imposing physician prescription at all medicine sales points is a crucial step to fight the deleterious consequences of self-medication. Although self-medication has some positive elements, its practice needs to be put under control to avoid grappling with long term health complications.
Key words: Self-medication, self-treatment, push factors, pull factors.
INTRODUCTION
Contrary to expectations that all patients should seek appropriate medical assistance, comply with prescriptions and be supervised by a medical doctor, (Larsson et al. 2000), self-medication remains rampant (Montgomery et al., 2011). The practice of self-medication is indicative of very strong existing push and pulls factors which influence patient behaviour in the process of seeking help and health in response to an infection or a disease condition (Agbor and Azobo, 2011; Oluwole et al., 2016). To achieve help, patients tend to look for the most accessible and, in some cases, the most affordable means (Yadav and Rawal, 2015; Aashi et al. 2016). Common approaches include taking medication without having a prescription, sharing medicines with others or using left-over medicine stored at home (Ullah et al. 2013; Shaghaghi et al. 2014). The inappropriate use of medicines with inappropriate doses, reducing treatment duration or stopping treatment when disease symptoms subside constitute other forms of self-treatment (Grigoryan et al., 2007; Shaghaghi et al. 2014; Turki et al. 2017; Alhomoud et al. 2017).
Self-medication is self-driven use of prescription medication by patients or individuals on his/her own initiative with or without therapeutic intent (Ullah et al., 2013; Darshana, 2014; Saber et al., 2015; Hitesh et al., 2018). It also refers to the use of nonprescription medicines (Ansam, 2007; Osemene and Lamikanra 2012; Sankdia et al., 2017; Turki et al., 2017), without advice or prescription by a physician or medical professional (Perwez and Dana, 2017; Khaled and Haytham, 2018) to treat self-recognized or self-diagnosed disorders or symptoms (Alhomoud et al., 2017; Olumide et al., 2018). Self-medication is therefore synonymous to self-treatment but not to self-care, which goes beyond self-medication to non-harmful health practices like water therapy, exercise, diet control and others to keep the body healthy (Naaraayan et al., 2016; Alhomoud et al., 2017; Olumide et al., 2018).
The practice of self-treatment has remained a global public health concern (Yadav and Rawal, 2015; Gupta and Singh, 2016; Chang et al., 2017), causing inadequate dosing, incomplete treatment courses, inappropriate usage of medicines and drug resistance (Olumide et al., 2018; Hitesh et al., 2018). The prevalence of self-treatment in Iran has been found to be three times more than global average (Nadia et al., 2016), with the most commonly used medications being analgesics, eye drops, antibiotics, cough and cold preparations, (Saber et al., 2015). Similar studies reported a prevalence of 86.4% in Egypt in 1995 (Agbor and Azobo, 2011; Aashi et al., 2016; Khaled and Haytham, 2018).
Antibiotics and antimalarial drugs are commonly self-administered in developing countries (Grigoryan et al., 2007; Gupta and Singh, 2016; Chang et al., 2017). Ullah et al. (2013) also reported incidence of self-medication of 76% in Karachi, 54% in Turkey, 88% in Croatia and 94% in Hong Kong among university students. A study by (Ansam, 2007) and Oluwole et al. (2016) reported a self-medication prevalence of 85.0%, 73.9 and 55.7% in Cameroon, Sudan and Nigeria respectively.
Pharmacies, drug shops, private and public health institutions were reported as sources of self-treatment drugs (Shankar et al., 2002; Skliros et al., 2010; Oluwole et al., 2016). Self-medication is also common with traditional medicine and often constitutes the first initial response to illness in Africa (Afungchwi et al., 2017; Kong et al., 2021). Of the different types of self-medication, over-the-counter (OTC) treatment constitutes the highest proportion (Chang et al., 2017), with paracetamol as the commonest (Darshana, 2014; Naaraayan et al., 2016).
Despite measures to limit self-medication, its prevalence continues to surge, indicative of some strong pull and push factors which need to be addressed. This study will evaluate the push and pull factors for self-medication in Cameroon and provide recommendations to address them.
METHODOLOGY
Study design and population
Cross-sectional survey on push and pull factors of self-medication among inhabitants in the city of Yaounde, Cameroon was conducted. Target sub-Divisions were Yaounde III, IV and VI, chosen for convenience and accessibility. Yaounde is the country’s political capital with a population of about 2.8 million and highly cosmopolitan with people from diverse economic, social and cultural backgrounds. Being an urban city, Yaounde competes with Douala in terms of number of pharmacies, which would be much fewer in any other towns. While all pharmacies open in the day, operations at night are on call basis. Convenience sampling method was used to select participants in this study. They include both male and female workers, students and all others from 16 years and above.
Study questionnaire
Data were collected using pre-validated close-ended questionnaires, self-developed for the purpose of the study. The questionnaire captured socio-demographic information, common diseases for which self-medication is practiced, means of diagnosis, action taken when sick, sources of information on medication, sources of drugs for self-medication, push factor for self-medication and whether self-medication is a good practice. While many of the questions had single options, some required checking multiple options, making the sum total of percentages not always equal to 100%. The questionnaire was pilot-tested, checked for face validity and modified in accordance with difficulties noticed. Only fully completed questionnaires were considered for final analysis.
After getting ethical clearance and directives from the national ethics committee, the questionnaire was administered to people of ages 16 and above and of both sexes. Prior to administering the questionnaires, there was a briefing on study background, objectives, methodology, constraints, data confidentiality, rights to opt out from the study, and procedure for completing the questionnaire. It was made clear that participation is voluntary, without compensation and data obtained will be treated anonymously and with utmost confidentiality. Participants were also told of the right to avoid answering questions they do not feel comfortable about. Consent was sought through a consent form and only those who signed the form were allowed to participate in accordance with the Helsinki Declaration.
Statistical analysis
Data collected was analysed using Microsoft Excel 2010 and expressed as counts and percentages in tables and bar charts.
RESULTS
Respondent demographics
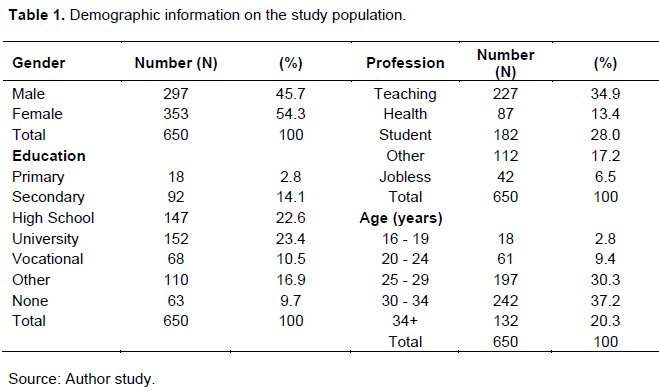
Of the 700 questionnaires administered, 353 were correctly filled by female respondents and 297 by males, giving a total of 650 respondents (92.9% participation). Majority of the respondents (87.8%) were 25 years or older (Table 1). A larger number were holders of high school certificate (22.6%) and university degree (23.4%). Of the 650 respondents, majority were workers.
Diseases for which self-medication is common
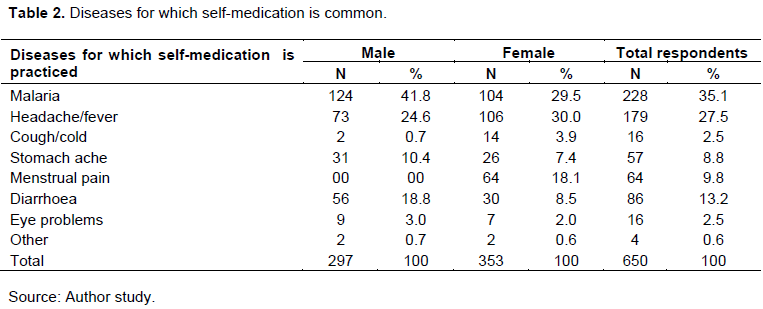
A total of 228 (35.1%) and 179 (27.5%) practiced self-medication to treat malaria and headache/fever respectively (Table 2).
Means of diagnosis of disease
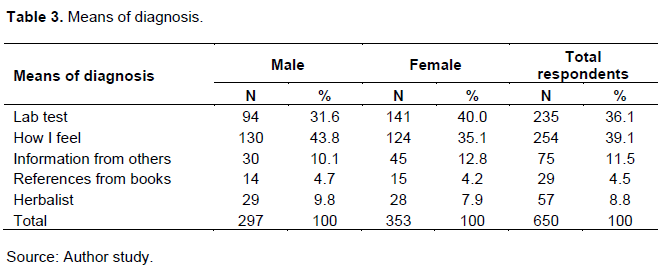
A majority of both male and female diagnose sickness mainly from how they feel (39.1%) and laboratory tests (36.1%), with more females (40.0%) using lab tests as opposed to 31.6% males (Table 3).
Educational Level and Action taken when sick
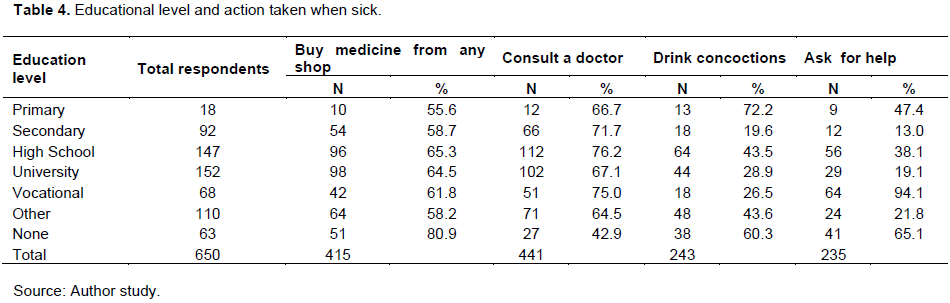
As shown in Table 4, 96 (65.3%) of high school students and 98 (64.5%) of university students buy medicines in any shop. Use of concoction (72.2%) is higher among primary school level participants.
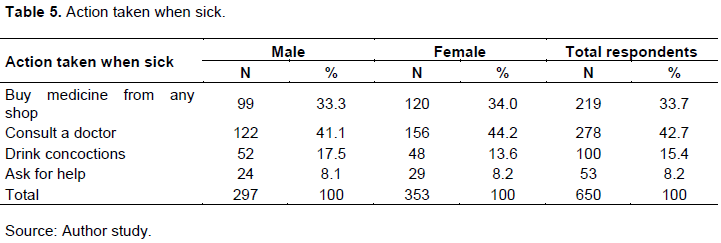
Action taken when sick
While 278 (156/353 females and 122/297 of males) consulted when they fell sick, 219 (120/353 females and 99/297 males) bought medicine from any shop (Table 5). Others either used medicinal plants concoction or sought for help from someone else.
Sources of information on drugs
A total of 186 (majority) of the respondents (119 or 33.7% females and 67 or 22.6% males) got information on drugs used for self-treatment from previous prescription. A good number equally used medical manuals while some consulted an herbalist (Figure 1).
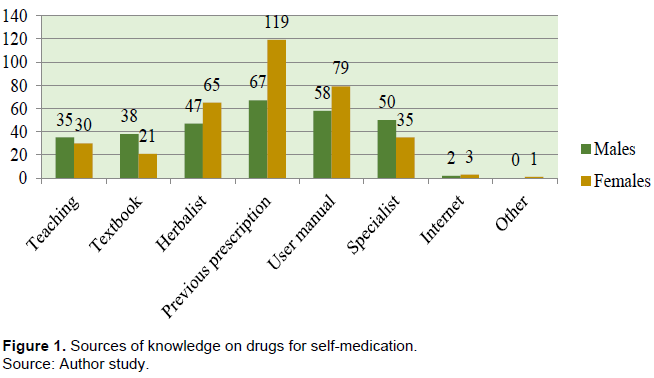
Table 6 shows that almost similar number of respondents got drugs from the pharmacy (216/650 or 33.2%) and nearby store (203/650 or 31.2%). A good number took remaining medication available at home.

Push factor for self-medication
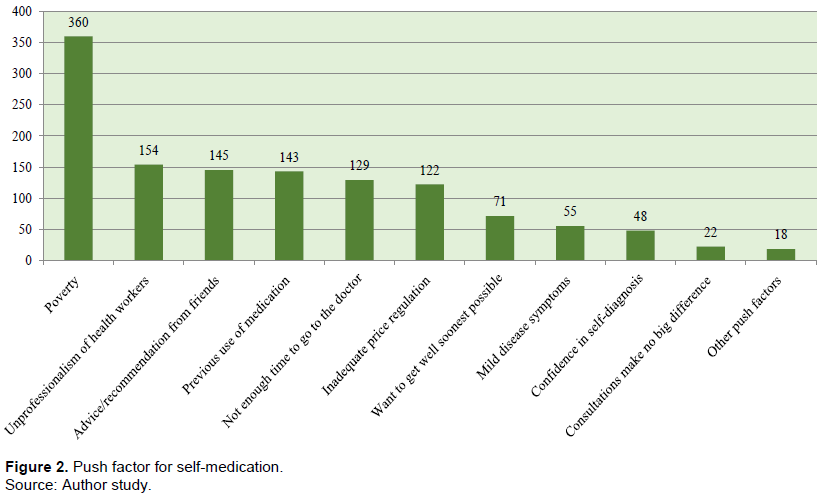
As shown in Figure 2, poverty constitutes the main push factor (360/650 or 55.4%) to self-medication. Health worker professionalism, advice from friends, previous use of medicines, time saving, and inadequate regulations are also major push factors.
Pull factor for self-medication
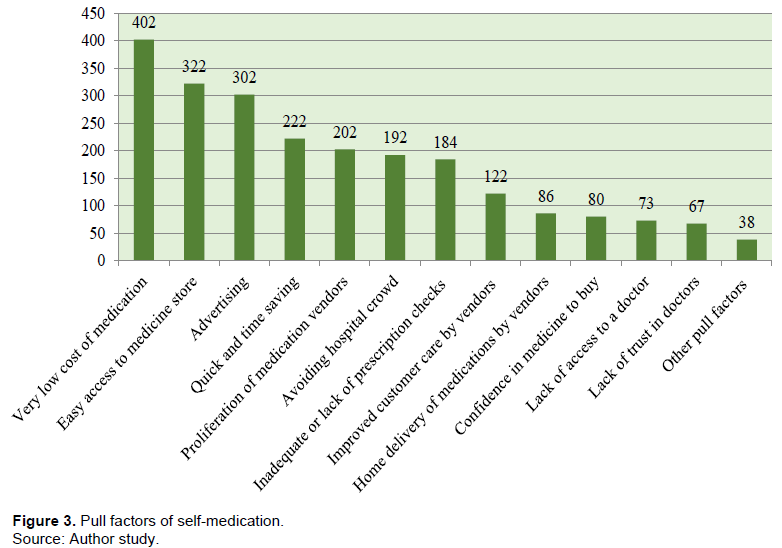
Low cost (402/650 or 61.9%) of medication was found to be the main pull factor, followed by easy access (322/650 or 49.5%) and rigorous advertisement (302/650 or 46.5%). Other pull factors include time saving, proliferation of drug vendors, avoiding hospital crowds, inadequate prescription checks (Figure 3). In order of priority, three principal reasons why people buy roadside medications are affordability, time-saving and accessibility.
Self-medication is a good practice
A total of 183 (28.2%) respondents (99 males and 84 females) believe self-medication is a good practice while 302 (46.4%), 132 males and 170 females, are of the opinion that it should be discouraged or controlled. However, 165 (25.4) are not sure if it is a good practice or not.
DISCUSSION
A total of 402/650 (61.9%) favoured self-medication due to low cost while 222/650 (34.2%) respondents practice it to gain time and 322/650 (49.5%) due to quick access. Self-medication was found to increase with increase in education level, with 65.3% of high school and 64.3%) university students indicating that they buy medicine fromany shop. This is contrary to the expectation that educated people should know about the risks of self-medication and rather contribute to reduce prevalence. This point to possible interpretation that higher levels of education translate to greater knowledge on medicines. This would be misleading the expectation
The most common disease for which self-medication is practiced was found to be malaria (35.1%), as supported by Gupta and Singh, (2016) and Chang et al. (2017), followed by headache and fever (27.5%). This is evident as malaria is endemic in Cameroon, with many high hospital consultations. Cough/cold, stomach-ache, menstrual pain, vomiting, diarrhoea, and ocular symptoms are other diseases for which self-treatment is common, as corroborated by Agbor and Azobo (2011), Aashi et al. (2016) and Khaled and Haytham (2018).
A majority (119/650 or 18.3%) of the respondents cited previous prescription (Figure 1) as source of information on medicines for self-treatment. This is supported by Oluwole et al. (2016), who further found that drug shops, private clinics, ordinary shops and government health centres offered information on self-treatment in Uganda. Shankar et al. (2002) and Skliros et al. (2010) also lend support to this finding through their report that pharmacies and medication leftovers from previous prescriptions constituted main sources in Greece. This indicates that patients liken symptoms for one illness to another and tend to depend more on how they feel. This gives room for the wrong treatment and also treating the wrong diseases and leading to drug resistance at subsequent treatment (Larsson et al., 2000; Ullah et al., 2013; Oluwole et al., 2016; Naaraayan et al., 2016; Olumide et al., 2018).
Ironically, a larger proportion of the respondents (33.2%) obtained medicine for self-medication from the pharmacy (Shankar et al., 2002; Skliros et al., 2010; Oluwole et al., 2016). This is quite disturbing because pharmacies are expected to function in respect of norms and ethics, ensuring that prescription medicines are not sold to patients without prescriptions (Ullah et al., 2013; Shaghaghi et al., 2014). As also reported by Osemene and Lamikanra (2012); Ullah et al. (2013) and Shaghaghi et al. (2014) 31.2% bought medicines from nearby stores or kiosks in the quarter. Apart from the low cost, quick access to these stores is a favourable pull factor. This study also found that patients share medicines with relatives or friends or using left-over at home as substantiated by Ullah et al. (2013) and Shaghaghi et al. (2014). This practice is dangerous as it exposes illicit users to the toxic effects of drugs, with long-term consequences.
Push factors for self-medication
Poverty was found to be the main push factor for self-medication (Figure 2), with unprofessionalism of health workers (Ullah et al., 2013; Oluwole et al., 2016; Naaraayan et al., 2016; Olumide et al., 2018), and friend’s advice (Ullah et al., 2013; Shaghaghi et al., 2014), as other reasons. Previous use of medicine (Shankar et al., 2002; Skliros et al., 2010; Oluwole et al., 2016), lack of time and inadequate price regulation (Rajakarunaa et al., 2006) were other major contributing factors. The quest for quick recovery pushes patients to go for quick relief while mild disease symptoms and self-confidence in diagnosis are other push factors.
Pull factors for self-medication
Low cost of medicines (Yadav and Rawal, 2015; Aashi et al., 2016; Elong et al., 2019) constituted the strongest pull factor for self-medication (Figure 3). Easy access to medicine in the vicinity of residences was found to be one of the pull factors (Esperanza, 2010, Yadav and Rawal, 2015; Aashi et al., 2016; Chang et al., 2017). The liberty to advertise anything in the name of medicine is causing untold organ damage as it attracts a huge market which benefits the medicine dealer but compromises the health of the patient through organ toxicity (Esperanza, 2010; Saber et al., 2015; El-Nimr et al., 2015) and drug resistance (Olumide et al., 2018; Oluwole et al., 2016; Naaraayan et al., 2016). The quick services offered by illegal and unprofessional medicine dealers are a strong pull factor to those who see consultation as time-wasting. Medicine vendors have become very innovative in how they deal with their customers. They exchange contacts with their regular customers and are available to supply the medicine at home. This further facilitates access, a practice which is uncommon with mainstream pharmacies. The proliferation of medicine vendors and kiosks along streets is a huge pull factor as they increase access to self-prescribed medicines (El-Nimr et al., 2015; Perwez and Dana, 2017; Khaled and Haytham, 2018; Elong et al., 2019).
Medicines are meant to cure illnesses but misuse could produce deleterious consequences. The fact that less than half of the respondents (302/650) found self-medication to be bad practice is seemingly conflicting. A cost-benefit analysis of self-medication is required to provide a guide on how to better address the conflicting interests in the practice of self-medication.
Recommendations to address push and pull factor
Considering the impact of poverty on purchasing power, there is a need to subsidise the cost of medication to reduce burden of care through out-of-pocket expenditures. Education and sensitisation constitute useful strategies to address ignorance, misdiagnosis, wrong prescription, and consequences on human health. Licenses should be issued only to trained and certified persons to own and operate medicine stores and kiosks, with signed engagement not to violate set norms. Also, control mechanisms should be put in place to ensure that only medicines of good quality are sold at homologated prices and misinformation through advertisements on social media, TV, the press, in buses or on the streets kept under check. The number of pharmacies should be increased to increase access to medicines. While human resources require an increase to reduce patient-to-doctor ratio and in turn reduce waiting time at hospital, pharmacies should equally innovate and introduce home deliveries and online sales upon submission of prescription.
Ethical considerations
This research was duly authorised by the competent administrative authorities and was carried out in strict compliance with national guidelines from the national ethics committee. Informed consent was sought directly from all adult participants while the much younger once were issued consent notes to be signed by their parents. Complete compliance to confidentiality and respect of anonymity of all respondents was strictly adhered to during data collection and management.
CONFLICT OF INTERESTS
The author has not declared any conflicts of interests.
REFERENCES
|
Aashi MM, Hisham AA, Rabaa HA, Bashair AA, Naif JA (2016). Self-medication among medical student in King Abdul-Aziz University. International Journal of Research in Medical Sciences 4(3):942-946. |
|
|
Afungchwi GM, Peter BH, Elena JL (2017). The role of traditional healers in the diagnosis and management of Burkitt lymphoma in Cameroon: understanding the challenges and moving forward. BMC Complementary and Alternative Medicine 17:209 |
|
|
Agbor MA, Clement CA (2011). Self-medication for oral health problems in Cameroon. International Dental Journal 61:204-209. |
|
|
Alhomoud F, Zainab A, Reem A, Khawlah A, Lama B, Farah KA (2017). Self-medication and self-prescription with antibiotics in the Middle East-do they really happen? A systematic review of the prevalence, possible reasons, and outcomes. International Journal of Infectious Diseases 57:3-12. |
|
|
Ansam FS (2007). Assessment of Self-Medication Practice among University Students in Palestine: Therapeutic and Toxicity Implications. The Islamic University Journal 15(2):67-82. |
|
|
Chang J, Wang Q, Fang Y (2017). Socioeconomic differences in self-medication among middle-aged and older people: data from the China health and retirement longitudinal study. BMJ Open 7:e017306. |
|
|
Darshana B (2014). Self?medication: A current challenge. Journal of Basic and Clinical Pharmacy 5:19-23. |
|
|
El-Nimr NA, Wahdan IMH, Wahdan AMH, Kotb RE (2015). Self-medication with drugs and complementary and alternative medicines in Alexandria, Egypt: prevalence, patterns and determinants. Eastern Mediterranean Health Journal (EMHJ) 21(4). |
|
|
Elong EG-A, Okalla EC, Penda IC, Nnanga NE, Mpondo ME, Eboumbou MCE (2019). Knowledge, practices and attitudes on antibiotics use in Cameroon: Self-medication and prescription survey among children, adolescents and adults in private pharmacies. PLoS ONE 14(2):e0212875. |
|
|
Esperanza MR (2010). Risks of self-medication practices. Current Drug Safety 5(4):315-323. |
|
|
Grigoryan L, Johannes GMB, Flora MH-R, John ED, Reginald D, Dominique LM, Antonella DM, Elizabeth AS, Ana-Claudia B, Cecilia SL, Joan B (2007). Is self-medication with antibiotics in Europe driven by prescribed use? Journal of Antimicrobial Chemotherapy 59:152-156. |
|
|
Gupta S, Singh M (2016). Self-medication among North Indian first-year undergraduate healthcare students: A questionnaire-based study. Tropical Journal of Medical Research 19:162-7. |
|
|
Hitesh S, Ravikant P, Sunil N, Hinaben RP, Diwakar S (2018). A questionnaire-based cross-sectional study on self-medication practices among undergraduate medical students of GMERS Medical College, Valsad, Gujarat. International Journal of Medical Science and Public Health 7:4. |
|
|
Khaled K, Haytham H (2018). Self-Medication Problem in Egypt: A Review of Current and Future Perspective. International Journal of Current Research and Review 10(4) |
|
|
Larsson M, Göran K, Nguyen TKC, Inga K, Fredrik L, Hoang DH, Göran T, Torkel F (2000). Antibiotic medication and bacterial resistance to antibiotics: a survey of children in a Vietnamese community. Tropical Medicine and International Health 5(10):711-721. |
|
|
Montgomery J, Bradley C, Rochfort A, Panagopoulou E (2011). A review of self-medication in physicians and medical students. Occupational Medicine 61:490-497. |
|
|
Naaraayan SA, Rathinabalan I, Seetha V (2016). Self-medication pattern among children attending a tertiary hospital in South India: a cross-sectional study. International Journal of Contemporary Pediatrics 3(4):1267-1271 |
|
|
Nadia A, Mohammad E, Sima R, Milad S, Arefeh T, Fatemeh S, Mohammad B (2016). Self-Medication and Contributing Factors: A Questionnaire Survey Among Iranian Households. Bali Medical Journal 5(3):17-21. |
|
|
Olumide A, Olusola AO, Anthonius AE, Semeeh AO (2018). Self-Medication with Antibiotics, Attitude and Knowledge of Antibiotic Resistance among Community Residents and Undergraduate Students in Northwest Nigeria. Molecular Diversity Preservation International (MDPI) Diseases 6(32). |
|
|
Oluwole AB, Joseph OF, Olujide JO, Kabir AD, Oladele AA, Paul OA, Temitope O (2016). Self-medication among health workers in a tertiary institution in South-West Nigeria. Pan African Medical Journal 24:312 |
|
|
Osemene KP, Lamikanra A (2012). A Study of the Prevalence of Self-Medication Practice among University Students in Southwestern Nigeria. Tropical Journal of Pharmaceutical Research 11(4):683-689. |
|
|
Perwez K, Dana HA (2017). Assessment of the Knowledge and Self-Medication Behaviours towards Antibiotics among Nursing Students at King Saud Bin Abdulaziz University for Health Sciences, Al Ahsa. Journal of Nursing and Care 6(6). |
|
|
Rajakarunaa RS, Weerasinghe M, Alifrangis M, Amerasinghe PH, Konradsen F (2006). The role of private drug vendors as malaria treatment providers in selected malaria endemic areas of Sri Lanka. Journal of Vector Borne Diseases 43:58-65. |
|
|
Saber AA, Mohammad M, Manal E, Sanaz R, Ahmad M, Majid N (2015). Prevalence and Cause of Self-Medication in Iran: A Systematic Review and Meta-Analysis Article. Iranian Journal of Public Health 44(12):1580-1593. |
|
|
Sankdia RK, Agrawal M, Rekha PB, Kothari N. (2017). A Questionnaire Based Study Regarding the Knowledge, Attitude and Practice of Self-Medication Among Second Year Undergraduate Medical Students. International Journal of Pharmacology and Clinical Sciences 6(1):01-05. |
|
|
Shaghaghi A, Marzieh A, Hamid A (2014). Predictors of Self-Medication Behavior: A Systematic Review. Iranian journal of Public Health 43(2):136-146. |
|
|
Shankar PR, Partha P, Shenoy N (2002). Self-medication and non-doctor prescription practices in Pokhara valley, Western Nepal: a questionnaire-based study. BMC Family Practice, p. 3. |
|
|
Skliros E, Panagiotis M, Athanasia P, Aristofanis G, George M, Christos P, Ioannis T, Irene Z, Alexios V, Petroula S, Alexios S (2010). Self-medication with antibiotics in rural population in Greece: a cross-sectional multicenter study. BMC Family Practice 11:58. |
|
|
Turki HA, Shahd A, Roqaih A, Razan A, Rawan A (2017). The self-medication use among adolescents aged between 13e18 years old; Prevalence and behavior, Riyadh e Kingdom of Saudi Arabia, from 2014e2015. International Journal of Pediatrics and Adolescent Medicine 4:19e25. |
|
|
Ullah H, Shujaat AK, Sayyad A, Sabiha K, Abdul B, Ossam C, Syed MFH, Kashif MK, Ghulam M (2013). Evaluation of self-medication amongst university students in Abbottabad, Pakistan; Prevalence, Attitude and Causes. Acta Poloniae Pharmaceutica and Drug Research 70(5):919-922. |
|
|
Yadav S, Gautam R (2015). Self-medication practice in low-income countries. International Journal of Pharmaceutical Chemistry and Analysis 2(3):139-142. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


