Full Length Research Paper

ABSTRACT
Cirrhosis carries high morbidity and mortality due to various complications and decompensation, which can be decreased by following various practice guidelines, which are variedly followed in actual practice. This multicentric prospective/retrospective study was conducted over a 3 month period to assess actual care of patients with cirrhosis. 416 patients with cirrhosis (median age 53 years, 316 males) were included in the study. A comprehensive protocol was devised taking into account various practice guidelines. Patients were divided into 3 groups. Group 1: Newly diagnosed patients evaluated as per protocol. Group 2: Patients previously diagnosed at the study centers, past practices assessed. Group 3: patients diagnosed previously at non-study centers, their surveillance practices were assessed. Patients in the 3 groups were similar in terms of age and gender ratio. There was significant difference between varices screening practices amongst 3 groups, however there was similar nonselective beta blockers (NSBB)/endoscopic variceal ligation (EVL) prophylaxis practices. Ultrasound surveillance for ascites varied significantly amongst 3 groups. There was significant difference between antibiotic prophylaxis practice in high risk ascites patients between groups 1 and 2. Evaluation of renal function at baseline and ultrasound surveillance for hepatocellular carcinoma was significantly different in 3 groups. All patients in group 1 underwent SpO2 monitoring, however none in groups 2 or 3 previously had SpO2 monitoring. Surveillance and treatment practices for various complications of cirrhosis vary widely in real life and falls well short of goals. Presence of dedicated protocols helps in improving the way we care for our patients with cirrhosis.
Key words: Portal hypertension, varices, ascites, hepatocellular carcinoma (HCC), surveillance
INTRODUCTION
Burden of disease due to liver cirrhosis is increasing worldwide because of increasing alcohol consumption, epidemic of diabetes and obesity and hepatitis C infection (Williams, 2006). Approximate prevalence of clinical cirrhosis is 0.1% and histological cirrhosis 1% in an adult population (Schuppan, 2008). Prevalence of cirrhosis increases as the age advances (Jansen, 2002). Hence improving life span worldwide will increase the burden of cirrhosis. Liver cirrhosis is defined as development of regenerative nodules surrounded by fibrous septa in response to chronic liver injury (GarciaTsao et al., 2010). This leads to vascular remodeling and giving rise to portal hypertension and end stage liver disease (Amarapurkar et al., 2007). Liver transplantation is the only treatment which improves both longevity and quality of life in patients with decompensated liver cirrhosis (O'Brien et al., 2013). However every patient with decom-pensated liver cirrhosis is not eligible for transplantation, and it is not available for majority of the patients.
Our current understanding of natural history, pathophysiology and treatment of complication has resulted in improved management and life expectancy in patients with decompensated liver cirrhosis (Tsochatzis et al., 2012). Median survival of patients with compen-sated cirrhosis is 12 years while that of decompensated patients is reduced to 2 years (GarciaTsao et al., 2010). Approximately 5 to 7% of the patients change from compensated stage to decompensated stage every year (D´Amico, 2001). Portal hypertension (PH) is a universal consequence of cirrhosis responsible for most of the complications like esophagogastric varices, variceal bleeding, ascites, spontaneous bacterial peritonitis, hepatorenal syndrome and hepatic encephalopathy (GarciaTsao et al., 2010). PH in cirrhosis is defined by hepatic venous pressure gradient (HVPG) more than 5 mm of mercury. HVPG is an indirect measure of portal pressure. Now it is clear that HVPG more than 10 is a significant PH above which the complications like variceal bleeding and ascites develop (Bosch et al., 2008). Currently, proposed classification of cirrhosis is based on the degree of PH and associated clinical features. Development of ascites, variceal bleeding and hepatic encephalopathy is considered to be decompensated cirrhosis (GarciaTsao et al., 2010). PH results from increase in the intrahepatic resistance which has dynamic and fixed components and it is coupled with increase in the portal blood flow (GarciaTsao et al., 2010). Therapeutic interventions which can reduce the HVPG like non selective beta blockers and transjugular intrahepatic portosystemic shunt (TIPS) can be helpful in combating complications of cirrhosis, and they have been shown to improve survival (Garcia-Tsao et al., 2009; Garcia-Tsao et al., 2007; Garcia-TsaoG and Bosch, 2010). A meta-analysis of many studies has shown non selective beta blockers and endoscopic band ligation as the effective therapies for primary and secondary prophylaxis of variceal bleeding due to portal hypertension which significantly improve the survival in patients with cirrhosis (Mellinger and Volk, 2013).
Angiogenesis in cirrhosis of any etiology leads to the development of hepatocellular carcinoma (HCC) (Bruix and Sherman, 2011). Incidence of HCC is also increasing world-wide due to epidemics of hepatitis C infection and non alcoholic steato-hepatitis (NASH). Surveillance for HCC in high risk population with ultrasound and alpha-feto protein (AFP) has been recommended by various guidelines (Bruix and Sherman, 2011; Asia Pacific Working Party on Prevention of Hepatocellular Carcinoma, 2010; Omata et al., 2010). This strategy has led to the detection of early HCC and curative treatment for the same. Bacterial infection is common in cirrhosis, especially spontaneous bacterial peritonitis, with one month mortality of 30%. Oral prophylactic antibiotics and bowel decontamination have shown to improve long term outcomes in patients with decompensated cirrhosis (European Association for the Study of the Liver (EASL), 2010; Runyon, 2013).
Therapeutic modalities can reverse the cirrhosis. These modalities according to the etiology are: (1) abstinence for alcoholic cirrhosis, (2) antiviral therapy for hepatitis B, (3) immune-suppression for autoimmune hepatitis, (4) relieving biliary obstruction in patients with secondary biliary cirrhosis, (5) antiviral therapy for hepatitis C, and (6) relieving obstruction in patients with Budd Chiari syndrome. Future therapies like anti fibrotic, anti-angiogenic agents and anti-coagulants may potentially reduce liver fibrosis, thereby reversing cirrhosis (GarciaTsao et al., 2010). Stem cell therapy may be helpful in patients with liver cirrhosis (Amin et al., 2013). Principles of management of patients with liver cirrhosis are: Prevent hepatic injury by identifying the etiology and treating it at the earliest. Identify cirrhosis at the asymptomatic stage, treat complications at the earliest. Avoid iatrogenic injuries and implement appropriate life style modification. Cirrhosis should be considered as a potentially treatable chronic disease. The treatment of cirrhosis should be based on a chronic care model with frequent follow-up. Surveillance practices for complica-tions of cirrhosis have been developed on the basis of large number of randomized control trials. Compliance with the practice guidelines for surveillance has shown to be associated with a significant improvement in survival in patients with variceal bleeding and HCC (Tsochatzis et al., 2012)(Garcia-Tsao et al., 2009; Garcia-Tsao et al., 2007; Garcia-TsaoG and Bosch, 2010; Mellinger and Volk, 2013) (European Association for the Study of the Liver (EASL), 2010; Runyon, 2013; Amarapurkar, 2012).
In spite of this overwhelming evidence, the guidelines in the management of cirrhosis are not followed properly (Mellinger and Volk, 2013). Hence, we planned this prospective/retrospective study to assess how appropriately we are caring for patients with cirrhosis.
MATERIALS AND METHODS
This was a prospective as well as retrospective multicenter observational study to evaluate practices in management of liver cirrhosis. Study was conducted at five tertiary care gastroenterology centers from Western and Central India, of these 5 centers, two centers were academic centers while three were private practice based centers. All patients with liver cirrhosis attending these centers from 1st January, 2013 to 31st March, 2013 were included in the study. Diagnosis of cirrhosis was based on clinical, biochemical, endoscopic, imaging findings as well as histological evidence of cirrhosis. A comprehensive protocol was written, taking into account various practice guidelines. Protocol included baseline evaluation of patients with cirrhosis with complete hemogram, liver and renal biochemistries, coagulation profile including prothrombin time and International Normalized Ratio (INR), lipid profile, serum electrolytes, an ultrasound with Doppler evaluation, ascites fluid examination for protein, albumin and cell count, an upper gastro intestinal (GI) endoscopy, electrocardiogram (ECG), 2D echo, assessment of oxygen saturation by pulse oximetry and if required, contrast echocardiography, serum iron studies, viral markers pertaining to hepatitis B virus (HBV) and hepatitis C virus (HCV), human immunodeficiency virus (HIV) status, autoimmune markers if clinically pertinent, vitamin D3 levels and alfa-feto protein. A 6-monthly ultrasound evaluation HCC surveillance was incorporated into the protocol.
Patients were divided into three groups and were assessed for the surveillance practices as follows: Group 1: Patients newly diagnosed as cirrhosis during the study period after setting the protocol. Group 2: Patients previously diagnosed by the study centers, the surveillance practices before the study period were assessed. Group 3: patients diagnosed by centers other than the study centers, their surveillance practices were assessed. Patients diagnosed as cirrhosis previously were included only if they attended the study centers during the study period. All patients diagnosed as cirrhosis previously were subjected to clinical history and physical examination. Their previous records were retrospectively assessed by two physicians for etiological workup, assessment of complications, surveillance for HCC and treatment followed. Newly diagnosed patients were also assessed similarly. Records pertaining to referral doctor, diagnosis, investigations and treatment done prior to presentation at one’s centre were noted in detail. The clinical history, examination, investigations and treatment done at centre were noted in detail (both outpatient and inpatient). Appropriate evaluation for etiology of cirrhosis included history of alcohol consumption, diabetes, obesity, dyslipidemia and screening for HBV and HVC. Patients without history of alcoholism and without evidence of chronic HBV and HCV were evaluated for autoimmune hepatitis. Work up for Wilson’s disease, hemochromatosis, primary biliary cirrhosis (PBC) and primary sclerosing cholangitis (PSC) was done whenever clinically suspected. Patients with cryptogenic cirrhosis were subjected to liver histology if autoimmune liver disease was suspected. In patients previously diagnosed, cirrhosis etiological work up based on the aforementioned factors was classified as adequate or inadequate.
All the patients diagnosed with cirrhosis were advised to undergo upper GI endoscopy; patients with previously diagnosed cirrhosis also were assessed whether they had undergone upper GI endoscopy at the time of diagnosis, irrespective of past history of upper GI bleed. Amongst those with large varices on endoscopy (F2 or F3 grade as per Japanese classification) with or without red wale signs, we assessed the proportion of patients who received non-specific beta blocker or endoscopic variceal ligation as prophylaxis, either primary or secondary. Patients with ascites were subjected to diagnostic ascitic fluid examination including serum ascitic fluid- albumin gradient, cell count. Records of patients previously diagnosed as cirrhosis were checked for ascitic fluid examination reports. Those with ascitic fluid protein < 1 gm/dl were considered to have high risk ascites. We determined antibiotic prophylaxis practices in those with high risk ascites as well as those with a prior history of spontaneous bacterial peritonitis (SBP).
We determined the frequency with which alpha-fetoprotein (AFP) was being done in patients at diagnosis in three groups. Since the patients in group 1 were newly diagnosed as cirrhosis, they were excluded from assessment of being in a surveillance ultrasound program. We determined number of patients in groups 2 and 3 who had been diagnosed as cirrhosis for at least 6 months, and who were receiving regular 6-monthly ultrasound surveillance for HCC. Records of all patients of previously diagnosed cirrhosis were checked for testing for minimal hepatic encephalopathy, cardiovascular status and pulmonary status. Results of all these tests were tabulated in a predetermined proforma. The study protocol was approved by institutional review boards and every patient gave written consent to participate in the study.
Statistical analysis
Numerical data were expressed as median, standard deviation and range (minimum to maximum) and categorical data as counts and percentages. Categorical variables were tested using the chi-square and Fisher’s exact test. Continuous variables with and without normal distribution were compared using Student’s t-test or the Mann-Whitney U test, respectively. P value < 0.05 was considered significant for all statistics.
RESULTS
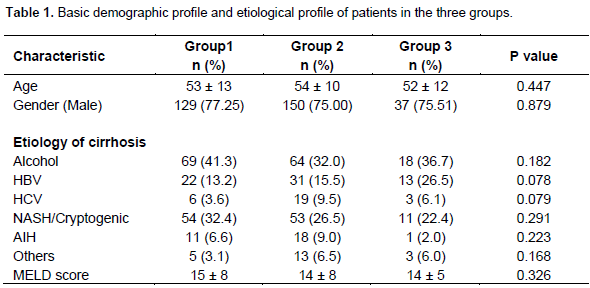
A total of 416 patients, either known cirrhotics or newly diagnosed during the study protocol period were included. Median age of the enrolled patients was 53 years (range: 8 to 91 years). 316 patients (75.96%) were males. Patients were divided into three groups as follows: Group 1: 167 patients. Group 2: 200 patients, Group 3: 49 patients. The three groups were similar in terms of median age (53 vs. 54 vs. 52 years, p value 0.447) and proportion of male patients (77.25, 75 and 75.51%, respectively, p value 0.879). Alcohol was the most common etiology of cirrhosis in the three groups, its prevalence varying from 32 to 41%, the difference being statistically non-significant (p value 0.182). NASH/cryptogenic etiology of cirrhosis were second most prevalent etiology, and exceeded HBV as a cause in groups 1 and 2. In group 3, HBV prevalence was slightly higher than NASH/cryptogenic etiology (26% vs. 22%). However this difference in terms of etiology was non-significant across groups (p values 0.078 and 0.291 for HBV and NASH/cryptogenic, respectively). Prevalence of HCV and AIH was under 10% across groups. PBC, PSC, Wilson disease formed the rest. Thus, all the three groups were similar in terms of etiological profiles. Mean MELD scores were similar in 3 groups (p value 0.326), thereby indicating uniform severity of liver disease in the three groups (Table 1).
Screening for varices at baseline and nonselective beta blocker (NSBB)/endoscopic variceal ligation (EVL) prophylaxis
We assessed screening practices among the three groups (Table 2). Amongst patients diagnosed for the first time as cirrhosis at the study centers, after the protocol was set, 91% (152 of 167) patients were screened for varices irrespective of past history of upper GI bleed in form of hemetemesis or malena. Amongst these, 54 patients had history of upper GI bleed. Thus, of those 113 patients without past history of upper GI bleed, 98 patients (86.72%) underwent screening for varices at dia-gnosis. On the other hand, amongst patients previously diagnosed by us as cirrhosis, only 65% (130/200) had underwent screening for varices at diagnosis while the screening rate was still poor in patients diagnosed at non-study centers as per available records, screening rate in this group being 39% only. The screening rate differences were quite significant amongst groups, clearly suggesting higher screening rates in group 1. Amongst patients who underwent screening for varices, proportion of patients with large varices was around 45, 34 and 68% in the three groups, difference being significant between groups 2 and 3. This difference was probably a bias, as in the group 3 which had the highest percentage of larger varices amongst the screened population, 12 patients of 19 screened had a history of upper GI bleed, thereby increasing the proportion of patients with larger varices in spite of poor screening rate. Amongst the three groups with large varices with or without history of upper GI bleed, proportion of patients receiving non-selective beta blocker or endoscopic variceal ligation as a primary or secondary prophylaxis was 90, 77 and 85%, differences being non-significant across individual groups.

Screening for ascites, ascitic fluid analysis and SBP prophylaxis
All patients diagnosed during the study period underwent ultrasound examination at diagnosis, to determine cirrhosis as well as presence of significant ascites (Table 3). In patients previously diagnosed as cirrhosis either by study centers or non-study centers, we assessed number of patients who had undergone at least two ultrasound examinations, one at diagnosis and other at least 3 month apart to determine ascites. Whereas all patients in group 1 were screened for ascites, only around 75 and 49% patients in groups 2 and 3 underwent screening of ascites (p values 0.001 or less across groups). However this included patients who also had clinical ascites. Amongst patients who were screened, proportion of patients who had significant ascites (grade 2 or 3 ascites by IAC criteria) was 60, 70 and 38% in the three groups, respectively. The difference in proportions was significant between groups 2 and 3 (p value 0.002). Amongst the patients with significant ascites, ascitic fluid analyses was done in 64, 57 and 67% patients, respectively in three groups (p values non-significant across groups). Thus only around 2/3rd of patients across groups underwent ascitic fluid analyses to determine presence of high risk ascites or SBP. Amongst patients in whom ascites fluid analyses was done high risk ascites or evidence of SBP was present in 80, 90 and 100%, respectively in 3 groups. The difference was significant between groups 1 and 3; however the numbers being too small in 3rd group, this could be a bias. Amongst patients with high risk ascites, or evidence of SBP, primary or secondary prophylaxis was given in 94, 60 and 67%. Thus, prophylaxis was given in only 2/3rd patients previously diagnosed by us or non-study centers, whereas after setting the protocol, > 90% patients with high risk ascites/SBP received prophylaxis.

Assessment of renal function at baseline
We evaluated the frequency of assessment of renal function at baseline in patients with cirrhosis in each group at diagnosis, by looking at serum creatinine estimations done at baseline (Table 4). All patients diagnosed as cirrhosis at the study centers during the protocol period underwent serum creatinine estimation. As compared to that, serum creatinine was done in 72 and 81% patients in groups 2 and 3. This differences between group 1, 2 and 3 were statistically significant (p values < 0.001).

Screening for hepatocellular carcinoma
We assessed the frequency with which alpha-fetoprotein was done at point of diagnosis in patients in 3 groups (Table 5). AFP was done in 43, 38 and 6% patients in 3 groups, respectively. The rates were similar at study centers before and after protocol (p value 0.276), but were significantly poor in those diagnosed at non-study centers (p values being < 0.001). In groups 2 and 3, who were already diagnosed as cirrhosis, we assessed number of patients who had been diagnosed as cirrhosis at least 6 months back and were on regular 6 monthly ultrasound evaluation schedules as screening for hepatocellular carcinoma. 126 patients in group 2 and 26 patients in group 3 qualified for screening, of which 53 and 38% patient in each group were receiving 6 monthly ultrasonography (USG) screening for HCC, this difference was not significant (p value 0.075).

Surveillance for hepato-pulmonary syndrome and portopulmonary hypertension
We assessed pulse oximetry screening practice in patients at diagnosis in 3 groups as also echocardiography evaluation in the enrolled patients. 117 patients out of 167 (70%) diagnosed as cirrhosis during the protocol period underwent pulse oximetry evaluation to detect hypoxia, orthodeoxia as markers of HPS. None of the patients in the other two groups had undergone pulse oximetry at diagnosis. However, 185 of these 249 patients of groups 2 and 3 (74.30%) underwent pulse oximetry at study centers during the protocol period. Similarly, echocardiography was done in only 14 patients in group 1 (8%) during the protocol period, whereas none of the patients in other two groups had any echocardiography done at diagnosis. However, 74 of these 249 patients of groups 2 and 3 (30%) had echocardiography evaluation done during the protocol period. As a whole group, we diagnosed 10 patients to be having hepato-pulmonary syndrome on transthoracic contrast enhanced echocardiography.
DISCUSSION
The aim of this study was to determine the actual practices in the care of cirrhotics pertaining to various complications associated with it and the adherence to practice guidelines established by various consortiums in real life scenarios. Accordingly, we designed a protocol incorporating various guidelines apart from the routine investigations and treatment carried out in a patient diagnosed as cirrhosis. The protocol was available to all the study investigators. Of the 416 patients enrolled in the study, 167 were diagnosed as having cirrhosis for the first time during the protocol period. We made an attempt to investigate, treat and care for these 167 patients with adherence to protocol as much as possible. We compared these practices, with what we had been previously doing at the study centers in 200 patients previously diagnosed by the study investigators as well in 49 patients who were being treated at non-study centers in the past and now had presented to the study center for further management. The three groups were similar in terms of demographics like age, gender as well as etiology and severity of underlying cirrhosis.
About 30 to 40% of patients with compensated cirrhosis and 60 to 80% of those with decompensation have esophageal varices, and evidence suggests that about a third of those with documented esophageal varices bleed within a period of 2 years from diagnosis (Fogel et al., 1982; Lo et al., 2001). Incidence of newly diagnosed varices is around 5% per year, while incidence of increase in size of the varices is in the order of 10 to 15% a year. Bleeding from esophageal varices is unpredictable and carries a mortality of 20 to 40% with each bleeding episode (Fogel et al., 1982; Lo et al., 2001). It is known that the complications of portal hypertension do not occur below a HVPG of 10 mm Hg, the risk of variceal bleed is higher when the portal pressure gradient is above 12 mm Hg, and that the goal of treatment of portal hypertension is to reduce below 12 mm Hg. Meta-analyses of various studies have shown that nonselective β-blocker (NSBB) and endoscopic variceal ligation (EVL) are effective as primary and secondary prophylactic therapies to prevent variceal bleeds. However, imparting primary prophylaxis in unselected cirrhotic patients has failed to show any benefit in reducing first bleeds. And hence, endoscopic surveillance of varices to determine their presence, size and red wale signs carries an immense importance to select patients who merit prophylaxis. In our study, > 90% of patients diagnosed as cirrhosis for the first time underwent endoscopy screening while only 65 and 40% of patients diagnosed previously at the study centers or non-study centers had such a screening done. It has been shown that despite evidence based guidelines, only 6 to 22% of patients with large esophageal varices receive primary prophylaxis with NSBBs (Wilbur et al., 2005). In our study, around 90% of patients in group 1 who deserved prophylaxis received either NSBBs or EVL as primary or secondary prophylaxis, which was statistically not different from those in groups 2 and 3 where 77 and 85% deserving patients received any kind of prophylaxis.
Like esophageal varices, presence of ascites in cirrhosis signifies significant portal hypertension. Ascites in cirrhosis is predominantly high risk with low albumin and protein content and carries an inherent risk of spontaneous bacterial peritonitis which is indeed most common type of bacterial infection in hospitalized cirrhotic patients associated with chance of hepatorenal syndrome and subsequent high mortality. Data from a randomized double blind control trial suggests that in a patient with low concentration of ascites protein (< 1 gm/dl) and significant liver disease, primary prophylaxis should be imparted to lower the incidence of first episode of SBP (Fernández et al., 2007). Secondary prophylaxis has to be imparted in those with a previous history of SBP. Kanwal et al. (2012) have shown that for 5 of 8 quality indicators of ascites care (pertaining to abdominal paracentesis at diagnosis or index hospitalization, ascitic fluid evaluation, and imparting of primary or secondary prophylaxis), less than two third of patients received recommended care even after accounting for possible justified exceptions (Kanwal et al., 2012).
In our study, ascites screening at baseline was done in all the newly diagnosed patients as compared to around 75 and 50% patients in the other two groups. The rates of detection of high risk ascites were similar in three groups. Whereas around 95% of patients in group 1 who underwent ascitic fluid analysis and did merit prophylaxis received one, only around two-thirds in the other two groups received such a prophylaxis. Thus, ascites scree-ning, ascitic fluid analysis and imparting of prophylaxis was significantly poor in patients previously diagnosed as cirrhosis and these rates significantly improved after writing of the protocol.
Renal dysfunction is quite common in cirrhosis. Patients with ascites have a 1 year and 5 year probabilities of 20 and 40% for development of hepatorenal syndrome (Gines et al., 1993). HRS type 1 carries a very poor prognosis. Renal function can also be secondary to various therapies of cirrhosis like diuretics, antiviral agents for HBV and HCV. Thus evaluation of renal function at baseline periodically is important. All our newly diagnosed patients (100%) had their baseline serum creatinine done as compared to 70 to 80% of patients previously diagnosed.
Around 1 to 6% patients with cirrhosis develop HCC annually (Amarapurkar et al., 2009). Survival is poor in most patients with HCC (5-year survival less than 5%) except in patients in the early stage who receive potentially curative therapy. HCC surveillance has been advocated to detect HCC at an early stage, when critical treatment can be applied. Ultrasonography and alpha-fetoprotein estimation every six months have been advocated as screening tools. However, rates of HCC screening vary 16 to 60%. A recent meta-analysis demonstrated that < 20% of the patients with cirrhosis undergo HCC surveillance and the most common cause of lack of surveillance is the failure of physicians to order it. In a study by Poustchi et al. (2005) to investigate the feasibility of randomized control trial in HCC, > 80% patients refused to be in no surveillance strategy (Poustchi et al., 2005). Thus, patients would definitely like to be in a screening program. In our study, AFP estima-tion was done in 37% patients previously diagnosed by us, which went up to 43% in the protocol driven diagnosed patients, which was still subpar. The screening rate was a paltry 6% in patients diagnosed at non-study centers. Around 50% of our previously diagnosed pa-tients were in a regular 6 monthly ultrasound surveillance program as compared to 38% of those at non study centers.
Hepato-pulmonary syndrome and portopulmonary hypertension are unique pulmonary complications of cirrhosis. Most patients with hepato-pulmonary syndrome have cirrhosis with varying degrees of portal hypertension. A prevalence of HPS of around 10 to 20% has been reported in cirrhotics listed for liver trans-plantation. However, there is no clear relation between HPS and degree of hepatic dysfunction and it should be suspected independently of the stage of liver disease. There are no symptoms or signs pathognomonic of HPS and indeed many patients with HPS may be completely asymptomatic. Once established, there is a progressive deterioration of arterial oxygenation even in a setting of stable liver disease. Diagnosis of HPS is also associated with high mortality. Similarly, portopulmonary hyperten-sion, though a rare complication of portal hypertension, carries a dreadful prognosis. Transthoracic echo-cardiography (contrast enhanced for HPS) is the most important screening test to diagnose above pulmonary complications (Grace and Angus, 2013; Porres-Aguilar et al., 2013). However; these entities are commonly neglected in daily clinical practice. In our study, none of the patients previously diagnosed at study centers or non-study centers had undergone pulse oximetry or transthoracic echocardiography at diagnosis. Though we could achieve pulse oximetry screening in almost 70% of our newly diagnosed patients, we still could do echocardiography in a minuscule percentage of patients.
Our study had certain limitations. First, the 3rd group of our study had too few a patients as compared to the other two groups. This could have affected few statistical results. Secondly, this was a short term study for a period of three months, during which all those involved in the care of the patients were sensitized to the new protocol. However, long term adherence to the protocol has not been studied. Thirdly, the effect of new protocol on the long term survival benefit of the patients was not studied.
Thus, we conclude that in spite availability of guide-lines, surveillance practices for various complications of cirrhosis are not adequately followed in real life clinical practice, even at tertiary care centers. Presence of a dedicated protocol based on these guidelines definitely helped us improve our surveillance strategies. Compliance with guidelines would definitely help us to take better care of our patients.
CONCLUSION
The author declared he has no conflict of interest.
REFERENCES
|
Amarapurkar AD, Amarapurkar DN, Vibhav Patel ND (2007). Angiogenesis in chronic liver disease Annals Hepatol. 6:170- 173. Pubmed |
||||
| Amarapurkar D (2012). Clinical Care of patients with Cirrhosis. ESCAB Clinical Updates: Gastroenterolgy and Hepatology pp. 104-26. | ||||
|
Amarapurkar DN, Han KH, Chan HLY, Ueno Y (2009). Application of Surveillance Programs For Hepatocellular Carcinoma in the Asia Paciï¬c Region. J. Gastroenterol. Hepatol. 24:955–61 Crossref |
||||
|
Amin MA, Sabry D, Rashed LA, Aref WM, el-Ghobary MA, Farhan MS, Fouad HA, Youssef YA (2013). Short-term evaluation of autologous transplantation of bone marrow-derived mesenchymal stem cells in patients with cirrhosis: Egyptian study. Clin. Transplant. 27(4):607- 12. Crossref |
||||
|
Asia Pacific Working Party on Prevention of Hepatocellular Carcinoma (2010). Prevention of hepatocellular carcinoma in the Asia-Pacific region: consensus statements. J. Gastroenterol. Hepatol. 25:657-663 Crossref |
||||
|
Bosch J, Bergiotti A, Garcia Pagan JC, Abraldes JG (2008). The management of portal hypertension; rational basis, available treatment and future options. J. Hepatol. Suppl 1:S68-92. Crossref |
||||
|
Bruix J, Sherman M (2011). American Association for the Study of Liver Diseases. Management of hepatocellular carcinoma: an update. Hepatology 53:1020-2. Crossref |
||||
| D’Amico G (2001). Natural history of compensated chirrosis and varices. In: TD Boyer & RK Groszmann (eds.), Complications of cirrhosis: pathogenesis, consequences and therapy. AASLD, Dallas. pp. 118-23, | ||||
|
European Association for the Study of the Liver. EASL (2010). Clinical practice guidelines on the management of ascites, spontaneous bacterial peritonitis, and hepato-renal syndrome in cirrhosis. J. Hepatol. 53:397–417 Crossref |
||||
|
Fogel MR, Knauer CM, Andres LL, Mahal AS, Stein DE, Kemeny MJ, Rinki MM, Walker JE, Siegmund D, Gregory PB (1982). Continuous intravenous vasopressin in active upper gastrointestinal bleeding. Ann. Intern. Med. 96:565-9. Crossref |
||||
|
Garcia-Tsao G, Bosch J (2010). Management of varices and variceal hemorrhage in cirrhosis. N. Engl. J. Med. 362:823–832 Crossref |
||||
|
Garcia-Tsao G, Friedman S, Iredale J, Pinzani M (2010). Now there are many (stages) where before there was one: In search of a Pathophysiological classification of cirrhosis. Hepatology 51:1445- 1449. Crossref |
||||
|
Garcia-Tsao G, Lim J, (2009). Management and treatment of patients with cirrhosis and portal hypertension: recommendations from the Department of Veterans Affairs Hepatitis C Resource Center Program and the National Hepatitis C Program. Am. J. Gastroenterol. 104:1802–1829 Crossref |
||||
| Garciaâ€Tsao G, Sanyal AJ, Grace ND, Carey W (2007). Prevention and management of gastroesophageal varices and variceal hemorrhage Gastroenterol. 16:149-58. | ||||
|
Ginès A, Escorsell A, Ginès P, Saló J, Jiménez W, Inglada L, Navasa M, Clària J, Rimola A, Arroyo V (1993). Incidence, predictive factors, and prognosis of hepatorenal syndrome in cirrhosis. Gastroenterology 105:229–36 Pubmed |
||||
|
Grace JA, Angus PW (2013). Hepatopulmonary syndrome: update on recent advances in pathophysiology, investigation, and treatment. J. Gastroenterol. Hepatol. 28:213-9. Crossref |
||||
|
Kanwal F, Kramer JR, Buchanan P, Asch SM, Assioun Y, Bacon BR, Li J, El-Serag HB (2012). The Quality of Care Provided to Patients With Cirrhosis and Ascites in the Department of Veterans Affairs. Gastroenterology 143:70–77 Crossref |
||||
|
Lo GH, Lai KH, Cheng JS, Chen MH, Chiang HT (2001). A prospective, randomized trial of butyl cyanoacrylate injection versus band ligation in the management of bleeding gastric varices. Hepatology 33(5):1060-4. Crossref |
||||
|
Mellinger JL, Volk ML (2013). Multidisciplinary management of patients with cirrhosis: a need for care coordination. Clin. Gastroenterol. 11(3):217-23. Crossref |
||||
|
O'Brien J, Triantos C, Burroughs AK (2013). Management of varices in patients with cirrhosis. Nat. Rev. Gastroenterol. Hepatol. In press. Crossref |
||||
|
Omata M, Lesmana LA, Tateishi R, Chen PJ, Lin SM, Yoshida H, Kudo M, Lee JM, Choi BI, Poon RT, Shiina S, Cheng AL, Jia JD, Obi S, Han KH, Jafri W, Chow P, Lim SG, Chawla YK, Budihusodo U, Gani RA, Lesmana CR, Putranto TA, Liaw YF, Sarin SK (2010). Asian Pacific Association for the Study of the Liver consensus recommendations on hepatocellular carcinoma. Hepatol. Int. 4:439- 74. Crossref |
||||
|
Porres-Aguilar M, Duarte-Rojo A, Krowka MJ (2013). Transthoracic echocardiography screening for the detection of portopulmonary hypertension: A work in progress. Liver Transplant. 19:573-4. Crossref |
||||
| Poustchi H, George J, Labio ED, Coverdale SA, Carney RG, Perry JF, et al. (2005). Screening for liver cancer: feasibility of a randomized controlled trial. Hepatology 42:376A | ||||
|
Runyon BA (2013). Management of adult patients with ascites due to cirrhosis: update 2012. Hepatology 57:1651-3. Crossref |
||||
|
Schuppan D, Afdhal NH (2008). Liver cirrhosis. Lancet 371:838-51 Crossref |
||||
|
Jansen PL (2002). Liver disease in the elderly. Best Pract. Res. Clin. 16: 149–158. Crossref |
||||
|
Tsochatzis EA, Bosch J, Burroughs AK (2012). New therapeutic paradigm for patients with cirrhosis. Hepatology 56:1983-92. Crossref |
||||
|
Wilbur K, Sidhu K (2005). Beta blocker prophylaxis for patients with variceal hemorrhage. J. Clin. Gastroenterol. 39(5):435-40. Crossref |
||||
|
Williams R (2006). Global challenges in liver disease. Hepatology 44:521-526. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


