Full Length Research Paper

ABSTRACT
The patterns of prescription drug use in Suriname in the year 2017 have been determined with the purpose of obtaining indications about the distribution of disease in the country. The claims database of the State Health Foundation (Staatsziekenfonds, SZF) of Suriname was used for calculations of prescription rates of the fifty most prescribed drugs overall and after stratification according to gender, age, and residence of the insured persons. Information in the database had been de-identified, and the prescribed medicines had been coded according to the Anatomic Therapeutic Chemical Classification System. Statistically significant differences among the prescription rates were assessed with the two-sample test of proportions using normal theory method and x2 Goodness of Fit tests (p < 0.05). Additionally, the Bonferroni adjustment was used to adjust for type 1 error inflation resulting from multiple comparisons. Overall, drugs for the cardiovascular, respiratory, and musculo-skeletal systems had the highest prescription rates (p < 0.001). Furthermore, rates were generally higher in females than in males, in the older age groups than in younger individuals, and in the coastal regions compared to the country's interior (p < 0.001). These findings are largely in line with data found in the literature and support the use of this pharmacoepidemiological approach to assess the distribution of disease in Suriname.
Key words: Suriname, distribution of disease, pharmacoepidemiology, claims database, prescription drugs.
INTRODUCTION
Information about the distribution of disease in society is crucial for planning health care policy (WHO et al., 2018). This information is often obtained from population-based disease registries, which collect data from a wide variety of sources to ensure that all cases in the community are covered (Gliklich et al., 2014). Population-based disease registries can be used as tools for tracking the clinical care and outcomes of a defined patient population in a particular geographic area (Rosenberg et al., 2016), to support the care and management of groups of patients with chronic diseases (Gliklich et al., 2014), in postmarketing surveillance of pharmaceuticals, evaluating, for instance, side effects in subpopulations, such as pregnant women (Willis et al., 2012).
The Republic of Suriname is situated in the north-eastern part of South America and borders French Guiana to the east, the Atlantic Ocean to the north, Brazil to the south, and Guyana to the west. The country’s land area of roughly 165,000 km2 can be distinguished into a relatively narrow northern part made up of urban-coastal and rural-coastal regions and a southern rural-interior region that covers about three-quarters of its surface area. The coastal regions are characterized by, among others, a 'western' lifestyle, and modern health care facilities, the interior region maintains a more traditional way of living and lacks comprehensive public health services (General Bureau of Statistics, 2020a). Roughly 80% of Suriname's ethnically highly diverse population (International Organization of Migration, 2015) lives in the coastal zone while the remaining 20% - mainly consisting of Indigenous peoples and Tribal peoples - populates the savannas and hinterlands in the rural interior (General Bureau of Statistics, 2019).
Suriname's gross domestic product (GDP) in 2020 was about USD 3 billion and the average per capita income in that year was USD 4,920 (International Monetary Fund, 2020), positioning the country on the World Bank’s list of upper-middle-income economies (World Bank, 2021). Furthermore, Suriname has made considerable progress in health care, sanitation, nutrition, and drinking water quality; the eradication of several infectious diseases; as well as improvements in average living and working conditions, income, and education (World Bank, 2021). The result was a decline of the death rate from 24 per 1,000 in 1923 to 6 per 1,000 in 2011 and the attainment of an average life expectancy of 70 years in 2011 (General Bureau of Statistics, 2020b).
However, as reported for many low- and middle-income countries (Chan et al., 2012), these developments occurred at the cost of a substantial increase in the prevalence and mortality of non-communicable diseases in the country, particularly hypertension and diabetes mellitus (Baldew et al., 2015; Krishnadath et al., 2016a, b). As well, certain infectious diseases such as cutaneous leishmaniasis seem to become more prevalent in Suriname (Mans et al., 2017), and although malaria has largely been eradicated (Van Eer et al., 2018), there is a constant threat of outbreaks from import cases from neighboring countries (Hiwat et al., 2018). Unfortunately, so far, there are no disease registries in Suriname, and information about the prevalence and mortality of the most common disorders in the country is limited to a handful of isolated studies (Mans et al., 2013).
A potentially feasible alternative to the use of disease registries to obtain information of disease in a society may involve the use of existing databases to collect information such as the numbers and types of prescriptions dispensed in that society in a certain period. In the current analysis, this possibility has been investigated in a pharmacoepidemiological analysis on the patterns of prescription drugs used in Suriname’s general population as a determinant of the distribution of disease in the country. For this purpose, the claims database of the State Health Foundation (Staatsziekenfonds, SZF) has been used. SZF is state-owned and is the largest insurance company in Suriname, covering more than half of the total population (Uitvoeringsorgaan Basiszorg Suriname, 2017). SZF ensures the quality of the information in the database by manually validating the prescribed and claimed medicines using the original paper prescription. With this background, the patterns of prescription drug use in Suriname in the year 2017 have been determined to obtain indications about the distribution of disease in the country. This information has been stratified according to gender, age, and geographical location of the insured persons. This provided indications about the types of drugs used by the main subgroups in the country and the distribution of disease in these subgroups.
METHODOLOGY
Study population
A descriptive pharmacoepidemiological analysis about the patterns of prescription medication use in the general Surinamese population in the period between 1st January and 31st December 2017 was conducted. Ethical approval has been granted by the Institutional Review Board of the Ministry of Health of Suriname (VG 023-14) and the Institutional Review Board of Tulane University, New Orleans (L.A.), USA.
Sources of data
Information about the numbers and types of prescribed medicines was obtained from the SZF claims database. The database also included patients’ gender, date of birth, as well as address and region of residence. For the current analysis, the data have been de-identified by SZF’s Management Information System Department and included information about the fifty most frequently claimed prescriptions in Suriname in the year 2017.
Data processing
Firstly, numbers of overall medicines prescribed in the year 2017 and numbers of insured persons claiming these prescriptions have been determined, overall as well as after stratification according to gender; age group (0-14 years, 15-29 years, 30-44 years, 45-59 years, and 60 years and older); as well as the region of residence (urban-coastal region, rural-coastal region,and rural-interior region). From these data, prescription rates have been derived, that is, average numbers of prescriptions per individual in each subgroup, which were determined by dividing the number of prescriptions in a subgroup by the number of individuals constituting that subgroup.
Secondly, the prescribed medicines have been categorized according to the Anatomical Therapeutic Chemical (ATC) Classification System of the World Health Organization (WHO) (WHO Collaborating Centre for Drug Statistics Methodology, 2018). In this system, the active ingredients of drugs are classified according to the system or organ on which they act, as well as their therapeutic, pharmacological, and chemical properties. Then, numbers of the most prescribed medicine categories in the year 2017 and numbers of insured persons claiming these prescriptions have been determined. Prescription rates of each ATC category have been determined by dividing the number of prescriptions in an ATC category by the number of individuals claiming a medicine in that category.
Thirdly, prescription rates in each ATC category have been stratified according to gender; age groups 0-14, 15-29, 30-44, 45-59, and 60+ years; and having permanent residency in Suriname's urban-coastal region, rural-coastal region, or rural-interior region. This was calculated by dividing the number of prescriptions in an ATC category by the number of individuals in each of the strata claiming a medicine in that ATC category.
Statistics
The data presented are average prescription rates and have been compared for statistically significant differences using x2 Goodness of Fit tests with α = 0.05. Overall prescription rates were compared with the two-sample test of proportions using the normal theory method. To adjust for type 1 error inflation resulting from multiple comparisons, the Bonferroni adjustment was applied. All analyses have been performed at the 5% significance level using SPSS Version 20 and Excel from Microsoft Office 365.
RESULTS
Overall prescription rates
A total of 2,273,089 prescriptions were dispensed to 229,463 insured patients in 2017. According to results presented in Table 1, this corresponded to an overall prescription rate of 9.9. The average prescription rates for males and females were 8.7 and 10.7, respectively, indicating that women received on average about 20% more prescription medications than men (p < 0.001).

Prescription rates were on average about 5 in individuals of 0-14 years and 15-29 years of age but increased roughly 2-fold, 3-fold, and 4-fold in individuals of 30-44 years, 45-59 years, and 60+ years, respectively. These observations clearly indicate that the need for prescription medication substantially increased with older age (p < 0.001). The average prescription rate for Suriname’s urban-coastal area was 9.8, that for the rural-coastal area was 11.0, and that for the country’s rural interior 7.4. Apparently, individuals from Suriname’s urban-coastal and rural-coastal areas had received a comparable number of prescriptions per person (roughly 10 per person), but those from the country's rural interior about 25% less (p < 0.001).
Rates of most prescribed categories of medicines
Table 2 gives the prescription rates of the most prescribed categories of medicines in 2017. The drugs with the highest prescription rates were those for conditions of the cardiovascular system (C), musculo-skeletal system (M), and respiratory system (R). These compounds were on average prescribed at rates of 26.5, 21.5, and 34.1, respectively, and mainly included antihypertensive drugs such as diuretics, β-blockers, calcium channel blockers, agents acting on the renin-angiotensin-aldosterone system (RAAS), and lipid-modifying agents; anti-inflammatory and antirheumatic products; as well as cough and cold preparations and other respiratory products, respectively.
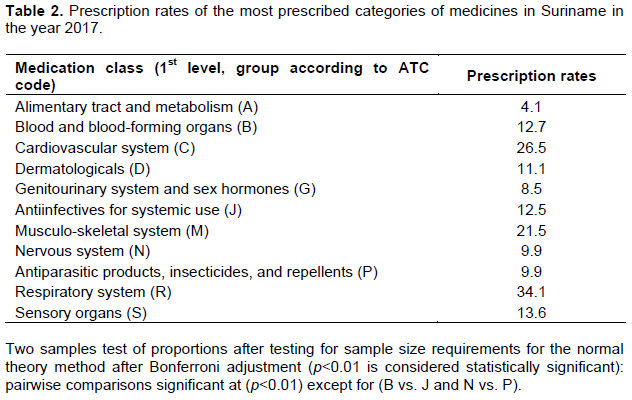
On the other hand, the prescription rates of drugs against conditions of the alimentary tract and metabolism (A) were only 4.1. These compounds included, among others, antidiabetic preparations, drugs for functional gastrointestinal disorders, and vitamins. Drugs for the blood and blood-forming organs (B), dermatologicals (D), drugs for the genitourinary system and sex hormones (G), anti-infectives for systemic use (J), drugs for the nervous system (N), antiparasitic products, insecticides, and repellents (P), and drugs for the sensory organs (S) were prescribed at rates between 8.5 and 13.6. These prescriptions mainly were for anti-anemic preparations, antifungals for dermatological use, antibacterials for systemic use, analgesics, and anthelmintics.
Rates of most prescribed medicine categories according to gender
As shown in Table 3, prescription rates of all medicine categories were higher in females than in males. This difference was most apparent for drugs for the genitourinary system and sex hormones (G), the prescription rate of which was 2.6 times higher in females than in males (8.6 vs. 3.3; p < 0.01). This difference was probably mainly due to the prescription of oral contraceptives for females. The prescription rates of dermatologicals (D), drugs for the sensory organs (S), drugs for the nervous system (N), drugs for the musculo-skeletal system (M), and anti-infectives for systemic use (J) were also (40 to 90%) higher in women than in men (p < 0.01). The prescriptions in these categories were mainly for antifungals for dermatological use; ophthalmologicals such as anti-infectives, antiglaucoma preparations, and miotics; analgesics and psycholeptics; topical products for joint and muscle pain, as well as antimicrobial compounds. The prescription rates of drugs for the respiratory system (R), the alimentary tract and metabolism (A), and the cardiovascular system (C) differed statistically significantly between males and females (p < 0.01). The most common prescriptions in these categories were for cough and cold preparations and drugs for obstructive airway diseases; antidiabetics, drugs for acid-related disorders, and vitamins; as well as lipid-modifying drugs, agents acting on RAAS, diuretics, β-blockers, and calcium channel-blocking agents.
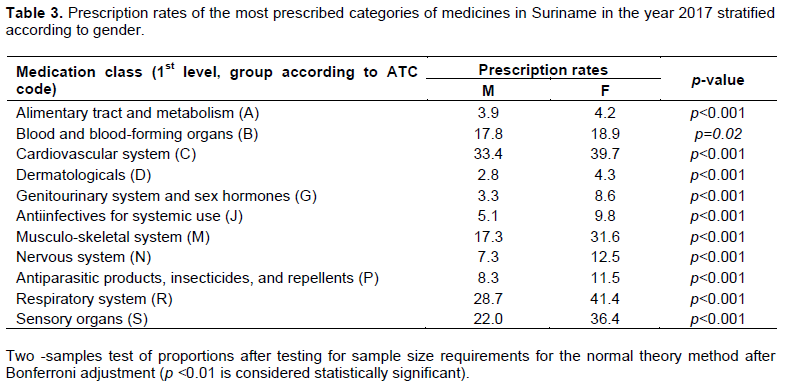
The highest prescription rates in both males and females were for drugs for the respiratory system (R), followed by drugs for the cardiovascular system (C), the sensory organs (S), the musculo-skeletal system (M), and the blood and blood-forming organs (B). The prescription rates of these drugs ranged in males from 17.3 to 33.4 and in females from 18.9 to 41.4. Drugs for the alimentary tract and metabolism (A), dermatologicals (D), drugs for the genitourinary system and sex hormones (G), anti-infectives for systemic use (J), drugs for the nervous system (N), and antiparasitic products, insecticides and repellents (P) were prescribed at rates between 2.8 and 8.3 in males, and between 4.3 and 11.5 in females.
Together, these observations indicate that women received, in general, more prescription medications than men. This was not only due to prescriptions for birth control pills for women but also to the higher prescription rates for women of many non-gender-related medications such as topical antifungals, various ophthalmologicals, pain medications, and sleeping pills, ointments for joint and muscle pain, as well as antimicrobials for systemic use.
Rates of most prescribed medicine categories according to age group
According to Table 4, the prescription rates of most ATC categories increased with older age, reaching the highest values in individuals aged 60 years and older. Notably, prescription rates of drugs for the nervous system (N), musculo-skeletal system (M), cardiovascular system (C), dermatologicals (D), and drugs for the sensory organs (S) were 12.7 to 32.5 times higher in individuals of 60+ years when compared to individuals of 0-14 years. This suggests that these drugs - which included, among others, analgesics, anti-inflammatory and antirheumatic products, antihypertensives, and antifungals for dermatological use - were much more frequently used in the oldest age groups when compared to the younger groups.
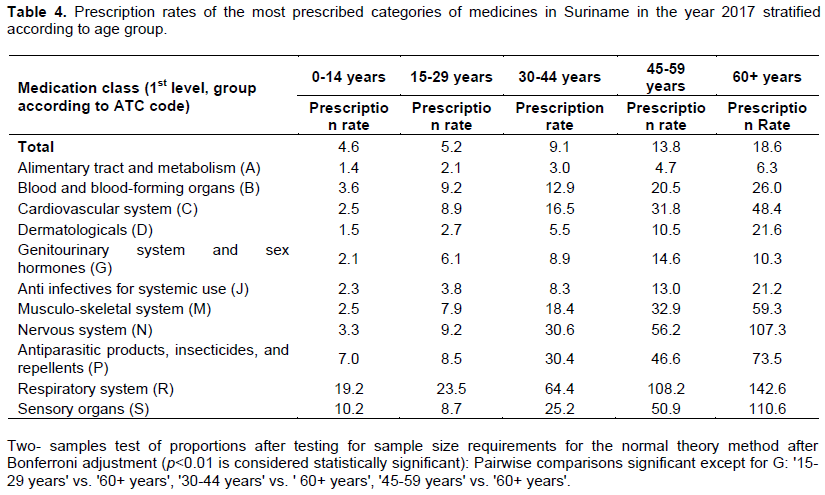
The age differences in prescription rates of drugs for the alimentary tract and metabolism (A), blood and blood-forming organs (B), anti-infectives for systemic use (J), and antiparasitic products, insecticides, and repellents (P) were less pronounced, being 4.5 to 10.8 times higher in the oldest age group when compared to the youngest. Nonetheless, the differences in prescription rates among all groups were still statistically significant (p < 0.01).
There were two exceptions. The prescription rates of drugs for the genitourinary system and sex hormones (G) increased until 45-59 years but decreased in people aged 60 years and older. This suggests that this category of drugs - which included oral contraceptives - were of less importance to individuals of 60+ years compared to those between 29 and 59 years of age. Furthermore, the rates of drugs for the sensory organs (S) in the group of 15-29 years were lower than those in the group of 0-14 years but increased from 30-44 years on to reach the highest values in individuals of 60 years and older. These drugs included, among others, ophthalmologicals (anti-infectives, antiglaucoma preparations, and miotics) and were apparently used at higher rates by adolescents and young adults when compared to individuals from the other age groups.
The highest prescription rates in all age groups were for drugs for the respiratory system (R), suggesting thatailments of the nasal cavity, throat, and lower airways requiring medications against coughing and colds were among the most common health problems in all age groups. The following highest prescription rates children of 0-14 years were for drugs for the sensory organs (S) and mainly included ophthalmologicals. In adolescents and young adults of 15-29 years, the highest rates were for drugs for the blood and the blood-forming organs (B) and the cardiovascular system (C) and mainly consisted of anti-anemic preparations and antihypertensives. In individuals of 30 years and older, they were for drugs for the nervous system (N), antiparasitic products, insecticides and repellents (P), and drugs for the sensory organs (S) and mainly consisted of analgesics and psycholeptics, antihelmintics, and ophthalmologicals.
The lowest prescription rates across the age groups were for drugs for the alimentary tract and metabolism (A) and dermatologicals (D), constituting 1.4 and 1.5, respectively, in children aged 0-14 years, and 6.3 and 21.6, respectively in adults of 60+ years. These compounds mainly included drugs for constipation but also drugs for diabetes mellitus and vitamins as well as antifungals for dermatological use.
Rates of most prescribed medicine categories according to the region of residence
The prescription rates of all ATC categories were highest in the rural-coastal region, lowest in the rural-interior region, and had intermediate values in the urban-coastal region. These results are presented in Table 5 and the differences were statistically significant (p < 0.01). The highest rates in each region were for drugs for the cardiovascular system (C), the respiratory system (R), the musculo-skeletal system (M), the sensory organs (S), and the blood and blood-forming organs (B), and they varied from 14.4 to 25.8 in the rural-interior region to 22.1 to 35.6 in the rural-coastal region. These medicine classes mainly represented antihypertensives, cough and cold preparations, products for joint and muscular pain, ophthalmologicals, and anti-anemic preparations.
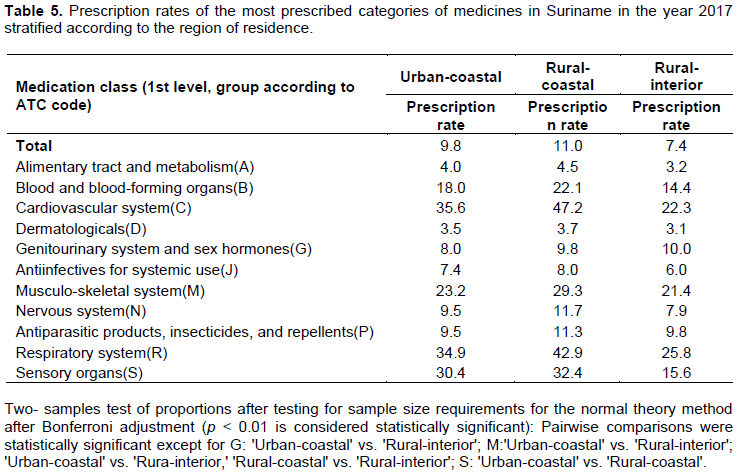
The remaining drug categories (drugs for the alimentary tract and metabolism (A), dermatologicals (D), anti-infectives for systemic use (J), drugs for the nervous system (N), those for the genitourinary system and sex hormones (G), as well as antiparasitic products, insecticides and repellents (P)) were prescribed at relatively low rates, that is, between 3.1 in the rural-interior region and 11.7 in the coastal regions. The most prescribed subclasses of the medicines in these categories were drugs for acid-related disorders, antidiabetics, and vitamins; topical antifungals; antibacterials for systemic use; analgesics and psycholeptics; contraceptives; and antihelmintics.
DISCUSSION
In order to obtain indications about the distribution of disease in Suriname, the patterns of use of the most prescribed drug categories in the country in the year 2017 have been determined using the claims database of the SZF. The data have been expressed as prescription rates (that is, the average number of prescriptions of a particular WHO ATC drug (sub)category per individual).The prescription rates have been calculated for the entire database as well as for males and females, different age groups, and groups of individuals living in one of the three geographical regions of Suriname. The overall prescription rate was 9.9. This was lower than the average prescription rates of the United States of America of 12.2 in 2013 (Health Policy Institute Georgetown University, n.d.; Statista Inc., 2014; IQVIA Institute, 2021)and that in the United Kingdom where an average prescription rate of 19.8 has been reported in 2015 (National Health Service United Kingdom, 2016). Rates were higher in females than in males, in general, increased with older age and were mostly higher in the urban-coastal and rural-coastal regions than in the rural-interior region. The highest prescription rates were for drugs for diseases of the respiratory system, cardiovascular system, and musculo-skeletal system, suggesting that these ailments were the most prevalent in Suriname in 2017. The prescription rates for these groups of medicines were also among the highest in females compared to males, in older individuals compared to younger persons, and in individuals from Suriname's urban-coastal and rural-coastal regions compared to the country's rural interior. These observations suggest substantial gender-associated, age-related, and geographic differences in the prescription patterns of medicines.
The higher prescription rate for Surinamese women when compared to men is in line with many previous findings, such as those from the Campania region in Italy (Orlando et al., 2020), the Catalan region in Spain (Santalucia et al., 2015), and various other parts of Europe (Eurostat, 2020)reporting the more frequent use of the health system by women when compared to men (Putignano et al., 2017). This has partly been attributed to the higher life expectancy of women when compared to men in many countries (Statistics Canada, 2015)including Suriname (General Bureau of Statistics, 2020b). The increase in prescription rates with older age agrees with the well-described increase in the burden of disease and use of medicines and health services with increasing age (Jaul and Barron, 2017; Atella et al., 2019). Furthermore, the higher overall prescription rate in the urban-coastal and rural-coastal regions compared to the rural-interior region was probably attributable to the considerable number of uninsured people in the hinterland who are taken care of by the Medical Mission (Medische, 2017). The Medical Mission is a government-subsidized non-governmental organization that operates a network of primary care clinics in the interior of Suriname and provides health care regardless of insurance status (Medische, 2017). In contrast, medical care in the entire coastal area is offered by general practitioners and the government-subsidized Regional Health Services whose patients are compulsory insured (Pan American Health Organisation, 2017).
Cardiovascular drugs such as diuretics, β-blockers, calcium channel blockers, agents acting on RAAS, and lipid-modifying agents were among the medicines with the highest prescription rates. This finding is in line with the relatively high prevalence of hypertension and metabolic syndrome in Suriname (Krishnadath et al., 2016b; Diemer et al., 2017). Although diabetes mellitus is also among the most prevalent non-communicable diseases and causes of death in Suriname (Bureau of Public Health, 2012), this is not reflected in the prescription rates for antidiabetic drugs, which were much lower than those for drugs for cardiovascular diseases. This might be due to underestimation of the prescription rate of antidiabetics since not all these compounds were among the fifty most frequently claimed prescriptions selected for the current analysis. The relatively high prescription rates for anti-inflammatory and antirheumatic products as well as cough and cold preparations and other respiratory products suggests that inflammations and rheumatic diseases, as well as respiratory tract infections, were also rather common in Suriname. These observations cannot readily be explained and must be investigated in future studies. However, respiratory infections are very common in Suriname's tropical and humid environment, particularly during the rainy seasons (Grunberg et al., 2021), and are among the most prevalent diseases throughout the world (Abbafati et al., 2020). The relatively high prescription rates for topical anti-inflammatory and antirheumatic drugs in the current analysis may be attributed to the fact that these medicines are reimbursed by SZF, while in other countries, they are considered over-the-counter drugs (Chini et al., 2011; Huber et al., 2013; Derry et al., 2015).
The higher prescription rates for females, when compared to males were, obviously, partially due to the use of oral contraceptives by females. Furthermore, when compared to males, females have been reported to more frequently use antifungals for topical application (Becker et al., 2020), eye medications including antiglaucoma and miotics (Vajaranant et al., 2010; Tehrani, 2015), analgesics and psycholeptics (Johnell and Fastbom, 2011; Bäckryd, 2018), and topical products for joint and muscular pain (Bäckryd, 2018). These data support the higher prescription rates of these medicines for women than men in the current analysis and can partially be attributed to the higher prevalence of glaucoma in women (Zetterberg, 2016)and the much higher prevalence of genital urethral infections such as candidiasis and cystitis in women (Lo et al., 2013; Skoog et al., 2014; He et al., 2018; Kaur et al., 2020).
The relatively high prescription rates of analgesics, anti-inflammatory and antirheumatic products, antihypertensives, antifungals for dermatological use, and antiglaucoma and miotic eye preparations in the older age groups when compared to the younger groups are in accordance with literature data mentioning an increasing prevalence of disease and use of medicines and healthcare with older age (Atella et al., 2019). This holds true for, among others, medications to treat musculoskeletal-related diseases and the associated back and neck pains such as osteoarthritis, eye-related diseases such as cataracts, chronic obstructive airway diseases, as well as non-communicable diseases such as hypertension, metabolic syndrome, and diabetes mellitus (World Health Organization, 2020, n.d.). Most of these conditions manifest and require chronic drug treatment from age 30 years on and increase in prevalence and severity with older age, accounting for the observed increase in prescription rates. The increasing rate for drugs for the genitourinary system and sex hormones until the age of 45-59 years and the decrease in people of 60 years and older may be explained by the increasing use of birth control pills by females until age 44 to 59, after which the use of these medications becomes less important (Skoog et al., 2014; Daniels and Abma, 2017). On the other hand, the relatively high rates in all age groups for cough and cold remedies suggest that ailments of the nasal cavity, throat, and lower airways were among the most common health problems in Suriname. As suggested above, this might be attributed to the climatic conditions in Suriname that facilitate respiratory infections (Grunberg et al., 2021). However, the current data do not support the previously reported preferential occurrence of these infections in children younger than ten years (Abbafati et al., 2020). The reasons for this discrepancy are not known and need to be investigated.
The relatively high prescription rates of antihypertensives, cough and cold preparations, compounds for joint and muscular pain, ophthalmologicals, and anti-anemic medications suggest that conditions associated with these medicines were in all regions of Suriname among the most prevalent causes of morbidity. This is mainly in line with the above-mentioned relatively high prescription rates of these drugs, overall, in both males and females and all age groups. The in general higher prescription rates of all drug (sub)categories in the urban-coastal and rural-coastal areas when compared to the interior, may be ascribed to the earlier mentioned under-representation of prescription claims from rural-interior people, many of whom are uninsured and taken care of by the Medical Mission (Medische, 2017). For antihypertensives, this difference may be attributed, in addition, to the much higher proportion of people of Asian descent in the coastal areas who are known to be more susceptible to hypertension and metabolic syndrome when compared to people from the interior (Krishnadath et al., 2016a, b; Diemer et al., 2017). Moreover, the regional differences in the prescription rates of ophthalmologicals may be due, at least partly, to the relatively high prevalence of glaucoma and other eye diseases in the interior when compared to the coastal areas of Suriname (Minderhoud et al., 2014).
Taken together, the results from the current analysis support the pharmacoepidemiological approach applied to estimate the distribution of disease in the Surinamese population. The relatively high prescription rates of cardiovascular drugs are in accordance with the high prevalence of cardiovascular disease in the country (Krishnadath et al., 2015). The high prescription rates of drugs for the respiratory system and the musculo-skeletal system suggest that the diseases associated with these medications are also highly prevalent in Suriname. This has not been reported before and should be further investigated. Thus, the pharmacoepidemiological approach of estimating disease distribution in Suriname by using prescription rates seems feasible.
However, it should be taken into account that the SZF database the current analysis has relied on covers only 60% of the total population of Suriname (Uitvoeringsorgaan Basiszorg Suriname, 2017), warranting caution when extrapolating the current results to the general population. This may hold particularly true for people living in the country's interior, an unknown proportion of whom is not insured at the SZF (Medische, 2017). Notably, the lack of supporting data from medical records, disease registries, and surveillance systems in Suriname to cross-check the current estimations and increase their reliability also warrants caution in using prescriptions as proxies to estimate the prevalence and distribution of disease in Suriname. Furthermore, as the analysis has focused on the fifty most prescribed medicines, specific categories of drugs (such as antidiabetics) and medicines dispensed by governmental public health agencies may have been left out of the analyses, leading to underestimating the associated diseases. Nevertheless, the pharmacoepidemiological approach followed in the current analysis seems feasible and realistic and may represent a cost-effective way to help design public health strategies to estimate and manage disease in Suriname.
CONCLUSIONS
The overall prescription rate of 9.9 in Suriname suggests a moderate prescribing policy in the country. Stratification according to gender, age, and geographic distribution of prescription rates indicates that disease was more common in females than in males, in older age groups than in younger individuals, and in the coastal regions when compared to the interior of the country. The relatively high prescription rates of drug for the respiratory, cardiovascular, and musculo-skeletal system in all three strata suggest that ailments associated with these medicines were the most prevalent in Suriname.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abbafati C, Machado DB, Cislaghi B, Salman OM, Karanikolos M, McKee M, Abbas KM, Brady OJ, Larson HJ, Trias-Llimós S, Cummins S, Langan SM, Sartorius B, Hafiz A, Jenabi E, Mohammad GMN, Borzouei S, Azarian G, Khazaei, S (2020). Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: a systematic analysis for the Global Burden of Disease Study 2019. The Lancet 396(10258):1204-1222. |
|
|
Atella V, Piano MA, Kopinska J, Belotti F, Lapi F, Cricelli C, Fontana L (2019).Trends in age-related disease burden and healthcare utilization. Aging cell 18(1):e12861. |
|
|
Bäckryd E (2018). Gender differences in dispensed analgesics in Sweden during 2006-2015- an observational, nationwide, whole-population study. International Journal of Women's Health 10:55-64. |
|
|
Baldew SSM, Krishnadath ISK, Smits CCF, Toelsie JR, Vanhees L, Cornelissen V (2015). Self-reported physical activity behavior of a multi-ethnic adult population within the urban and rural setting in Suriname. BMC Public Health 15(1):1-9. |
|
|
Becker P, Lecerf P, Claereboudt J, Devleesschauwer B, Packeu A, Hendrickx M (2020). Superficial mycoses in Belgium: Burden, costs and antifungal drugs consumption. Mycoses 63(5):500-508. |
|
|
Bureau of Public Health (2012). Doodsoorzaken in Suriname (causes of death) 2010-2011. Department Epidemiologie en Biostatistiek. |
|
|
Chan KY, Adeloye D, Grant L, Kol?i? I, Maruši? A (2012). Estimating the burden of non-communicable diseases in low- and middle-income countries. Journal of Global Health 2 :020101. |
|
|
Chini F, Pezzottim P, Orzella L, Borgia P, Guasticchi G (2011). Can we use the pharmacy data to estimate the prevalence of chronic conditions? a comparison of multiple data sources. BMC Public Health 11(1):1-8. |
|
|
Daniels K, Abma JC (2017). NCHS Data Brief, Number 388, October 2020. National Survey of Family Growth. |
|
|
Derry S, Moore RA, Gaskell H, Mcintyre M, Wiffen PJ (2015). Topical NSAIDs for acute musculoskeletal pain in adults. Cochrane Database of Systematic Reviews. |
|
|
Diemer FS, Baldew SSM, Haan YC, Aartman JQ, Karamat FA, Nahar-Van VLMW, Van MGA, Oehlers GP, Brewster LM (2017). Hypertension and Cardiovascular Risk Profile in a Middle-Income Setting: The HELISUR Study. American Journal of Hypertension 30(11):1133-1140. |
|
|
Eurostat (2020). Medicine use statistics - Statistics Explained. General Bureau of Statistics (2019). Demografische Statistieken 2015-2018. |
|
|
General Bureau of Statistics (2020a). 9th Environment Statistics Publication 2015-2019. |
|
|
General Bureau of Statistics (2020b). Statistisch Jaarboek 2018-2019 Suriname. |
|
|
Gliklich RE, Dreyer NA, Leavy MB (2014). Patient Registries. |
|
|
Grunberg M, Sno R, Adhin MR (2021). Epidemiology of respiratory viruses in patients with severe acute respiratory infections and influenza-like illness in Suriname. Influenza and Other Respiratory Viruses 15 :72-80. |
|
|
He K, Hu Y, Shi JC, Zhu YQ, Mao XM (2018). Prevalence, risk factors and microorganisms of urinary tract infections in patients with type 2 diabetes mellitus: a retrospective study in China. Therapeutics and Clinical Risk Management 14:403-408. |
|
|
Health Policy Institute Georgetown University (n.d.) Prescription Drugs | Health Policy Institute | Georgetown University. |
|
|
Hiwat H, Martínez-López B, Cairo H, Hardjopawiro L, Boerleider A, Duarte EC, Yadon ZE (2018). Malaria epidemiology in Suriname from 2000 to 2016: Trends, opportunities and challenges for elimination. Malaria Journal 17(1):1-13. |
|
|
Huber CA, Szucs TD, Rapold R, Reich O (2013). Identifying patients with chronic conditions using pharmacy data in Switzerland: An updated mapping approach to the classification of medications. BMC Public Health 13:1030. |
|
|
International Monetary Fund (2020). World Economic Outlook (October 2020) - GDP, Current Prices. |
|
|
International Organization of Migration (2015). Suriname Migration Profile A study on emigration from, and immigration into Suriname. |
|
|
IQVIA Institute (2021). The Use of Medicines in the U.S. Spending and using trends and outlook to 2025. |
|
|
Jaul E, Barron J (2017). Age-Related Diseases and Clinical and Public Health Implications for the 85 Years Old and Over Population. Frontiers in Public Health 5 :335. |
|
|
Johnell K, Fastbom J (2011). Gender and use of hypnotics or sedatives in old age: A nationwide register-based study. International Journal of Clinical Pharmacy 33 :788-793. |
|
|
Kaur R, Kaur R (2020). Symptoms, risk factors, diagnosis and treatment of urinary tract infections. Postgraduate Medical Journal. |
|
|
Krishnadath I, Smits C, Jaddoe V, Hofman A, Toelsie JR (2015). A National Surveillance Survey on Noncommunicable Disease Risk Factors: Suriname Health Study Protocol. JMIR Research Protocols 4, e75. |
|
|
Krishnadath I, Jaddoe VWV, Nahar-van Venrooij LM, Toelsie JR (2016a). Ethnic differences in prevalence and risk factors for hypertension in the Suriname Health Study: a cross sectional population study. Population Health Metrics 14:33. |
|
|
Krishnadath I, Toelsie J, Hofman A, Jaddoe VWV (2016b). Ethnic disparities in the prevalence of metabolic syndrome and its risk factors in the Suriname Health Study: a cross-sectional population study. BMJ Open 6:e013183. |
|
|
Lo DS, Shieh HH, Ragazzi SLB, Koch VHK, Martinez MB, Gilio AE (2013). Community-acquired urinary tract infection: age and gender-dependent etiology. Jornal brasileiro de nefrologia?: 'orgão oficial de Sociedades Brasileira e Latino-Americana de Nefrologia 35:93-98. |
|
|
Mans D, Pelswijk K, Boschveld I, Culbard G, Tewarie A, Adhin S, Ramautar, B, Sewgobin, S, Jagesar, A, Mohan, R, Bansie, R, Wangsawirana A, Vrede MA (2013). Occurrence of cancers of the gastrointestinal tract in the Republic of Suriname. Results from a descriptive study between the years 1980 and 2008. Translational Biomedicine 4. |
|
|
Mans D, Kent A, Hu R, Schallig H (2017). Epidemiological, Biological and Clinical Aspects of Leishmaniasis with Special Emphasis on Busi Yasi in Suriname. Journal of Clinical and Experimental Dermatology Research 08. |
|
|
Medische Z (2017). Medische Zending Primary Healthcare Suriname. |
|
|
Minderhoud J, Mans DRA, Pawiroredjo JC, Pameijer JH, Saeed P, Moll AC (2014). Causes of blindness and visual impairment in the interior Maroon population in the Republic of Suriname. Acta Ophthalmologica 92:162-164. |
|
|
National Health Service United Kingdom (2016). Prescriptions Dispensed in the Community - Statistics for England, 2005-2015 - NHS Digital. |
|
|
Orlando V, Mucherino S, Guarino I, Guerriero F, Trama U, Menditto E (2020). Gender differences in medication use: A drug utilization study based on real world data. International Journal of Environmental Research and Public Health 17. |
|
|
Pan American Health Organisation (2017). Country Report Suriname. Health in the Americas+, 2017 Edition. Summary: Regional Outlook and Country Profiles. |
|
|
Putignano D, Bruzzese D, Orlando V, Fiorentino D, Tettamanti A, Menditto E (2017). Differences in drug use between men and women: an Italian cross sectional study. BMC Women's Health 17. |
|
|
Rosenberg BL, Kellar JA, Labno A, Matheson DHM, Ringel M, VonAchen P, Lesser RI, Li Y, Dimick JB, Gawande AA, Larsson SH, Moses,H (2016). Quantifying Geographic Variation in Health Care Outcomes in the United States before and after Risk-Adjustment. (Taniyama, Y., Ed.) PLOS ONE 11:e0166762. |
|
|
Santalucia P, Franchi C, Djade CD, Tettamanti M, Pasina L, Corrao S, Salerno F, Marengoni A, Marcucci M, Nobili A, Mannucci PM (2015). Gender difference in drug use in hospitalized elderly patients. European Journal of Internal Medicine., 26, 483-490. |
|
|
Skoog J, Midlöv P, Borgquist L, Sundquist J, Halling A (2014). Can gender difference in prescription drug use be explained by gender-related morbidity?: a study on a Swedish population during 2006. BMC Public Health 14:1-7. |
|
|
Statista Inc. (2014). U.S. average number of prescriptions per capita. |
|
|
Statistics Canada (2015). Prescription medication use by Canadians aged 6 to 79. |
|
|
Tehrani S (2015). Gender difference in the pathophysiology and treatment of glaucoma. Current Eye Research. |
|
|
Uitvoeringsorgaan BS (2017). Statistieken Basiszorgverzekering. |
|
|
Vajaranant TS, Nayak S, Wilensky JT, Joslin CE (2010). Gender and glaucoma: What we know and what we need to know. Current Opinion in Ophthalmology. |
|
|
Van Eer ED, Bretas G, Hiwat H (2018). Decreased endemic malaria in Suriname: Moving towards elimination. Malaria Journal 17. |
|
|
WHO, UNICEF (2018). The ATC/DDD Methodology. |
|
|
WHO Collaborating Centre for Drug Statistics Methodology (2018). The ATC/DDD Methodology. |
|
|
Willis CD, McNeil JJ, Cameron PA, Phillips LE (2012). Monitoring drug safety with registries: Useful components of postmarketing pharmacovigilance systems. Journal of Clinical Epidemiology. |
|
|
World Bank (2021). Suriname | Data. |
|
|
World Health Organization (2020). Decade of healthy ageing: baseline report. Geneva. |
|
|
World Health Organization (n.d.) Ageing and health. |
|
|
Zetterberg M (2016), January 1. Age-related eye disease and gender. Maturitas. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


