Full Length Research Paper

ABSTRACT
This study aims to determine the prevalence of asthma, wheeze and dry nocturnal cough, and also to assess predictors of these health outcomes among adolescents from nine different geographic regions in the United Arab Emirates (UAE). Guided by the population health framework, analysis focused on responses to select items from a survey that was administered on 6,363 UAE adolescents. Frequency analyses determined the prevalence of health outcomes and explanatory variables. Bivariate analyses assessed associations between each outcome and all explanatory variables. Logistic regression models were used to identify significant predictors of asthma, wheeze, and dry nocturnal cough for each geographic region. The prevalence of asthma, wheeze, and dry nocturnal cough ranged from 7.0 to 16.9%, 9.3 to 14.8% and 30.4 to 48.2% respectively. Associations between health outcomes and explanatory variables vary across regions. Results of multivariate regression modeling identified significant predictors of the respiratory conditions, which varied across regions. The prevalence proportions of respiratory symptoms and particularly dry nocturnal cough are relatively high in the UAE. Predictors of respiratory health in the UAE differ across regions and may be closely tied to the regional physical and social environments, which are linked to individual behaviors and lifestyles.
Key words: Air quality, respiratory health, asthma, health determinants, adolescents, population health, United Arab Emirates.
INTRODUCTION
Respiratory diseases are among the leading causes of death worldwide (World Health Organization, 2015). This is concerning given that many chronic respiratory conditions that affect millions of people worldwide are preventable (Lopez, 2006; Masoli et al., 2004). Research documents that chronic respiratory conditions are also associated with poor health status and greater work disability (Eisner, 2001). Preventable chronic respiratory conditions include chronic obstructive pulmonary disease (COPD) and asthma (World Health Organization website). COPD is used to describe chronic lung diseases that cause limitations in lung airflow such as chronic bronchitis or emphysema. In 2012, COPD was the third leading cause of global deaths, accounting for 3.1 million deaths (World Health Organization, 2015). Asthma is the most common non-communicable disease among children, characterized by recurrent attacks of breathlessness and wheezing (Islam et al., 2007; World Health Organization, 2003).
Asthma is usually triggered from inflammation of the airway that tightens the surrounding muscle, narrowing or restricting airflow. Persistent respiratory symptoms are generally used to suggest the presence of acute respiratory conditions. For example, recurrent symptoms of wheezing, cough, difficulty breathing, and chest tightness may be signals of asthma presence in children (Lai et al., 2009; Chung and Pavord, 2008). An estimated 235 million people across the globe suffer from asthma (World Health Organization Fact Sheet 307, 2013). The fundamental causes of asthma are not completely understood. Current evidence suggests that the strongest risk factors for developing asthma are genetic predisposition and environmental exposures to inhaled pollutants that interfere with the airways (World Health Organization Fact Sheet 307, 2013). Moreover, research findings suggest that asthma diagnosis is a significant risk factor for COPD raising the level of risk by a factor of 12 (Silva et al., 2004). Therefore, identifying significant predictors of asthma and respiratory symptoms such as wheeze and dry nocturnal cough is a preliminary step for prevention, which has the potential to decrease the global mortality and morbidity burden of respiratory diseases.
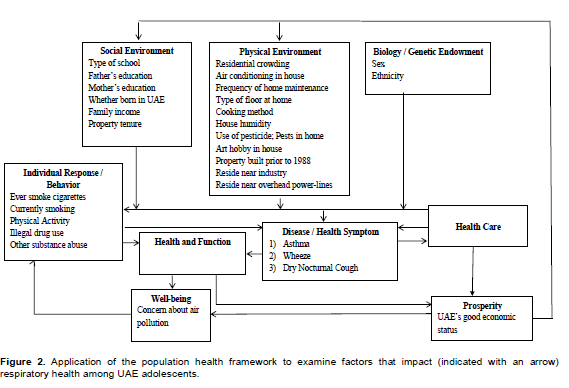
The population health framework can be a useful tool for examining disease health determinants (Evans and Stoddart, 1990). The framework highlights ways in which different types of factors and forces interact to impact different conceptualizations of health. Possible health determinants relate to the physical environment, social environment, biology or genetic endowment, individual responses or behaviors to a particular disease, accessibility to healthcare, well-being, and prosperity. In relation to asthma and respiratory symptoms, several physical environmental factors have been shown to strongly correlate to these health outcomes; these include exposures to allergens, air pollutants, and other environmental chemicals (Kelly and Fussell, 2011). For instance, low levels of air quality due to traffic pollution or high ozone levels have been associated with both asthma development and increased asthma severity (Esposito et al., 2014; NRDC, 2014). In addition, asthma is associated with exposure to indoor allergens including dust mites, cockroaches, animal dander and mold (Bush, 2008; Arshad, 2009). There is also strong evidence linking parental smoking with asthma in children (Pattenden, 2006; Cook and Strachan, 1999).
Research suggests that the social environment, such as socioeconomic status, also plays a role in increasing the risk for developing respiratory conditions (Gorman and Asaithambi, 2008). For instance, significant associations were documented between low education and each diagnosis with asthma and wheeze (Arif et al., 2003; Litonjua et al., 1999). Furthermore, research documents show negative associations between income and asthma prevalence (Gwynn, 2004; Rona, 2000). In relation to biology, sex and ethnic variations in respiratory health are most commonly studied by researchers. Although, most research documents show higher prevalence rates of asthma and wheeze among male children compared to female children (Wieringa et al., 1999), there appears to be an increase in susceptibility for asthma in ‘post-pubescent’ girls and women (Balzano et al., 2008). Ethnic variations in asthma diagnosis have been reported in various countries. For example, in the US, asthma rates are higher among Native Americans (11.6%) and African Americans (9.4%), followed by Caucasians (7.6%), Hispanics (5.0%), Asians (2.9%), and Hawaiian Pacific Islanders (1.3%) (Gorman et al., 2008; CDC, 2004). Individual behavior choices are also important in determining respiratory health, influencing the risk of developing asthma and respiratory conditions. Indeed, research show significant associations between tobacco use and asthma diagnosis (Al-Sheyab et al., 2014; Mcleish and Zvolensky, 2010).
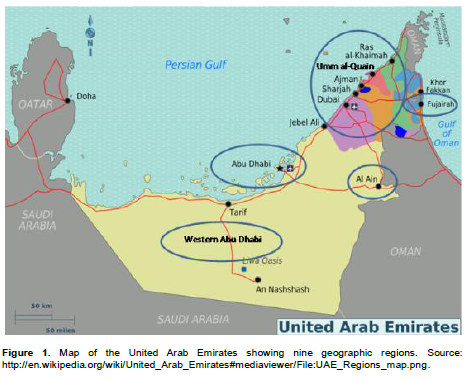
Health determinants that relate to many diseases are place-specific. This is particularly true for asthma and respiratory conditions, which are influenced by regional physical and social factors such as geographic features, anthropogenic activities that occur in particular places, and exposures to risk factors. Situated in the Arabian Gulf peninsula, the United Arab Emirates (UAE) is a federation that is undergoing fast-paced development characterized by heavy construction, demographic shifts, and changes to the social and physical landscapes. It consists of seven Emirates: Abu Dhabi, Dubai, Sharjah, Ajman, Umm al-Quain (UAQ), Ras al-Khaimah (RAK), and Fujairah (Figure 1). The Emirate of Abu Dhabi accounts for 87 percent of the geographic area and consists of three geographical regions. Abu Dhabi City is the largest by area and relies largely on oil production (UAE Ministry of Environment, 2005). The Western region of Abu Dhabi exhibits mixed development dependent on agriculture and industry, while Al-Ain in Abu Dhabi has many oases and parks. The second largest emirate, the Emirate of Dubai, is located in emirate's northern coastline. Unlike Abu Dhabi city, Dubai is a growing metropolis with main revenues coming from tourism, real estate and financial services. Sharjah relies on tourism largely due to its rich and cultural place in the Arab region. Ajman experienced development in the construction industry, but remains less populous than Dubai and Sharjah. UAQ relies on agriculture, fisheries and tourism, while RAK and Fujairah are dependent on the industrial sector and agriculture respectively.
Although, economic growth and development in the UAE have improved the living conditions of its people, they may also have increased respiratory health risk levels (Khondker, 2009). For example, studies have suggested that air pollutants in Sharjah include carcinogens and are at concentrations similar to or exceeding those in Beijing and Mexico City (The National, 2014). In fact, research suggests that many pollutants in the UAE may be at levels above the standards (The National, 2014). These findings couple with research and other documents reports high prevalence rates of asthma and cardiovascular diseases, which are the leading causes of overall death in the UAE (Al-Maskari et al., 2000).
Adolescence is an important time period in a person’s lifestyle, where exposures that impact respiratory health range from those that are related to the physical and social environments, to those result from individual choices and behaviors. Furthermore, behavioral factors that impact health during adolescents tend to remain and solidify in adulthood, while at the same time, health outcomes that affect respiratory health in adolescence may lead to longer-term new health outcomes. Very few studies have explored the prevalence and risk factors of respiratory conditions among adolescents in the UAE or neighboring countries. Implementation of the International Study of Asthma and Atopy in Children (ISAAC) in countries neighboring the UAE, suggest that the prevalence of asthma among adolescents is between 5 to 10%, of wheeze between 6 to 11%, and below 20% for dry nocturnal cough (ISAAC, 1998; Pearce et al., 2007). Results from worldwide implementation of the ISAAC questionnaire on adolescents reveal geographic variations in the prevalence of asthma ranging between 4.4 and 25.9%, of wheeze past 12 months ranging between 6.0 and 29.9%, and between 12.2 and 33.7% for night cough within the past 12 months. The total global prevalence of these three outcomes is 11.3%, 13.8 and 22.3% respectively (ISAAC, 1998). Barakat-Haddad et al. (2014), embarked on a research project that examined the respiratory health profile among adolescents from the UAE and the possible link with air quality, at the national scale. Results suggest that the prevalence of chronic bronchitis, emphysema, asthma, wheeze, and dry cough among UAE adolescents is 1.8, 0.5, 12.3, 12.2 and 34.8% respectively (paper submitted). While the prevalence of wheeze appears to be below the global prevalence, both the prevalence of asthma and dry cough are relatively higher. Results of this recent study also suggest that significant predictors of respiratory health among adolescents from the UAE include outdoor and indoor air quality, as well as behavioral factors related to smoking and drug use.
While these results were novel, variations in the physical and social landscapes of geographic regions within the UAE suggest that analysis at a regional scale can better inform prevention efforts, by focusing on assessing regional predictors of respiratory health. To that extent, and guided by the population health framework, this research addresses three main objectives: to determine the prevalence of asthma, wheeze, and dry nocturnal cough among adolescents from each of nine different regions in the UAE; to examine associations between respiratory health and each of social and physical factors in relation to the nine different regions in the UAE; to assess differences in the predictors of each asthma, wheeze and dry nocturnal cough among the UAE adolescent population in relation to the nine geographic regions in the UAE.
METHODOLOGY
Data source
The National Study of Population Health in the UAE (NSPHUAE) (2007 to 2009) research program consisted of developing and administering a cross-sectional survey on 6,363 adolescents age between 13 and 20 years, and who attend schools in nine different geographic regions in the UAE; that is Abu Dhabi city, Al Ain (Abu Dhabi), Western region (Abu Dhabi), Ajman, Dubai, UAQ, RAK, Sharjah, Fujairah (Figure 1). Survey details are described in Barakat-Haddad (2013). Guided by the population health framework, this research utilizes data from the NSPHUAE that relates to health measures, demographics, lifestyle, residential and neighborhood characteristics (Figure 2).
Outcome variables
Outcome variables were based on responses to three items adopted from the ISAAC. Participants were asked if they were ever diagnosed with asthma by a doctor or health care professional, if they experienced wheezing or whistling in the chest in the last 12 months, and if they had a dry cough at night, apart from a cough associated with a cold or chest infection in the last 12 months.
Explanatory variables
Guided by the population health framework, the physical environment was characterized using variables that relate to indoor and outdoor air quality (Figure 2). These include responses to questions on whether the residence has air conditioning, how often the residence is maintained, the type of flooring in the main living area of the residence, the type of cooking method, whether the residence feels humid, whether the residence is subject to regular use of pesticides or insecticides, whether there are pests seen in the past 12 months, whether anyone in the participants’ household does arts, crafts, ceramics, stained glass work or similar hobbies on a regular basis, whether the property of residence was built prior to 1988. These variables are known to influence indoor air quality due to the presence of possible toxins such as dust of silica and lead, and would further increase the risks of respiratory symptoms. Factors influencing outdoor air quality include whether participants reside near industrial plants, gas stations, dumpsites, or construction sites; whether participants reside near overhead power lines or plants; and residential crowding. The latter was calculated using the ratio for the number of individuals who reside in the household over the number of bedrooms in the residence.
Variables related to the social environment include type of school attended, father’s education, mother’s education, whether the participant was born in the UAE, monthly family income and residential property tenure. Variables related to biology or genetic endowment includes sex and ethnicity. The latter was classified on the basis of similar cultures, traditions, ancestral linkages or geographical origins. Data related to individual responses and behaviors include ever smoking cigarettes or any form of tobacco such as shisha or midwakh, and whether it was on an occasionally or daily basis for the past 30 days. Participants were categorized as current smokers if they reported occasional or daily use of at least one form of tobacco in the past 30 days. This categorization is consistent with WHO guidelines. The participants were asked series of questions: whether they participated in any number of physical activities in the past 12 months. Other variables include responses to questions on whether participants ever used illegal drugs such as marijuana, hashish, or cocaine; and whether they ever purposely smelled gasoline fumes, glue, correctors, car exhaust, or burning black ants. Reports suggest that UAE adolescents tend to purposely smelled gasoline fumes, glue, correctors, car exhaust, or burning black ants for recreational purpose, the latter are described as ‘other substance abuse’ throughout this paper, and are common knowledge among the UAE adolescent population. Well-being is characterized using responses to whether participants are concerned about air pollution in their neighborhood. Living conditions in the UAE are characterized by good health coverage and relative prosperity and hence these domains were not included in the analysis.
Statistical analysis
Data were analyzed using statistical package for social sciences (SPSSv20) using descriptive statistics for all outcome and explanatory variables. To address the second research goal, the Chi-square statistic was used for bivariate analyses that assessed associations between each outcome and all explanatory variables for each of the nine geographic regions. After discovering the correlation between outcome variables and explanatory variables, all va riables that were significant in the bivariate analyses were entered into logistic regression models in order to identify significant predictors of respiratory conditions and symptoms. For each of the health outcomes, multivariate analysis was performed in order to identify significant predictor of those specific health outcomes in relation to each geographic region. Logistic regression was used by entering all explanatory variables that were significant in the bivariate analyses for each of the geographic regions separately. For each of the modeled outcomes, direct entry of explanatory variables was conducted using a significance level of p≤0.05.
RESULTS
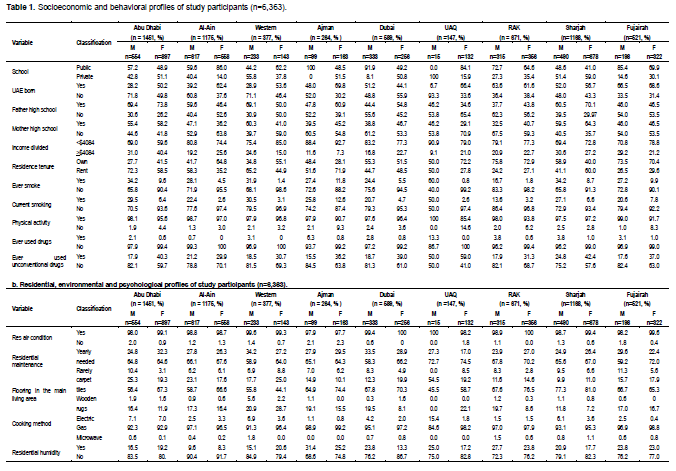
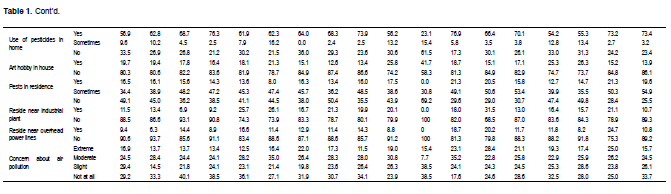
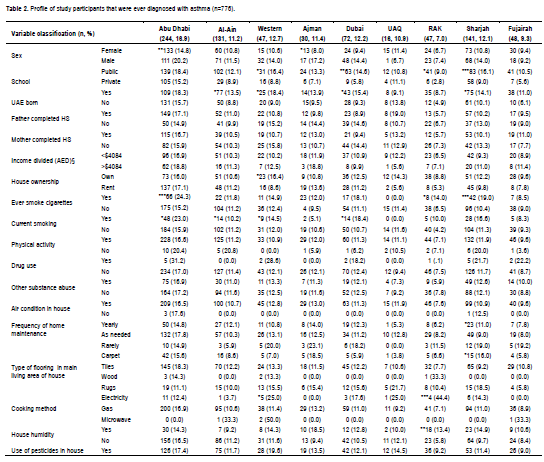
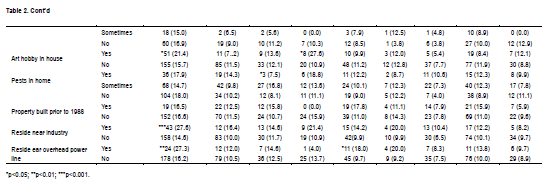
This paper is based on responses from 6,363 adolescents with a mean age of 16 years old, which is a representative sample for our study. Majority of participants reside in Abu Dhabi city (n=1451, 22.8%), Al Ain (n=1175, 18.5%), and Sharjah (n=1168, 18.4%). Table 1a summarizes the socio-demographic and behavioral profiles, whereas Table 1b includes residential, environmental, and psychosocial profiles of the study participants. Overall, 50% of participants in this study are of local national origin and 45% of participants are male. These results suggest that our sample is representative of the UAE population for this age category. For all regions except Sharjah, a higher proportion of participant attend public school. A higher proportion of participants across nine regions report a family annual income less than AED15,000 dirhams ($4,087US) compared to a family annual income of at least AED15,000 dirhams. For all nine regions, males have a higher prevalence of current smoking, ever smoke, physical activities, and drug use whereas female participants have a higher prevalence of other substance abuse (Table 1a).
In relation to the physical environment, for all nine regions, a higher proportion of participants have air conditioning in their home, maintain their residence as needed, use ceramic tiles as floors in main living areas and cook with gas (Table 1b). Except for UAQ, the majority of participants report that they have seen pests at home in the past 12 months, as well as regular use of pesticides or insecticides. Compared to other regions, more participants from the western region of Abu Dhabi report living near industrial plant, gas stations, dumpsites, or construction sites.
In terms of our second research goal, we found that explanatory variables differ in the association with outcome variables within different regions. Variability in the prevalence of respiratory outcomes is apparent with the prevalence of asthma, wheeze, and dry nocturnal cough ranging from 7.0 to 16.9%, 9.3 to 14.8% and 30.4 to 48.2% respectively. For the Western region, Dubai, and Sharjah, bivariate analyses suggest that asthma is significantly associated with the type of school attended and whether participants were born in the UAE. Smoking emerges as a significant variable for most geographic regions except for Ajman, UAQ, and Fujairah. A number of significant associations are found between proxies of indoor air quality, as well as outdoor air quality, and asthma for all nine regions except UAQ and Fujairah (Table 2).
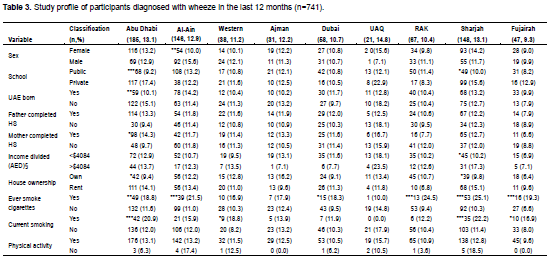
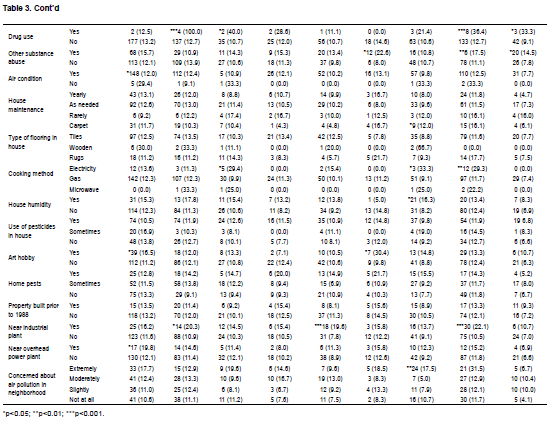
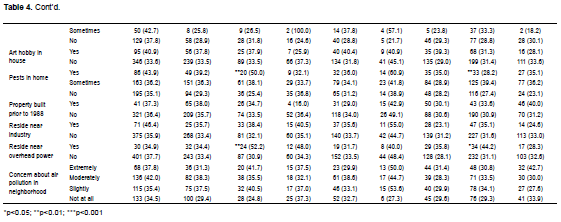
For wheeze in the last 12 months, smoking and other substance abuse are significantly associated with wheeze across all geographic regions except Dubai (Table 3). Residing near industry is associated with wheeze in Dubai and Sharjah, whereas residing near over-head power plants, type of school attended, and whether born in UAE are associated with wheeze in Abu Dhabi. Sex and other substance abuse are significantly associated with dry nocturnal cough in Abu Dhabi, Al-Ain, Sharjah and Fujairah. Proxies of indoor air quality are associated with cough, and residing near overhead power-linesis associated with dry nocturnal cough in the Western regions of Abu Dhabi and Sharjah (Table 4).

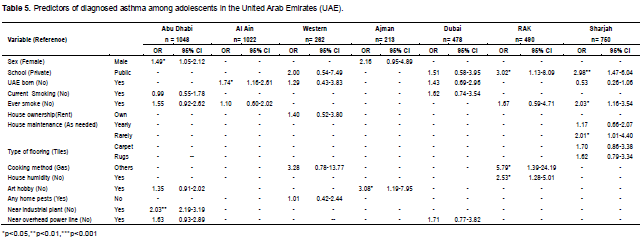
Age, ethnicity, residential crowding, and whether the property of residence was built prior to 1988, are not statistically significant with any respiratory conditions in any regions and therefore are excluded from this paper. After assessing bivariate associations, results of multivariate regression modeling suggested that predictors of respiratory health outcomes vary across regions. Table 5 shows that among demographic factors, sex is a significant predictor of asthma in Abu Dhabi, while the type of school attended is a significant predictor of asthma in RAK and Sharjah, and born in the UAE significantly predicts asthma in Al-Ain and Dubai. Ever smoking is a predictor of asthma in Sharjah, and those who rarely maintain their house are twice more likely to develop asthma compared to those who maintain their house as needed. In RAK, people who tend to use electricity or microwave as their cooking methods, and those who feel that their house is humid, are more likely to develop asthma. Having someone in the household who is regularly involved in arts, crafts, ceramics, stained glass work and similar hobby work is a predictor of asthma in Ajman. Lastly, residing near industrial plant, gas station, dumpsite, or construction sites is a predictor of asthma in Abu Dhabi.
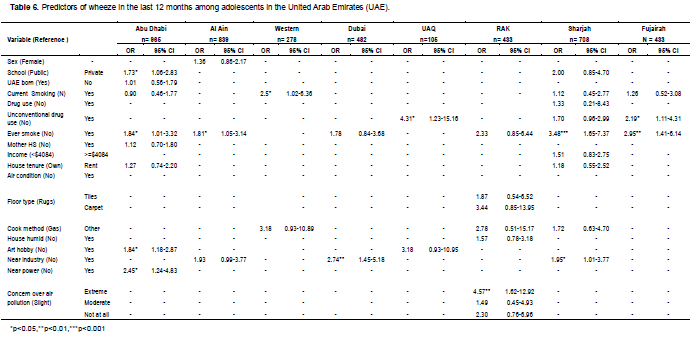
The type of school attended is a significant predictor of wheeze in Abu Dhabi, with those who attend private school are more likely to experience wheeze than students who attend public schools (Table 6). Current smoking is a significant predictor of wheeze in the Western region, while other substance abuse is a significant predictor in UAQ and Fujairah. Ever smoking is a significant predictor of wheeze in Abu Dhabi, Al-Ain, Sharjah and Fujairah. Having someone in the household who is regularly involved in arts, crafts, ceramics, stained glass work and similar hobby work are predictors of wheeze in Abu Dhabi. Lastly, participants who reside near an industrial plant in Dubai or Sharjah, and those who reside near an overhead power-line in Abu Dhabi are more likely to experience wheeze in the past 12 months. Extreme concern over air pollution is a significant predictor of wheeze in RAK.
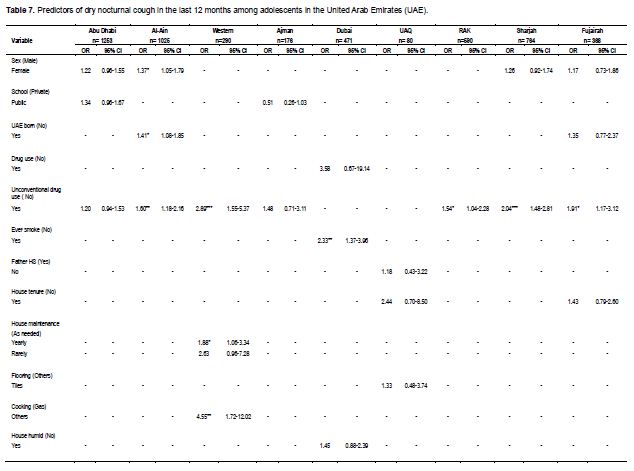
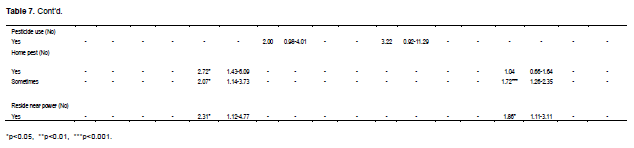
Being female and being born in the UAE are predictors of dry nocturnal cough in Al-Ain (Table 7). Other substance abuse is a consistent predictor of experiencing dry nocturnal cough across different regions including AlAin, Western, RAK, Sharjah and Fujairah. Ever smoking is a predictor of dry nocturnal cough in Dubai. In terms of proxies of indoor air quality, results suggest that those who maintain their house yearly are more likely to experience cough than those who maintain it when needed, in the Western region. Participants who use gas as their main cooking method at home are less likely to experience cough in the past 12 months. The presence of home pests is a predictor of cough in Western and Sharjah region. Lastly, residing near industrial plants, gas station, dumpsite, or construction sites is a predictor of cough in the Western and Sharjah region (Table 7).
DISCUSSION
Variations in the prevalence of asthma and wheeze in the nine regions in the UAE are in accordance with global estimates (7 to 16.9% versus 11.3 and 9.3% to 14.8% versus 13.8% respectively), while the prevalence of dry nocturnal cough in the UAE is much higher (30.4 to 48.2% versus 22.3%) (UAE Ministry of Environment, 2005).
Our results suggest that physical environments in the UAE play a role in the prevalence of respiratory health for UAE adolescents. Residing in proximity to industrial plants, gas station, dumpsite, or construction sites, as well as residing in proximity to overhead power-lines are associated with the respiratory health of adolescents in at least one region in the UAE. This is not surprising given that air quality has been linked to respiratory health (World Health Organization Fact sheet 307; Kelly and Fussell, 2011; Esposito et al., 2014). For instance, adolescents from RAK and Fujairah are less likely to report asthma (7.0 and 9.3% respectively) than those from Abu Dhabi and Western region (16.9 and 12.7%). Essentially, Abu Dhabi and the Western regions such as Al Ruwais primarily generate their income through oil and gas industries, which are contributors of air pollution (Al-Maskari, 2000; The National, 2013), while RAK and Fujairah rely more on agriculture and fisheries. Exposures to arts, crafts, ceramics, stained glass work and similar hobbies are associated with respiratory health in Abu Dhabi, Ajman and UAQ.
Adolescents who attend public schools in RAK and Sharjah are more likely to have asthma. While this finding may be a reflection of the participants’ socioeconomic status, it may also be indicative of indoor air quality inside public schools. In contrast, we found an association between attending private schools in Abu Dhabi City and wheeze. These inconsistent findings point to the possible need for a wide-scale national campaign that assesses indoor air quality in public and private schools in the UAE. It is interesting to note that sex and being born in the UAE emerge as significant predictors of respiratory health only for participants who reside in the emirate of Abu Dhabi. These findings may be reflective of gender behaviors in Abu Dhabi but are worth further investigations.
In terms of individual responses and behaviors, our study suggests that current or exposure to smoking is associated with respiratory health for most UAE regions. This is not surprising, given that exposure to environmental tobacco is a well-recognized risk factor of asthma and respiratory symptoms (Al-Sheyab et al., 2014; Mcleish and Zvolensky, 2010). These findings highlight the importance of reducing tobacco usage among all adolescents in the UAE. In the UAE, there is zero tolerance for illegal drug use and harsh judicial penalties. Therefore, adolescents often choose to smoke burning ants, which are high in formic acid, as may be perceived as a legal alternative to getting high (The National, 2014).
Building on current knowledge (The National, 2014; Rudell et al., 1996), we found associations between other substance abuse and respiratory health in Al-Ain, Western, RAK, Sharjah and Fujairah. It may be that adolescents residing in these regions are less aware of the potential risk of smoking burning ants, therefore it is important to develop educational campaigns that focus on the consequences and health risks of other substance abuse.
CONCLUSION
This study was subject to several limitations. First, exposure data used in our analyses are proxies of exposure assessments. For instance, air quality was assessed based on proximity to pollution sources rather than on actual exposure assessments. Unfortunately, data on air quality exposure is scarce in the UAE. Second, data were self-reported and may have been subject to response bias.
Sampling led to lower representations of adolescents who attend private schools in Dubai and among males who reside in the UAQ. This is relevant as the population of Dubai consists of a large proportion of expatriates; hence results related to the expatriate population in Dubai are likely to be biased. Finally, response to the self-administered survey may have been influenced by the presence of social workers, with the possibility of under-reporting tobacco use among females given social norms.
Despite these limitations, this study contributed to knowledge of a detailed profile and regional environmental predictors of respiratory health among UAE adolescents that is crucial for public health planning.
ACKNOWLEDGEMENTS
The authors acknowledge the contribution of Dr. Rania Dghaim in the design and data collection phase of the NSPHUAE.
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
REFERENCES
| Al-Maskari F, Bener A, Al-Kaabi A, Al-Suwaidi N, Norman N, Brebner J (2000). Asthma and respiratory symptoms among school children in United Arab Emirates. Allergy Immunol. 32(4):159-63. | ||||
|
Al-Sheyab N, Alomari MA, Shah S, Gallagher P, Gallagher R (2014). Prevalence, Pattern and Correlated of Cigarette Smoking in Male Adolescents in Northern Jordan, and the Influence of Waterpipe Use and Asthma Diagnosis: A Descriptive Cross-Sectional Study. International Journal of Environmental Research and Public Health, 11, 9008 – 9023. crossref |
||||
|
Arif A, Delclos G, Lee E, Tortolero S, Whitehead L (2003). Prevalence and risk factors of asthma and wheezing among US adults: An analysis of the NHANES III data. European Respiratory Journal, 827-833. crossref |
||||
| Arshad S (2009). Does Exposure To Indoor Allergens Contribute To The Development Of Asthma And Allergy? Current Allergy and Asthma Reports, 49-55. | ||||
|
Balzano G, Fuschillo S, Melillo G, Bonini S (2008). Asthma and Sex Hormones.Allergy 56(1):13–20. crossref |
||||
|
Barakat-Haddad C. (2013). Prevalence of High Blood Pressure, Heart Disease, Thalassemia, Sickle-Cell Anemia, and Iron-Deficiency Anemia among the UAE Adolescent Population.Journal of Environmental and Public Health.Article ID 680631, crossref |
||||
|
Bush R (2008). Indoor allergens, environmental avoidance, and allergic respiratory disease. Allergy and Asthma Proceedings, 575-579. crossref |
||||
|
Center for Disease Control (CDC). (2004) Asthma Prevalence and Control Characteristics by Race/Ethnicity—United States, 2002 Morbidity and Mortality Weekly Report 53(07):145–48. Pubmed |
||||
|
Chung K, Pavord I (2008). Prevalence, pathogenesis, and causes of chronic cough. Lancet 371:1364-74. crossref |
||||
|
Cook DG, Strachan DP (1999). Summary of effects of parental smoking on the respiratory health of children and implications for research. Thorax 54:357-66. crossref |
||||
|
Eisner MD, Yelin EH, Trupin L, Blanc PD (2001). The Influence of Chronic Respiratory Conditions on Health Status and Work Disability. Am. J. Public Health 92(9):1506-13. crossref |
||||
|
Esposito S, Tenconi R, Lelii M, Preti V, Nazzari E, Consolo S, Francesca Patria M (2014). Possible molecular mechanisms linking air pollution and asthma in children. BMC Pulmonary Medicine 14:31. crossref |
||||
|
Evans R, Stoddart G. (1990). Producing health, consuming health care. Soc. Sci. Med. 31(12):1347-1363. crossref |
||||
|
Gorman B, Asaithambi R (2008). Biology, Social Environment, and Health: How Family History and Social Conditions Affect Adult Asthma. Social Science Quarterly, 89(3):728-750. crossref |
||||
|
Gwynn R (2004). Risk Factors for Asthma in US Adults: Results from the 2000 Behavioral Risk Factor Surveillance System. J. Asthma 41:91-98. crossref |
||||
|
Islam T, Gauderman WJ, Berhane K, Mcconnell R, Avol E, Peters JM, Gilliland FD (2007). Relationship between air pollution, lung function and asthma in adolescents. Thorax 62(11):957-63. crossref |
||||
|
Kelly FJ, Fussell JC (2011). Air pollution and airway disease. Clin. Exp. allergy 41(8):1059-71. crossref |
||||
| Khondker HH (2009). Social change in the United Arab Emirates: challenges of migration and 'Emiratization'. Middle East Institute, Singapore, Perspectives 001. | ||||
|
Lai CK, Beasley R, Crane J, Foliaki S, Shah J, Weiland S (2009). Global variation in the prevalence and severity of asthma symptoms: phase three of the International Study of Asthma and Allergies in Childhood (ISAAC). Thorax 64(6):476-83. crossref |
||||
|
Litonjua A, Carey V, Weiss S, Gold D (1999). Race, Socioeconomic Factors, And Area Of Residence Are Associated With Asthma Prevalence. Pediatr. Pulmonology 28:394-401. crossref |
||||
|
Lopez AD (2006). Chronic obstructive pulmonary disease: current burden and future projections. Eur. Respir J. 27(2):397-412 crossref |
||||
|
Masoli M, Fabian, D, Holt S, Beasley R (2004). The global burden of asthma: executive summary of the GINA Dissemination Committee Report. Allergy 59(5):469-78. crossref |
||||
|
Mcleish A, Zvolensky M (2010). Asthma and Cigarette Smoking: A Review of the Empirical Literature. J. Asthma, 345-361. crossref |
||||
| Natural Resources Defence Council (NRDC), Asthma and Air Pollution. (2014, January 28). http://www.nrdc.org/health/effects/fasthma.asp | ||||
|
Pattenden S (2006). Parental smoking and children's respiratory health: independent effects of prenatal and postnatal exposure. Tobacco Control 15(4):294-301. crossref |
||||
|
Pearce N, Ait-Khaled N, Beasley R, Mallol J, Keil U, Mitchell E, Robertson C (2007). Worldwide trends in the prevalence of asthma symptoms: Phase III of the International Study of Asthma And Allergies In Childhood (ISAAC). Thorax 62(9):758-766. crossref |
||||
|
Rona RJ (2000). 'Asthma and Poverty.' Thorax 55:239–44. crossref |
||||
|
Rudell B, Ledin, M, Hammarstrom U, Stjernberg N, Lundback B, Sandstrom T (1996). Effects on symptoms and lung function in humans experimentally exposed to diesel exhaust. Occup. Environ. Med. 53:658-62. crossref |
||||
|
Silva GE, Sherrill DL, Guerra S, Barbee RA (2004). Asthma as a Risk factor for COPD in a Longitudinal Study. Chest 126(1):59–65. crossref |
||||
|
The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variations in the prevalence of asthma symptoms: the International Study of Asthma and Allergies in Childhood (ISAAC). Eur. Respiratory J. 12(2):315-335. crossref |
||||
| The National (2013). Air quality master plan to battle pollution in Abu Dhabi, http://www.thenational.ae/uae/environment/air-quality-masterplan-to-battle-pollution-in-abudhabi [accessed 03.03.14] | ||||
| The National (2014a). Air pollution in Sharjah as toxic as in Beijing, survey shows, http://www.thenational.ae/uae/environment/air-pollution-in-sharjah-as-toxic-as-in-beijing-survey-shows [accessed 13.03.14] | ||||
| The National (2014b). What to do with carcinogenic Sharjah smog? http://www.thenational.ae/thenationalconversation/editorial/what-to-do-with-carcinogenic-sharjah-smog [accessed 13.03.14] | ||||
| The National (2014c). Experts call for careful eye to be kept on UAE air pollution levels, http://www.thenational.ae/uae/environment/experts-call-for-careful-eye-to-be-kept-on-uae-air-pollution-levels | ||||
| The National (2014d). UAE: More than a third of youth smoke ants to get high, http://www.edarabia.com/25120/uae-more-than-a-third-of-youth-smoke-ants-to-get-high/; [Accessed 23.04.14]. | ||||
| UAE Ministry of Environment, Tedad Census (2005) Preliminary Results of Population, Housing and Establishment Census 2005, United Arab Emirates, Ministry of Economy, Abu Dhabi, UAE, 2006 .www.cscc.unc.edu.uaee/public/UNLICOMMUAE2005CensusResults07282008.pdf [accessed 30.04.14] | ||||
|
Wieringa MH, Weyler JJ, Van Bever HP, Nelen VJ, Vermeire PA (1999). Gender differences in respiratory, nasal and skin symptoms: 6-7 versus 13-14-year-old children. Acta Paediatr. 88(2):147-9. crossref |
||||
| World Health Organization (2003).Prevention of Allergy and Allergic Asthma.Accessed via http://whqlibdoc.who.int/hq/2003/WHO_NMH_MNC_CRA_03.2.pdf?ua=1 on January 6, 2015. | ||||
| World Health Organization Fact sheet No 307. Asthma. November 2013. Accessed on January 6, 2015 via http://www.who.int/mediacentre/factsheets/fs307/en/ | ||||
| World Health Organization Fact sheet No 310. The Top 10 Causes of Death. May 2014. Accessed on January 6, 2015 via http://www.who.int/mediacentre/factsheets/fs310/en/. | ||||
| World Health Organization. Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach, http://www.who.int/gard/publications/GARD%20Book%202007.pdf?ua=1;2007[accessed02.04.14) | ||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


