ABSTRACT
Worldwide, the population of orphans and vulnerable children is estimated to be around 160 million with sub-Sahara Africa accounting for 80% of these children owing largely to the effect of HIV/AIDS, civil wars, road accidents, sectarian violence, terrorism, and other factors. Efforts have been made over the years by governments and development partners to mitigate the effects of orphanhood, but these efforts have failed to achieve the required objectives because various socio-demographic factors influence receipt of support services provided to OVC. This study therefore, examined the socio-demographic determinants of child health support services provided to OVC in Nigeria by employing a cross sectional research design utilizing secondary data obtained from the household recoded dataset of the 2013 Nigeria Demographic Health Survey (NDHS) and analyzed at univariate, bivariate, and multivariate levels (n=5114). The findings showed that region and age of child influenced receipt of health support at the bivariate level (p<0.05). Furthermore, at the multivariate level, only region of residence was significantly associated with the receipt of health support as residence in the North East, North West, and South South regions significantly influenced receipt of health support services by OVC in these regions (p<0.05). The study concluded that socio-demographic factors influenced health support services provided to OVC and recommends that interventions should ensure an equity-focused approach based on vulnerability status of children in providing support services. Also, innovative and integrated approaches should be employed in identification, service provision, tracking and monitoring of services provided to OVC in Nigeria.
Key words: Nigeria demographic health survey, sub-Saharan Africa, orphanhood.
In recent times, the definition of orphanhood and vulnerability across the development context has remained the same but with little differences in inclusion criteria. An orphan is defined as a child under the age of 18 who has lost one or both parents. Maternal orphans have lost mothers; paternal orphans lost fathers and double orphans have lost both parents (Skinner et al., 2004; UNICEF, 2006). However, there have been various definitions of a “vulnerable child”, including children whose parent(s) or caregivers are ill or deceased, children in poverty or conflict, and children without caregivers. Furthermore, in Nigerian Demographic and Health Survey (NDHS, 2013), an orphan is defined as a child under age 18 with one or both parents deceased while a vulnerable child is defined as a child under age 18 who has a very sick parent (sick for three or more consecutive months during the past 12 months) or who lives in a household where an adult was very sick or died during the 12 months preceding the survey (NPC and ICF International, 2014). In year 2000, there was an estimated thirty-five million children who had lost one or both parents due to different causes. By 2013, this number has quadrupled to almost 140 million with slightly above 10% of these children estimated to have become orphaned due to HIV/AIDS (UNICEF, 2016). It is also estimated that more than 80% of AIDS orphans live in sub-Saharan Africa (Hong et al., 2010; Bryant et al., 2012) as it is the region affected the most by the HIV/AIDS pandemic with the adult HIV-prevalence six times higher than the global average. The prevalence of orphans and vulnerable children has serious consequences for the well-being of children in any country.
They are prone to drop-out from school, lack basic needs such as shoes and clothes and more likely to be underweight or malnourished, while for the ladies, they are at higher risk of early sexual activity which exposes them to serious reproductive health problems including higher risk of pregnancy and diseases (NPC and ICF International, 2014). In Nigeria, it is reported that more than 12 million out of the Nigeria’s 69 million children are either orphaned or vulnerable. A major contributor to the high rate of vulnerable children include the increased rate of insurgency which have left 2 million children orphaned or vulnerable especially in the North East region of the country and the continued sectarian violence as experienced in the North West and middle belt regions of the country. Presently, almost half of the orphaned and vulnerable children are malnourished, three-quarter have no access to health care services and more than 70% have never attended school (
Save the Children, 2016). They would invariably mature into disenfranchised youths facing prospects of a lifetime of insecure employment, marginalization and poverty. The case of child vulnerability in Nigeria is worsened by the generally poor health and nutrition status of the country’s children. Responding to the needs of Orphans and Vulnerable Children (OVC) remains a public health challenge in Nigeria. Since 2005, the National Priority Agenda (NPA) was developed to assure and improve the quality of services provided for the well-being, protection, and development of the children considered most vulnerable in Nigeria.
Also, the Federal Ministry of Women Affairs and Social Development (2007) developed national guidelines and standards of practice for care of vulnerable children. These guidelines and standards focus on seven programme areas, including food and nutrition, shelter and care, child protection, health, psychosocial support, education and skills training; and household economic strengthening with the aim of strengthening existing safety nets and providing additional resources without undermining the capacity of communities and families to care for and protect vulnerable children (Biemba et al., 2009). However, recent estimates from the 2013 NDHS show that a high proportion of OVCs (95%) lived in households that did not receive any type of support whereas 5% of orphans and vulnerable children received at least one type of support. Presently, various international and local non-governmental organizations are involved in service provision across different program areas for orphans and vulnerable children in Nigeria but with the increasing economic crisis, high rate of insurgency and militancy, the need arises for targeted and strategic programs and interventions aimed at making the most impacts with adequate consideration of factors both socio-demographic and otherwise that influences support services to orphans and vulnerable children; hence the need for this study.
The data for this study was obtained from the Nigeria Demographic and Health Survey (NDHS) of 2013. A total 5,114 orphaned or vulnerable children met the inclusion criteria of being under age 18 with one or both parents deceased or living with a very sick parent (sick for three or more consecutive months during the past 12 months) or lives in a household where an adult was very sick or died during the 12 months preceding the survey and received a support service for health/medical support. The Data on variables such as father/mother dead or being sick for 3 or more months and socio-demographic characteristics at the individual (age of the child, sex of the child, place of residence, region of residence) was extracted from the people recoded dataset.
Data analysis
The data analysis was carried out using the STATA 13 statistical software. Data processing included exploring the dataset to ‘keep’ or ‘drop’ relevant variables, weight samples and apply the svy commands to correct sampling errors. The data analysis was carried out at three levels. The analysis included the usage of appropriate weighting procedure to handle biases that may result from over or under sampled respondents. Weighting procedure used was v005/1000000 being the weighting number for the Demographic and Health Survey datasets. Analysis at the univariate level entailed simple frequencies and percentages which enabled the understanding of the population characteristics, test of associations were conducted between the dependent and independent variables at the bivariate level while the binary logistic regression was employed to analyze the effect of each individual dependent variable against the outcome variable with the dependent variable indexed into a single categorical variable of two categories (Yes and No), measuring OVC that received or did not receive any medical support.
Socio-demographic characteristics of orphans and vulnerable children
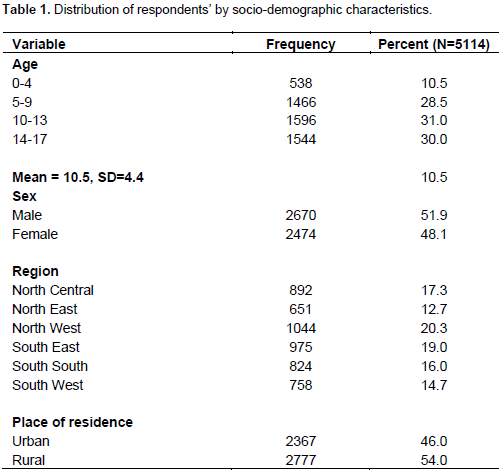
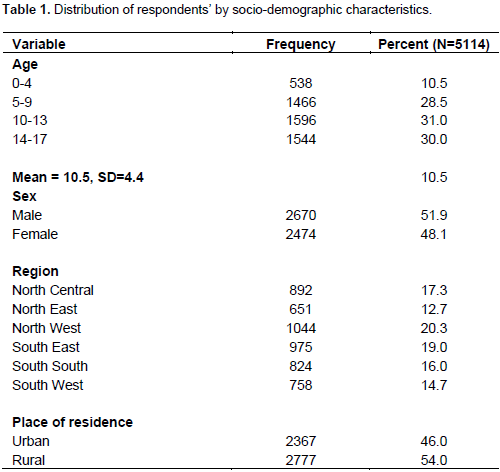
Table 1 shows the distribution of the orphans and vulnerable children in the study by their socio-demographics. It was observed that almost equal proportion of respondents belonged to the three highest age groups; with 28% being between ages 5 and 9 years, 31% between ages 10 and 13 years, 30% between ages 14 and 17 years, while only about one-tenth of the respondents were between ages 0 to 4. The mean age of the children was found to be 10 years with a standard deviation of 4.4. Furthermore, a little above half (52%) of the respondents were male as compared to 48% female. Respondents’ region revealed that almost an equal proportion of respondents, which accounted for the highest numbers were from the North West and South East with 20 and 19%, respectively while the lowest proportion of respondents was from the North East with 13%. Meanwhile, more than half (54%) of the total respondents are resident in rural areas while 46% reside in urban areas.
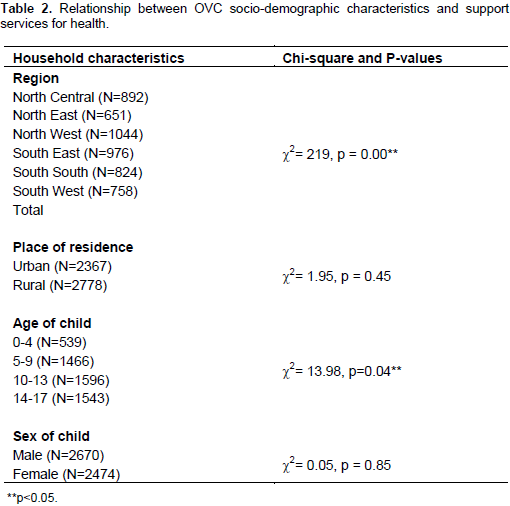
Bivariate analyses
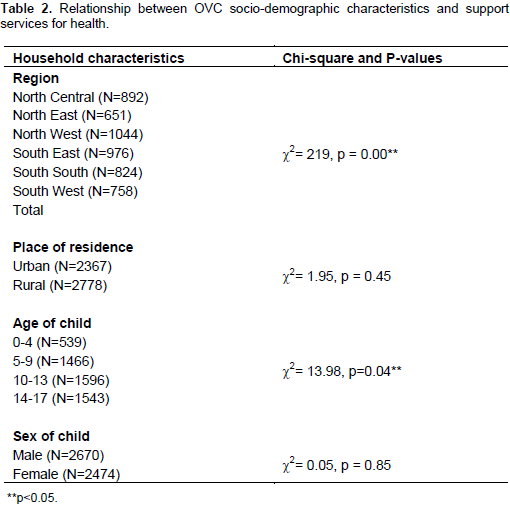
An examination of the bivariate relationship showed that region of residence and age of child were associated with receiving health support services while no relationship existed between place of residence of OVC, sex of child and receipt of support services for health (Table 2).
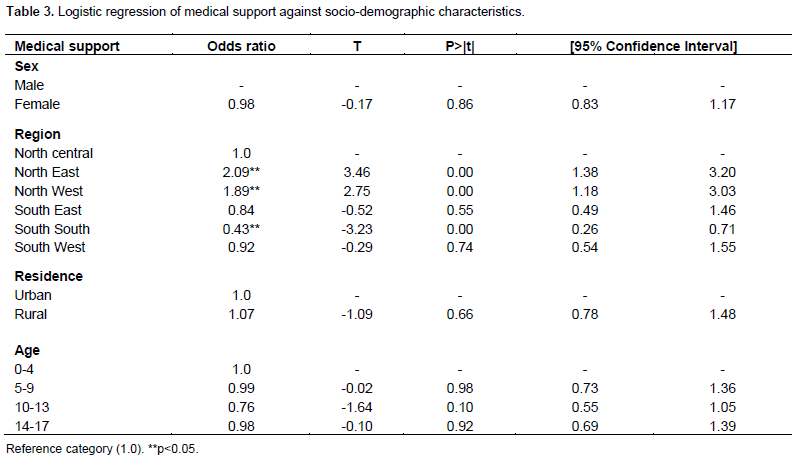
Multivariate analyses
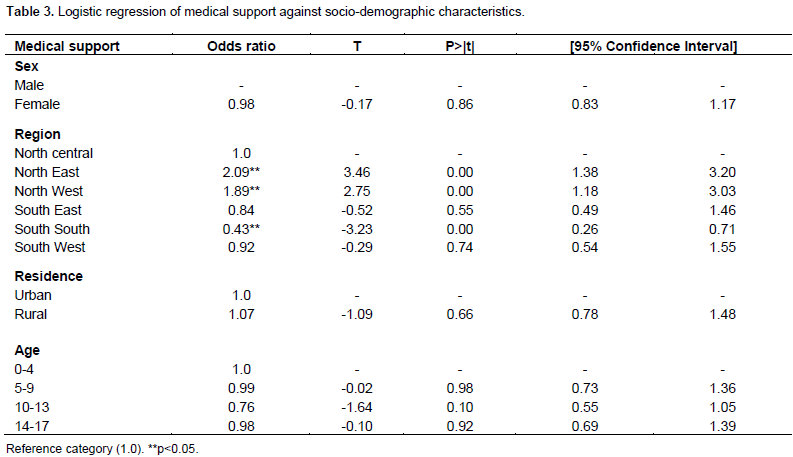
Table 3 shows the odds of predicting the relationship between OVC support services received for health and their socio-demographic characteristics. Result revealed that female OVC is less likely to receive support service for health than their male counterparts (OR=0.98, p>0.05). Considering region, the result showed that the OVC in the North East region was 2.09 times more likely to receive health services support than other regions (OR=2.09, p<0.05). It was also revealed that those in the North-West region were 89% more likely to receive health services support as compared to other regions (OR=1.89, p<0.05). The result further revealed that support services for health were 16, 8 and 57% less likely to be received by orphaned and vulnerable children in the South East, South West and South-South, respectively. In the examination of place of residence, findings revealed that OVC who resided in rural areas were 7% more likely to receive health support services as compared those in urban areas (OR=1.07, p>0.05). Adjusting for other socio-demographic characteristics and considering respondents age, OVC who were between ages 5 and 9 were slightly less likely to receive health support services as compared to those between ages 0 and 4 (OR=0.99, p>0.05). An increment in age reduces the likelihood of receiving health support services but this was inconsistent for children between ages 14 and 17 as it was noticed that they were more likely to receive support services for health in comparison to those in age group 10 to 13.
The purpose of this study was to examine the socio-determinants of health support services among orphans and vulnerable children in Nigeria. The study found that sex of child and region of residence were significantly associated with receiving support services for orphans and vulnerable children. This finding is consistent with the findings of Schenk et al. (2010) and Goodman et al. (2014). who concluded that household characteristics influenced receipt of health support services to orphans and vulnerable children in Kenya.Although, the finding stated that household income was the most important predicting factor as it also affected child health accessibility and receipt of household economic strengthening services. Other studies, including those of Tagurum et al. (2015) and Aspaas (1999) found that region of residence influences OVC support services received. They were also stated to influence the range and value of resource options available to orphans and vulnerable households and has implied consequences on access to services for vulnerable populations. Furthermore, in other studies, Ainsworth and Filmer (2006), Campbell et al. (2010) and Olanrewaju et al. (2015) who conducted studies on orphans and vulnerable and their access to other support services such as education and psychosocial support, it was found that socio-demographic and household factors also influenced receipt of these support services as it was specifically stated that wealth, gender and regional variation are all more important predictors of receipt of support services. Therefore, this study supports other studies including those of Foster and Germann (2002), Harber (2009) and Datta (2013) that proposed community-based care as viable approach to taking care of orphans and vulnerable children as it places children at the centre of all development programmes, ensures different levels of community ownership and participation (Ansell and Young, 2004; Sanou et al., 2009) and believed to be the most cost-effective strategy for providing care and support to OVC but proposes that interventions on service provision for OVC should be integrated into other programs such as the Hard-to-Reach (HTR) programs and the new Community Health Influencers, Promoters and Services (CHIPS) program Community Health Influencers, Promoters and Services (CHIPS) program (Adebayo, 2017) as this would help improve service provision to households, case management, tracking, monitoring and follow-up of services and militate against the influence of socio-demographic factors such as region of residence.
The study concludes that socio-demographic factors play a major role in receipt of health services by orphans and vulnerable children in Nigeria, although there might be other associated factors. Hence, programs and interventions should consider the dynamics of socio-demographic factors in the design and implementation of orphan and vulnerable children programs and interventions in Nigeria.
The authors have not declared any conflict of interests.
The author wish to thank ICF Macro and Measure DHS for granting the permission to use the NDHS 2013 dataset. ICF Macro provided technical assistance as well as funding to the survey through Measure DHS, a project funded by the United States Agency for International Development (USAID) that provides support and technical assistance for the implementation of population and health surveys in many countries of the world.
REFERENCES
|
Adebayo T (2017). FG To Improve Community Health Services. The Independent Newspaper Online.
View
|
|
|
|
Ainsworth M, Filmer D (2006). Inequalities in children's schooling: AIDS, orphanhood, poverty, and gender. World Dev. 34(6):1099-1128.
Crossref
|
|
|
|
Ansell N, Young L (2004). Enabling households to support successful migration of AIDS orphans in southern Africa. AIDS Care 16 (1):3-10.
Crossref
|
|
|
|
Aspaas HR (1999). AIDS and Orphans in Uganda. Geographical and Gender Interpretations of Household Resources J. Soc. Sci. 36 (2): 201226. ISSN: 0362-3319
|
|
|
|
Biemba G, Walker E, Simon J, Costello J, Beard J, Brooks B (2009). Nigeria Research Situation Analysis on Orphans and Other Vulnerable Children. OVC-CARE Project. Boston, USA, Boston University Center for Global Health and Development.
View
|
|
|
|
Bryant M, Beard J, Sabin L, Brooks MI, Scott N, Larson BA, Simon J (2012). PEPFAR's support for orphans and vulnerable. Some beneficial effects, but too little data, and programs spread thin. Health Affairs 31(7):1508-1518.
Crossref
|
|
|
|
Campbell P, Handa S, Moroni M, Odongo S, Palermo T (2010). Assessing the orphan effect in determining development outcomes for children in 11 eastern and southern African countries. Vulnerable Children Youth Stud. 5(1):12-32.
Crossref
|
|
|
|
Datta D (2013). Protecting rights of orphan and vulnerable children: no substitute for community action in Nyanza, Kenya. Com. Dev. J. 48(1):105-118.
Crossref
|
|
|
|
Foster G, Germann S (2002). The orphan crisis. In: Myron, E. (Ed.), AIDS in Africa. Kluwer Academic, New York. pp. 664-675.
Crossref
|
|
|
|
Goodman ML, Kaberia R, Morgan RO, Keiser PH (2014). Health and livelihood outcomes associated with participation in a community-based empowerment program for orphan families in semirural Kenya. A cross-sectional study. Vulnerable Children and Youth Studies. Int. Interdiscipl. J. Res. Pol. Care 9(4).
Crossref
|
|
|
|
Harber M (2009). Developing a Community-based AIDS Orphan Project: A South African Case Study.
View
|
|
|
|
Hong Y, Li X, Fang X, Zhao L, Zhao J, Zhao Q, Lin X, Zhang L, Stanton B (2010). Health Policy and Planning. J. Health Pol. Plan. 26:15-123.
|
|
|
|
Olanrewaju AD, Jefferey C, Crossland N, Valadez JJ (2015). Access to Education for Orphans and Vulnerable Children in Uganda. A Multi-District Cross-Sectional Study Using Lot Quality Assurance Sampling from 2011 to 2013. PLoS One 10(7):e0132905.
Crossref
|
|
|
|
National Population Commission (NPC) Nigeria] and ICF International (2014). Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International
|
|
|
|
Sanou D, Turgeon-O'Brie H, Ouedraogo S, Desrosiers T (2009). Caring for orphans and vulnerable children in the contexts of poverty and cultural transition: a case study of a group foster homes program in Burkina Faso. J. Children Poverty 14(2):139-155.
Crossref
|
|
|
|
Save the Children (2016). North East Nigeria. Children's Lives and Futures at Risk Briefing Paper (2016).
|
|
|
|
Schenk KD, Michaelis A, Sapiano TN, Brown L, Weiss E (2010). Improving the lives of vulnerable children: Implications of Horizons Research among orphans and other children affected by AIDS. Publ. Health Reports 125(2):325-336.
Crossref
|
|
|
|
Skinner D, Tsheko N, Mtero-Munyati S, Segwabe M, Chibatamoto P, Mfecane S, Chitiyo G (2004). Defining orphaned and vulnerable children. AIDS Behav. 10(6):619-625.
Crossref
|
|
|
|
Tagurum YO, Chirdan OO, Bello DA, Afolaranmi TO, Hassan ZI, Idoko L (2015). Situational analysis of orphans and vulnerable children in urban and rural communities of Plateau State. Ann. Afr. Med. 14(1):18-24.
Crossref
|
|
|
|
United Nation Children's Fund (UNICEF) (2006). Africa's Orphaned and Vulnerable Generations. Children affected by AIDS. ISBN-13: 978-92-806-4035-9. New York, UNICEF.
View
|
|
|
|
United Nations Children's Fund (UNICEF) (2016). Nigeria crisis. Reaching children affected by conflict. ISBN-10: 92-806-4035-6. New York, UNICEF.
View
|