Full Length Research Paper

ABSTRACT
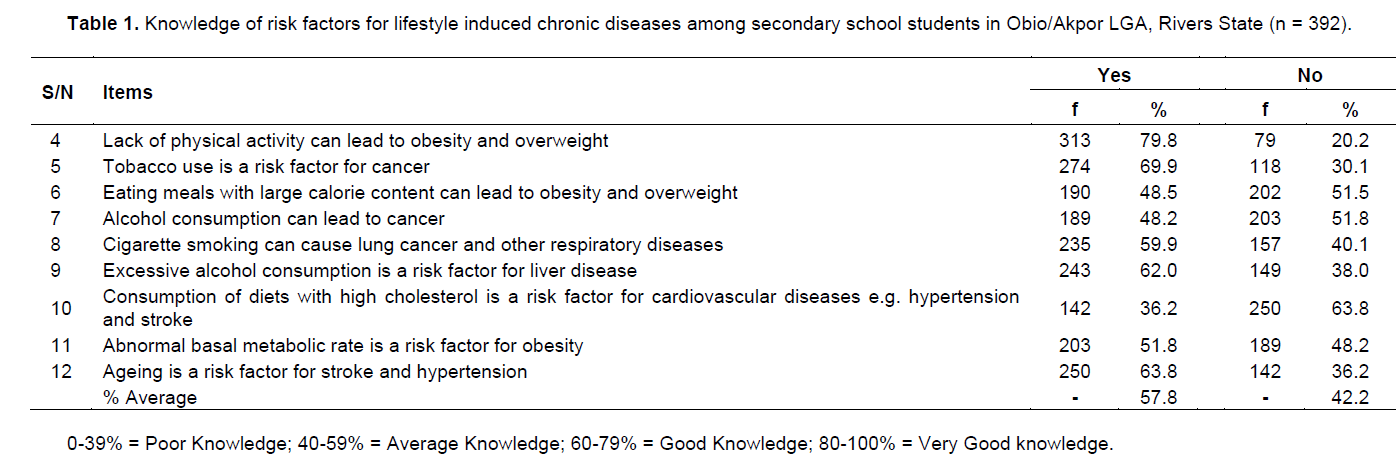
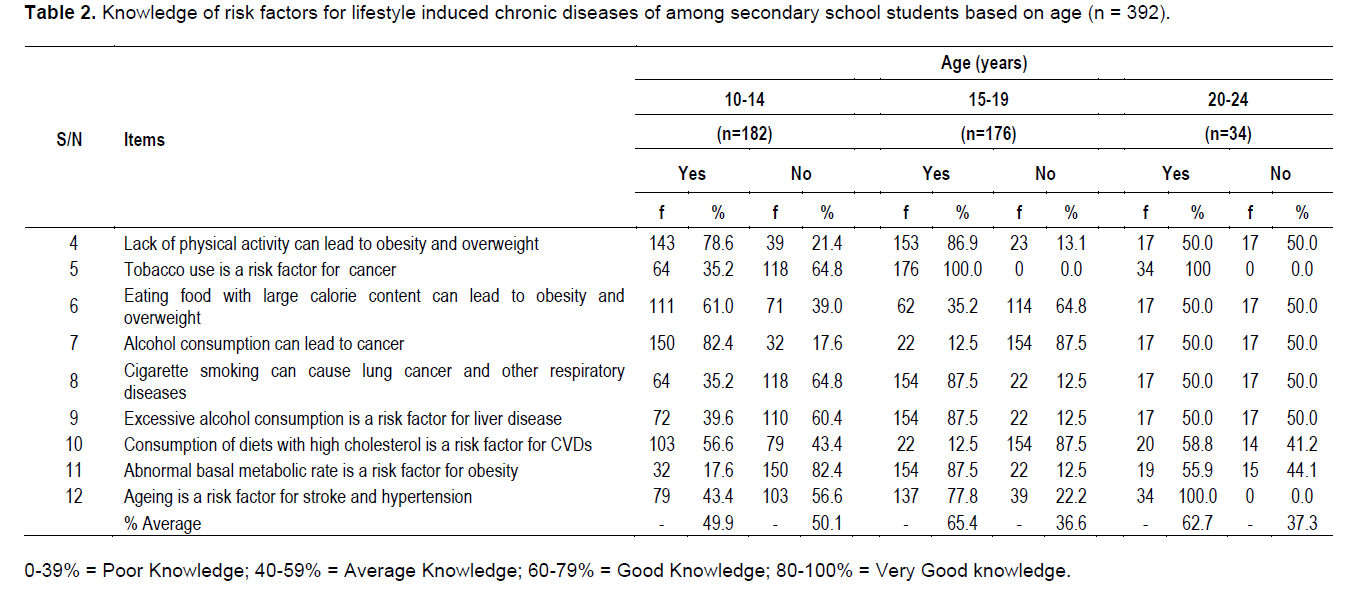
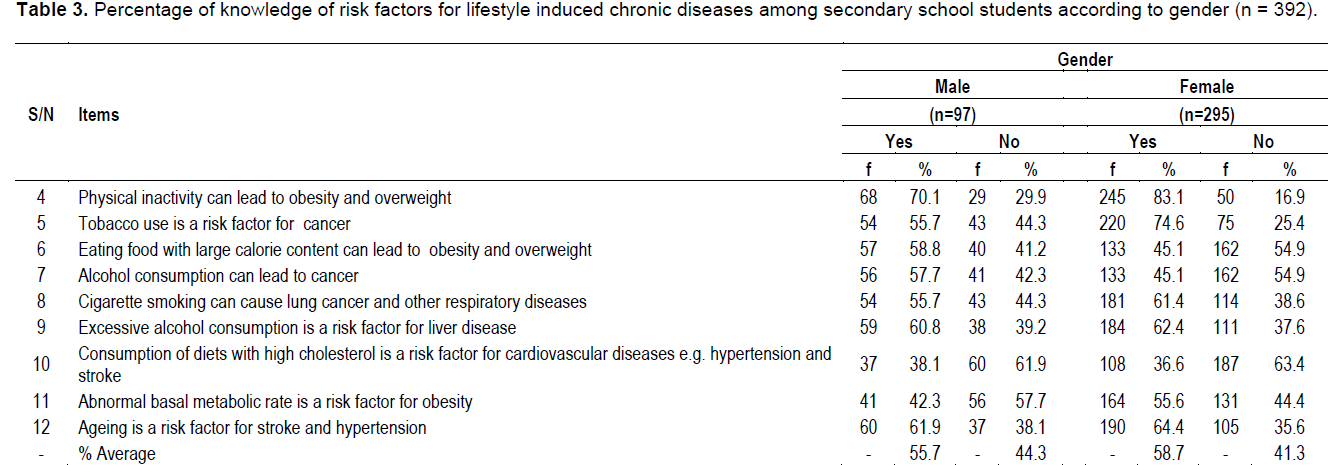
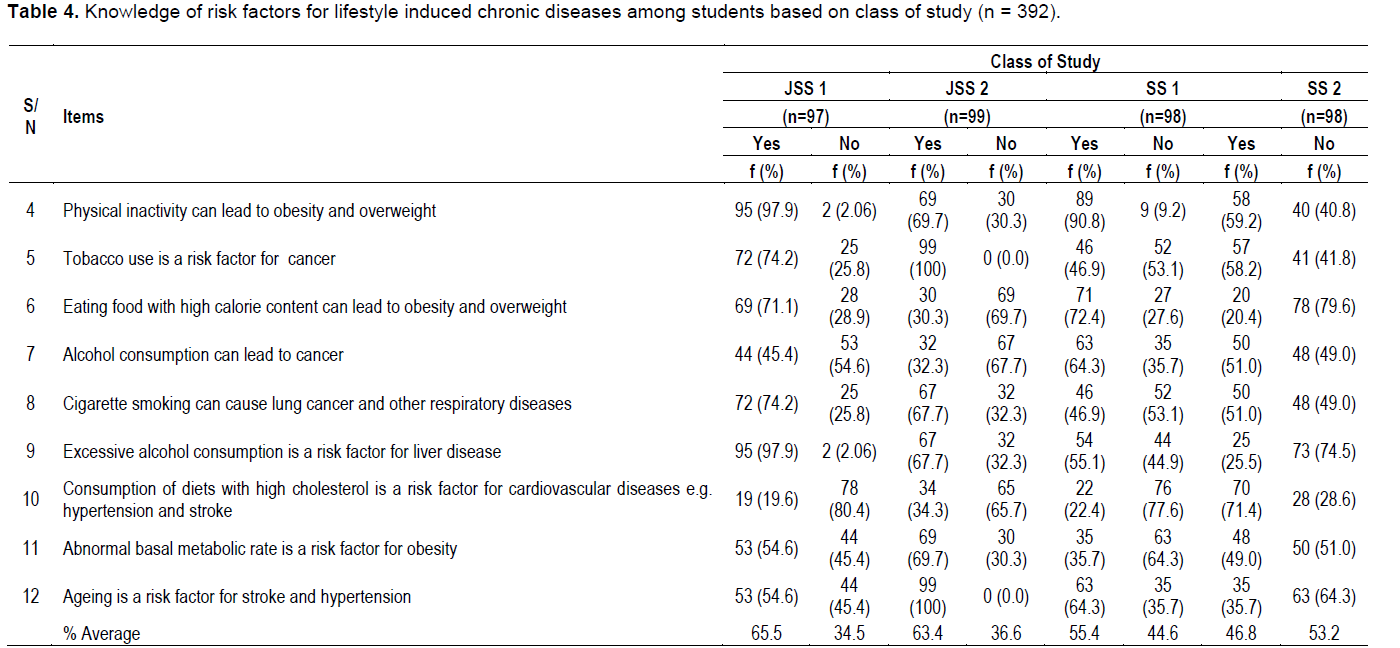
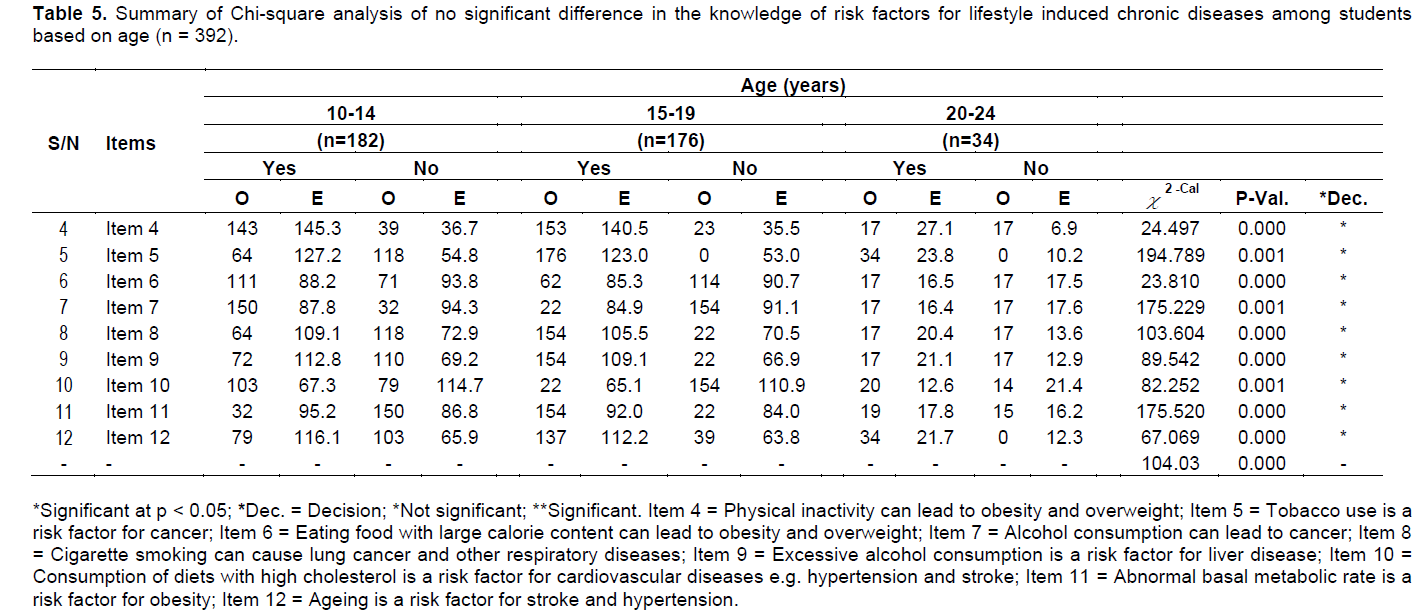
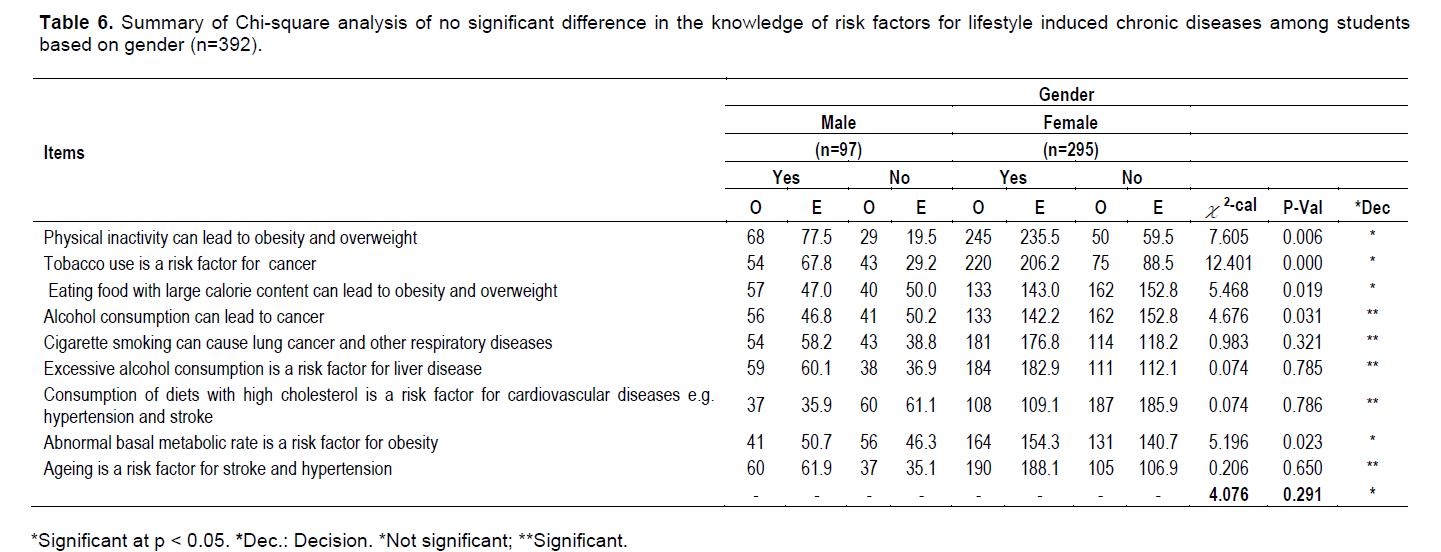
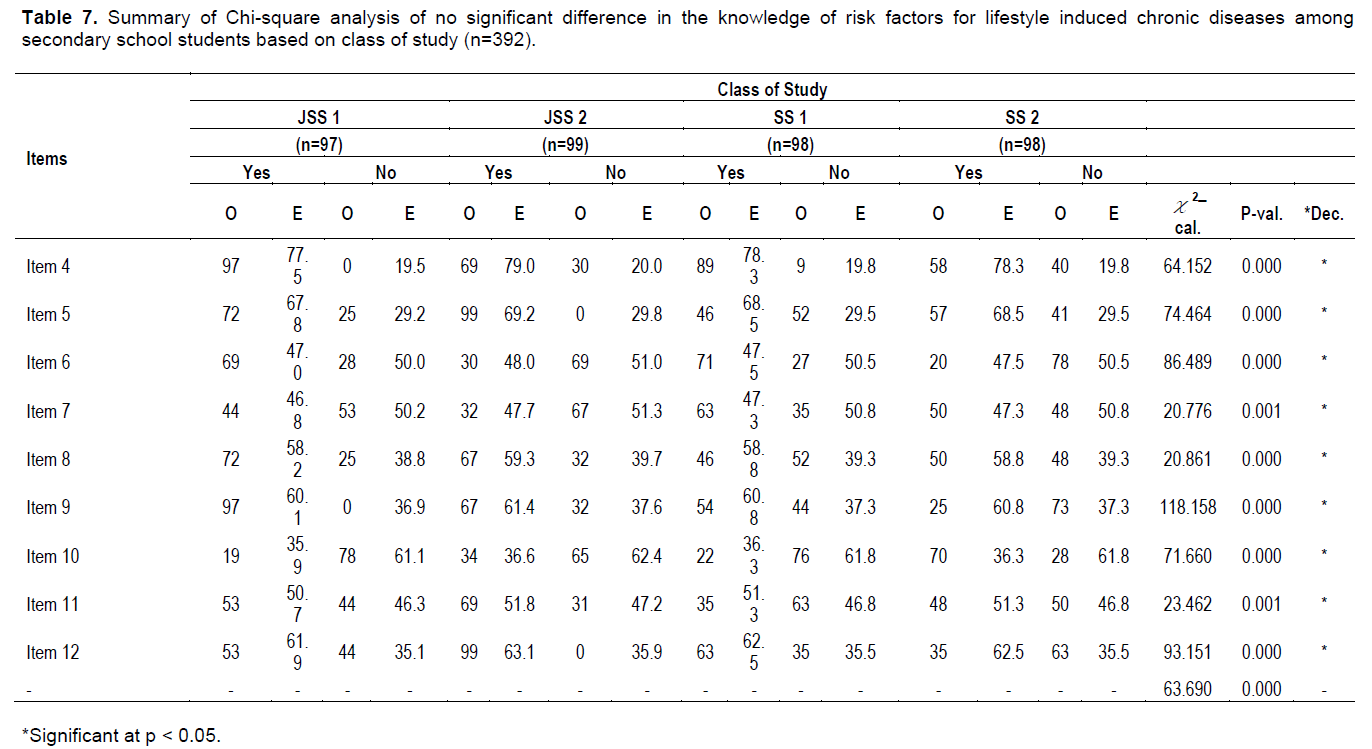
The study determined knowledge of risk factors for lifestyle induced chronic diseases among secondary school students in Obio/Akpor LGA, Rivers State. The sample for the study consisted of 480 secondary school students. The sample was drawn using multistage sampling procedures. The instrument for data collection was a researcher-designed structured questionnaire. Three experts validated the instrument. Reliability of the instrument was established using Split-half method and Spearman-Brown Correction Formula. The reliability coefficient of the instrument was 0.60. Data analysis was performed using frequency and percentages while inferential statistics of Chi-square (![]() 2) was employed to test the null hypotheses. Results showed that students had average knowledge (57.8%) of risk factors for lifestyle induced chronic diseases. Recommendations such as implementation of vigorous awareness campaign through health education on health risks of lifestyle induced diseases in schools, integration of nutrition education into the curricula of subjects such as Health Education, Home Economics, Biology and Health Science will help educate students on risk factors for lifestyle induced chronic diseases were made. In addition, interventions directed at reducing or modifying unhealthy lifestyles such as smoking, substance abuse/misuse and sedentary behaviours should be designed and effectively implemented at schools.
2) was employed to test the null hypotheses. Results showed that students had average knowledge (57.8%) of risk factors for lifestyle induced chronic diseases. Recommendations such as implementation of vigorous awareness campaign through health education on health risks of lifestyle induced diseases in schools, integration of nutrition education into the curricula of subjects such as Health Education, Home Economics, Biology and Health Science will help educate students on risk factors for lifestyle induced chronic diseases were made. In addition, interventions directed at reducing or modifying unhealthy lifestyles such as smoking, substance abuse/misuse and sedentary behaviours should be designed and effectively implemented at schools.
Key words: Physical activity, risk factors, adolescents, unhealthy lifestyles, chronic diseases.
INTRODUCTION
MATERIALS AND METHODS
RESULTS AND DISCUSSION
RECOMMENDATIONS
CONFLICT OF INTERESTS
REFERENCES
|
Anderson P, Chisholm D, Fuhr DC (2009). Effectiveness and cost-effectiveness of policies and programmes to reduce the harm caused by alcohol. Lancet 373:2234-2246. |
|
|
Atherton JS (2013). Forms of knowledge. Retrieved from |
|
|
Blum RW (2009). Young people: not as healthy as they seem. The Lancet 374:853-854. |
|
|
Ezzati M, Lopez AD, Rodgers A, Van der Hoorn S, Murray CJ (2002). Comparative risk assessment collaborating group. Selected major risk factors and global and regional burden of disease. Lancet 360:1347-1360. |
|
|
Gorard S (2003). Quantitative methods in social science. London: Continuum International Publishing. |
|
|
Ferlay J, Parkin DM, Steliavora-Foucher E (2010). Estimates of cancers incidence and mortality in Europe. J. Public Health Policy 46(4):765-781. |
|
|
Fezeu L, Minkoulou E, Balkau B, Kengne AP, Awah P, Unwin N, Alberti GKM, Mbanya J (2006). Association between socioeconomic status and adiposity in urban Cameroon. Int. J. Epidemiol. 35(1):105-111. |
|
|
Kiberd B (2006). The chronic kidney disease epidemic: Stepping back and looking forward. J. Chronic Disease Alliance 17:2967-2973. |
|
|
Lau-Walker M (2006). Predicting self-efficacy using illness perception components: A patient survey. British J. Health Psychology 11:643-661. |
|
|
Leventhal H, Leventhal EA, Cotrada RJ (1998). Self-regulation, health, and behaviour: A perception-cognitive approach. Psychology of Health 13:717-733. |
|
|
Lopez AD, Mathers CD, Ezzati M (2006). Global burden of disease and risk Factors. Washington, DC: World Bank. |
|
|
Mills ME, Davidson R (2002). Cancer patients' sources of information: Use and quality issues. Psych Oncol. 11:371-378. |
|
|
Morris J, Gwinn M, Clyne M, Khoury MJ (2003). Public knowledge regarding the role of genetic susceptibility to environmentally induced health conditions. Community Genetics 6:22-28. |
|
|
Norman P, Conner M (1999). The role of social cognition models in predicting health behaviours: Future directions. In Conner M, Norman P (Eds.). Predicting Health Behaviour. Buckingham, Open University Press. pp. 197-225. |
|
|
Peacey V, Steptoe A, Davídsdóttir S, Baban A, Wardle J (2006). Low levels of breast cancer risk awareness in young women: An international survey. Eur. J. Cancer 42:2585-2589. |
|
|
Perlitz U (2009). Diabetes- the price of increasing prosperity. Deutsh Bank Research. |
|
|
Sanderson SC, Waller J, Humphries S, E, Wardle J (2011). Public awareness of genetic influence on chronic disease risk: Are genetic and lifestyle causal beliefs compatible? Public Health Genomics 14:290-297. |
|
|
Soerjomataram I, de Vries E, Pukkala E, Coebergh JW (2007). Excess of cancers in Europe: A study of eleven major cancers amenable lifestyle change. Int. J. Cancer 120(6):1336-1343. |
|
|
Soerjomataram I, Oomen D, Lemmens V, Oenema A, Benetou Increased consumption of fruit and vegetables and future cancer incidence in selected European countries. Eur. J. Cancer 46(14):2563-2580. |
|
|
Schwarzer R, Fuchs R (1999). Self-efficacy and health behaviours. In M. Conner, & P. Norman (eds.), Predicting Health Behaviour. Buckingham, Open University Press. pp. 163-196. |
|
|
South African Medical Research Council (SAMRC) (2013). Chronic diseases of lifestyle (CDL). |
|
|
Tesfaye F, Byass P, Wall S (2009). Population based prevalence of high blood pressure among adults in Addis Ababa: Uncovering a silent epidemic. BMC Cardiovascular Disorders 9(39):1-5. |
|
|
Tylee A, Haller DM, Graham T, Churchill R, Sanci LA (2007). Youth-friendly primary-care services: how are we doing and what more needs to be done? Lancet 369(9572):1565-1573. |
|
|
Vaughan JP, Morrow RH (1989). Manual of epidemiology for district health management. Geneva: WHO, pp. 175-179. |
|
|
Witte K, Allen M (2000). A meta-analysis of fear appeals: Implications for effective public health campaigns. Health Education Behaviour 27:591-615. |
|
|
WHO (World Health Organization) (2008). Interventions on diet and physical activity. What Works? Geneva: WHO Publications. |
|
|
WHO (World Health Organization) (2010). Adolescents: Health risks and solutions. Geneva: WHO Publications |
|
|
WHO (World Health Organization) (2012). Global status report on non-communicable diseases. Available from |
|
|
WHO (World Health Organization)(2014). Adolescents: Health risks and solutions. Geneva: WHO. |
|
|
Yach D, Hawkes C, Gould C, Hofman K (2004). The global burden of chronic diseases: Overcoming impediments to prevention and control. JAMA 291(21):2616-2622. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


