Review

ABSTRACT
As the development and upkeep of the United States healthcare becomes increasingly debated in society, the systems in place of other successful countries provide opportunities for erudition and comparison. One country’s system which seems to be consistently overlooked despite its vast improvement to the country is Costa Rica’s universal healthcare. In this comprehensive study of the healthcare systems in both the United States and Costa Rica, there is evidence of a middle ground, as well as areas for improvement to current policies in the United States. Acknowledging the long-term implementation of Costa Rica’s universal healthcare, which was split into three unique major reforms, reveals the need for patience and planning. In the midst of heavy debate regarding healthcare reform, this paper seeks to provide an in-depth analysis of Costa Rica’s history of reform, their current institutions, and recent statistical improvements in overall health, with the goal of providing a better understanding of how the United States should proceed in order to achieve parity.
Key words: Healthcare, healthcare reform, United States, Costa Rica, universal healthcare, history of reform
Abbreviation: ACA, Affordable Care Act; CCSS, Caja Costarricense de Seguro Social.
INTRODUCTION
Over nine years after the latest attempt at reform, the status and future of the United States healthcare system remains a heated controversy among members in political power, employees in the field, and in the general population. During the last century, there have been five official attempts at implementing a system of universal healthcare in the United Sates, of which none were entirely successful. The most recent attempt has been arguably the most controversial to date. The Affordable Care Act (ACA) was signed into law by President Barack Obama in March of 2010. Since then there have been over 60 attempts to reform or repeal it (Obama, 2016).
In truth, no single system will effectively capture every needed aspect of healthcare, but there is undoubtedly room for improvement. With reference to the opinions of incoming professionals and current politics, the United States healthcare system needs reform. In a survey conducted of over 1200 medical students from 10 different United States medical schools, 94.8% believed that our current system requires change Huntoon et al., 2011). Though deemed effective in many aspects, the United States healthcare system consistently demonstrates a lack of efficiency in representing the cumulative population in need, prohibitive expenses that outprice almost every other country, and a declining interest from students in pursuing medical careers due to an increased focus and integration of political matters in hospitals.
Though change is required for future prosperity of the nation, various factors, including financing, and hyper-partisanship of government, make it incredibly difficult to even attempt. The primary obstacle we face is the concept of financing reform. Not only does it take vast amounts of labor, but it also demands millions of dollars for research, public advertisement, and the opportunity cost of time spent planning. A subsequent body of this paper is dedicated to outlining how reform is financed. A second obstacle in our path is the general politics of it. In our current hyperpartisan government, ideas can be advocated for or refuted purely based on the political party presenting. An article written by President Barack Obama (2016), explains how members of government voted against aspects of the ACA that they had supported in a bill presented just 7 years prior. Having voted in favor of near identical ideas not long before, these same individuals backtracked and voted against the ACA when presented by a different party (Obama, 2016). Though not true for every case, having a government that works in an almost exclusively bipartisan fashion can hinder progress and passing of legislation purely based on which party cultivated the idea.
Though challenged with difficult circumstances, work towards reform continues to progress. The system we deal with today is valuable, but it does not maximize its benefits in a universal, cost effective manner. In an effort to compare the pros and cons of the current United States healthcare system, while simultaneously cross referencing them to one of the top existing healthcare institutions based in Costa Rica, this article looks to explain past reform failures, future outlooks, and ultimately propose a solution that may incorporate the beneficial aspects of both systems.
UNITED STATES HEALTHCARE STRUCTURE
In contrast to the health systems currently being utilized in most developed countries, the United States bases its available healthcare off a complex series of private insurances and state programs. The healthcare system can essentially be divided into three categories: Medicare, Medicaid, and Private (Bodenheimer, 2003). This unique structure allows for efficiency and specialization but can be expensive. Concurrent with this condition, there is a clear lack of coverage for many citizens.
Due to the various negative aspects of the United States healthcare system, many times its extraordinary benefits are overlooked. In comparison to other nations, we actually provide healthcare in a much more rapid, specialized fashion. Highly specified education for practitioners leads to impressive treatment capabilities. Alongside this educational system, research is highly prioritized and allows for rapid advancements in the field. The current system incentivizes research experience, which provides an outlet for expansive medical progress in universities and larger organizations (Rice et al., 2013). Our system of specialization differs from other countries in that treatments are higher quality and focus directly on patient symptoms compared to the more generalized treatments from universal physicians. Something that is taken with great pride in the United States are results. The United States ranks among the top in the world when referencing treatment outcomes in several different fields (Rice et al., 2013). Though medical technology and medication in the United States is much further advanced than most other countries, the affordability of such progressive treatments proposes a severe problem in today’s society by making personal access only truly available to those able to cover the expenditure.
Conflicting with the benefits of specialization, inefficiencies relating to resource allocation, expenditure, and coverage remain detrimental to citizens (Lichtenstein 1993). Unlike areas of universal care, physicians in the United States are focused by discipline which allows in depth knowledge, in turn leading to higher quality of treatments based on illness or injury. However, this can also lead to a lack of physicians in certain fields, specifically primary care. Primary healthcare only recruits around 34% of new physicians, which is 11% lower than what is deemed optimal (Lichtenstein 1993). This stems from the incentivization for physicians to allocate themselves based on program type and reimbursement rather than the need of an area. As an example, Bozeman, MT may be short staffed on doctors and require the help of extra specialized physicians, but a bigger city such as Seattle will end up getting those physicians due to location, program, and salary (Xierali and Nivet, 2018). Higher salaries attract more impressive individuals, which can lead to a surplus of one specialty while simultaneously causing a demand for others.
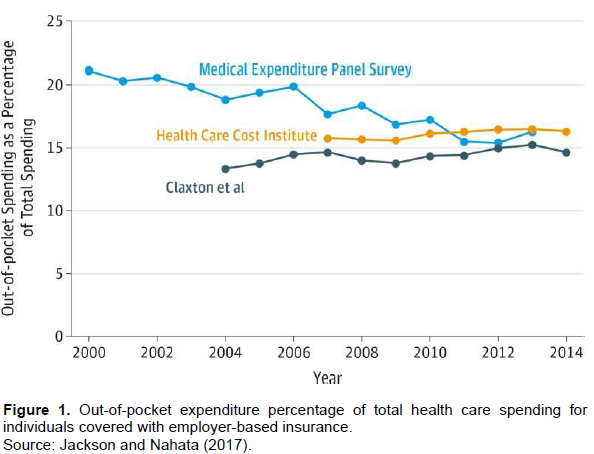
Yet another major flaw in the United States’ system is the inflation of medical care costs due to economical greed, including astronomically high prices for vital medication such as cancer remedies. As there are over 1.6 million new cancer cases annually, it is clear that cancer treatment prescriptions are in high demand. This, in turn, causes corporations that produce said drugs to raise their prices and cost the insurance companies significantly more (Jackson and Nahata, 2017). Due to this fact, many insurance companies have stopped covering cancer treatments, leaving families to pay millions out of pocket. Figure 1 shows the steep out of price expenses for individuals with specific coverage. Even though these employees have health insurance, 15-20% of all health expenditures are still out of pocket. This is a high expense as 15% of hospital bills can cost tens of thousands of dollars depending on the procedure. Though the idea of “pay for quality” seems just, it fails to take into account the price inflation of new medical drugs.
This allows insurances to pick and choose which individuals they will cover, and base it off risk. Lower insurance rates are offered to low risk groups, leaving those deemed “high risk” unable to afford coverage. For this reason, elder citizens and those who are disadvantaged must turn to state programs such as Medicare and Medicaid.
Data for the Medical Expenditure Panel Survey (MEPS) report were calculated from MEPS Household Component. This displays the percentage of out-of-pocket expenses for nonelderly citizens claiming full-year employer coverage. Data for the Health Care Cost Institute (HCCI) report were calculated from the HCCI claims database reported in (Herrera et al., 2013), HCCI (2014, 2015), both data sets utilized the most current values reported annually. Data for the Claxton et al. (2016) report was calculated from the analyses of the Trueven Marketscan reports by Claxton et al. (2016).
Recent reform
Healthcare systems in the United States have gone through only several successful reforms, despite there having been a high number of attempts (Hirsch et al., 2020). The most recent successful attempt occurred almost a decade ago in 2010 led by President Barack Obama. Via the Affordable Care Act, new legislation was passed to form a more universal approach to healthcare which strongly restricted private insurance company power. The biggest change which stemmed from the ACA was directed towards how insurance companies could provide coverage. Rather than focusing on medical background, economic standing, and living location, insurance companies could only review customers based on age and gender (Pant et al., 2017). This led to over nine million previously uninsured citizens being covered within a month’s time (Hall and Mark, 2014). The ACA was primarily directed at who was allowed to be covered, not how the system was set up. The passing of this legislation led to an eruption of dispute and contradiction, mainly due to the large loopholes it created. Since insurance agencies cannot set premiums based on preexisting conditions, they would most likely just deny people healthcare altogether rather than offer it at a more expensive rate. Not only this, but forcing insurance agencies to cover previously existing healthcare issues would allow for citizens to simply not purchase healthcare until after they actually need it (Taylor, 2012). The new system allows for a major increase in coverage, but in return causes major loopholes that citizens can expedite in order to receive healthcare similar to others who are paying more.
Reform may be needed, but pushing for actual change is expensive, both monetarily and timely (Geyman, 2003). In the last century, true reform has been attempted five times, and has failed all five times. True reform here refers to change to the overarching system, not just small reforms that adjust the current system in place. One of the biggest problems faced when pushing for change is propaganda put forth by major companies in order to contradict any movement for reform. According to JP Geyman of the Department of Family Medicine at the University of Washington, there are six main myths that big companies push to repel change (1) "Everyone gets care anyhow;" (2) "We don't ration care in the United States"; (3) "The free market can resolve our problems in health care"; (4) "The U.S. healthcare system is basically healthy, so incremental change will address its problems;" (5) "The United States has the best health care system in the world"; and (6) "National Health Insurance is so unfeasible for political reasons that it should not be given serious consideration as a policy alternative" (Geyman, 2003). Each of these arguments have been debunked through convincing evidence, yet continually advertised my larger insurance agencies. Another difficulty comes in the face of bipartisan government. Hyper partisanship leads to voting based on who brings forth the legislation, not the content of the actual bill. How specific republican candidates voted against the ACA, after backing a very similar bill just seven years prior (Bodenheimer, 2003), have been earlier discussed in this work. Many citizens acknowledge the need for change in our healthcare system, but the obstacles which prevent reform is less commonly known.
COSTA RICA’S HEALTHCARE STRUCTURE
Healthcare in Costa Rica is unique in both structure and function. Contrary to popular practices, the system in Costa Rica actually provides three different services: health, water, and sanitation services. Water and sanitation services are controlled by the government in a public fashion; however, the health division is partitioned into two sectors, public and private (SáenzMdel et al., 2011). The public health sector is run by the Caja Costarricense de Seguro Social (CCSS), an institution funded almost solely by employers and the state. The CCSS has individual buildings to provide services which include maternity/illness insurance, disability, and life insurance. This coverage is universal to citizens which causes heated debate due to funding sources compared to who benefits from it. The private sector is set up somewhat similarly to the United States in that hospital care coverage comes from either private insurance premiums or out of pocket expense (SáenzMdel et al., 2011). Along with all systems, there are both benefits and costs to Costa Rica’s tertiary setup, many of which the United States can use educationally. The fundamental idea of universal healthcare has a negative connotation, yet when implemented successfully can be beneficial to all parties.
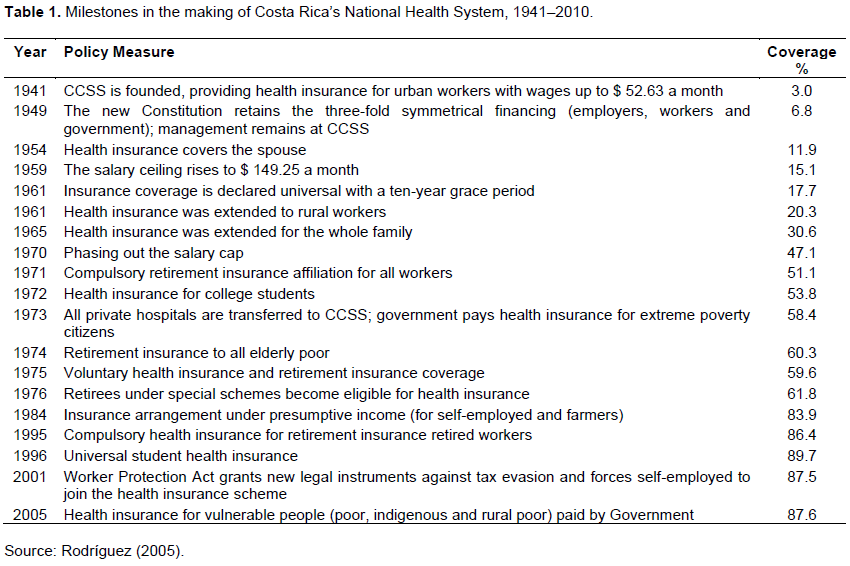
One of the most evident benefits of Costa Rica’s healthcare system is the extended outreach. Successfully providing universal healthcare is an impressive expansion from the social security measures that covered only 5% of the population in 1940 (Vargas and Muiser, 2013). As seen in Table 1, in just 60 years, CCSS was able to grow its coverage from 5% to just over 88% of the 4.6 million legal Costa Rican citizens. Even with such a substantial increase, the total health spending still only represents 11% of their total GDP (GHO, 2002). This is substantially lower than the United States which currently spends 17.7% of its annual GDP on health expenses (Centers for Medicare and Medicaid Services,1960). This clear difference in health expenditures stems from the basic systems that are set. Costa Rican citizens are provided free universal health care in which the only expenses come from employers, businesses, and government institutions. The United States has a significantly greater portion of citizens covered via private insurance, leading to a much greater cost regardless of a smaller percentage benefitting from it (Jaramillo, 2004).
History of reform
In order to sustain a movement for universal healthcare, Costa Rica essentially resorted to a three-part reform that took place over a 30-year period, allowing for slow implementation which worked through the controversies at hand before moving on. Prior to the 1940s, which is when the first major reform occurred, economic growth was static yet there were three developments which presented a grace period where citizens were ready for reform: primary education was established as mandatory for citizens in 1888 (US Census Bureau, 2019), the Ministry of Health was founded and officially implemented in 1922 (Palmer, 2003), and democratic institutions began to thrive (Sojo, 2010). The first reform took place in 1940 with the establishment of the CCS, a public institution set in place by President Calderon, to provide health and pension benefits to white collar employees. This course of action set up the foundation from which universal healthcare would stem (Sáenz et al., 1994). By establishing a system where health benefits were provided to all manual employees, it began a process advocating for the expansion of that same coverage.
Just 30 years later came the second major reform, noted by the expansion of social democracy, a sharp decline in infectious disease which had previously been the leading cause of death, as well as healthcare delivery reaching an all-time low in cost. This led to a spike in the population, and a drop off of unemployment. Having more white-collar employees allowed for a massive increase in CCSS health coverage, which rose non-fold to 39% (Mata and Rosero-Bixby, 1988). Not only that, but during this section of socio-economic reform there was a 300% improvement in maternal mortality rate during childbirth, population with access to sanitation reached 86%, and employee medical doctors tripled (Mohs, 1995). This second period of reform was centered around an overall improvement in national health, political transform towards democracy, and a rise in coverage from the CCSS. There is a clear correlation with the increase in coverage and the improvement of national well-being.
The third major reform was the most well known, labeled as “the primary healthcare reform” due to its emphasis on the implementation of excelling primary care.
Over the last 40 years, the CCSS had matured to a state where laws and methods of taxation were in place to keep them fully funded and allow them to cover healthcare costs of those unable to pay. Due to growth of the institution and long-term savings, the CCSS now had the resources and incoming revenue to provide universal health care to the point where the ability to receive coverage is available to all citizens regardless of socio-economic status. With over 94% of today’s Costa Rican population receiving health care (Caja Costarricense de Seguro Social, 2012), and studies showing a dramatic increase in overall citizen health after the third reform (Bixby, 2004), it is easy for us to see that successful implementation of universal healthcare is not only possible but also significantly beneficial.
Disadvantages of the system
As with all working systems, there are definitive limitations when regarding universal healthcare, the biggest of which is its reliance on the economy. Considering a major source of funding for Costa Rica’s system comes from large businesses, employers, and government institutions, the efficiency of its healthcare is volatile, fluctuating with economic performance. During an economic boom, healthcare shows excessive proficiency in medical advancement and treatment success rates. However, during recessions, such as the crisis of the 1980s, it can be seen to halt or even reverse the improvements that were abundantly clear throughout the 1970s. This specific recession showed a clear deterioration in overall health, increasing struggles in the government's financial ability to uphold medical services, a higher dependence for foreign aid and intervention in order to stabilize healthcare, and the introduction to a large period of citizen debate over the worthiness of the system (Morgan, 1987). During the economic crisis, Costa Rica’s biggest asset was their political stability, which in turn lead to a spike in immigration as political turmoil caused social unrest in the neighboring countries. This jump in population became the basis for a second limitation for the implementation of healthcare, population size. It made what was an already high healthcare expense even more difficult to maintain. This caused them to seek international help and appeal for loans from other countries which they are still working to repay (Ramos, 1988). It is evident that healthcare reform is not only timely, but financially costly which means that in order to be successful, the country must be in good economic standing. In order to reach the highest level of success, it is important to find a median where extensive healthcare coverage is maintained, and the efficiency of provided care is as independent as possible of the economy.
OVERALL COMPARISON
The leading difference in the healthcare systems in the United States and Costa Rica stems from the countries advancement itself. The United States is a more mature, longer developed country established 45 years prior to Costa Rica which gained independence in September of 1821 (Pant et al., 2017). 45 years of maturation, growth, and development provided a more stable environment during the implementation of institutional healthcare. Costa Rica’s movement for reform came at a period of much needed expansion. When the motion began in the 1940s, Costa Rica was suffering from low sanitation outreach, poor water availability, and high rates of infant mortality coinciding with low life expectancy. For this reason, their best course of action was to get healthcare out to as many people as possible, regardless of the quality. In order to improve their overall state of wellbeing, they need to provide outreach, that is, as extensive as possible. An even bigger factor in Costa Rica pushing for universal healthcare is that their minor population of just under 5 million citizens (The World Factbook, 2019) is much more manageable than the United States which houses more than 331 million inhabitants (US Census Bureau, 2020). Universal healthcare is more achievable in small countries as there is a smaller base of citizens requiring coverage. Providing free healthcare to 5 million people is understandably easier than attempting to do the same for 331 million.
Lessons for future reform
The biggest takeaway from this study is that healthcare systems and implementation take extended periods of time. In order to provide a successful system, multiple step plans are necessary. Single legislations and movements are in progress, but not enough to fully advance an institution. Aside from time, a country must find a period of economic prosperity and stability as reform is monetarily expensive. Specifically, pushing for extended coverage and government financing requires extensive savings and funding from taxes, reserve backing, and in some cases international help.
Another lesson to be seen is that financing of healthcare must be diversified. Similar to a general investment portfolio, healthcare cannot rely on funding from one or two main sources. When a large percentage of the allotted budget comes from a small source base, it can be easily influenced, and negative impacts are likely during times of economic disparity. This is where private insurance companies become most beneficial. If public sources fall into a rut, having private insurance can be a way of ensuring quality care. This could also then provide an incentive for people to maintain private insurance if they can afford it rather than just accept the free healthcare provided.
Reform also requires intense compromise. A big push back of reform comes from large corporations, such as the pharmaceutical industry, feeling threat to their profits (Karlin-Smith and Norman, 2016). In order to provide affordable healthcare at an extensive range, the companies which produce drugs need to agree to even the most modest of changes. Without large public company backing, reform can be shot down due to previously mentioned propaganda.
CONCLUSION
Providing healthcare is intensely complex due to the multitudinal influential tradeoffs. Examples include looking to provide quality healthcare through specialization, but also needing to keep medical professionals for primary care; wanting to expand coverage but reduce financial burdens; and pushing for change while simultaneously wanting to maintain systemic stability.
The United States is uniquely advanced due to large investments in research and technology, with a large focus on extended education for specialty focuses. It is a system which provides quality that is among the highest in the world and allows for quick treatment without requiring appointments months in advance. However, it is also a system that is extremely expensive, as even with insurance a broken leg could cost up to $7500 in out of pocket expenses, with a 3-day hospital stay reaching up to $30,000 (US Healthcare 2020). It is a system that requires someone to pay for it no matter the treatment kind (MIT Medical, 2019), which provides an unfortunate business type backbone for all institutions, focusing on profits over personal care.
Costa Rica’s healthcare is one of the most overlooked and understudied considering their high levels of success in recent years. Through employer, corporation, and government funding, 94% of citizens receive free healthcare. Their system shows an emphasis on primary healthcare, and success rates were shown through massive decreases in infant mortality rate, increases in life expectancy, and larger access to sanitation and clean water within the first 2 decades of the first reform. Its success stems from a combination of systems, where businesses and governments can afford private insurance, while lower class citizens are still provided coverage through the universal system.
Though the current systems are efficient in many aspects, lessons can still be learned through the observation of other international institutions. First is that reform is successful when given long periods of time for adjustment. Costa Rica’s three-part implementation allowed for progress to be made once previous progress was successful. Reform also requires stable economic standing with good international relations. It is an expensive process which could put a monetary burden and lead to national debt if not done during a time in which it could be afforded. Alongside this, the budget for healthcare must be diverse so as not to rely too heavily on the economy which can in turn significantly impact it through booms and busts. Reform is a compromise which requires agreements from citizens, major corporations, and government officials. It is a timely, and expensive process that, when done right, can lead to massive benefits for all citizens.
A follow up review could be conducted to ensure the success of Costa Rica’s healthcare is maintained as the population continues to grow. Considering the system is still fairly new, it would be worthwhile to do a secondary analysis in several years to see if the rates of coverage remain the same with an increasing population. A follow up study can be done to ensure that this data can apply to a bigger scaled nation such as the US.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
"GHO | By Country | Costa Rica - Statistics Summary (2002 - Present). World Health Organization, World Health Organization, |
|
|
The World Factbook (2019). Costa Rica." Central Intelligence Agency, Central Intelligence Agency, |
|
|
Bixby LR (2004). Assessing the impact of health sector reform in Costa Rica through a quasi-experimental study. Pan American Journal of Public Health 15(2):94-103. |
|
|
Bodenheimer T (2003). Primary care in the United States.Innovations in primary care in the United States. BMJ (Clinical research ed.) 326(7393):796-799. |
|
|
CajaCostarricense de Seguro Social (2012).Blog de Noticias; CCSS ofrececobertura con EBAIS al 94% de la población; 2012. |
|
|
Centers for Medicare and Medicaid Services (1960). "Historical." CMS, |
|
|
Claxton C, Levitt L, Long M (2016). Payments for cost sharing increasing rapidly over time. Peterson-Kaiser Health System Tracker. |
|
|
Geyman JP (2003). Myths as Barriers to Health Care Reform in the United States. International Journal of Health Services 33(2):315-329. |
|
|
Hall MA, Lord R (2014). Obamacare: what the Affordable Care Act means for patients and physicians. BMJ 349:g5376. |
|
|
Health Care Cost Institute (HCCI) (2014). Health care cost and utilization report. |
|
|
Health Care Cost Institute (HCCI) (2013). Out-of-pocket spending trends. |
|
|
Herrera CN, Gaynor M, Newman D, Town RJ, Parente ST (2013).Trends underlying employer-sponsored health insurance growth for Americans younger than age sixty-five.Herrera CN, Gaynor M, Newman D, Town RJ, ParenteSTHealthAff (Millwood). Oct; 32(10):1715-1722. |
|
|
Hirsch JAMD, Benyamin RAMD, Manchikanti LMD, Helm IISMD (2020). Evolution of US Health Care Reform. |
|
|
Huntoon KM, McCluney CJ, Scannell CA, Wiley EA, Bruno R, Andrews A, Gorman P (2011). Healthcare reform and the next generation: United States medical student attitudes toward the Patient Protection and Affordable Care Act. PloS ONE 6(9):e23557. |
|
|
Jackson K, Nahata MC (2017). Rising Cost of Anticancer Medications in the United States. Annals of Pharmacotherapy 51(8):706-710. |
|
|
Jaramillo J (2004). Historia y EvolucióndelSeguro Social de Costa Rica. San José: EDNASSS. |
|
|
Karlin-Smith S, Norman B (2016). Pharma unleashes on Part B demo. Politico. |
|
|
Lichtenstein RL (1993). The United States' health care system: problems and solutions.Survey of Ophthalmology38(3):310-316; discussion 316-7. |
|
|
Mata L, Rosero-Bixby L (1988). National Health and Social Development in Costa Rica: A Case Study of Intersectorial Action. Technical Paper N.13. Washington, DC.Pan American Health Organization. |
|
|
MIT Medical (2019).Internationals."Healthcare in the United States: The Top Five Things You Need to Know | MIT Medical. Source: |
|
|
Mohs E (1995). LaReformadel Sector Salud en Costa Rica Durante la Década del 70. San José: UNICEF. [Google Scholar] [Ref list] |
|
|
Morgan LM (1987). Health without Wealth?Costa Rica's Health System under Economic Crisis. Journal of Public Health Policy, U.S. National Library of Medicine, |
|
|
Obama B (2016). United States Health Care Reform: Progress to Date and Next Steps. JAMA, 316(5):525-532. |
|
|
Palmer S (2003). From Popular Medicine to Medical Populism.Durham: Duke University Press. |
|
|
Pant S, Burgan R, Battistini K, Cibotto C, Guemara R (2017). Obamacare: A View From the Outside. Hawai'i journal of medicine & public health : a journal of Asia Pacific Medicine & Public Health 76(3 Suppl 1): 42-44. |
|
|
Ramos J (1988). Costa Rica Turns to the World for Help. Integration (Tokyo, Japan), U.S. National Library of Medicine, July, |
|
|
Rice T, Rosenau P, Unruh LY, Barnes AJ, Saltman RB, van Ginneken E (2013). United States of America: Health system review. Health Systems in Transition 15(3):1-431. |
|
|
Rodríguez A (2005). La Reforma de Salud en Costa Rica. Santiago: CEPAL. |
|
|
Sáenz O, Vargas JR, Vargas JR, Saenz JO, (1994). Costa Rica en Cifras II.mimeo. Costa Rica en Cifras. San José: MIDEPLAN - PNUD;. |
|
|
SáenzMdel R, Acosta M, Muiser J, Bermúdez JL (2011). The health system of Costa Rica.SaludPublica Mex.53 Suppl 2:s156-167. |
|
|
Sojo C (2010). Igualiticos - La Construcción Social de la Desigualdad en Costa Rica. San José, Costa Rica: PNUD. |
|
|
Taylor JS (2012).The Carelessness of Affordable Care. Hastings Center Report 42:24-27. |
|
|
United States. Department of State.Bureau of Public Affairs.Office of Public Communication (1992).Costa Rica.Department of State Publication. Background Notes Series, U.S. National Library of Medicine, June. |
|
|
US Census Bureau (2019). Health Insurance Coverage in the United States: 2018. The United States Census Bureau, 8 November. |
|
|
US Census Bureau (2020).U.S. and World Population Clock. Population Clock. |
|
|
US Healthcare (2020).Health Coverage Protects You from High Medical Costs. HealthCare.gov, |
|
|
Vargas JR, Muiser J (2013). Promoting universal financial protection: a policy analysis of universal health coverage in Costa Rica (1940-2000). Health Research Policy and Systems 11:28. |
|
|
Xierali IM, Nivet MA (2018). The Racial and Ethnic Composition and Distribution of Primary Care Physicians. Journal of Health Care for the Poor and Underserved 29(1):556-570. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


