Full Length Research Paper

ABSTRACT
Health systems face multimorbidity as the leading cause of the burden of disease and demand for healthcare services. Although non-communicable diseases are well known, and countries in Latin America have implemented strategies to its approach, tackling multimorbidity is still a challenge and an emerging topic. In response to this, Centro de Innovación en Salud ANCORA UC, in association with Servicio de Salud Metropolitano Sur Oriente and the National Health Fund, implemented a pilot study a Multimorbidity Patient-Centered Care Model in the health network. The objective was to evaluate the health care services utilization and mortality. The authors performed a cohort study with adults with non-communicable diseases, stratified by ACG® System. Analysis used logistic regression, adjusted by confounding variables. The intervened group had a significantly lower incidence of hospital admissions, length of stay, number of consultancies to hospital emergency, and number of consultancies to primary care emergency than the control group. Further, it was associated with significantly less mortality (OR 0.54; 95% CI 0.47 – 0.63). Barriers and facilitators proper from a complex intervention were approached. The model showed positive results in mortality and health services utilization. A description is provided to contribute to this emerging topic and facilitate its reproducibility.
Key words: Multimorbidity, patient-centered care, risk stratification, impact analysis.
INTRODUCTION
Multimorbidity has become the first cause of the burden of disease and the primary determinant of demand for healthcare services in the health systems worldwide (Hajat and Stein, 2018). In a pandemic context, the impact and growth of multimorbidity and the effects of COVID-19 will probably be the main problem in the coming years (Mair et al., 2020; Wold Health Organization, 2020). Demographic change, modern lifestyles, and increased life expectancy have contributed to a high prevalence of multimorbidity, especially in 65 years of age patients (Leijten et al., 2018; Margozzini and Passi, 2018; Nguyen et al., 2019; Palmer et al., 2018). Moreover, multimorbidity appears 10 to 15 years early in people with lower socioeconomic levels, deepening health inequalities (Nguyen et al., 2019; OPS/OMS, 2019). The negative impact of multimorbidity not only decreases the quality of life at mid-life (Kanesarajah et al., 2018), it also leads to higher mortality rates (age at death: increased in 6,3 with four or more NCDs (Diane Zheng et al., 2021; Menotti et al., 2021)and greater healthcare services utilization, (de Souza and Braga, 2020; Heins et al., 2020; Leijten et al., 2018).
Hence, health systems are facing the challenge of a care delivery based on individual diseases that needs to transit towards a patient-centred care with multimorbidity approach (Margozzini and Passi, 2018; Pearson-Stuttard et al., 2019).
Today´s available evidence has shown that an organization based on patient-centered care for patients with noncommunicable diseases (NCDs) can result in positive health outcomes. Although there is still no consensus on a standardized international strategy to follow, shifting towards a patient-centered care model seems to be today the best alternative for multimorbidity approach (Barros et al., 2019; Kuluski et al., 2016; Poitras et al., 2018). In addition, international experiences have shown that risk stratification, continuity of care, self-management strategies, shared decision making, and individual care plans result in positive outcomes (Poitras et al., 2018)(Palmer et al., 2018).
Implementing these elements in the health system requires a complex process involving structural, organizational, cultural, and political changes. Probably because when particular strategies are implemented in different contexts and jurisdictions, they face local barriers that deliver in adaptations of these intervention strategies (Navickas et al., 2016)(Palmer et al., 2018). Descriptions on the literature are often very general, probably because the approach for multimorbidity is still an emerging topic in constant growth (Leijten et al., 2018; Poitras et al., 2018; Smith et al., 2021).
Back in 2003, Chile began a health system reform that included essential components such as: the introduction of explicit guarantees regarding the care of selected problems (GES) and the change of care model towards the family health model and community. Since then, despite people-centered model, as proposed by the Family and Community Health Model (de Almeida et al., 2018; Dominguez-Cancino et al., 2020; Montero et al., n.d.), care approach is still focus on identifying and treating diagnostics in the context of disease-specific programs (Ministerio de Salud; Gobierno de Chile, 2017; MINSAL Chile, n.d.). However, these programs operate as structured protocols that provide separate management for each diagnosis; they are not synchronized with the other care services that each person requires, especially if they suffer from several diseases. Consequently, patients receive a fragmented care, with lack of coordination, prescribing frequently redundant and contraindicated medications, affecting the safety and efficiency of care (4,22,23).
As response, in 2017 Centro de Innovación en Salud ANCORA UC (CISAUC), Faculty of Medicine, Pontificia Universidad Católica (PUC), in association with the Servicio de Salud Metropolitano Sur Oriente (SSMSO) and the National Health Fund (FONASA) implemented the “Multimorbidity Patient-Centered Care Model” (MPCM) (Tellez et al., 2020), as a pilot intervention at the public health network. It aimed to reorganized care delivery to incorporate a multimorbidity approach based on risk stratification and other five core elements. The objective of this study is to evaluate the impact on utilization of health care services (Hospital admissions, length of stay, and emergency room consultations) and mortality.
MATERIALS AND METHODS
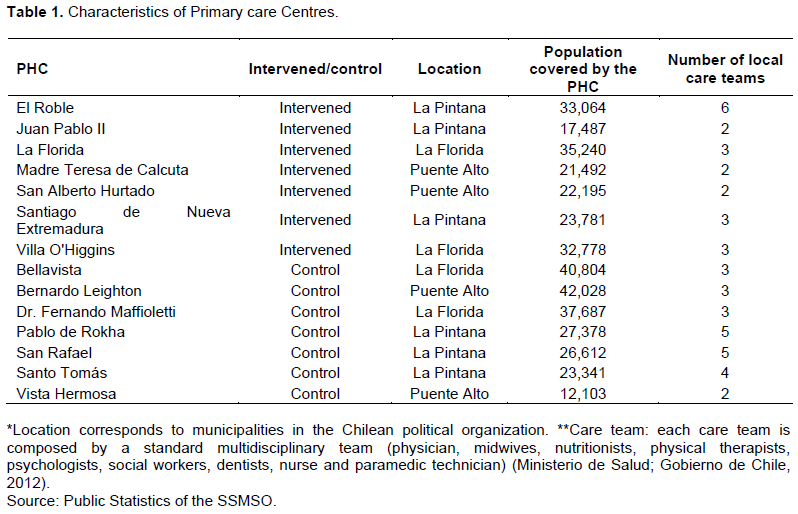
The authors conducted a cohort study with secondary data routinely collected by the Unidad de Gestión y Análisis de la Información of the SSMSO between April 2017 and December 2019. The intervened primary health centres (PHC), were compared with non-intervened PHC that maintained the standard single diagnosis approach for NCDs. PHC were located in the southeast of the Metropolitan Region, Chile and were selected seeking similar size, geographical location and socioeconomic characteristic, being blind to health care team composition. Data about the PHC is summarized in Table 1.
Population
The studied population were patients older than 15 years who were already enrolled in each PHC. Person’s data were processed with the Johns Hopkins ACG® System (Adjusted Clinical Groups, ACG), which uses existing data from, for example, medical records and demographic characteristics to model and predict individual health over time (ACG System Excerpt from Technical Reference Guide, 2009). A study on the use of the ACG system to classify risk and the potential use of resource allocation mechanism PHC shows that they fit well with the Chilean population ((Santelices et al., 2014).
Patients were selected following two steps. First, an ACG processing was done by the SSMSO with all the available data of the health network, including primary, secondary, and tertiary care. They were segmented into three groups according to criteria of ACG: (1) High risk defined by a RUB (Resource Utilization Band) 4-5, two or more chronic conditions, the current consumption of three or more medicines; (2) Moderate Risk defined as a RUB 3 and one or more chronic conditions; and (3) Low Risk defined by a RUB 1-2, and one or more chronic conditions. Second, we applied the following exclusion criteria: for high-risk persons, we exclude patients receiving palliative care, currently pregnant, confirmed cancer diagnosis or terminal stage 5 renal diseases, severe physical dependencies or disabilities, drug/alcohol addiction, immunosuppressive transplants. Finally, we excluded patients currently receiving palliative care, severe physical dependencies, or disabilities for moderate and low-risk persons. These criteria were applied to both groups, intervened/control.
The exclusion criteria mentioned above, such as palliative care, currently pregnant, confirmed cancer diagnosis or terminal stage 5 renal disease, severe physical dependencies or disabilities, were applied mainly because, in our health system, these health problems have specific programs that provide sufficient health services (Ministerio de Salud; Gobierno de Chile, 2005, 2011, 2015; Ministerio de Salud, 2009; Subsecretaria de salud publica, división y control de prevención de enfermedades, 2018). Therefore, adding case management services would result in an over-intervention for patients without achieving the expected effects.
After exclusion and inclusion criteria for patients of high risk, an average of 37% were eligible for this intervention; for moderate and low-risk eligibility, average 95%. The number of participants was 32,881 unexposed and 20,642 exposed. Recruiting was dynamic, enrolling patients during their health attention. The matching process was done according to the personal characteristics of each patient, like age, gender, and comorbidities.
Recruitment
High-risk person’s data were given to the local clinical team by the SSMSO. They were contacted through phone calls. If persons cannot be reached by phone, a nurse technician makes a home visit to enrol the person. If the person is hospitalized, enrolment was done by a Nurse Case Manager in coordination with the secondary level. An individual informational session was held with each enrolled person to communicate the general aspects of the upcoming changes and the new model of care. Moderate and low-risk persons were enrolled at the first visit with members of the primary care team. In this visit, health professionals elaborated the individualized care plan and explained the new model of care to the patient.
Some patients were not available to enrol mainly were because the phone number didn´t work or there wasn’t a valid address. The users who rejected the intervention were mainly categorized as high risk, and the reason for rejection was that they could not attend the case management activities, which required frequent face-to-face contact.
Multimorbidity patient-centered care model (MPCM)
The MPCM is a complex health intervention built from the best international and national experiences found in the literature (Tellez et al., 2020)describing patient-centered care with multimorbidity approach. Core elements such as risk stratification, self-management, shared participation and responsibility, continuity of care, and case management (only for high-risk persons) offer differentiated care according to each person's risk (Figure 1). The description of the elements is the following:
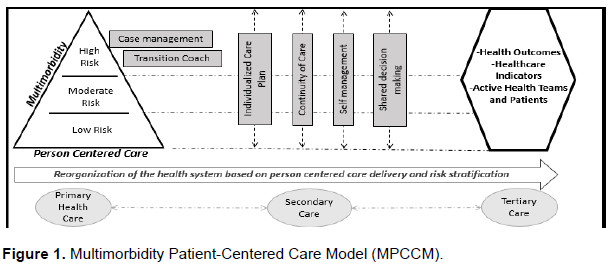
1) Risk stratification: Based on Kaiser Permanente Model (McCarthy et al., 2009), risk stratification aims to keep sick people under control and avoid complications, encouraging their involvement, autonomy, and support from health teams. It also facilitates the reorganization and frequency of care services according to patients risk (Consejería de Salud de la Comunidad de Madrid, 2013).
2) Self-management: Increases skills and self-confidence that persons require to manage their NCDs and prevent complications (Ministerio de Salud Argentina, 2013; Ministerio de Salud de Chile, 2013). Significantly, conducting education in small groups can improve behaviours, health outcomes, communication with providers, and reduce services use ([NIH] et al., 2013).
3) Shared participation and responsibility: Express in the agreed plan, allows patients to incorporate their values, lifestyle ??and daily routine in medical treatment beneficiating their health. Hence, professionals facilitate the identification of the patient motivations through motivational strategies based on the Motivational Interview Style (Mercado et al., 2008; William R. Miller, n.d.).
4) Continuity of care: Coordination and continuity of care through health care teams, including horizontal and vertical integration on the health network, can deliver better decision-making about patient care (Ministerio de Salud; Gobierno de Chile, n.d.). Coordination between Hospital and PHC professionals in discharge planning facilitates the continuity of the care process, follow-up and could reduce 18% hospital readmissions (Gonçalves-Bradley et al., 2016)and increase the time to readmission (Consejería de Salud de la Comunidad de Madrid, 2013).
5) Case management: Essential high-risk patients approach, potentially having fewer services utilization of complications from NCDs (McCarthy et al., 2009; Tortajada et al., 2017). The process of planning, facilitation, coordination of care, evaluation, and advocacy for obtaining services in order to understand individual and family health needs, can promote cost-effective results and quality (Shilpa et al., 2011).
The model introduced an individualized care plan that listened to patients´ priorities, for which we restructured care teams and defined new roles to nurses, family health practitioners, general practitioners, allied health professionals, and auxiliary staff. In addition, coordination and follow-up of continuity of care across health networks were done by a specialized team, which improved person information delivery and primary healthcare continuity.
The primary team included a nurse case manager, clinical pharmacist, trained general physician, a nurse technician, and a nurse coordinator in the secondary and tertiary care for high-risk persons. Activities such as integrated initial evaluation, phone counselling, family counselling, self-management workshops, phone follow-up for drug adherence, and others were offered according to the individualized care plan. Also, operational changes were made to facilitate the implementation, such as incorporating a unique chronic registration form and unique permanent drugs prescription. In addition, when persons were hospitalized or consult emergency room, transition coach services were offered during their stay. Upon discharge, primary care received the information about the patient's hospitalization to guarantee continuity of care.
Moderate and low-risk persons differ from high-risk persons in the quantity and periodicity of the services provided. For example, this group does not receive case management services. Furthermore, it is expected that low-risk persons have little face-to-face contact with the primary care team because we implemented strategies that support remote self-management, including more capacities to identify situations that require professional assistance.
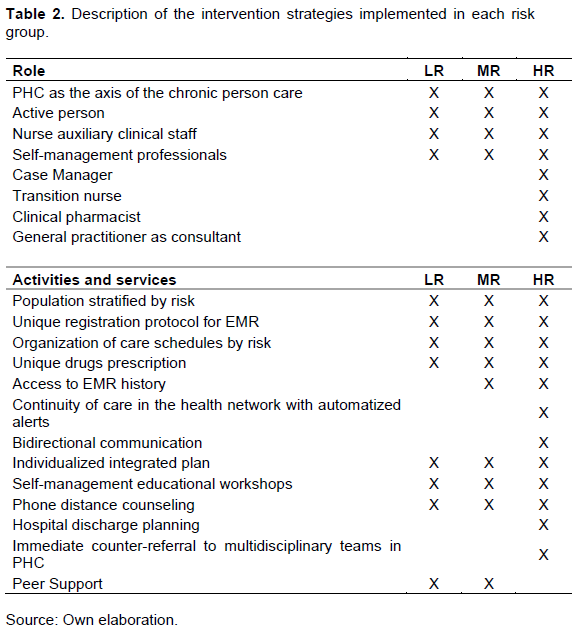
The variety of activities and services are offered in primary care, and specialty levels can vary in periodicity and intensity. As long as persons and their families gain competencies and improve their self-management, self-confidence, and knowledge of the health network, services can decrease. The description of the new roles, activities, and services that were implemented are summarized in Table 2, organized by risk, in high risk (HR, moderate risk (MR), and Low Risk (LR).
The implementation process considered the local characteristics of the territories, the preparation of the health teams, and the review of the organizational and operational conditions to adopt the new interventions. The process was the following: preparation and training of health teams, start-up, monitoring, and continuous improvement. During this process, the essential elements of the MCMP were put into practice in their vast majority, observing only one PHC where the process was slower than others. As the health system operates with rigid inertia, it was challenging to implement such reorganization in this structure. However, fortunately, the basis and central concepts that MCMP relies on aligned with the PHC philosophy, especially the Comprehensive family and community health model (Ministerio de Salud; Gobierno de Chile, 2012).
In order to support the incorporation of new roles and intervention strategies, periodic monitoring and advice were carried out to the teams of the pilot centers to favor the implementation process and its fidelity to the proposed model. This consultancy was carried out by a multidisciplinary team addressing operational, technical, and change management issues.
Outcomes
The impact was assessed on the following outcomes: (1) death by all causes; (2) number of hospital admissions; (3) length of in-hospital stay; (4) number of consultancies to hospital emergency; and (5) number of consultancies to primary care emergency. The following confounder variables adjusted the effect estimate: (1) sex; (2) age; (3) number of comorbidities; (4) time enrolled; (5) ACG RUB category; and (6) insurance category. Selection bias was addressed by confounding variables. ACG RUB was a discrete variable of 6 categories, between 0 and 5, where a higher category means higher utilization resources. The insurance category was a covariate of 8 categories related to the socioeconomic level of each person.
Statistical analysis
Binary outcomes were analysed using logistic regression. Count variables were analysed using zero-inflated models given the high proportion of zero’s in all these variables. Poisson and negative binomial were evaluated in all cases, choosing negative binomial for all variables because it showed better goodness of fit according to the Akaike information criterion. For descriptive analysis, we showed the univariate (crude) analysis results to compare intervention and control groups. All models were adjusted by the set of confounding variables indicated above. Analyses were performed in STATA 14. For the variables used in this study, it was found that the data highly complete, that is, the amount of missing data was never higher than 5% of the data in each variable. No multiple imputations were performed.
RESULTS
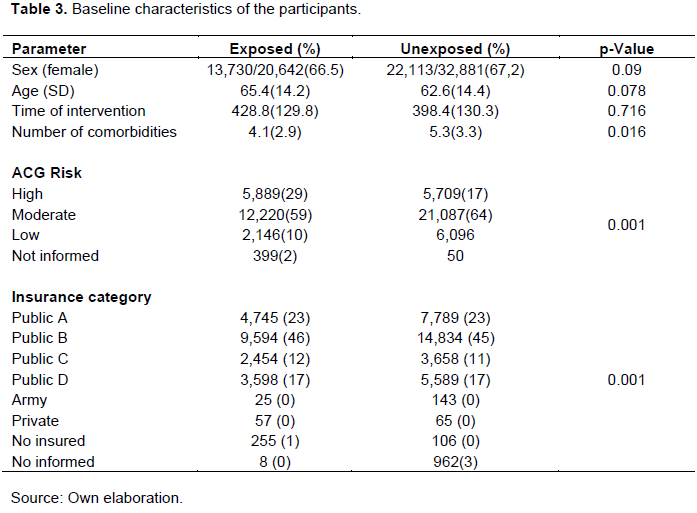
The analysis of results was carried out based on a population of 32,881 unexposed to the intervention and 20,642 exposed. The loss of participants during the study was 17% for high-risk persons and 2% for moderate and low-risk persons and the main reason was death (75%). Table 3 presents baseline characteristics of the patients of the study. As can be observed, all variables showed statically significant differences between groups, which is expected in the context of real-world data.
The impact analysis is summarized in Table 4. After a median time of intervention of 426 days from enrolment, we found that the intervention was associated with a statistically significant lower odds of death (OR 0.54; 95% CI 0.47 - 0.63) and also a lower odds of “at least one hospitalization” (OR 0.69; 95% CI 0.57-0.83). In addition, the incidence rate of the number of hospital admissions, length of hospital stays, number of consultancies to hospital emergency, and the number of consultancies to primary care emergency showed to be significantly lower in the intervention group than the control group. It is essential to highlight that these variables contained many zeroes, considered in the zero inflate two-part model for the estimation.
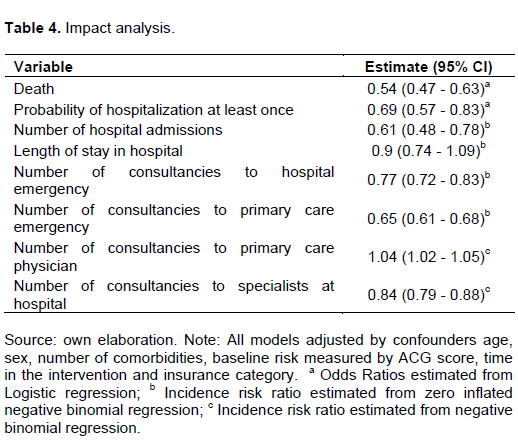
Finally, the incidence rate of the number of consultancies to a primary care physician was slightly but significantly higher in the intervention group than the control group; this was consistent with the design of the intervention. In contrast, the incidence rate of consultancies to specialists at the hospital was significantly lower in the intervention group than in the control group. This outcome was also consistent with the care model, which implemented measures to manage persons in primary care.
The implementation enabled the CISAUC and local teams to systematize the intervention strategies, the new roles, activities, and services. During this period, barriers and difficulties were mainly from the operational and organizational structure of the PHC, where organized registry, agendas, and other core aspects d based on a single diagnosis approach. Also, resistance from some, not all, the health care team became from the fear of changing to new tasks and new challenges, as expected on a complex change like this. On the other hand, the main facilitator that we could experience during the implementation was the relationship between the MCPM and the Family and Community Health Model (21–23). As both care strategies have similar principles, but the last one had gaps in its implementation, health teams felt that this innovation was in the right place and at the right time.
During this period, the process was followed and supported by the expert team of the Cento de Innovación en Salud ANCORA UC. This team worked weekly locally with each care team at the PHC and hospitals. The experience of providing external support made it possible to follow the intervention strategies as they were planned. Minimal changes and process times were adjusted to each local team to ensure the success of the intervention. Finally, the CISAUC team systematized several interventions for scale-up, such as self-management workshops, description of the new roles, description of the implementation steps, and also the minimal conditions for national scale-up (Tellez et al., 2020).
Health care teams incorporated new roles into the general practice in all intervened PHC and hospitals. They were able to perform the activities of each role, though it took about six-eight months to achieve their full performance in the new role. During this period, they were supported by the CISAUC team to solve problems and propose solutions that could improve their skills. Also, operational adjustments such as agendas and clinical working space were provided. The clinical pharmaceutical was the role that had the most barriers during the implementation. For example, the electronic health software did not incorporate agendas and citation processes; patients felt strange to have a consultant with this professional. Finally, there was no registry protocol available to record the clinical attention. In contrast, the case manager role was the easiest to implement. Probably, the incorporation of a full-time nurse to perform the activities facilitated the implementation process.
Achieving the best performance of the health staff meant that additional training was provided, including courses dictated by different faculties of the Universidad Católica. The main topics of the courses were self-management and case management for Nurses, medication review to the Clinical Pharmacists, multimorbidity approach of high-risk patients for general practitioners, and Patient-centered care approach for all the PHC clinical staff. The mentioned courses make today an academic program which the local Ministry of Health is scaling up (Ministerio de Salud: Subsecretaria de Redes Asistenciales, 2020).
The model began incorporating telemedicine into PHC, which was an innovation at this level. Phone consultants and self-management support were provided to patients avoiding face-to-face consultants. Although operational adjustments were provided for citations and registries, health care teams were motivated to facilitate the integration process. Moreover, the benefit for patients was shown in savings of transportation time, out-of-pocket spending for traveling gaining more proximity with their care teams.
From the patient's perspective, the implementation of the MCPM allowed them to have a designed clinical care team, improve their continuity and confidence with the clinical staff. Their families were more involved in the clinical attention as this model improved self-care strategies in families with NCD members.
DISCUSSION
The study reveals that implementing a patient-centered care model for multimorbidity can improve health outcomes and health system performance indicators. Therefore, this re-organization of the current resources in the health system decreased the number of hospitalizations, length of stays, and the number of consultancies in an emergency room.
Moreover, it reduces the probability of death. Probably the core elements of the model, when they are implemented all together, results in a more profound impact on health as described in the methods section, case management, continuity of care, self-management and risk stratification have positive health outcomes by their own.
The multimorbidity approach is an emerging topic that despite single interventions documented in the literature, there´s still a gap in the implementation processes and recommendations for reproduction in other jurisdictions. The description provided in this study about the core elements, the intervention strategies, and the implementation process could be taken from other countries of the region that need to start the transition to a multimorbidity approach. Although the intervention strategies have differences from other experiences described in the United States and Europe (Palmer et al., 2018; Poitras et al., 2018), it is believe that this experience could facilitate the approach in the health care systems for Latin American countries.
The main strength of this study is the organization and structure of the interventions that the MCPM proposes a multimorbidity approach. The intervention took place in the public health system, with a vulnerable population from a limited territory. The Ministry of Health, based on this pilot and other national experiences, is scaling up the change in the care strategy for people with non-communicable diseases at the level of the entire public health system. This experience could be used as a reference for other countries, particularly in Latin America, introducing the corresponding local adjustments. Still, the intervention strategies converge adequately with the bases of primary care and the health network, making it highly transferable to other jurisdictions.
A relevant feature of this assessment is the source of the data. The authors used routine information records of a public health service, which usually faces the challenge of incomplete data or inconsistencies of the registry. During the follow-up, we had the opportunity to analyse the data twice before, and the results were highly consistent with the final estimates presented in this report. Based on these repeated analyses, we can conclude that the data was consistent with no significant quality problems in the registry. Thus, we were able to undertake an evaluation of the model in a real-world setting, providing reliable estimates of the effectiveness of the strategies.
One limitation of the study was that ACG risk stratification was estimated with data collected at least another, they argue that their estimates capture well the one year before the stratification was performed because most variables are stable from one year to risk at the time of enrolment. Nonetheless, to mitigate any bias due to risk factors appearing between the data collection and enrolment, the second step of clinical classification was done, as explained in the methodology. Although the PHCs were chosen based on population and territorial similarity only, some differences were found regarding the population distribution. Even though they did not perform randomization, it is expected that some unbalance can occur due to context variability in real-world studies. However, although the differences are statistically significant, their magnitude is relatively smaller.
Another limitation, specifically related to the analysis, is the existence of endogeneity due to potential residual confounding. We argue that the set of control variables used in this analysis capture most residual confounding, limiting any relevant endogeneity in our statistical models. Regarding the outcomes examined, the authors are aware that they are a limited number of variables and may omit critical other consequences such as patient´s reported outcomes. Unfortunately, our analysis was limited to the routine records available in the information of SSMSO. Indeed, they recommended collecting additional variables, incorporating psychosocial determinants in clinical records that would enhance the impact evaluation in the future.
Even though the authors have provided evidence of the impact of the MPCM in the Chilean setting, its effectiveness, beyond the context where it was implemented, requires further research. One first element that needs to be considered is the comparator. Regarding the standard care model and organization, if other jurisdictions are similar to the Chilean health system, then it will determine any judgment of external validity of the impact. Second, it is highly likely that the impact depends on the set of current activities in the health systems. Third, the impact reported here is most likely to depend mainly on the changes implemented in the system, and this magnitude of change depends on the baseline performance of each intervention activity.
CONCLUSION
Overall, it was concluded that implementing the MPCM in the health facility can be a recommendation for the country to start the transition to a multimorbidity approach with a solid focus on patient-centered care. This process showed that better health outcomes could be reached with the change proposed by the model, especially on improvements in the health system performance, such as the number of hospitalizations, length of stay, and the number of consultancies in hospitality emergency, as well as decreased mortality in the, intervened population.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors would like to thank the Family Health Center (CESFAM) La Florida, La Florida; CESFAM Villa O'Higgins, La Florida; CESFAM Santiago Nueva Extremadura, La Pintana; CESFAM El Roble, La Pintana; ANCORA UC Mother Teresa Calcutta; ANCORA UC San Alberto Hurtado; ANCORA UC Juan Pablo II. La Florida Hospital, Dr. Sotero del Rio Hospital and Padre Hurtado Hospital and also the Department of Public Health, School of Nursing, Pontificia Universidad Católica de Chile and South East Metropolitan Health Service and National Health Fund.
REFERENCES
|
ACG System Excerpt from Technical Reference Guide (2009). December, 0-41. |
|
Barros J, Zamorano P, Varela T, Irazoqui E, Téllez Á (2019). Cambios en el modelo de atención de personas con multimorbilidad crónica: una revisión narrativa. ARS MEDICA Revista de Ciencias Médicas 44(4):35-40. |
|
Consejería de Salud de la Comunidad de Madrid. (2013). Estrategia de Atención a Pacientes con Enfermedades Crónicas. |
|
de Almeida PF, de Oliveira SC, Giovanella L (2018). Network integration and care coordination: The case of Chile's health system. Ciencia e Saude Coletiva 23(7):2213-2228. |
|
de Souza ASS, Braga JU (2020). Trends in the use of health services and their relationship with multimorbidity in Brazil, 1998-2013. BMC Health Services Research 20(1):1-12. |
|
Diane ZD, Loewenstein DA, Christ SL, Feaster DJ, Lam BL, McCollister KE, Curiel-Cid RE, Lee DJ (2021). Multimorbidity patterns and their relationship to mortality in the US older adult population. Plos ONE 16(1):e0245053. |
|
Dominguez-Cancino KA, Palmieri PA, Martinez-Gutierrez MS (2020). National Health Policy Reform for Primary Care in Chile: A Qualitative Analysis of the Health Program Documents. Journal of primary care & community health 11:2150132720924884. |
|
Gonçalves-Bradley DC, Lannin NA, Clemson LM, Cameron ID, Shepperd S (2016). Discharge planning from hospital (Review) Summary of findings for the main comparison. Cochrane Database Systematic Reviews 1:74. |
|
Hajat C, Stein E (2018). The global burden of multiple chronic conditions: A narrative review. Preventive Medicine Reports 12(10):284-293. |
|
Heins M, Korevaar J, Schellevis F, Rijken M. (2020). Identifying multimorbid patients with high care needs - A study based on electronic medical record data. European Journal of General Practice 26(1):189-195. |
|
Kanesarajah J, Waller M, Whitty JA, Mishra GD (2018). Multimorbidity and quality of life at mid-life: A systematic review of general population studies. Maturitas 109:53-62. |
|
Kuluski K, Peckham A, Williams AP, Upshur REG (2016). What Gets in the Way of Person-Centred Care for People with Multimorbidity? Lessons from Ontario, Canada. Healthcare Quarterly (Toronto, Ont.) 19(2):17-23. |
|
Leijten FRM, Struckmann V, van Ginneken E, Czypionka T, Kraus M, Reiss M, Tsiachristas A, Boland M, de Bont A, Bal R, Busse R, Mölken MRV (2018). The SELFIE framework for integrated care for multi-morbidity: Development and description. Health Policy 122(1):12-22. |
|
Mair FS, Foster HM, Nicholl BI (2020). Multimorbidity and the COVID-19 pandemic - An urgent call to action. Journal of Comorbidity 10:2235042X2096167. |
|
Margozzini P, Passi Á. (2018). Encuesta Nacional de Salud, ENS 2016-2017: un aporte a la planificación sanitaria y políticas públicas en Chile. ARS MEDICA Revista de Ciencias Médicas 43(1):30. |
|
McCarthy D, Mueller K, Wrenn J (2009). Case Study Kaiser Permanente: Bridging the Quality Divide with Integrated Practice, Group Accountability, and Health Information Technology P 17 (June). |
|
Menotti A, Puddu PE, Tolonen H. (2021). Age at death in elderly cohorts of four European countries of the Seven Countries Study: the role of comorbidities. Aging Clinical and Experimental Research 33(3):521-528. |
|
Mercado SR, Cassinelli MFV, Grez AI (2008). Motivational interviews: What are their effectiveness in prevalent primary care problems? Atencion Primaria 40(5):257-261. |
|
Ministerio de Salud Argentina (2013). Abordaje integral de personas con enfermedades cronicas no transmisibles - Buenosaires-Argentina-Redes 137 p. |
|
Ministerio de Salud de Chile (2013). Automanejo De Enfermedades No Transmisibles. pp.1-48. |
|
Ministerio de Salud (2009). Manual del cuidado de personas mayores dependientes y con pérdida de autonomía. 194 p |
|
Ministerio de Salud: Subsecretaria de Redes Asistenciales. (2020). Estrategia de cuidado integral centrado en las personas para la promoción, prevención y manejo de la cronicidad en contexto de multimorbilidad. |
|
Ministerio de Salud; Gobierno de Chile. (2005). Guía Clínica Insuficiencia Renal Cronica Terminal. Santiago: Minsal 37 p. |
|
Ministerio de Salud; Gobierno de Chile. (2011). Guía Clínica Alivio del Dolor por Cáncer Avanzado y Cuidados Paliativos. Salus Revista de La Facultad de Ciencias de La Salud. Universidad de Carabobo 19(2):5-10. |
|
Ministerio de Salud; Gobierno de Chile. (2012). Orientaciones Para La Implementacion Del Modelo De Atencion Integral De Salud Familiar Y Comunitaria pp. 1-143. |
|
Ministerio de Salud; Gobierno de Chile (2015). Guia Perinatal 2015. In Guia perinatal 2015. |
|
Ministerio de Salud; Gobierno de Chile. (2017). Orientación Técnica Programa de Salud Cardiovascular. |
|
Ministerio de Salud; Gobierno de Chile (n.d.). MSPAS Modelo de atención integral en salud pp. 1-62. |
|
MINSAL Chile (n.d.). Plan Nacional De Salud Mental 2017-2025. |
|
Montero, Alvaro Téllez J, Herrera C (n.d.). Temas de la agenda Pública Reforma sanitaria chilena y la atención primaria de salud. Algunos aspectos críticos. |
|
Shilpa R, Natasha C, Nick G (2011). Case management. What it is and how it can best be implemented. King's Fund pp. 1-32. |
|
Navickas R, Petric VK, Feigl AB, Seychell M (2016). Multimorbidity: What Do We Know? What Should We Do? Journal of Comorbidity 6(1):4-11. |
|
Nguyen H, Manolova G, Daskalopoulou C, Vitoratou S, Prince M, Prina AM (2019). Prevalence of multimorbidity in community settings: A systematic review and meta-analysis of observational studies. Journal of Comorbidity 9:2235042X1987093. |
|
Ahn S, Basu R, Smith ML, Jiang L, Lorig K, Whitelaw N, Ory MG (2013). The impact of chronic disease self-management programs: healthcare savings through a community-based intervention. BMC Public Health 13(1):1-6. |
|
OPS/OMS (2019). control prevención no transmisibles en las Americas enfermedades. |
|
Palmer K, Marengoni A, João M, Jureviciene E, Laatikainen T, Mammarella F, Muth C, Navickas R, Prados-torres A, Rijken M, Rothe U, Souchet L, Valderas J (2018). Multimorbidity care model?: Recommendations from the consensus meeting of the Joint Action on Chronic Diseases and Promoting Healthy Ageing across the Life Cycle (JA-CHRODIS) 122(1):4-11. |
|
Pearson-Stuttard J, Ezzati M, Gregg EW (2019). Multimorbidity-a defining challenge for health systems. The Lancet Public Health 4(12):e599-e600. |
|
Poitras M, Maltais M, Bestard-denommé L, Stewart M, Fortin M (2018). What are the effective elements in patient-centered and multimorbidity care?? A scoping review. BMC Health Services Research 18(1):1-9. |
|
Santelices CE, Muñiz VP, Arriagada BL, Delgado SM, Rojas FJ. (2014). Adjusted Clinical Groups as a risk assessment model for healthcare resource allocation. Revista Medica de Chile 142(2):153-15360. |
|
Smith SM, Wallace E, O'Dowd T, Fortin M. (2021). Interventions for improving outcomes in patients with multimorbidity in primary care and community settings. In Cochrane Database of Systematic Reviews (Vol. 2021, Issue 1). John Wiley and Sons Ltd. |
|
Subsecretaria de salud publica, división y control de prevención de enfermedades, D. M. I. D. C. Y. O. T. (2018). Plan Nacional de Cáncer. Plan Nacional de Cáncer 2018-2028, 185. |
|
Tellez A, Irazoqui E, Zamorano P, Varela T, Barros J, Muñoz P, Rain C, Campos SCP (2020). Modelo de Atención Centrado en la persona con Morbilidad Crónica MACEP. Redireccionando los servicios de salud según riesgo. |
|
Tortajada S, Giménez-Campos MS, Villar-López J, Faubel-Cava R, Donat-Castelló L, Valdivieso-Martínez B, Soriano-Melchor E, Bahamontes-Mulió, A, García-Gómez JM (2017). Case management for patients with complex multimorbidity: Development and validation of a coordinated intervention between primary and hospital care. International Journal of Integrated Care 17(2):1-8. |
|
William RM, Rollnick S (n.d.). La entrevista motivacional 3a edición: Ayudar a las personas a cambiar. |
|
Wold Health Organization (2020). The impact of the COVID-19 pandemic on noncommunicable disease resources and services: Results of a rapid assessment. In World Health Organization. |
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


