Full Length Research Paper

ABSTRACT
Although viral load (VL) measurement has become the reference tool for monitoring antiretroviral treatment in patients living with HIV, most West African countries do not have it systematically. Long-term virological data are rare. Here, the matter is to describe virological outcomes and resistance patterns at 5 years in HIV-1+ patients and to identify early factors associated with long-term virological outcome. This is a prospective cohort study of 971 HIV-infected adults and measurement of HIV viral load and genotyping test. Association between early factors and virological outcome at 5 years after treatment has been evaluated between 2007 and 2012, in Abidjan, Côte d’Ivoire, West Africa. 971 adults on Non-Nucleoside Reverse Transcriptase Inhibitors were included. At M12, M24 and M60 follow-up, 95, 80 and 65% were on active follow-up. 25, 27 and 29% had detectable viral load, of which 53, 75 and 72% had at least one resistance mutation. Of the 109 viruses resistant to M60, 84% were definitely resistant to NRTIs, 97% to NNRTIs and 13% were possibly or definitely resistant to PIs. Adherence (estimated by the Medication Possession Ratio -MPR) and age were significantly associated with virological outcome at M60. Proportion of patients with high viral load and at least one resistance mutation remains high at M60. MPR is useful as early as month 6 to identify patients who could benefit from early interventions, to reinforce adherence and thus avoid selection and accumulation of resistance.
Key words: Human immunodeficiency virus, virological outcome, medication possession ratio.
INTRODUCTION
HIV/AIDS is among the leading causes of death in the world and remains the leading cause of death in Africa. In 2018, the country had 430,000 people living with HIV and 11,000 AIDS-related deaths, a 52% decrease from 2010. 12,000 new HIV infections were recorded, a 54% decrease compared to 2010 (UNAIDS, n.d). The treatment coverage rate was around 63% for all persons living with HIV, while 73% of them knew their serological status.
According report presented in 2018, less than one million of people died from acquired immunodeficiency syndrome (AIDS )-related illnesses. This was largely due to sustained access to antiretroviral therapy, but global disparities remain very large. Despite being one of the most affected regions, West Africa antiretroviral (ARV) coverage rates remain among the lowest: 24%, compared to 42% in sub-Saharan Africa and 47% in Eastern and Southern Africa (MSF, 2016).
Since 2013, several studies have shown the benefits of early treatment (INSIGHT START Study Group et al., 2015; TEMPRANO ANRS 12136 Study Group, 2015) , reduction in mortality, reduction in events classifying as AIDS and in transmission of the virus. WHO (2016) adopted the "test and treat" strategy and recommends that all HIV-infected people receive antiretroviral treatment as soon as possible after screening. This approach essentially recommends starting HIV-infected individuals on first-line ART regardless of the health system capacities to provide adequate treatment monitoring (WHO, 2010) and the number of people on ARVs will therefore continue to rise. The targets set for scaling up HIV treatment beyond 2015 (90% of people living with HIV know their HIV status, 90% of HIV-infected people tested receive sustained antiretroviral treatment and 90% of people receiving antiretroviral treatment have sustained viral load suppression) mean that 15.5 million more people will be on ARVs by 2020, that is, an additional 3.1 million per year, while ensuring that the millions of patients already on ARVs (WHO, 2017 ) are monitored.
This exponential increase in the number of people on antiretroviral therapy will inevitably lead to an increase in treatment failure with associated public health costs (Pham et al., 2017). Maintaining a situation of virological failure in a patient on ARVs exposes them to the risk of selection and accumulation of resistance mutations, as well as to immunological deterioration that can lead to disease progression and an increased risk of transmission of the virus (CNS, ANRS, 2016). According to World Health Organization HIV drug resistance could be responsible for 135,000 additional deaths and 105,000 new infections over the next five years in sub-Saharan Africa alone (WHO, 2017). Diagnosing treatment failures and preventing the build-up of resistance mutations with a timely switch to second- or third-line treatment is one of the remaining challenges (Eholie et al., 2019).
Boender et al. (2015) showed moderate virological success rates (85, 86, 84, 89, 89 and 85% on a per-protocol (PP) basis and 75, 67, 64, 68, and 62% on an intention-to- treat (ITT) basis after 6, 12, 24, 36, 48 and 60 months) with high levels of drug resistance in patients with virological failure (87% of patients had at least one resistance mutation at the time of their first virological failure) . Other studies have shown similar (Boender et al., 2016; Taieb et al., 2017) or suboptimal (Ivers et al., 2005; Hammond and Harry, 2008; Barth et al., 2010) short-term virological outcomes but still with high levels of resistance in virological failure patients (Ivers et al., 2005; Hammond and Harry, 2008; Barth et al., 2010; Hamers et al., 2012; Taieb et al., 2017).
In settings where drug resistance profile is not performed prior to the initiation of ARVs and where viral load measurements and genotyping are not yet the standard of care and few patients switch to second-line ART and switching happens late in the absence of routine viral load monitoring (Haas et al., 2015; Namakoola et al., 2016), describing the rate and pattern of resistance over time can be an important aid to defining appropriate treatment strategies: choice of second- and third-line and measures to avoid selection and accumulation of resistance on one hand, and mutations and unnecessary regime changes on the other hand (Sigaloff and de Wit, 2015).
In 2006, a prospective cohort study of HIV-infected adults who started antiretroviral therapy in three health centres equiped with computerised prescription databases was launched in Abidjan, the economic capital of Côte d'Ivoire, West Africa. According to previous results of this study, 20, 25 and 27% of patients had a detectable viral load (detection threshold of 300 copies/ml) at 6, 12 and 24 months, of which 35, 54 and 75% had at least one resistance mutation, respectively (Messou et al., 2011, 2013).
Long-term virological data are scarce. The aim of the current study design was to describe the prevalence of virological suppression and the prevalence and pattern of resistance mutations and drug susceptibilities after 12 and 60 months of treatment in Côte d’Ivoire, West Africa.
METHODOLOGY
Study design
It is a prospective cohort study of long-term virological outcomes. HIV positive adults who started antiretroviral treatment between February 2006 and 2012 at one of three outpatient clinics in Abidjan and returned for their six-month visit were eligible for this study . HIV-2 positive patients were not eligible. The three clinics were the ‘’Centre de Prise en Charge de Recherche et de Formation Yopougon-Attié (CePReF) (18), the service de prise en charge des personnes vivant avec le VIH de l'hôpital général de Yopougon Attié, and the Centre Médical de Suivi des Donneurs de Sang à Treichville (CMSDS).
All patients received the same standard care and treatment as other patients in their respective clinics (Messou et al., 2011, 2013).
In addition, they received free plasma viral load testing every six months and genotyping at 6, 12, 24 and 60 months.
Viral load measurements were carried out using real time polymerase chain reaction (RT-PCR) every six months, whenever possible. Otherwise, they were carried out on the basis of samples taken and frozen at a later date. Genotyping for resistance was performed at M6, M12, M24 and M60.
Study population
These are the patients included in the study who initiated treatment with non-nucleoside reverse transcriptase inhibitor (NNRTIs) as first-line therapy. The inclusion criteria were as follows: HIV-1 positive or HIV-1+2 positive serology; age > 18 years; antiretroviral treatment naïve patient; ARV treatment started in the center and ongoing for 6 months; for women: no history of antiretroviral prophylaxis at PMTCT. Exclusion criteria: HIV-2 positive serology alone; refusal to participate.
Patients gave written informed consent to participate in the cohort and the study was approved by the Côte d'Ivoire ethics committee.
Changes in viral load and resistance testing between the 6-month (M6) and 12-month (M12) visit and between 12-month (M12) and 24-month (M24) visit for all patients enrolled in this study have been previously documented (Messou et al., 2013, 2010). Factors associated with virological outcomes at M6 and M12 have also been described and the drug possession ratio was strongly associated with virological outcomes at both visits (Messou et al., 2013). The objective of this study is to report on the evolution of viral load and resistance testing between months 12 (M12) and 60 (M60) for all patients who started antiretroviral therapy with an NNRTI-based regimen as first-line treatment.
Care and treatment
All patients followed in the three study clinics started ARV therapy according to the WHO (2003-2006) criteria: WHO clinical stage 4, regardless of CD4 count, CD4 count ≤200 mm-3 regardless of WHO stage, or WHO stage 3 and CD4 count 200-350 mm-3. As of July 2010, the 2010 WHO criteria have been applied (WHO, 2010).
Blood investigations (blood counts, blood sugar, serum creatinine and transaminases) were performed before starting with antiretroviral therapy. CD4 count and complete blood count were measured every six months.
When patients were infected with HIV-1, the first line consisted of two nucleoside reverse transcriptase inhibitors (NRTIs ); zidovudine or stavudine plus lamivudine) and one non-nucleoside reverse transcriptase inhibitor (NNRTI ; efavirenz or nevirapine). When patients were infected with HIV-2 or HIV-1 and HIV-2, first-line antiretroviral therapy consisted of two NRTIs and a protease inhibitor (PI; lopinavir/ritonavir). Only patients who started antiretroviral therapy with an NNRTI-based regimen are included in this study.
Patients paid a flat fee of US$2 per month for antiretroviral drugs and laboratory tests until August 2008, when the national HIV programme made them available free of charge. All patients with a CD4 count ≤500mm-3 also received cotrimoxazole prophylaxis. Isoniazid (INH) prophylaxis was not recommended as it is not part of the national treatment guidelines. Support groups were organized to encourage patients to follow the therapy, and a community team made telephone calls or home visits when patients did not attend the clinic or take antiretroviral
Control and monitoring procedures
All three studied centres used the same standardised forms to record the following variables at routine visits: (i) initial visit: date, sex, date of birth (or age), height, weight, type of HIV (HIV-1, HIV-2, or both); (ii) follow-up visit: date, weight; (iii) ARV initiation visit date: WHO clinical stage, weight; (iv) prescription of drugs (antiretrovirals or others), name and amount of drugs dispensed; (v) CD4 count and complete blood count measurement, CD4 count, CD4 percentage, haemoglobin level and count, name and quantity of drugs dispensed; (v) CD4 count and complete blood count measurement, CD4 count, CD4 percentage, haemoglobin level and platelet, granulocyte and leucocyte counts; (vi) telephone call and home visit dates; patients were contacted and marital status at that time; (vii) patients known to have died, date of death.
Additional procedures
The care provided to patients who agreed to participate in the study differed from that provided to other patients in the same clinic and from the guidelines of the National AIDS Control Programme of Côte d'Ivoire in three ways: (i) plasma HIV-1 RNA viral load measurements were performed every six months (ANRS generic real-time PCR; Biocentric, Bandol, France; detection limit, 300 copies/ml) (Rouet et al., 2005); (ii) for all samples with a detectable viral load (VL ≥ 300 copies/ml), genotypic testing was performed using the ANRS technique (Pasquier et al., 2001) (www.frenchresistance.org). After extraction of plasma RNA, amplification of the reverse transcriptase and protease genes and sequencing were performed. After sequence alignment, interpretation of resistance mutations was done using the latest update of the ANRS algorithm (http://www.hivfrenchresistance.org/2017/Algo2017-HIV1.pdf); (iii) a research coordinator who is dedicated to the monitoring and data management of the cohort and assists in following up patients by telephone and/or home visit. Genotype testing was performed in the virology laboratory of the Necker Hospital in Paris, France. This laboratory undergoes an annual external quality assurance assessment (Descamps et al., 2006).
Data description
Patients were defined as lost to follow-up if: (i) their last contact with the study team was less than month 60; (ii) their death or transfer to another site was not known before month 60; or (iii) no further information on their health status could be obtained within 12 months of the end of the study (that is, between months 60 and 72).
Virological treatment outcome at 5 years (M60) is defined as a categorical variable with three categories: (i) undetectable viral load (UVL); (ii) detectable viral load and no resistance mutations (DVL NoR); (iii) detectable viral load and resistance mutations (DVLR).
Data analysis
The association between early factors (M0-M6) and virological outcome at M60 defined as a three-category categorical variable was assessed using multinomial regression. The main explanatory variables were: variables at initiation (M0): centre, sex, age, WHO stage, CD4 count, body mass index (BMI), haemoglobin level, history of tuberculosis, ARV regimen at initiation; variables during the first 6 months of treatment (M0-M6): delta CD4 M0-M6, delta BMI M0-M6, MPR M0-M6.
Statistical analyses were performed using Stata® software and SAS® software.
RESULTS
Main characteristics of NNRTI patients
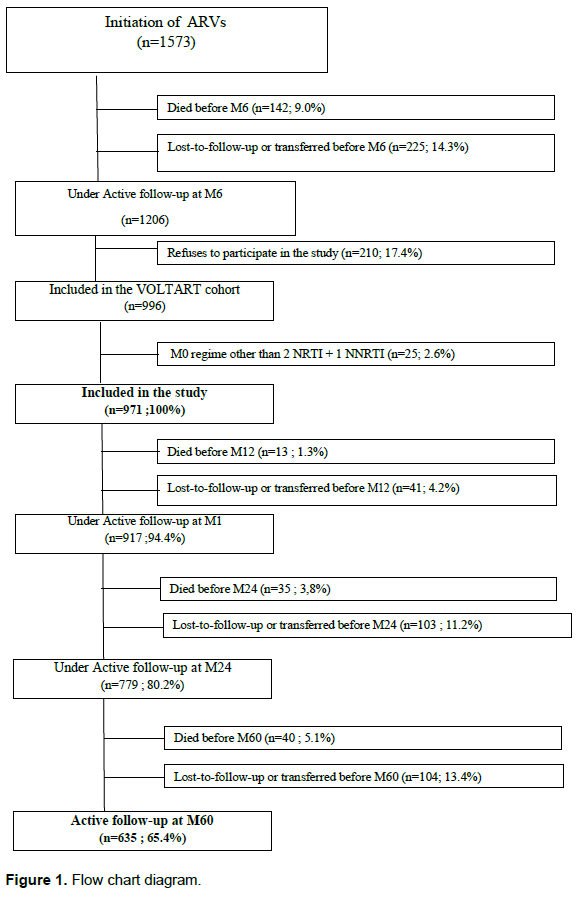
One thousand and five hundred seventy three adults started antiretroviral therapy at the three studied centres between February 2006 and May 2007. At M6, 1206 patients were still alive and being managed, of whom 996 gave their consent to participate. The median age was 36 years (interquartile range [IQR], 30-43) and 731 patients (75%) were female. The distribution of patients between the three study centres was as follows: 96 patients at the CMSDS (10%), 626 patients at CePReF (64%) and 249 patients at the Yopougon Attié General Hospital (26%). At treatment initiation, 971 were on first-line NNRTIs and were included in this study. At M60, 635 (65%) were still alive and under active follow-up, 88 had died, 147 were lost to follow-up and 101 had been transferred (Figure 1).
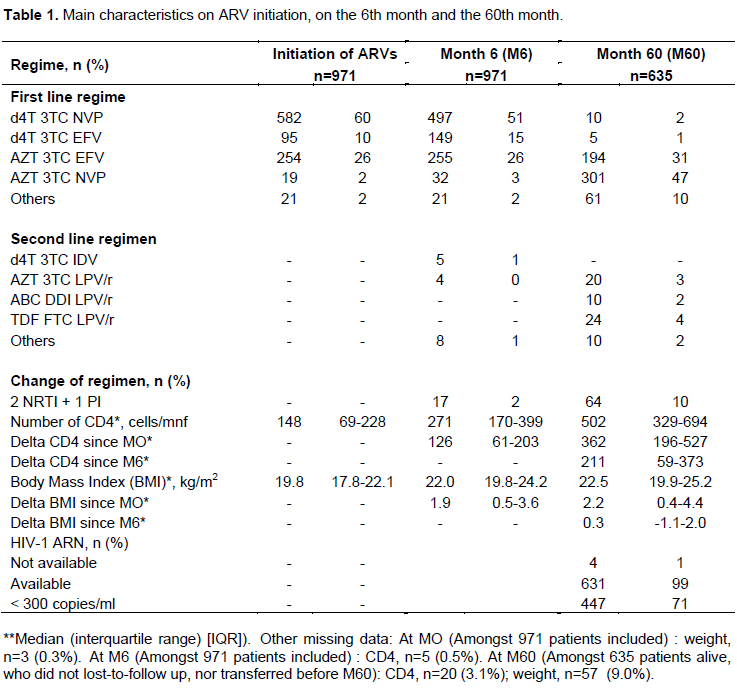
The main characteristics of the 971 NNRTI patients are shown in Table 1. The main ARV regimens at initiation were d4t+3TC+NVP (60%), AZT+3TC+EFV (26%) and d4T+3TC+EFV (10%). At M60, 571 patients (90%) were still on a first-line regimen and 64 patients (10%) were on a second-line regimen. While d4T was the main regimen at M0, the main first-line regimens at M60 were AZT+3TC+NVP (47%) and AZT+3TC+EFV (31%), reflecting the phasing out of d4T. The main second-line regimens at M60 were TDF+FTC+LPV/r (4%) and AZT+3TC+LPV/r (3%). The median CD4 count was 148 cells/mm3 (IQR, 69-228) at baseline, 271 cells/mm3 (IQR, 170-399) at M6 and 502 cells/mm3 (IQR, 329-694) at M60.
Virological status of patients during follow-up (M12, M24, M60)
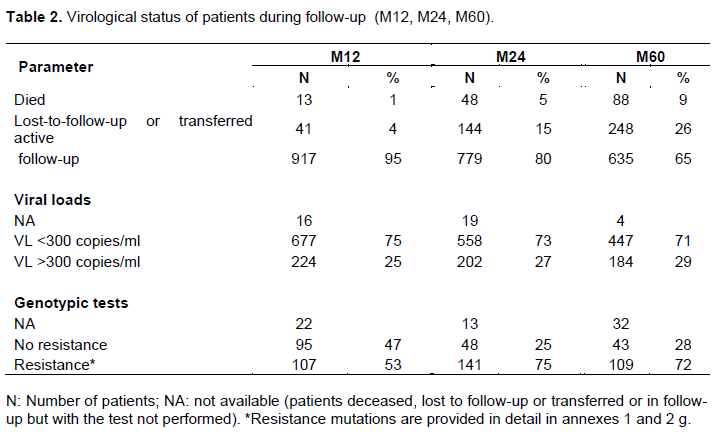
Viral load results were available for 901 patients at M12, 760 patients at M24 and 631 patients at M60. 25, 27 and 29% of patients had detectable viral loads at M12, M24 and M60, respectively.
Genotypic resistance testing could be performed in 202 (90%) patients at M12, 189 (94%) patients at M24 and 152 (83%) patients at M60. 53, 75 and 72% had at least one resistance mutation at M12, M24 and M60, respectively (Table 2).
Description of virus loads and resistance profile at M60
At M60, 631 patients had a viral load measurement (2 patients were in follow-up but not sampled and 2 patients were sampled but their results were not available). Of these, 184 (29%) had a detectable viral load (VL ≥300 copies/ml) and 447 (71%) had an undetectable viral load (VL <300 copies/ml) (Table 2).
Out the 184 patients with detectable viral load, 22 (12%) had a viral load between 300 and 1000 copies/ml and 162 (88%) had a viral load greater than 1000 copies/ml.
At M60, 109 patients had virus carrying at least one resistance mutation. These patients represent 59% of the patients with a detectable viral load at M60 and 72% of the patients with genotyping results available (Table 2).
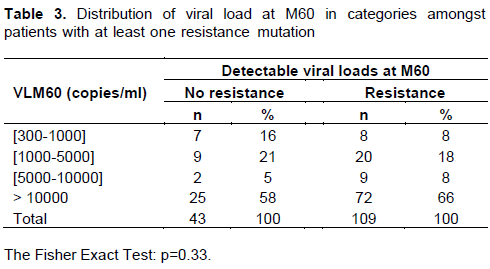
Out of the 109 patients with a detectable viral load and at least one resistance mutation, 8 (7%) had a viral load between 300 and 1,000 copies/ml, 20 (18%) had a viral load between 1,000 and 5,000 copies/ml, 9 (8%) had a viral load between 5,000 and 10,000 copies/ml, and 72 (66%) had a viral load above 10,000 copies/ml. The class distribution of viral load at M60 did not differ significantly between patients with and without M60 resistance (p=0.33) (Table 3).
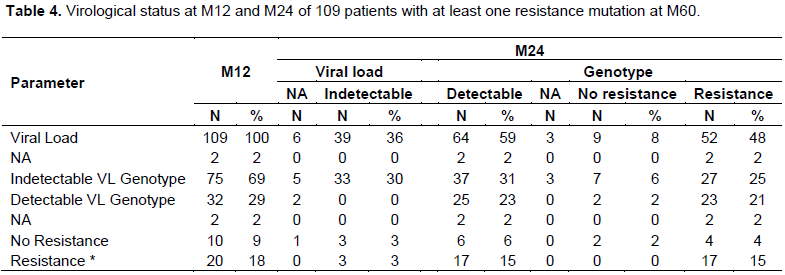
Out of the 109 patients with a detectable viral load and at least one resistance mutation at M60, 64 (59%), it is noticed that those patients had a detectable viral load at M24, of which 52 (48%) already had at least one resistance mutation. 17 (15%) patients carried at least one resistance mutation from M12 to M60. Out of the 45 patients who had no detectable or available viral load at M24 with a resistance at M60, 4 (3%), were no more seen, or were transferred at M24, 2 (2%) had no viral load measurement and 39 (36%) patients had undetectable viral load (Table 4).
Out of the 109 virus resistants at M60, 92 (84%) had a proven resistance to NRTI, 106 (97%) had a proven resistance to NNRTI, and 14 (13%) had an established or possible resistance to PI. 17 patients (15%) were resistant to a certain type; namely: (the NRTI alone, n=T (1%); NNRTI alone, n=15 (14%); PI alone, n=l (1%)), 81 (74%) were resistant to two types: (NRTI+NNRTI, n=79 (72%); NRTI+PI, n=l (1%); NNRTI+PI, n=l (1%)) and 11 (10%) were resistants to three types (NRTI+NNRTI+PI, n = 1 1 (10%)) (Appendix 1).
Concerning resistance to NNRTIs, 106 (97%) patients carrying a resistant virus to nevirapine, 102 (94%) to efavirenz, 48 (44%) to rilpivirine and, 44 (40%) to etravirine, with a proven (resistance, n=32 (29%); resistance, n=12 (11%)) (Annexe 1).
Concerning resistance to NRTI, 92 (84%) patients carriers of a resistance to lamivudine/emtricitabine, 27 (25%) stavudine, 25 (23%) zidovudine, 9 (8%) patients being treated with tenofovir (with a resistance which is sure at n=7 (6%); possible resistance n=2 (2%)), 92 (85%) patients treated with abacavir (with a resistance at n=16 (15%); a possible resistance at n=76 (70%)), 3 (3%) patients being treated with didanosine (Appendix 1).
Concerning the resistance to PI, 14 (13%) patients carriers of a resistance to saquinavir (resistance which is confirmed, at n=2 (2%); possible resistance, n=12 (11%)) and 3 (3%) had a possible resistance to atazanavir (Appendix 1).
The most frequent mutation associated with resistance to NNRTIs was 103N. The most frequent mutation associated with resistance to NRTIs was 184V and 215 Y/F (Appendix 2).
Analysis of early factors associated with virological outcome at M60
This ancillary study aims to describe early factors associated with virological outcome at M60. The study population corresponds to patients still in active follow-up at M60, with viral load results (631 patients). Patients who died, were lost to follow-up or transferred before M60 were excluded from the analysis (340 patients).
This ancillary study aims to analyse early factors associated with virological outcome at M60. The study population consisted of patients still under active follow-up at M60 with viral load results (631 patients). Patients who died, were lost to follow-up or transferred before M60 were excluded from the analysis (340 patients).
Comparison of their initial characteristics with patients not included in the analysis (deceased, transferred, lost to follow-up) shows that there is no statistically significant difference between the two groups, except for the centre, which can be explained by the different patient profiles in each centre. The patients at the CMSDS are blood donors, more aware of the care system and this centre follows, for example, seroconverters with low immunosuppression.
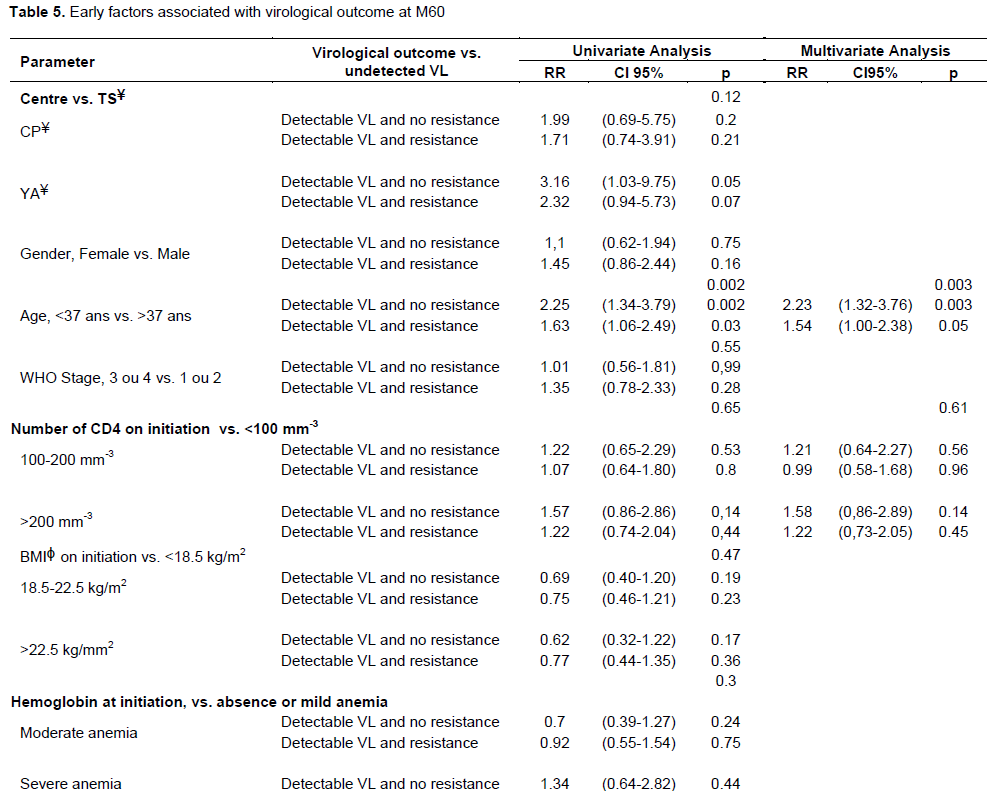
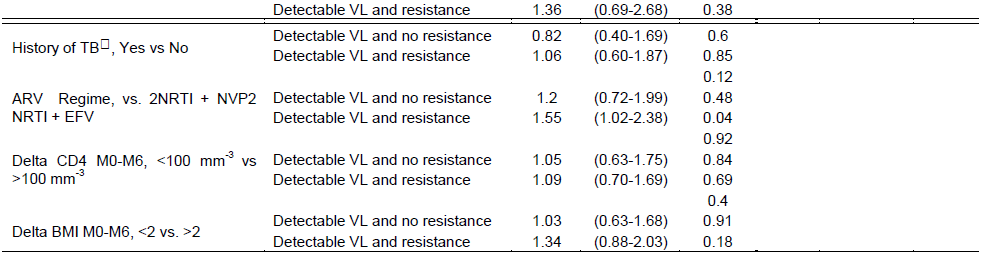
In terms of risk factors, adherence (p=0.001) and age group (p=0.003) were significantly associated with virological outcome at M60. Patients with an MPR of less than 80% between initiation and month 6 were 3.12 times more likely to have a detectable viral load with resistance mutations than an undetectable viral load at M60, compared with patients with a MPR of 95% or greater (p<0.0001). Similarly, patients under 37 years of age were 2.23 times more likely to have a detectable viral load without resistance mutations than an undetectable viral load at M60 and 1.54 times more likely to have a detectable viral load with resistance mutations than an undetectable viral load at M60, compared to patients over 37 years of age. CD4 count at initiation was not significantly associated with virological outcome at M60 (Table 5).
DISCUSSION
This study is a prospective cohort in three major HIV care programs in Abidjan, Côte d'Ivoire. These almost 10-year-old results are still relevant in a "test and treat" context in which asymptomatic patients have been starting ARV treatment immediately since 2015, with a major compliance issue for patients who do not feel "sick". The lessons to be learned are also important in terms of the management of virological failure and resistance mutations by practitioners, in the era of “dolutegravir switch” (an integrase inhibitor and powerful antiretroviral, very effective); many countries in sub-Saharan Africa are gradually substituting NNRTIs to adopt the WHO-recommended second-generation integrase-strand transfer inhibitor (WHO, 2019). In order to maintain the long-term efficacy of these new therapies, all factors involved in the management and follow-up of a patient (along the continuum of care), both individual, structural and programmatic, must be effectively monitored (Villabona-Arenas et al., 2016).
The establishment of a data analysis and monitoring system for sites where this new therapeutic guideline is being implemented or will soon be implemented would be useful for HIV programs in sub-Saharan Africa; this data would undoubtedly help them to capitalize as soon as possible on the actions to be taken in order to preserve the gains and benefits of these powerful treatments. It is clearly established that when ARVs are not effective (due to de facto monotherapy, poor adherence to treatment or monitoring of therapeutic response), the waiting time until the appearance of virological failure or resistance mutation should be shorter and vice versa (Feder et al., 2016).
To our knowledge, this is one of the largest cohort studies of long-term virological outcomes in sub-Saharan Africa with such detailed data on resistance mutations. Data on this type of intervention, as in Senegal, are invaluable to ensure a « smooth » transition to dolutegravir or EFV 400 mg as recommended (Diouara Diop-Ndiaye et al., 2014; Diouara Ndiaye et al., 2014a, b). However, these results must be interpreted taking into account limitations of the study.
First of all, there was no genotypic resistance test carried out before the initiation of antiretroviral treatment, which makes it impossible to know the proportion of primary resistance. However, it has been estimated to be less than 5% in Côte d'Ivoire (Toni et al., 2007; Ayouba et al., 2009). Secondly, some data are missing. 17% of patients refused to participate in this study. The current study found 2, 2 and 1% of patients being followed up at M12, M24 and M60 did not have viral load measurements; 10, 6 and 17% of patients with detectable viral load at M12, M24 and M60 did not have resistance genotyping test results. Thirdly, the detection threshold was 300 copies/ml, which may have led to an underestimation of the proportion of patients with detectable viral load. On the other hand, amplification difficulties are to be expected in the case of a viral load of less than 1,000 copies/ml, so that the detection threshold for HIV must have had an impact on the proportion of patients with resistant virus. Finally, almost one third of the patients who started ARV treatment at the three sites who died, were transferred or were lost to follow-up before the 6th month. Their outcomes were probably worse than those of the patients included in the study 25% and 29% of patients who started antiretroviral therapy and were still on active follow-up at M60 had a detectable viral load (≥ 300 copies/ml) at M12 and M60. Of these, 85 and 88% had a viral load ≥ 1000 copies/ml. These figures are more than 2 times higher than what is expected to achieve the 90-90-90 targets.
Out of the patients who had an undetectable viral load at M12, 26% had a detectable viral load at M60, two out of three of whom harboured resistant viruses. These results underline that viral load suppression is a dynamic process and that adherence must be constantly monitored. While viral load measurement has become the reference tool for ARV monitoring, access is still limited in most West African countries (MSF, 2016) and more needs to be done.
The percentage of patients infected with resistant HIV-1 strains, representing 54 and 72% of patients with detectable viral load and genotype test results available at 12 and 60 months. Previous studies in sub-Saharan Africa have shown similar or higher rates of resistance mutations in virological failure (Boullé et al., 2016; Konou et al., 2015; Loubet et al., 2015; Namakoola et al., 2016; Steegen et al., 2017; Villabona-Arenas et al., 2016). This finding has several implications. First, 46 and 28% of patients with virological failure had virus that was still susceptible to ongoing treatment at M12 and M60. These patients need to be identified in order to enhance adherence to treatment and avoid unnecessary regime changes. Second, according to previous results from this study (Namakoola et al., 2016; Pham et al., 2017), 35, 54, 75, and 72% of patients with detectable viral load and available genotype test results, had a resistance mutation at M6, M12, M24 and M60. The mutation rates tend to stabilise or decrease over time, but at M60 there is still a high proportion of patients with high viral loads and at least one resistance mutation, that is, patients with fewer treatment options, who are likely to have an unfavourable disease course and to transmit resistant HIV strains.
In the era of Dolutegravir, these patients who are not "virologically suppressed" would not benefit from it because the national recommendations recommend switching to this molecule only for those who are virally suppressed; otherwise, intense reinforcement of compliance and if still unsuccessful, switching to 2nd line. Adherence data from two large cohorts in Africa and Asia have highlighted that these are interventions that need to occur as early as possible to minimize virologic failure and the emergence of ARV resistance (Bijker et al., 2017).
The genotypic resistance profile in patients receiving antiretroviral therapy with an NRTI-based regimen was as initially described (Loubet et al., 2015; Namakoola et al., 2016; Steegen et al., 2017; Villabona-Arenas et al., 2016). 95 and 100% of resistant viruses were resistant to lamivudine/emtricitabine and/or nevirapine/ efavirenz at M12 and M60. During the study period, most patients started antiretroviral therapy with ZDV or d4T plus 3TC plus NVP or EFV. As expected, the most frequent NRTI mutations were M184V and TAMs (T215Y/F) while tenofovir, abacavir and didanosine selected resistance mutations are rare. The frequency of TAMs increases from 8.1 to 25% in all resistant strains from months 12 to 60. In addition, five patients harboured virus with codon 69 insertion. These results reflect the increased complexity of NRTI resistance patterns over time, with more multiple NRTI.
In addition, although most viruses remained susceptible to the NRTIs used for second-line treatment (tenofovir, abacavir), some studies have shown that tenofovir-based regimens fail in a significant proportion of patients who have evidence of prior exposure and drug resistance to older thymidine analogues such as zidovudine and stavudine (Gregson et al., 2017). At M60, 98% of the resistant viruses had lost sensitivity to the first-generation NRTIs nevirapine and efavirenz, and only 54% remained fully sensitive to the second-generation NRTIs rilpivirine and etravirine. Finally, only one patient harboured virus potentially resistant to saquinavir/ritonavir. Other studies showed higher rates of PI resistance, but the patients included had been on antiretroviral therapy for more years (Namakoola et al., 2016).
In conclusion, prevention of the emergence of resistance mutations by monitoring viral load and reinforcing compliance in patients with detectable viral load is important beyond 5 years of follow-up. Increasing access to viral load and genotypic resistance testing for detectable viral load should be a priority and the use of an integrase inhibitor such as Dolutegravir with a high genetic barrier is an alternative for patients with resistance to all NRTIs.
Ensuring a continuous supply of drugs and facilitating timely reporting of viral load and genotypic results when available are issues that are still difficult to implement in practice but should no longer be. Finally, it remains important to determine the factors associated with mutation selection, such as advanced stages of infection (De Beaudrap et al., 2013), that can help predict the presence of resistance in order to help clinicians choose the best treatment option when genotyping tests are not available.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Ayouba A, Lien TTX, Nouhin J, Vergne L, Aghokeng AF, Ngo-Giang-Huong N, Diop H, Kane CT, Valéa D, Rouet F, Joulia-Ekaza D, Toni TD, Nerrienet E, Ngole EM, Delaporte E, Costagliola D, Peeters M, Chaix ML (2009). Low prevalence of HIV type 1 drug resistance mutations in untreated, recently infected patients from Burkina Faso, Côte d'Ivoire, Senegal, Thailand, and Vietnam?: The ANRS 12134 study. AIDS Research and Human Retroviruses 25(11):1193?1196. |
|
|
Barth RE, van der Loeff MFS, Schuurman R, Hoepelman AIM, Wensing AMJ (2010). Virological follow-up of adult patients in antiretroviral treatment programmes in sub-Saharan Africa: A systematic review. The Lancet Infectious Diseases 10(3):155?166. |
|
|
Bijker R, Jiamsakul A, Kityo C, Kiertiburanakul S, Siwale M, Phanuphak P, Akanmu S, Chaiwarith R, Wi FW, Sim BL, Boender TS, Ditangco R, Rinke De Wit TF, Sohn AH, Hamers RL (2017). Adherence to antiretroviral therapy for HIV in sub-Saharan Africa and Asia?: A comparative analysis of two regional cohorts. Journal of the International AIDS Society 20(1):21218. |
|
|
Boender TS, Kityo CM, Boerma RS, Hamers RL, Ondoa P, Wellington M, Siwale M, Nankya I, Kaudha E, Akanmu AS, Botes ME, Steegen K, Calis JCJ, Rinke de Wit TF, Sigaloff KCE (2016). Accumulation of HIV-1 drug resistance after continued virological failure on first-line ART in adults and children in sub-Saharan Africa. The Journal of Antimicrobial Chemotherapy 71(10):2918?2927. |
|
|
Boullé C, Guichet E, Kouanfack C, Aghokeng A, Onambany B, Ikaka C M, Ngock E, Tsoumsta L, Msellati P, Mpoudi-Ngolé E, Peeters M, Delaporte E, Laurent C (2016). Virologic Failure and Human Immunodeficiency Virus Drug Resistance in Rural Cameroon With Regard to the UNAIDS 90-90-90 Treatment Targets. Open Forum Infectious Diseases 3(4). |
|
|
De Beaudrap P, Thiam M, Diouf A, Toure-Kane C, Ngom-Guèye NF, Vidal N, Mboup S, Ndoye I, Sow, PS, Delaporte E, ANRS 1215 Study Group. (2013). Risk of virological failure and drug resistance during first and second-line antiretroviral therapy in a 10-year cohort in Senegal?: Results from the ANRS 1215 cohort. Journal of Acquired Immune Deficiency Syndromes 62(4):381?387. |
|
|
Descamps D, Delaugerre C, Masquelier B, Ruffault A, Marcelin AG, Izopet J, Chaix ML, Calvez V, Brun-Vézinet F, Costagliola D. (2006). Repeated HIV-1 resistance genotyping external quality assessments improve virology laboratory performance. Journal of Medical Virology 78(2):153-160. |
|
|
Diouara AAM, Diop-Ndiaye H, Kebe-Fall K, Tchiakpè E, Ndiaye O, Ayouba A, Peeters M, Mboup S, Kane CT (2014). Dried blood spots for HIV-1 drug resistance genotyping in decentralized settings in Senegal. Journal of Medical Virology 86(1):45-51. |
|
|
Diouara AAM, Ndiaye HD, Guindo I, Bangoura N, Cissé M, Edmond T, Bougoudogo F, Mboup S, Peeters M, Ayouba A, Kane NCT (2014). Antiretroviral treatment outcome in HIV-1-infected patients routinely followed up in capital cities and remote areas of Senegal, Mali and Guinea-Conakry. Journal of the International AIDS Society 17, 19315. |
|
|
Eholie SP, Moh R, Benalycherif A, Gabillard D, Ello F, Messou E, Zoungrana J, Diallo I, Diallo M, Bado G, Cisse M, Maiga AI, Anzian A, Toni T, Congo-Ouedraogo M, Toure-Kane C, Seydi M, Minta DK, Sawadogo A, Thilao ANRS 12269 Study Group (2019). Implementation of an intensive adherence intervention in patients with second-line antiretroviral therapy failure in four west African countries with little access to genotypic resistance testing?: A prospective cohort study. The Lancet HIV 6(11):e750-e759. |
|
|
Feder AF, Rhee SY, Holmes SP, Shafer RW, Petrov DA, Pennings PS (2016). More effective drugs lead to harder selective sweeps in the evolution of drug resistance in HIV-1. ELife 5:e10670. |
|
|
Haas AD, Keiser O, Balestre E, Brown S, Bissagnene E, Chimbetete C, Dabis F, Davies MA, Hoffmann CJ, Oyaro P, Parkes-Ratanshi R, Reynolds SJ, Sikazwe I, Wools-Kaloustian K, Zannou DM, Wandeler G, Egger M (2015). IeDEA southern Africa, east Africa, and west Africa. Monitoring and switching of first-line antiretroviral therapy in adult treatment cohorts in sub-Saharan Africa?: Collaborative analysis. The Lancet HIV 2(7):e271-278. |
|
|
Hamers RL, Sigaloff KCE, Wensing AM, Wallis CL, Kityo C, Siwale M, Mandaliya K, Ive P, Botes ME, Wellington M, Osibogun A, Stevens WS, Rinke de Wit TF, Schuurman R (2012). PharmAccess African Studies to Evaluate Resistance (PASER). Patterns of HIV-1 drug resistance after first-line antiretroviral therapy (ART) failure in 6 sub-Saharan African countries?: Implications for second-line ART strategies. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America 54(11):1660-1669. |
|
|
Hammond R, Harry TC (2008). Efficacy of antiretroviral therapy in Africa?: Effect on immunological and virological outcome measures -- a meta-analysis. International Journal of STD & AIDS 19(5):291-296. |
|
|
INSIGHT START Study Group, Lundgren JD, Babiker AG, Gordin F, Emery S, Grund B, Sharma S, Avihingsanon A, Cooper DA, Fätkenheuer G, Llibre JM, Molina JM, Munderi P, Schechter M, Wood R, Klingman KL, Collins S, Lane HC, Phillips AN, Neaton JD (2015). Initiation of Antiretroviral Therapy in Early Asymptomatic HIV Infection. The New England Journal of Medicine 373(9):795?807. |
|
|
Ivers LC, Kendrick D, Doucette K. (2005). Efficacy of antiretroviral therapy programs in resource-poor settings?: A meta-analysis of the published literature. Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America 41(2):217-224. |
|
|
Konou AA, Dagnra AY, Vidal N, Salou M, Adam Z, Singo-Tokofai A, Delaporte E, Prince-David M, Peeters M (2015). Alarming rates of virological failure and drug resistance in patients on long-term antiretroviral treatment in routine HIV clinics in Togo. AIDS (London, England) 29(18):2527?2530. |
|
|
Loubet P, Charpentier C, Visseaux B, Borbor A, Nuta C, Adu E, Chapplain JM, Baysah M, Tattevin P, Yazdanpanah Y, Descamps D (2015). Prevalence of HIV-1 drug resistance among patients failing first-line ART in Monrovia, Liberia?: A cross-sectional study. The Journal of Antimicrobial Chemotherapy 70(6):1881-1884. |
|
|
Messou E, Chaix ML, Gabillard D, Minga A, Losina E, Yapo V, Kouakou M, Danel C, Sloan C, Rouzioux C, Freedberg KA, Anglaret X (2011). Association between medication possession ratio, virologic failure and drug resistance in HIV-1-infected adults on antiretroviral therapy in Côte d'Ivoire. Journal of Acquired Immune Deficiency Syndromes 56(4):356-364. |
|
|
Messou E, Chaix ML, Gabillard D, Yapo V, Toni T, Minga A, Kouakou MG, Ouattara E, Rouzioux C, Danel C, Eholie SP, Anglaret X (2013). Increasing rate of TAMs and etravirine resistance in HIV-1-infected adults between 12 and 24 months of treatment?: The VOLTART cohort study in Côte d'Ivoire, West Africa. Journal of Acquired Immune Deficiency Syndromes 64(2):211-219. |
|
|
Médecins sans frontières (MSF) (2016). Rapport Le Prix de l'oubli-Des millions de personnes en Afrique occidentale et centrale restent en marge de la lutte mondiale contre le VIH. Médecins sans frontières. |
|
|
Namakoola I, Kasamba I, Mayanja BN, Kazooba P, Lutaakome J, Lyagoba F, Kapaata AA, Kaleebu P, Munderi P (2016). CoLTART study team. From antiretroviral therapy access to provision of third line regimens?: Evidence of HIV Drug resistance mutations to first and second line regimens among Ugandan adults. BMC Research Notes 9(1):515. |
|
|
Pasquier C, Millot N, Njouom R, Sandres K, Cazabat M, Puel J, Izopet J (2001). HIV-1 subtyping using phylogenetic analysis of pol gene sequences. Journal of Virological Methods, 94(1-2):45-54. |
|
|
Pham MD, Romero L, Parnell B, Anderson DA, Crowe SM, Luchters S (2017). Feasibility of antiretroviral treatment monitoring in the era of decentralized HIV care?: A systematic review. AIDS Research and Therapy 14(1):3. |
|
|
Rouet F, Chaix ML, Nerrienet E, Ngo-Giang-Huong N, Plantier JC, Burgard M, Peeters M, Damond F, Ekouevi DK, Msellati P, Ferradini L, Rukobo S, Maréchal V, Schvachsa N, Wakrim L, Rafalimanana C, Rakotoambinina B, Viard JP, Seigneurin JM, Rouzioux C (2007). Impact of HIV-1 genetic diversity on plasma HIV-1 RNA Quantification?: Usefulness of the Agence Nationale de Recherches sur le SIDA second-generation long terminal repeat-based real-time reverse transcriptase polymerase chain reaction test. Journal of Acquired Immune Deficiency Syndromes 45(4):380-388. |
|
|
Sigaloff KCE, de Wit TFR (2015). ART in sub-Saharan Africa: The value of viral load monitoring. The Lancet HIV 2(7):e261-262. |
|
|
Steegen K, Bronze M, Papathanasopoulos MA, van Zyl G, Goedhals D, Variava E, MacLeod W, Sanne I, Stevens WS, Carmona S (2017). HIV-1 antiretroviral drug resistance patterns in patients failing NNRTI-based treatment?: Results from a national survey in South Africa. The Journal of Antimicrobial Chemotherapy 72(1):210-219. |
|
|
Taieb F, Madec Y, Cournil A, Delaporte E (2017). Virological success after 12 and 24 months of antiretroviral therapy in sub-Saharan Africa?: Comparing results of trials, cohorts and cross-sectional studies using a systematic review and meta-analysis. PloS One 12(4):e0174767. |
|
|
TEMPRANO ANRS 12136 Study Group, Danel, C, Moh R, Gabillard D, Badje A, Le Carrou J, Ouassa T, Ouattara E, Anzian A, Ntakpé JB, Minga A, Kouame GM, Bouhoussou F, Emieme A, Kouamé A, Inwoley A, Toni T, Ahiboh H, Kabran M, Anglaret X (2015). A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa. The New England Journal of Medicine 373(9):808-822. |
|
|
Toni T. d'Aquin, Masquelier B, Minga A, Anglaret X, Danel C, Coulibaly A, Chenal H, Dabis F, Salamon R, Fleury HJ, Primo-CI ANRS 1220 Study Group (2007). HIV-1 antiretroviral drug resistance in recently infected patients in Abidjan, Côte d'Ivoire?: A 4-year survey, 2002-2006. AIDS Research and Human Retroviruses 23(9):1155-1160. |
|
|
UNAIDS (n. d.). UNAIDS (2020). Country factsheets, Côte d'Ivoire. Consulté 10 décembre 2021, à l'adresse. |
|
|
Villabona-Arenas CJ, Vidal N, Guichet E, Serrano L, Delaporte E, Gascuel O, Peeters M (2016). In-depth analysis of HIV-1 drug resistance mutations in HIV-infected individuals failing first-line regimens in West and Central Africa. AIDS (London, England) 30(17):2577-2589. |
|
|
World Health Organization (WHO) (2010). Antiretroviral Therapy for HIV Infection in Adults and Adolescents?: Recommendations for a Public Health Approach: 2010 Revision. World Health Organization. |
|
|
World Health Organization (WHO) (2019). Policy brief?: Update of recommendations on first- and second-line antiretroviral regimens (WHO/CDS/HIV/19.15). World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


