Full Length Research Paper

ABSTRACT
There is growing evidence suggesting that young people in school are practicing risky sexual behaviors. Ethiopian people aged 10 to 24 years have emerged as the segments of the population most vulnerable to a broad spectrum of serious sexual health problems. Therefore, the main aim of this study was to assess risky sexual behaviors and associated factors among preparatory school students in Arba Minch, Southern Ethiopia. An institution based cross sectional study was conducted among 465 study participants from April 20 to June 2, 2018. A self-administered pre-tested questionnaire was used to collect the data. Bivariate and multivariate analysis was done using binary logistic regression. In this study, 22.4% (95%CI: 18.6%, 26.2%) of study participants had risky sexual behaviors. Marital status, education and occupational status of the father, occupation of the mother, watching pornographic movies, drinking alcohol, using hashish/shisha and knowledge about HIV/AIDS were significantly associated with odds (AOR=3.28, 95%CI: 1.24, 8.70), (AOR=5.96, 95%CI: 1.35, 26.25), (AOR=0.33, 95%CI: 0.12, 0.93), (AOR=0.22, 95%CI: 0.09, 0.51), (AOR=8.80, 95%CI: 4.04, 19.17), (AOR=2.71, 95%CI: 1.35, 5.46), (AOR=14.88, 95%CI: 4.52, 48.96) and (AOR=2.89, 95%CI: 1.42, 5.88), respectively. This finding noted that significant numbers of students were engaged in risky sexual behaviours. Those students had multiple sexual partners, used condoms inconsistently, had sex with risky individuals, and an early sexual start. Watching pornographic movies, substance abuse and a knowledge gap on HIV/AIDS were some of the significant factors. Awareness creation for youths to reduce substance abuses, HIV/AIDS and sexual and reproductive health in the school community is recommended.
Key words: Risky sexual behaviors, sexual and reproductive health problems, youths
Abbreviation: AIDS, Acquired immune deficiency syndrome; AOR, adjusted odds ratio; CI, confidence interval; CSWs, commercial sex workers; HIV, human immune deficiency virus; STIs, sexual transmitted infections
INTRODUCTION
There is currently no universal acceptable definition of youth. The United Nations (UN) defines the youth as persons between 15 and 24 years; WHO, 10 and 24 years; and the Ethiopian Social Security and Development Policy, 15 and 24 years. However, youth policy of Ethiopia under minister of youth, sport and culture defines it to include parts of the society who are between 15 and 29 years of age (MYSC, 2014; UNESCO, 2013).
The world's population is young: 42% of people are under the age of 25. In South Asia and sub-Saharan Africa, the number of people aged 12 to 24 has steadily risen to 525 million in 2015, almost half the global youth population (SDGs, 2017). Ethiopia is a developing country with the youth population aged 15 to 24 years old, with the most productive force representing 20.11% of total population (CIA, 2018). Dramatic shift in sexual behavior among youths concedes with the rapid disseminations of HIV/ADIS and STIs (Yohannes et al., 2016). Many young people engage in risky sexual behavior and experiences that can result in unintended health outcomes (CDC, 2018). Risky sexual behaviors place youth at risk for HIV infection, other sexually transmitted diseases (STDs), unwanted and unintended pregnancy, abortion, and psychological distress (Cherie and Berhanie, 2015; Tadesse and Yakob, 2015; Adeomi et al., 2014; Alamrew et al., 2013; HWS, 2017). Evidences from different studies stated that, risky sexual behaviors include having more than one sexual partner, early sexual initiation, inconsistent use of condom, having sex with commercial sex workers, use of substances during sexy, and alcohol use (Cherie and Berhanie, 2015; Tadesse and Yakob, 2015; Adeomi et al., 2014; Alamrew et al., 2013; HWS, 2017; Adera et al., 2015; Asrese and Mekonnen, 2018).
AIDS is the second leading cause of death among people worldwide. An estimated 36.9 million people were living with HIV worldwide in 2017. Of these, 3.0 million were children and adolescents under 20 (UNAIDS, 2013, 2015). Adolescent girls and young women aged 15 to 24 years are at particularly high risk of HIV infection, accounting for 20% of new HIV infections among adults globally in 2015 (UNAIDS, 2016). However, AIDS is now the leading cause of death among young people in Africa. Majority of young people living with HIV are in low- and middle-income countries, with 84% in sub-Saharan Africa. In sub-Saharan Africa, adolescent girls and young women account for 25% of new HIV infections among adults, and women account for 56% of new HIV infections among adults (UNAIDS, 2013, 2015, 2016). The Ethiopian Demographic Health Survey HIV report showed that HIV prevalence is 0.3% among young women and 0.1% among young men, aged 15 to 24. Among women, HIV prevalence increases from 0.8%
those with one lifetime sexual partner to 7.0% among those with 10 or more, and increases from 0.3% among men with 1 lifetime sexual partner to 2.9% among those with 10 or more. In Ethiopia, 24% of women aged 15 to 24 and 39% of men aged 15 to 24 have comprehensive knowledge of HIV (CSA, 2018). A study conducted among youth in Botswana stated that correct knowledge about prevention of HIV transmission is also low with only 16.3% (14.1-18.4) of students displaying adequate knowledge about the prevention of HIV transmission (Majelantle et al., 2014).
Sexual behaviors in high HIV/AIDS prevalence countries have generally been unfavorable over the last decade (UNAIDS, 2013). Studies conducted in developing countries showed that 75% of males aged 15 to 24 years who reported having sexual intercourse in the 12 months preceding the survey engaged in higher-risk sex. The proportion of higher-risk sex among male youth, aged 15 to 19 years was nearly 90% in 21 of the 26 countries (Berhan and Berhan, 2015).
Recent surveys in several countries in sub-Saharan Africa have detected decreases in condom use and/or an increase in the number of sexual partners. The overall proportion of condom use during youths’ most recent higher-risk sexual encounter was 40 and 51% among 15 to 19 year olds and 20 to 24 year olds, respectively (UNAIDS, 2013; Berhan Yand Berhan, 2015).
Most of the risks for sexually transmitted infections (STIs) and HIV infection were identified with an attention seeking magnitudes. More than half of the students were at risk for STIs and/or HIV infection due to their varying levels of sexual behaviors such as having multiple sexual partners, regular casual sexual sex and sex with risk commercial sexual workers (CSWs) (Mengistu et al., 2013). One of the studies conducted in Ethiopia stated that more than one third of in-school youths (37.1%) reported having two or more than two lifetime sexual partners (Negeri, 2014). A considerable proportion of school youths were involved in risky sexual practice like early sexual initiation (by age 13 to 14), having multiple sexual partners and inconsistent condom use which predispose them to sexual related health (SRH) problems (Mariam et al., 2018). A study conducted in Southeast Ethiopia showed that more than half of the students were at risk for STIs and/or HIV infection. Additionally, it showed that engaging in casual sex with first sexual partner and having multiple sexual partners in the last 12 months (four and above sexual partners) were independent risk predictors of STIs and/or HIV infections (Mengistu et al., 2013).
Peer pressure, alcohol consumption, watching pornographic materials, early sexual initiation, multiple sexual partnerships, inconsistence use of condoms, chewing ‘khat’ and substance use, depression, poor living arrangement, educational status of parents, family connectedness, having sex with CSWs, and poor knowledge towards HIV/AIDS are the major predictors of risky sexual behaviors among youths (Tadesse and Yakob, 2015; Alamrew et al., 2013;
Mariam et al., 2018; Nigatu et al., 2018; Fentahun and Mamo, 2014; Abebe et al., 2013; Manee and Aria, 2018; Mullu et al., 2016). Alternatively, interpersonal processes like succumbing to peer-norms, intergenerational gaps regarding beliefs about sexual behavior, the socio-economic context of students, and the interplay between desiring love. Also, included are material gain, power, and social status, HIV/AIDS messaging and programs, and the gendered nature of sex information played a great role in sexual risk-taking and exposure to risky sexual behaviors (Ndumiso et al., 2016).
Very few studies have assessed youth and particularly preparatory school student’s risky sexual behavior. Most of these studies were conducted in major towns and used different categories of population. Therefore, the main aim of this study was to assess risky sexual behaviors and associated factors in Arba Minch town, Southern Ethiopia.
MATERIALS AND METHODS
Study setting and period
This study was conducted using preparatory schools students of Arba Minch town from 20th April to 2nd June, 2018. Arba Minch town is the administrative and trading center of the Gamo Gofa Zone, located at 505 km from Addis Ababa the capital city of Ethiopia and 275 km southwest of Hawassa, the regional town of South Nations Nationalities and Peoples Republic. The topography of the land is characterized by undulating feature that favors for the existence of different climatic zones. The general elevation of the zone ranges from 680 to 4207 m above sea level. Mount Gughe, the highest mountain peak in the zone as well as in the SNNPR stretches 4207 m above sea level. The climate here is tropical. In winter, there is less rainfall in Arba Minch than in summer. The climate here is classified as Aw by the Köppen-Geiger system (Figure 1). According to the 2007 Census conducted by the Central Statistical Authority (CSA), the town has a total population of 74,879, of whom 39,208 are men and 35,671 women. The annual population growth rate is found to be 4.8% with 15 years doubling time and the population density of the town is 13 people per hectare.
Study design
An institution-based cross-sectional study design was used to address the objectives.
Study population and sample collection
All preparatory school students (grades 11 and 12) of Arba Minch town were the source population and those selected were study population for this study. Those students who were attending class during data collection period were included; whereas those who were seriously ill and unable to respond were excluded from this study. The sample size for this study was calculated using Epi info7 software Stat Cal. Sample size for each objective was determined separately. For the first objective (to determine the status of risky sexual behaviors), single population proportion and identify associated factors with two sample comparison proportion was used. The sample size used for this study was 495, after adding 10% to the larger sample size from two objectives. The calculated sample size of this study was proportionally allocated to each preparatory school based on the number of students in each school. Then, separate sampling frame (student list from director’s office) was used to select the study participants from each grade (grades 11 and 12) as well as each section. Finally, study participants for this study were selected using a systematic random sampling method.
Data collection methods
A structured pretested self-administered questionnaire, adapted and modified from other similar studies was used to collect data. The tool had four main parts: socio-demographic, sexual and reproductive history, substance abuse and knowledge about HIV/AIDS. Four BSc holder nurses who are fluent in the local language, after taking informed consent, collected the data. Two MSc holder nurses supervised them. A three-day extensive training regarding the objectives of the study, ethical issues on research and data collection procedures was given for both data collectors as well as supervisors.
Measurements
Respondents have risky sexual behaviors if they had at least one of the following: multiple sexual partners; early sexual start, before the age of 18; inconsistent use of condom (incorrect use of condom or failure to use condom at least once during sexual intercourse); and sexual intercourse with commercial sex workers (Tadesse and Yakob, 2015; Alamrew et al., 2013; Mullu et al., 2016). Respondents, who mentioned three or more transmission and prevention ways of HIV/AIDS in addition to the other HIV/AIDS related questions correctly, were categorized to have good knowledge; while those who mentioned below were classified as having poor knowledge towards HIV/AIDS.
Data quality control
The questionnaires were first drafted in English then translated to the local language “Amharic” by a languages expert and finally before data entry again re-translated back to English in order to ensure consistency and quality. Questionnaires were pre-tested in an area with similar characteristics and possible modifications and amendments were done before actual data collection. Data were checked for completeness, accuracy, clarity and consistency at spot by data collections, after data collection by supervisors and before entry into software by principal investigator. Proper coding and categorization of data were maintained for the quality of the data to be analyzed. Double data entry was done for its validity and compared to the original data (data entered by the other data clerk).
Data processing, management and analysis
The data were coded and entered into Epi data version 3.1 in order to maintain logical errors and skipping patterns. Then, the data were exported to SPSS window version 22 for cleaning, editing and analysis. A descriptive analysis was done by computing proportions and summary statistics. The information was presented using simple frequencies, summary measures, tables and figures. Bi-variate s and multivariate analysis was done to see the association between each independent variable and the outcome variable using binary logistic regression. The goodness of fit was tested by Hosmer-Lemeshow statistic and Omnibus tests. All variables with P<0.2 in the bivariate analysis were included in the final model of multivariate analysis in order to control all possible confounders. In addition, variables that were significant in previous studies and from context point of view included in the final model even if the aforementioned criteria was not followed. During multivariate analysis, backward logistic regression was used. Multi co-linearity test was carried out to see the correlation between independent variables using standard error and collinearity statistics. The direction and strength of statistical association was measured by odds ratio with 95% CI. Adjusted odds ratio along with 95% CI was estimated to identify associated factors for risky sexual behaviors. In this study, P-value < 0.05 was considered to declare a result as statistically significant association.
Ethical considerations
Ethical clearance was obtained from Arba Minch University, College of Medicine and Health Sciences, Institutional Ethical Review Committee (AMU-IERC). All the study participants were informed about the purpose of the study, their right to refuse and the signed voluntary consent was obtained from all study participants prior to offering the data collection instruments. The respondents were also been told that the information obtained from them was treated with complete confidentiality and will not inflict any harm on them.
RESULTS
Socio-demographic characteristics of study participants
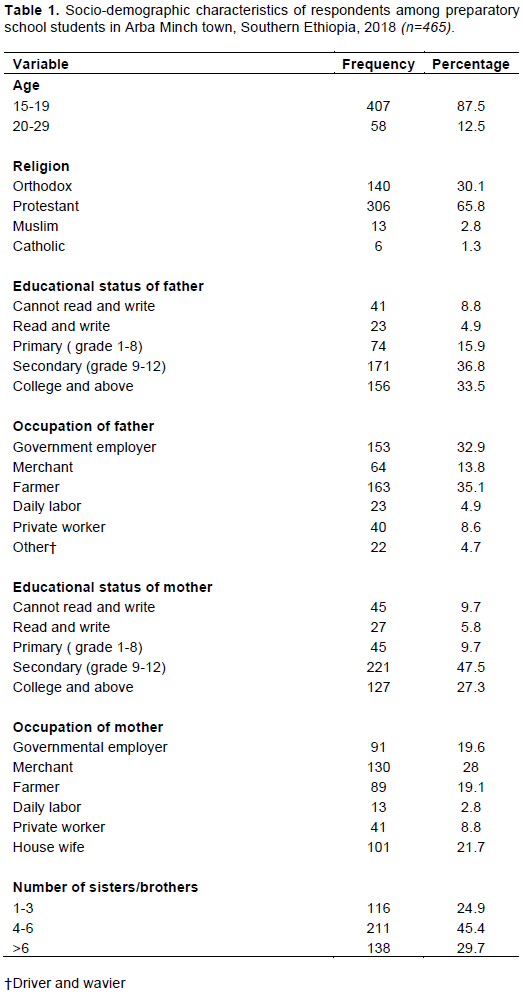
Of the total questionnaire, 465 participants responded with a response rate of 93.9%. From the total respondents, 255 (54.8%) were male. Regarding marital status, 421 (90.5%) were single, while 44 were married (9.5%). The mean age of study participants was 17.92 (±1.34SD). Protestant religion followers constituted 306 (65.8%), 413 (88.8%) lived with family and 412 (88.6%) had participated in religious education. Table 1 shows the other socio-demographic characteristics.
Sexual and reproductive history of respondents
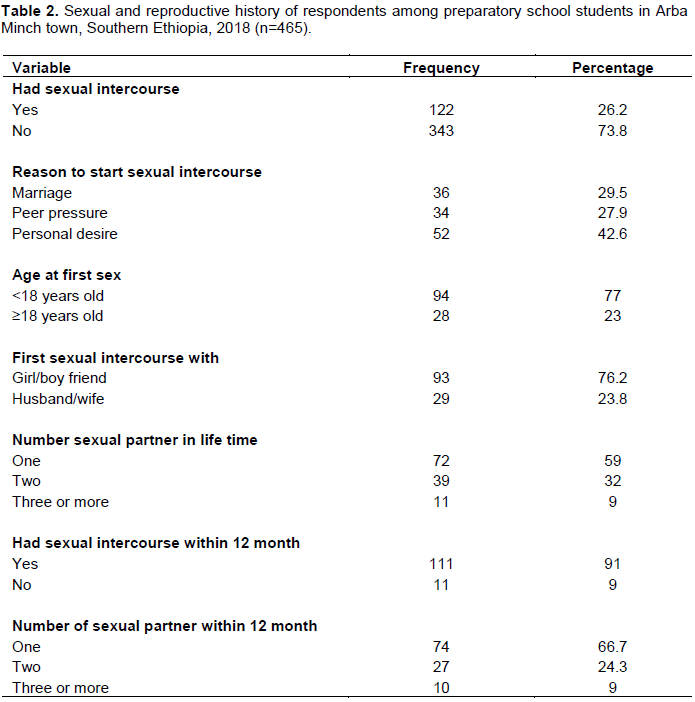
Out of the total respondents, 122 (26.2%) had sexual intercourses and 52 (42.6%) started sex for personal desire. Ninety-four (77%) of the respondents started sex before the age of 18 years, with mean age of 16.18±1.81. Ninety-three (76.2%) had first sex with their partners. From those who had sexual intercourses, 11 (9%) had sex with CSWs. Seventy two (59%) had 1 sexual partner in their lifetime and 74 (66.7%) had sex within 12 months prior to study period. Those who watched pornographic movies made up 213 (45.8%). One hundred forty seven (31.6%) had discussed about sexual intercourse with a family member, relatives and friends (Table 2).
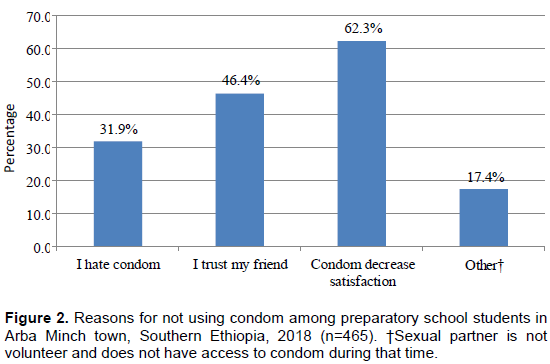
Of the respondents who had sexual intercourse, 93 (76.2%) had used condom in lifetime and 91(82%) used condom for the sexual intercourse within 12 months prior to study period. From those who sometimes used, 45 (49.4%), 4 (4.4%) and 42 (46.2%) used often, constantly and consistently, respectively. Forty-three (62.3%) stated that using a condom decreases satisfaction (Figure 2).
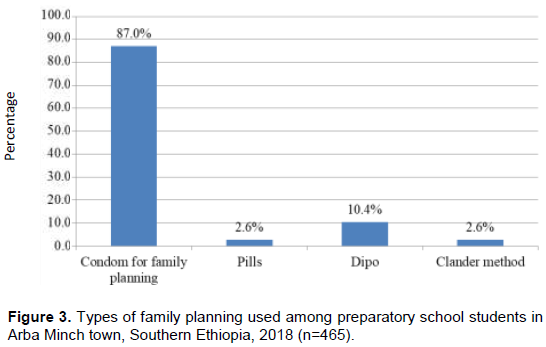
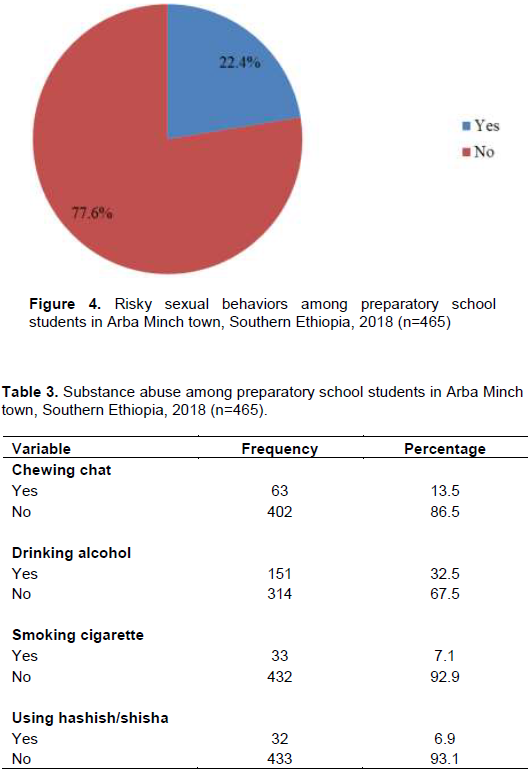
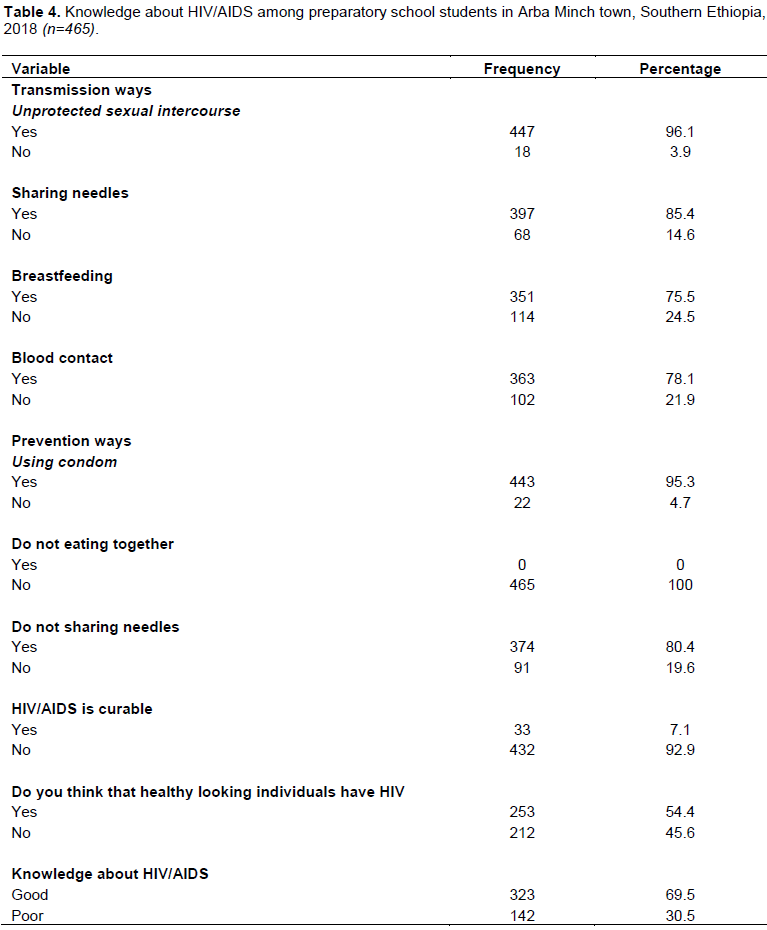
Regarding family planning, 77 (16.6%) used any type of method for family planning, while 67 (87%) used condom (Figure 3). Overall, in this study, 22.4% (95% CI: 18.6, 26.2) study participants had risky sexual behaviors (Figure 4). One hundred fifty one (32.5%) had drinking alcohol (Table 3).
Knowledge about HIV/AIDS among respondents
All the study participants displayed basic knowledge about HIV/AIDS, transmission and prevention ways. As regards to testing knowledge of transmission, 447 (96.1%) stated unprotected sexual intercourse and 397 (85.4%) stated needles. Thirty three (7.1%) of the study participants had reported that HIV/AIDS is curable and 253 (54.4%) thought that healthy looking individuals may have HIV. Overall, 142 (30.5%) respondents had poor knowledge about HIV/AIDS (Table 4).
Factors associated with risky sexual behaviors among study participants
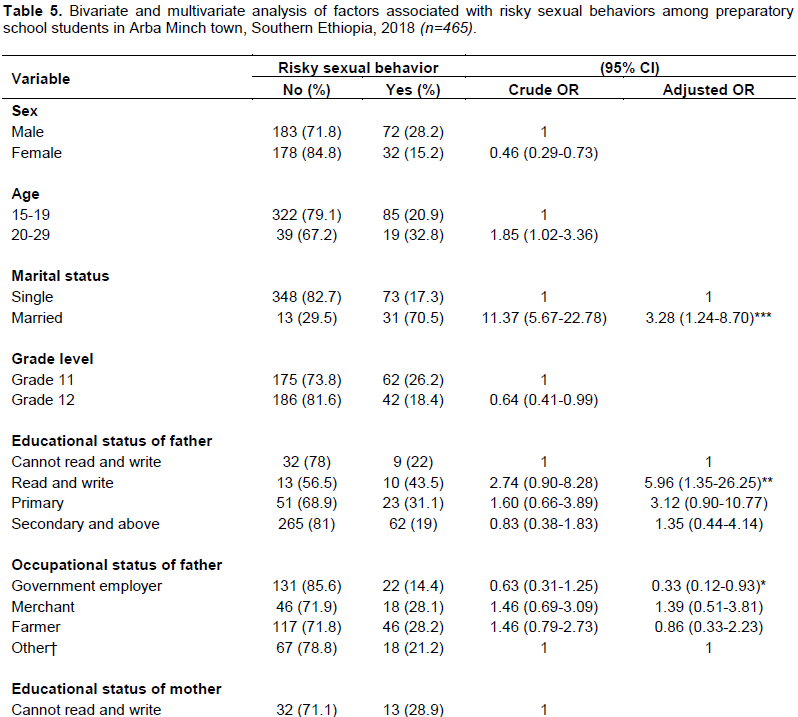
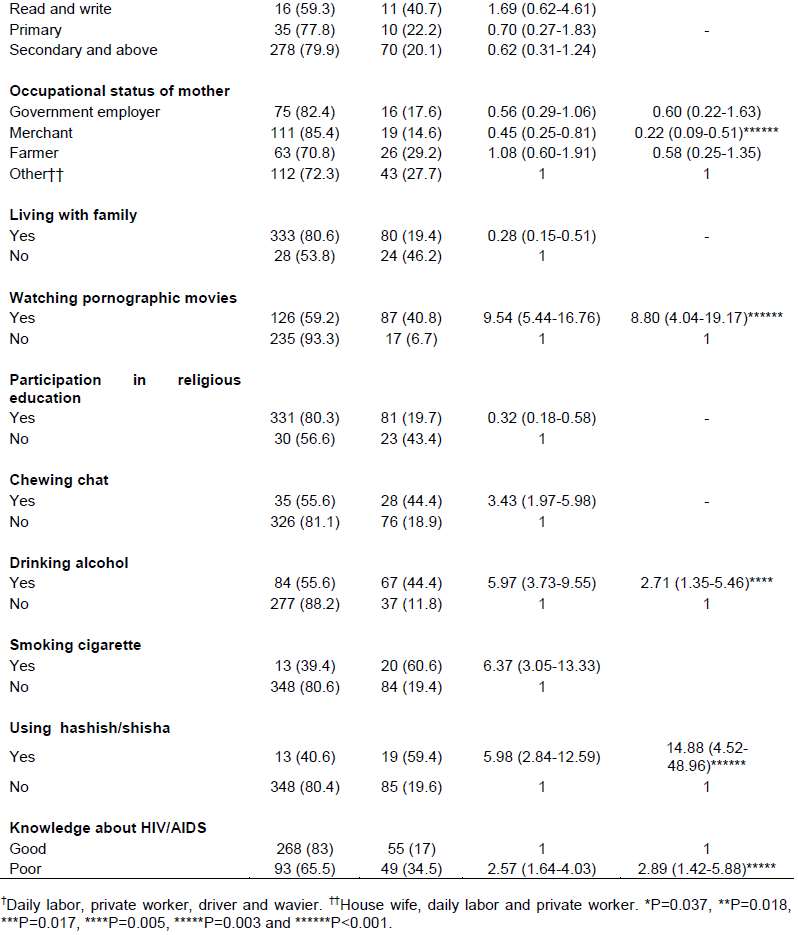
After controlling for possible cofounders in the multivariate model marital status, educational and occupational status of father, occupation of the mother, watching pornographic movies, drinking alcohol, using hashish/shisha and knowledge about HIV/AIDS were significantly associated with risky sexual behaviors. However, sex, age, grade level, educational status of mother, living with family, participation in religious education, chewing chat and smoking cigarette were not.
Married respondents were 3.28 times more likely and students with fathers with a low educational status as compared to others were 5.96 times more likely to be engaged in risky sexual behaviors (AOR=3.28, 95%CI: 1.24, 8.70) and (AOR=5.96, 95%CI: 1.35, 26.25), respectively. Students with fathers who were employed in government were 67% more likely, and those whose mother’s occupational were merchants as compared to others were 78% less likely to be engaged in risky sexual behaviors. The odds of engaging in risky sexual behaviors were 8.8 among respondents who watch pornographic movies (AOR=8.80, 95%CI: 4.04, 19.17) and 2.71 among respondents consuming alcohol (AOR=2.71, 95%CI: 1.35, 5.46). Study participants who had used hashish/shisha were 14.88 times more likely to practice risky sexual behaviors. Additionally, those who had poor knowledge about HIV/AIDS were 2.89 times more likely to practice risky sexual behaviors (AOR=14.88, 95%CI: 4.52, 48.96) and (AOR=2.89, 95%CI: 1.42, 5.88), respectively (Table 5).
DISCUSSION
In this study, the prevalence of risky sexual behaviours was 22.4% (95%CI: 18.6, 26.2). Married respondents were 28% and respondents with educational status with the ability read and write were 96% to be engaged in risky sexual behaviors. The odds of practice of risky sexual behaviors were 0.33 among respondents, whose fathers were employed by the government and 0.22 among those whose mothers were merchants. Study participants who watch pornographic movies were 8.8 times more likely to be engaged in risky sexual behaviors and those who consume alcohol were 2.71 times more likely to be engaged in risky sexual behaviors. The odds of practice of risky sexual behaviors were 14.88 and 2.89 among respondents who use hashish/shisha and poor knowledge about HIV/AIDS, respectively.
The status of risky sexual behaviors was in line with some of the studies done in Ethiopia and Nigeria. This finding was low, compared to different studies conducted in Ethiopia, Spain and Iranian. However, it was inconsistent with some studies conducted in parts of Ethiopia (Cherie and Berhanie, 2015; Tadesse and Yakob, 2015; Adeomi et al., 2014; Alamrew et al., 2013; Asrese and Mekonnen, 2018; Mariam et al., 2018; Abebe et al., 2013; Manee and Aria, 2018; Mullu et al., 2016; Abdu et al., 2017; Dadi and Teklu, 2014; Kahsay et al., 2017; Mamo et al., 2016; Ali, 2017). The reason for this discrepancy is due to the difference in the study area and period difference, socio-cultural factors and difference in methodological aspects.
In this study, 26.2% study participants had sexual intercourse and of them, 91% had sexual intercourse within the last twelve months. This was incongruent with some of the studies done in different parts of the world (Cherie and Berhanie, 2015; Adeomi et al., 2014; Asrese and Mekonnen, 2018; Dadi and Teklu, 2014). Regarding sexual start, 77% of respondents began before the age of 18 years. This was inconsistent with studies done in Nigeria and Ethiopia (Mullu et al., 2016; Ali, 2017). This incongruence may be due to socio-cultural and environmental factors and advance in different factors that promote early sexual start (peer pressure, visiting night clubs, watching different moves and substance abuse).
This finding indicated that 41% of participants had multiple sexual partners having more than one partner in lifetime and 33.3% had within twelve month. This finding was comparable with some studies done in Ethiopia (Furry, 2015; Regassa et al., 2016). However, it was low when compared with other studies done in Ethiopia and Nigeria (Cherie and Berhanie, 2015; Tadesse and Yakob, 2015; Alamrew et al., 2013; Asrese and Mekonnen, 2018; Mengistu et al., 2013; Kahsay et al., 2017; Mamo et al., 2016; Ifeadike et al., 2018; Teferra et al., 2015) and high as compared to some studies done elsewhere (Negeri, 2014; Abebe et al., 2013). The reason for this may be the fact that lives in risky place or environments (urban with a number of nightclubs), luxuries life style and substance abuses. As stated in this study, 82% of respondents had used condom for sex and from them only 46.2% used constantly and consistently. This finding was congruent with studies done in parts of Ethiopia (Cherie and Berhanie, 2015; Kahsay et al., 2017). However, it was inconsistent with studies conducted in Ghana and Ethiopia (Fentahun and Mamo, 2014; Abebe et al., 2013; Amoah, 2017; Gizaw et al., 2018; Henok et al., 2015; Mavhandu-Mudzusi and Asgedom 2016). This may be due to an awareness gap, lack of access to sexual and reproductive health services in friendly way and environmental factors. In this study, only 9% had contact with high risky individual or commercial sex workers (CSWs). This was more or less congruent with one of the study done in Ethiopia (Mamo et al., 2016).
In this study, marital status, those of whose fathers had low educational status and occupational status of governmental employer and mother’s educational status of merchant were significantly associated with risky sexual behaviors. This was in line with studies done in Ethiopia (Tadesse and Yakob, 2015; Alamrew et al., 2013). However, it was inconsistent with Nigeria and Ethiopia studies (Ali, 2017; Ifeadike et al., 2018). The reason for these controversies is socio-economic stability and environmental factors in favor of socio-cultural factors. Exposure to pornographic movies was one factor that promotes unhealthy sexual relationship and this study showed those who had exposure were more likely to practice risky sexual behaviors. This result was supported by different studies done in Tanzania and parts of Ethiopia (Tadesse and Yakob, 2015; Mariam et al., 2018; Nigatu et al., 2018; Kahsay et al., 2017; Yarro and Kafanabo, 2016). Nevertheless, contradictory to some studies done in Ethiopia (Alamrew et al., 2013; Ali, 2017). Drinking alcohol and using hashish/shisha result in inappropriate judgments and unwanted outcomes. This study speculated that those individuals were more prone to risky sexual behavior. This finding correlates with studies done in parts of Ethiopia, in three Asian countries (Hanoi, Shanghai, and Taipei) and Nigeria (Negeri, 2014; Mariam et al., 2018; Nigatu et al., 2018; Fentahun and Mamo, 2014; Kahsay et al., 2017; Ifeadike et al., 2018; Mavhandu-Mudzusi and Asgedom, 2016); however, inconsistent with some studies done elsewhere (Alamrew et al., 2013, Dadi and Teklu, 2014). For this discrepancy, methodological aspects over weight other situations. In general, knowledge gap can be a major factor that results in sexual and reproductive health problems. In this finding those students who had poor knowledge about HIV/AIDS was significantly associated with risky sexual behaviors. This is in line with a study conducted in Ethiopia (Mullu et al., 2016).
Sex, current age of participants, grade level, live with family and participation in religious education were not significantly associated with risky sexual behaviors. This was congruent with studies conducted in Ethiopia (Negeri, 2014; Mariam et al., 2018; Mullu et al., 2016; Ali, 2017). However, it contradicts studies conducted in three Asian countries (Hanoi, Shanghai, and Taipei), Nigeria, Bahamas, Cambodia and else were in Ethiopia (Nigatu et al., 2018; Dadi and Teklu, 2014; Kahsay et al., 2017; Ifeadike et al., 2018; Wang et al., 2015). Maternal educational status was not a significant contributing factor to student’s risky sexual behaviors. This agreed with studies done in Cambodia and Ethiopia (Derbie et al., 2016). In addition, chewing chat and smoking cigarettes were not significant after controlling for confounders in this study.
CONCLUSION
This finding noted that significant numbers of students were engaged in risky sexual behaviours. Those students had multiple sexual partners, inconsistent use of condoms, sex with risky individuals and an early sexual start (by ages 13 to 14). Marital status, educational and occupational status of father’s, occupational status of mother’s, watching pornographic movies, drinking alcohol and using shisha/hashish and poor knowledge about HIV/AIDS were associated factors for risky sexual behaviours in this study. Awareness creation for youths to reduce substance abuse, HIV/AIDS and sexual and reproductive health within the school system should be promoted. Further research should identify other contextually specific factors that contribute to risky sexual behaviours in youth, and develop and tailor programs accordingly.
ACKNOWLEDGEMENTS
The authors’ unreserved thanks go to Arba Minch University, College of Medicine and Health Sciences for financial assistance. They would like to forward their deepest appreciation and thanks to Zonal Educational Office of Gamo Gofa and schools’ director, data collectors and study participants. Also, they would like to appreciate all who supported directly or indirectly. Arba Minch University, College of Medicine and Health and Sciences funded the research for the data collection and stationary materials.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abdu S, Tesfaye HBF (2017). Assessment of Risky Sexual Behaviour and Associated Factors among Jimma University of Kitto Furdisa Campus Students, Jimma Town, Oromia Region, South West of Ethiopia, 2015. Primary Health Care Research and Development |
|
|
Abebe M, Tsion AFN (2013). Living With Parents and Risky Sexual Behaviors among Preparatory School Students in Jimma Zone, South West Ethiopia. African Halth Sciences 13:498-506. |
|
|
Adeomi AA, Adeoye OA, Adewole A, Israel OATO (2014). Sexual Risk Behaviors among Adolescents Attending Secondary Schools in a Southwestern State in Nigeria. Journal of Behavioral Health 3(3):176-180. |
|
|
Adera A, Belete T, Yassin Z, Adem MWG (2015). Assessment of Risk Sexual Behaviors among Adults at Adigrat Town, Tigray, Ethiopia. American Journal of Health Research 3:248-256. |
|
|
Alamrew Z, Bedimo MMA (2013). Risky Sexual Practices and Associated Factors for HIV/AIDS Infection among Private College Students in Bahir Dar City, Northwest Ethiopia. Hindawi Publishing Corporation Isrn Public Health 9 p. |
|
|
Ali AM (2017). Risky Sexual Behavior and Factors Associated with it Among Public and Private Secondary School Students in Addis Ababa City (Ethiopia): A Cross-Sectional Comparative Study. Journal of Gynecology and Reproductive Medicine 1:1-10. |
|
|
Amoah BO (2017). Risky Sexual Behavior and Sexually Transmitted Infections among Students in The Ministry of Health Training Institutions in The Tano North District. |
|
|
Asrese K, Mekonnen A (2018). Social Network Correlates of Risky Sexual Behavior among Adolescents in Bahir Dar and Mecha Districts, North West Ethiopia: An Institution-Based Study. Reproductive Health 15(1):61. |
|
|
Berhan Y, Berhan A (2015). A Meta-Analysis of Risky Sexual Behaviour among Male Youth in Developing Countries. AIDS Research and Treatment 9 p. |
|
|
CDC (2018). Sexual Risk Behaviors: HIV, STD, & Teenage Pregnancy Prevention. |
|
|
Cherie A, Berhanie Y (2015). Assessment of Parenting Practices and Styles and Adolescent Sexual Behavior among High School Adolescents in Addis Ababa, Ethiopia. Journal of AIDS and Clinical Research 6(2):424. |
|
|
CIA (2018). Ethiopia Demographics Profile 2018. |
|
|
Central Statistical Agency (CSA) (2018). Central Statistical Agency (CSA)[Ethiopia] and ICF. 2018. Ethiopia Demographic and Health Survey 2016: HIV Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF. |
|
|
Dadi AF, Teklu FG (2014). Risky Sexual Behavior and Associated Factors among Grade 9-12 Students in Humera Secondary School, Western Zone of Tigray, NW Ethiopia, 2014. Science Journal of Public Health 2:410-416. |
|
|
Derbie A, Assefa M, Mekonnen D, Biadglegne F (2016). Risky Sexual Behaviour and Associated Factors among Students of Debre Tabor University, Northwest Ethiopia: A Cross-Sectional Study. Ethiopian Journal of Health Development 30(1):11-18. |
|
|
Fentahun N, Mamo A (2014). Risky Sexual Behaviors and Associated Factors among Male and Female Students in Jimma Zone Preparatory Schools, South West Ethiopia: Comparative Study. Ethiopian journal of health sciences 24(1):59-68. |
|
|
Furry DB (2015). Intervention Strategies for the Reduction of Sexual Risk Practices among Adolescents in Ethiopia. |
|
|
Gizaw AT, Abreha GK, Legesse T, Hailesilassie H (2018). Predictors of HIV/AIDS Preventive Behavior among College Students in Gambella Town, Southwest Ethiopia Using Health Belief Model. Journal of Aids and HIV Research 10:13-21. |
|
|
Henok A, Kassa A, Lenda A, Nibret A, Lamaro T (2015). Knowledge, Attitude and Practice of Risky Sexual Behavior and Condom Utilization among Regular Students of Mizan-Tepi University, South West Ethiopia. Journal of Child and Adolescent Behavior 3:244. |
|
|
Healthwise Staff (HWS) (2017). High-Risk Sexual Behaviour. |
|
|
Ifeadike CO, Nnebue CC, Oparaji CI, Okorie OF, Okoro UC, Okoyechira VC (2018). Sexual Risk Behaviors and Associated Factors among Senior Secondary Schools Adolescents in Owerri, Imo State Nigeria. International STD Research and Reviews 7:1-12. |
|
|
Kahsay T, Jejaw AKM (2017). Risky Sexual Behaviors and Associated Factors Among Mizan, Bonga and Tepi Preparatory School Students, Southwestern, Ethiopia, 2016: A Cross Sectional Study. J Aids Clin Res Sex Transm Dis 4 p. |
|
|
Majelantle Rg, Keetile M, Bainame KPN (2014). Knowledge, Opinions and Attitudes Towards HIV and AIDS among Youth In Botswana. Journal of Global Economics 2:108. |
|
|
Mamo K, Admasu EMB (2016). Prevalence and Associated Factors of Risky Sexual Behavior among Debremarkos University Regular Undergraduate Students, Debremarkos Town North West Ethiopia, 2016. Journal of Health, Medicine and Nursing 33 p. |
|
|
Manee FM, Aria AM (2018). Personal and Social Predictors of Risky Sexual Behaviours in Iranian Youth. Global Journal of Psychology Research: New Trends And Issues 8:10-24. |
|
|
Mariam S, Assefa N, Tejineh SHZ (2018). Substance Use and Factors Associated with Risky Sexual Practice in School Youth in sella Town, South-East Ethiopia, 2017. Journal of Public Health and Epidemiology 10:6-15. |
|
|
Mavhandu-Mudzusi AH, Asgedom TT (2016). The Prevalence of Risky Sexual Behaviours amongst Undergraduate Students in Jigjiga University, Ethiopia. Health Sagesondhe 21:179 -186. |
|
|
Mengistu TS, Melku AT, Bedada NDTEB (2013). Risks for STIS/HIV Infection among Madawalabu University Students, Southeast Ethiopia: A Cross Sectional Study. Reproductive health 10(1):38. |
|
|
Mullu G, Degu G, Yitayew M, Misganaw W, Muche M, Demelash T Mesele MMA (2016). Risky Sexual Behaviors and Associated Factors among Jiga High School And Preparatory School Students, Amhara Region, Ethiopia. Hindawi Publishing Corporation International Scholarly Research Notices 7 p. |
|
|
Ministry of Youth, Sports and Culture (MYSC) (2014). Youth Policy. Ministry of Youth, Sports and Culture of Ethiopia. |
|
|
Ndumiso DN, Sibusiso M, Thobile Z, Jamila KA, Suresh BKN (2016). Qualitative Evaluation of Selected Social Factors that Impact Sexual Risk-Taking Behaviour among African Students in Kwazulu-Natal, South Africa, Sahara-J. Journal of Social Aspects of HIV/AIDS 13:96-105. |
|
|
Negeri EL (2014). Assessment of Risky Sexual Behaviors and Risk Perception among Youths in Western Ethiopia: The Influences of Family and Peers: A Comparative Cross-Sectional Study. BMC Public Health 14:301. |
|
|
Nigatu DT, Seme A, Fituma STSM (2018). Sexual Initiation and Associated Factors among Young Women in West Shoa, Ambo Town, Ethiopia: A Community-Based Cross-Sectional Study. BMC women'shealth 18:76. |
|
|
Regassa T, Chala D, Adeba E (2016). Premarital Sex in The Last Twelve Months and Its Predictors among Students of Wollega University. Ethiopian journal of health sciences 26(4):351-358. |
|
|
Sustainable Development Goals (SDGs) (2017). The 2017 Atlas of Sustainable Development Goals: A New Visual Guide To Data and Development. How is The World's Youth Population Changing? Teferra TB, Erena AN, Kebede A (2015). Prevalence of Premarital Sexual Practice and Associated Factors among Undergraduate Health Science Students of Madawalabu University, Bale Goba, South East Ethiopia: Institution Based Cross Sectional Study. Pan African Medical Journal 20(1):209. |
|
|
Tadesse G, Yakob B (2015). Risky Sexual Behaviors among Female Youth in Tiss Abay, A Semi-Urban Area of The Amhara Region, Ethiopia. PlosOne 10 p. |
|
|
UNAIDS (2013). Joint United Nations Programme on HIV/AIDS. Global Report. UNAIDS Report on the Global Aids Epidemic. |
|
|
UNAIDS (2015). Active Involvement of Young People is Key To Ending the AIDS Epidemic By 2030. |
|
|
UNAIDS (2016). Global AIDS Update. |
|
|
UNESCO (2013). What Do We Mean By "Youth"? Social And Human Sciences: UNESCO. |
|
|
Wang B, Stanton B, Deveaux L, Li X, Lunn S (2015). Dynamic Relationships Between Parental Monitoring, Peer Risk Involvement and Sexual Risk Behavior among Bahamian Midadolescents. Int Perspect Sex Reprod Health 41:89-98. |
|
|
Yarro SJ, Kafanabo EJ (2016). Major Causes and Perpetrators of Sexual Activities among Teenage Students in Tanzania: A Cross Sectional Survey In Kinondoni District. International Journal of Public Health Research 4:23-29. |
|
|
Yohannes M, Tegabu D, G/Slassie M, Gidey BGG (2016). Value of Virginity Related with Sexual Behaviour and Associated Factors among Youth in Mekelle City, Northern Ethiopia. European Journal of Pharmaceutical and Medical Research 3:199-205. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


