Full Length Research Paper

ABSTRACT
Management of multi drug resistant tuberculosis (MDR-TB) patients remains a challenge in the control of tuberculosis worldwide. MDR-TB patients require long term treatment with drugs that cause various adverse effects especially ototoxicity associated with aminoglycoside. Current treatment guidelines still include aminoglycosides use especially in developing countries. However, there is dearth of information regarding ototoxic effects of MDR-TB treatment in Nigeria. This study explored the prevalence of ototoxicity and associated factors among MDR-TB patients during the intensive phase of treatment. A retrospective review of records of 383 MDR-TB patients admitted at two specialist treatment centers in South West Nigeria from 2012-2017 was conducted. Using a structured proforma, socio demographic characteristics and clinical history were extracted. Ototoxicity was assessed as any abnormality reported from a pure tone audiometry. Discrete data were summarized with frequencies, proportions while bivariate analysis was done using chi square test to identify associated factors. Multivariate analysis was performed to identify independent predictors of ototoxic effects. All statistical significance was set at 5%. Out of the 383 records extracted, only 143(37.3%) had audiometry performed. Of these 143 MDR-TB patients, mean age was 36.2 ± 11.3 years and prevalence of any ototoxic effect was 72.7 %. This was higher in older age groups, females and those underweight. (p>0.05) Patients who did not sputum convert at the end of treatment and HIV co infected had higher proportions with ototoxic effects (p < 0.05). However, on multivariate analysis only age remained a significant independent predictor of ototoxic effect (AOR: 8.7; 95% CI: 1.4-52.2). Adverse effects are main deterrents to compliance and completion of long term treatment regimen. High rates of ototoxic effects as seen in this study could affect successful management of MDR-TB patients. Auditory monitoring and rehabilitation should be recommended for MDR-TB patients even after completion of the intensive phase of treatment.
Key words: Aminoglycoside ototoxicity, drug resistant tuberculosis, Nigeria.
INTRODUCTION
Multidrug-resistant tuberculosis (MDR-TB) caused by Mycobacterium tuberculosis strains resistant to at least isoniazid and rifampicin – has emerged as a growing public health concern that jeopardizes the progress made in tuberculosis care and control worldwide due to complexities in diagnosis, high treatment failure and cost of treatment (WHO, 2016). Management of multi drug resistant tuberculosis (MDR-TB) patients remains a challenge in the control of tuberculosis worldwide. MDR-TB patients require long term treatment with drugs that cause various adverse effects especially ototoxicity associated with aminoglycoside.
Fluoro-quinolones and aminoglycosides constitute the core of all recommended MDR-TB regimens. Current treatment guidelines still include aminoglycosides use especially in developing countries as aminoglycosides are very cheap and accessible injectable anti tuberculous drugs (WHO, 2016). Aminoglycosides are very effective anti -bacterial agents especially for mycobacterium species. The common aminoglycosides used in the management of multi drug resistant tuberculosis are Amikacin, Kanamycin and Capreomycin. Amikacin is a known semi-synthetic aminoglycoside that shows excellent activity against Mycobacterium tuberculosis and atypical mycobacteria and has been used in the treatment of disseminated atypical Mycobacterium infection in HIV/AIDS patients (Black et al., 1976; Fausti et al., 1992). Kanamycin is also very effective but more toxic to the ear but useful in patients with resistant to more commonly used drugs while capreomycin despite its proven value in the treatment of drug resistant or treatment failure tuberculosis, it is equally toxic as most aminoglycosides. However, these injectable agents have significant side effects in the form of progressive irreversible ototoxicity and usually reversible nephrotoxicity (Vakulenko and Mobashery, 2003). Ototoxicity is defined as: ‘the tendency of certain therapeutic agents and other chemical substances to cause functional impairment and cellular degeneration of the tissues of the inner ear, and especially of the end-organs and neurons of the cochlear and vestibular divisions of the eight cranial nerve (Hawkins, 1976).
Aminoglycoside ototoxicity is the pharmacological adverse reaction affecting the inner ear or auditory nerve, characterized by cochlear or vestibular dysfunction and is recognized by a distinctive pattern of hearing loss starting in the high frequency range (4000–8000 Hz) with lower frequencies being affected only later (Duggal and Sarkar, 2007; Ganesan et al., 2018).
Various studies have reported different levels of ototoxicity of these agents across high burden TB countries. A study in India, reported prevalence of 18% among hospitalized multidrug resistant tuberculosis patients with low socio economic status and co morbidities like diabetes and hypertension being associated with hearing loss(Sharma et al., 2016). Similar findings were also seen in another study in Netherlands where hearing loss was found in 18% of patients, with patients on kanamycin based regimen having the higher proportion with ototoxicity (de Jager and van Altena, 2002) .
However, higher proportions have been reported from African studies. A study carried out in Botswana revealed a relatively high prevalence of hearing loss of 62 % though majority had good treatment outcome. "Findings from this study also showed that longer amikacin duration and higher dosage per weight per month were associated with development of hearing loss (Modongo et al., 2014). Ototoxicity was also documented as 57% in a study in Cape Town and this was found to be significantly higher in HIV positive patients as compared to HIV negative patients.
One of the few studies conducted among multi drug resistant tuberculosis patients admitted for intensive phase management in a treatment center in Nigeria revealed that 22.9% were confirmed to have ototoxicity by audiometric criteria. Others even reported higher prevalence of ototoxicity of 50% in South East Nigeria (Ibekwe and Nwosu, 2016). Ototoxicity has been found to be associated with age, BMI on admission and retroviral positivity (Sogebi et al., 2017). Another study carried out to explore the pattern of adverse events experienced by patients admitted across 9 multi drug resistant centers in Nigeria showed that ototoxicity was the third leading adverse effects following gastrointestinal and neurological disorders experienced by these patients. However, Ototoxicity was found to be the most severe and debilitating among these patients (Avong et al., 2015).
However, there is still dearth of information regarding ototoxic effects of MDR-TB treatment in specific locations in Nigeria. This study investigated the prevalence of ototoxicity and associated factors among hospitalized MDR-TB patients during the intensive phase of treatment in South Western Nigeria.
MATERIALS AND METHODS
This study was conducted in Oyo State. Oyo State has two out of Nigeria. A retrospective review of records of multi-drug resistant Oyo State has two out of the five active multi-drug resistant treatment centers in South Western Nigeria tuberculosis patients admitted at the two specialist treatment centers in Oyo State between 2012 – 2017 was carried out. A semi-structured abstraction form was developed to extract information from the patient clinical and laboratory records. The form contained 3 sections which include socio demographic characteristics, past history of tuberculosis including drug regimen and clinical/laboratory characteristics. Two trained research assistants abstracted information from these records over a period of 8 weeks. Primary outcome variable in this study was ototoxicity. Due to the nature of this study, ototoxicity was assessed as any abnormality reported from a pure tone audiometry (PTA) based on the American Speech-Language-Hearing Association (ASHA). Those that had any form of abnormality were regarded has having ototoxicity. In addition, based on the pattern of result on the PTA, patients were further classified in mild, moderate and severe hearing loss. In addition, treatment outcome was documented in this study and was classified as favourable (patients that were discharged to Directly Observed Treatment (DOTs) centers) and unfavourable (patients who died or discharged against medical advice. A total of 383 records were retrieved from the two specialist centers in Oyo State. However, not all patients had pure tone audiometry performed on them and these were excluded from analysis.
Data were entered using Microsoft Excel and analyzed using STATA v 14.1. Descriptive Statistics such as frequencies, proportions and relevant summary indices were obtained for socio- demographic variables, previous TB history while bivariate analysis was done using chi-square test to identify factors associated with ototoxic effect or not among MDR-TB/HIV co infected or non co infected patients. Independent predictors of ototoxicity were identified by fitting a binary logistic regression model. All statistical significance was set at 5%. Ethical approval for this study was obtained from the Oyo State Ministry of Health and verbal approval from the Medical Director of the specialist center.
RESULTS
One hundred and forty-three multi-drug resistant tuberculosis with a mean age of 36.2 ± 11.2 years were included in this study. Majority of the patients were aged between 25-44 years (66.3%) and males (62.2%). However, a slightly higher proportion were underweight (51%) and 14.7% were co- infected with HIV. About ninety percent had ever been previously treated for tuberculosis with majority of them failing first line 6 months’ regimen. Sputum AFB was also found to be positive in 73.9% of the patients. Following interpretation of the pure tone audiometry results, prevalence of ototoxicity was found to be 72.7% in these groups of patients. However, majority of the patients affected had mild sensorineural hearing loss (61.1%) and had both ears affected (72.2%) (Table 1).
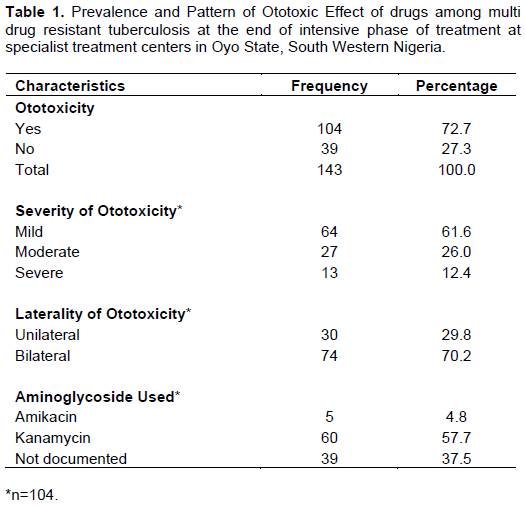
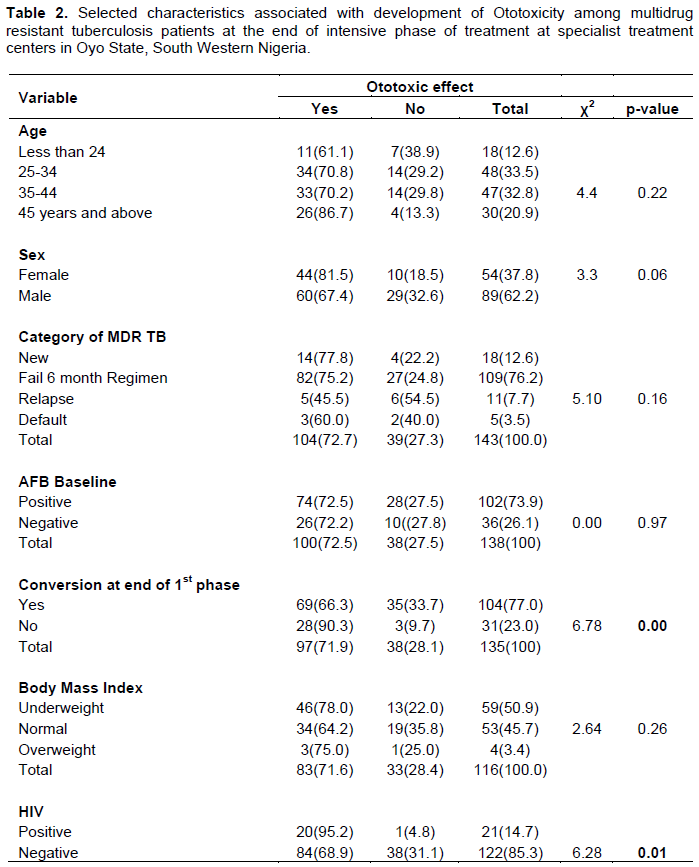
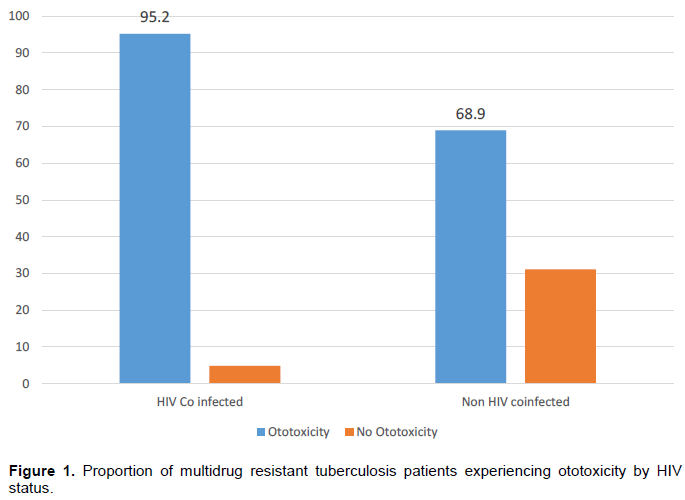
Table 2 shows that the prevalence of ototoxicity increased with age as patients aged 45years and above had the highest proportion (86.7%). Females also had a higher proportion of patients with ototoxic effects (81.5%) as compared to males (67.4%) and patients in the extremes of weight had higher proportions with ototoxic effects (underweight (78.0%) and overweight (75.0%); however all these were not statistically significant (p > 0.05). HIV positive patients had a significantly higher proportion of patients with ototoxic effect (95.2 %) as compared to 68.9 % among those who were HIV negative (Figure 1). In addition, about 90% of the patients who did not sputum convert at the end of the intensive phase had some form of ototoxic effect (p < 0.05).
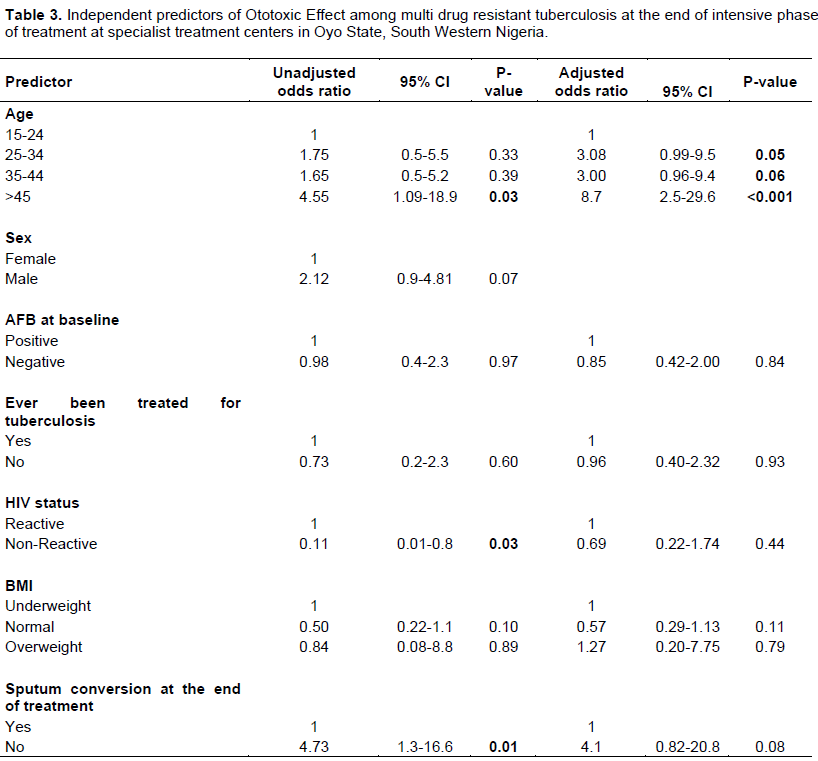
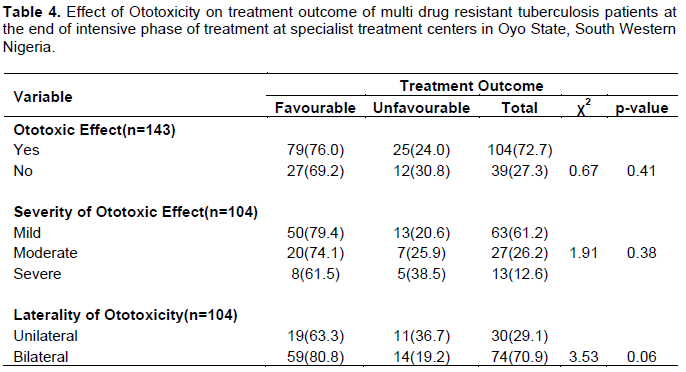
On multivariate analysis after controlling for possible confounders, age remained a significantly independent predictor of ototoxicity among multi drug resistant patients as those aged 45 years and above were 8.7 times more likely to develop ototoxicity (OR: 8.7; 95% CI 2.5-29.6). Although the model also shows patients who did not sputum convert at the end of the intensive phase were 4.1% more likely to develop ototoxicity it was marginally insignificant (OR: 4.1; 0.8-20.8) (Table 3). In terms of treatment outcome, the presence of ototoxicity did not have any statistically significant effect on the treatment outcome; however patients with severe sensorineural hearing loss had a higher proportion with unfavourable treatment outcomes (42.9%) as compared with those with mild hearing loss (19.7%) as shown in (Table 4).
DISCUSSION
Adverse effects continually remain a challenge to long term use of second line anti tuberculosis drugs. Findings from this study show majority of the patients admitted into these specialist sites had some level of ototoxicity. The high prevalence of 72.7% was however similar to findings from studies done among these group of patients in countries like Botswana and South Africa (Modongo et al., 2014). Though, these values were much higher compared to studies conducted in Europe and Asia (Torun et al., 2005; Sturdy et al., 2011; Yang et al., 2017). So also, this study reported a much higher prevalence of ototoxicity compared to a study conducted in Nigeria by Sogebi et al. This disparity could be due to the method of assessing ototoxicity and the relatively smaller study population.
This study also revealed that there was an association between HIV and development of ototoxic effects which is in consonance with most studies that have explored the ototoxic effect of aminoglycosides in multi- drug resistant tuberculosis patients (Harris et al., 2012; Schnippel et al., 2016). A systematic review of studies in sub Saharan Africa also shows an increased relative risk among HIV co infected patients (Hong et al., 2018). Nevertheless, following further analysis this association disappeared emphasizing Modongo et al. (2014) argument that HIV on its own cannot predict ototoxicity suggesting that there are other underlying factors including anti-retroviral drugs in itself which could account for the effect on hearing. Furthermore, prior studies that reported lower prevalence of ototoxicity were conducted in settings with low prevalence of HIV buttressing the effect of anti-retroviral drugs being a predictor of worsening adverse events.
Moreover, increasing age was found to be independently associated with ototoxicity in this group of people which is in line with findings from most studies (Modongo et al., 2014; Sogebi et al., 2017). This is probably consistent because vestibular functions decline with increasing age. Further findings from this study suggest that sputum conversion at the end of the intensive phase could be used as a proxy of detecting some adverse effects of drugs. Though not significant after adjusting other variables, patients who did not sputum convert had a higher proportion with ototoxicity. Most studies have reported on sputum conversion as a predictor of treatment outcome and not on associations with adverse events (Kurbatova et al., 2015). This could be explored further and help in the addressing reversible adverse effects of multidrug resistant therapy before they become permanent.
Considering the treatment outcome of these patients, successful treatment outcome was reported in this study despite the high prevalence of ototoxic effects. These findings are also similar to previous studies. This shows that multidrug resistant tuberculosis programs might be recording high success rates and set targets might have been met in some countries; a lot of debilitating effects which linger on in life are being caused by these treatments. Patients who survive multi drug resistant tuberculosis might in future not be able to compete with their peers and thus leading to productive years lost. Researchers need to shift focus on not just achieving good treatment outcomes but measuring the long-term disease burden following treatment of tuberculosis.
CONCLUSION
High prevalence of ototoxicity exists among multi drug resistant tuberculosis patients following intensive phase of treatment. Increasing age is a major factor for the development of ototoxicity among these groups of people. Caution needs to be taken in managing and monitoring of older patients on multi drug resistant tuberculosis.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Avong YK, Isaakidis P, Hinderaker SG, Van den Bergh R, Ali E, Obembe BO, Dakum PS (2015). Doing no harm? Adverse events in a nation-wide cohort of patients with multidrug-resistant tuberculosis in Nigeria. PLoS One 10(3):e0120161. Crossref |
||||
|
Black RE, Lau WK, Weinstein RJ, Young LS, Hewitt WL (1976). Ototoxicity of amikacin. Antimicrobial Agents Chemotherapy 9(6):956-961. Crossref |
||||
| de Jager P, van Altena R (2002). Hearing loss and nephrotoxicity in long-term aminoglycoside treatment in patients with tuberculosis. International Journal of Tuberculosis and Lung Dieaase 6(7):622-627. | ||||
|
Duggal P, Sarkar M (2007). Audiologic monitoring of multi-drug resistant tuberculosis patients on aminoglycoside treatment with long term follow-up. BMC Ear Nose Throat Disorder 7:5. Crossref |
||||
|
Fausti SA, Henry JA, Schaffer HI, Olson DJ, Frey RH, McDonald WJ (1992). High-frequency audiometric monitoring for early detection of aminoglycoside ototoxicity. Journal of Infectious Disease 165(6):1026-1032. Crossref |
||||
|
Ganesan P, Schmiedge J, Manchaiah V, Swapna S, Dhandayutham S, Kothandaraman PP (2018). Ototoxicity: A Challenge in Diagnosis and Treatment. Journal of Audiology and Otology 22(2):59-68. Crossref |
||||
|
Harris T, Bardien S, Schaaf HS, Petersen L, De Jong G, Fagan JJ (2012). Aminoglycoside-induced hearing loss in HIV-positive and HIV-negative multidrug-resistant tuberculosis patients. South African Medical Journal 102(6). Crossref |
||||
|
Hawkins JE (1976). Drug ototoxicity. Handbook of sensory physiology 5:707-748. Crossref |
||||
|
Hong H, Budhathoki C, Farley JE (2018). Increased risk of aminoglycoside-induced hearing loss in MDR-TB patients with HIV coinfection. International Journal of Tuberculosis Lung Disease 22(6):667-674. Crossref |
||||
|
Ibekwe M, Nwosu C (2016). Pure tone audiometric findings in patients on second-line treatment for multidrug-resistant tuberculosis. Port Harcourt Medical Journal 10(3):97-101. Crossref |
||||
|
Kurbatova EV, Cegielski JP, Lienhardt C, Akksilp R, Bayona J, Becerra MC, Zignol M (2015). Sputum culture conversion as a prognostic marker for end-of-treatment outcome in patients with multidrug-resistant tuberculosis: a secondary analysis of data from two observational cohort studies. Lancet Respiratory Medical 3(3):201-209. Crossref |
||||
|
Modongo C, Sobota RS, Kesenogile B, Ncube R, Sirugo G, Williams SM, Zetola NM (2014). Successful MDR-TB treatment regimens including Amikacin are associated with high rates of hearing loss. BMC Infectious Diseases 14(1):542. Crossref |
||||
|
Schnippel K, Berhanu RH, Black A, Firnhaber C, Maitisa N, Evans D, Sinanovic E (2016). Severe adverse events during second-line tuberculosis treatment in the context of high HIV Co-infection in South Africa: a retrospective cohort study. BMC Infectious Diseases 16(1):593. Crossref |
||||
| Sharma V, Bhagat S, Verma B, Singh R, Singh S (2016). Audiological Evaluation of Patients Taking Kanamycin for Multidrug Resistant Tuberculosis. Iranian Journal of Otorhinolaryngology 28(86):203-208. | ||||
|
Sogebi OA, Adefuye BO, Adebola SO, Oladeji SM, Adedeji TO (2017). Clinical predictors of aminoglycoside-induced ototoxicity in drug-resistant Tuberculosis patients on intensive therapy. Auris Nasus Larynx 44(4):404-410. Crossref |
||||
|
Sturdy A, Goodman A, José RJ, Loyse A, O'Donoghue M, Kon OM, Cooke GS (2011). Multidrug-resistant tuberculosis (MDR-TB) treatment in the UK: a study of injectable use and toxicity in practice. Journal of Antimicrobial Chemotherapy 66(8):1815-1820. Crossref |
||||
| Torun T, Gungor G, Ozmen I, Bolukbasi Y, Maden E, Bicakci B, Tahaoglu K(2005). Side effects associated with the treatment of multidrug-resistant tuberculosis. International Journal of Tuberculosis and Lung Disease 9(12):1373-1377. | ||||
|
Vakulenko SB and Mobashery S (2003). Versatility of Aminoglycosides and Prospects for Their Future. Clinical Microbiology Reviews, 16(3):430-450. Crossref |
||||
|
World Health Organization (WHO) (2016). WHO drug treatment guidelines for drug resistant tuberculosis. |
||||
|
Yang TW, Park HO, Jang HN, Yang JH, Kim SH. Moon SH, Kang DH (2017). Side effects associated with the treatment of multidrug-resistant tuberculosis at a tuberculosis referral hospital in South Korea: A retrospective study. Medicine (Baltimore) 96(28):e7482. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


