ABSTRACT
Rabies, one of the oldest and deadliest diseases known to human, is incurable and neglected viral zoonosis which has been threatening the human life for many years despite being entirely preventable. Community awareness play significant role in preventing this fatal disease. Therefore, this cross sectional study was conducted from November to December 2016 with the objective to assess the community knowledge, attitudes, and practices (KAP) regarding rabies in Munesa district, Arsi zone, south eastern Ethiopia. A multistage sampling technique was employed for selection of sample unit and data were collected from 150 household by face-to-face interview using a semi structured pretested questionnaire. Logistic regression was used for assessing the association of independent variable with KAP score. Out of 150 participants interviewed 59.3% of them were males and 40.7% were females. The respondents from urban, peri-urban and rural residence comprise about 32.7%, 30% and 37.3% of total participants, respectively. Almost all (99.3%) participants had heard about rabies and 88.7% of them knew its zoonotic significance which is a good Knowledge. However, knowledge gap was observed regarding the cause, transmission, incubation period and prevention methods. The overall KAP result revealed that 57.3% and 42.3% of participants had a good and poor KAP score, respectively. Multivariable logistic regression analysis indicated that good KAP score was significantly higher in male than female (OR= 3.14, CI=1.01 - 9.79, P = 0.048), in those who experienced dog bite than those who were not bitten by dog (OR=7.37, CI=1.83-29.61, P=0.005), in dog owners than non-dog owners (OR=7.53, CI=2.01-28.19, p=0.003) and in trained participants than untrained (OR= 18.62, CI=1.56-222.47, p= 0.021). Furthermore, education level (p=0.021) and residence (p=0.031) participants were also significantly associated with a higher good KAP score. This study showed that community in munesa district has good general information about rabies. However, there is a need for further awareness creation which requires the collaborative effort of government authority, medical and veterinary professionals.
Key words: Attitudes, community knowledge, Ethiopia, rabies, zoonotic disease.
Rabies is a fatal zoonotic central nervous system disease that is transmitted by both wild and domestic animals. This disease affects all warm- blooded mammals including human and has been threatening the lives of mankind for more than 4,000 years (Schnell et al., 2010; Liu et al., 2011). Globally, it is estimated that at least 55,000 people die of rabies each year (Zhao et al., 2008; Matsumoto et al., 2010). The causative agent for rabies is rabies virus which belongs to the order Mononegavirales, family Rhabdoviridae, and genus Lyssavirus. This virus has a negative single-stranded RNA genome and the virions are bullet-shaped (Schnell et al., 2010). The disease is characterized by the development of severe nervous symptoms that lead to paralysis and death (Abera, 2015). Once symptoms of the disease develop, it is invariably fatal and deadly viral disease that can only be prevented but not cured (Blackmore, 2014). Dogs remain the primary reservoir in developing countries, whereas wildlife species serve as hosts in developed nations (Rupprecht et al., 2007). According to the WHO, dog rabies potentially threatens over three billion people in Africa and Asia. People most at risk live in rural areas, where vaccines and immunoglobulin are not readily available (WHO, 2013).
The World Health Organization considers rabies to be a neglected disease and declare it to be primarily a problem in areas troubled with poverty and with a lack of economic resources (WHO, 2013). With over several deaths per year (Nilsson, 2014) and signs of it re-emerging (Depani et al., 2012). In Ethiopia rabies has been known for centuries in society as “Mad Dog Disease (Fekadu, 1997) and has been recorded scientifically since 1903 (Pankhrust, 1990). To date, rabies is an important disease in Ethiopia both in human and animals (Tschopp et al., 2016; Deressa et al., 2010; Yimer et al., 2012; Teklu et al., 2017). In Four-Year Retrospective Study by Teklu et al. (2017) in Northwestern Tigray the incidence of human rabies exposure cases calculated per 100,000 populations was 35.8, 63.0, 89.8 and 73.1 in 2012, 2013, 2014 and 2015, respectively. The proximity of the site of the virus entry to the CNS increases the likelihood of a short incubation period (Yin et al., 2012). Following the bite of rabid animal the incubation period varies from 5 days to several years (usually 2 to 3 months; rarely more than 1 year) depending on the amount of virus in the inoculum, the density of motor endplates at the wound site and the proximity of virus entry to the central nervous system (WHO, 2013). In animal the initial clinical signs are often nonspecific and may include fearfulness, restlessness, anorexia or an increased appetite, vomiting, diarrhea, a slight fever, dilation of the pupils, hyperreactivity to stimuli and excessive salivation. The first sign of post-vaccinal rabies is usually lameness in the vaccinated leg. Animals often have behavioral and temperament changes, and may become either unusually aggressive or uncharacteristically affectionate (OIE, 2012). Rabies is fatal and incurable disease once the clinical signs appear (Deressa et al., 2010). However, it can be prevented before the latent symptoms can develop by giving an injection of rabies immune globulin and another injection of rabies vaccine as soon as possible after the bite or exposure to saliva from an infected animal (Yousaf et al., 2012). Essential components of rabies prevention and control include community awareness, responsible pet ownership, routine veterinary care and vaccination, and professional continuing education (Chernet and Nejash, 2016). The community knowledge, attitudes and practices are important both for prevention of human deaths due to rabies and for control of the disease in animals (Dhand et al., 2012). To realize this knowledge, attitudes and practices (KAP) studies have been widely used (Sambo et al., 2014; Serebe et al., 2014; Tiembre et al., 2014; Kabeta et al., 2015; Digafe et al., 2015; Yalemebrat et al., 2016). Even though rabies is endemic disease in Ethiopia, little is known about awareness level of the community and no information were available particular in munesa district despite, the significance of such study in evaluation of community awareness and thereby helping in planning and implementation of rabies control programs.
Therefore, the objective of this study was to assess the community knowledge, attitudes, and practices regarding rabies in Munesa district, Arsi zone, south eastern Ethiopia.
Study area
The study was conducted from November 2016 to December 2016 to assess the level of knowledge, attitudes and practices towards rabies in Munesa district, Southeastern Ethiopia. Munesa is one of the districts in the Arsi Zone located in the Great Rift Valley. The administrative center of the woreda is Kersa town which is found at distance of 232 km away from Addis Ababa, the capital city of Ethiopia and 57 km from the capital of Arsi Zone, Asella. Munesa district is bordered on the south and west by the Mirab Arsi Zone and Lake Langano, on the northwest by Ziway Dugda, on the north by Tiyo, on the northeast by Digeluna Tijo and on the east by Bekoji.
The altitude of Munesa woreda ranges from 1500 over 4100 m above sea level. The annual average rainfall is 800 to 1200 mm and mostly with clay type of soil and rare case black soil. Vegetation of the area changes with altitude and rainfall ranging from scattered trees and bushes to dense shrubs and bushes. According to CSA (2016) the total population of Munesa is 211,762, of whom 104,628 are males and 107,134 are females. Livestock are the major agricultural resources in the area and has livestock population of 230,300 cattle, 103,000 sheep, 9,390 goat, 27,732 horses, 18,806, donkeys 83,806 poultry, 937 mules, 22,764 canines and 12,460 feline (LHDOMW, 2012).
Study design and study population
Community based cross-sectional questionnaire survey was conducted to assess the knowledge, attitude and practice about rabies Munesa district. The questionnaire was semi-structured with both open and closed-ended questions and the details of individual participated in the interview were incorporated. Knowledge of the disease, treatment and prevention practices were also included in the questionnaire.
The study population comprises of community of Munesa district in five randomly selected kebele which includes the residents from urban, peri-urban and rural community. The household who live at least 6 months as the permanent resident in the Munesa were included based on their willingness and informed consent. However, the household who live less than 6 months and who are under 15 years were excluded from the study. The questionnaire was first prepared in English and translated to Afaan Oromo for appropriateness and easiness in approaching the study participants. Before the interview begun they were briefed about the purpose of the study and asked for their consent. Only voluntary participants were involved in the study and all the information obtained from the study participants were kept confidential.
For assessing the community knowledge, attitude and practices (KAP) about rabies each respondent were asked a questions regarding cause, sources, mode of transmissions, clinical signs, prevention practices and treatment measures. Furthermore, actions for rabid animal, rabies fatality, feeling if infected by rabies, preferred actions taken for bitten human, immediate action (first aid) for bitten human, time for anti-rabies vaccine in human after exposure, whether rabies is preventable by vaccination of dog and eliminating stray or confining dogs helps to prevent rabies or not were asked. Respondents who answered the questions correctly had got one mark and zero for incorrect or do not know responses. Then, the responses for which respondents give correct answer was counted and scored.
This score was then pooled together and the mean score was computed to determine the overall KAP of respondents. Respondents who scored greater than or equal to the mean value (Mean=10.55, SD=3.574) were grouped to good KAP and coded as 1 whereas, the respondent who scored less than the mean value were grouped to Poor KAP level and coded as 0.
Sample size determination and sampling techniques
The sample size was calculated using the formula given by Arsham (2005). N = 0.25 / SE2 Where N = sample size, S = standard error, 5%. Accordingly, the required sample size was 100. However, to increase the precision and representativeness the sample size was increased to 150. For the selection of the sampling units a multi-stage sampling technique was employed. From the entire study population in the district six kebele (the smallest administrative unit) were selected by simple random sampling methods, namely Adare, Munessa, Gunguma, Khote, and Kersa 01 and Kersa 02. Then the household in the selected kebeles was further selected using a systematic random sampling technique. Finally, from all the eligible respondents in a household, only one was selected randomly for the interview.
However, in the absence of eligible respondent in a given household, a replacement was immediately made by an individual in the next household until required sample size was obtained. Data were collected by face-to-face interview using pre-tested questionnaire.
Before starting data collection the questionnaire was first pre tested on 10 randomly selected individual in district to check for completeness, clarity, reliability, and sociocultural acceptability then after edited as required. The individual used in validation of questionnaire was not included in the main study.
Data management and analysis
The data collected from questionnaire survey were cleaned and checked for its completeness and entered into Microsoft Excel 2010 spread sheet and analysed using the Statistical Package for Social Science (SPSS) Version 20. The descriptive statistics was used for calculating frequency and percentage both dependent and independent variable. Logistic regression used was for calculating the association between independent variables and dependent variable (KAP scores) of community regarding rabies. A 95% confidence interval of the OR and p-values were used to describe statistical significance associations. The association is judged as significant when p- value is less than 0.05.
Socio demographic character of the participants
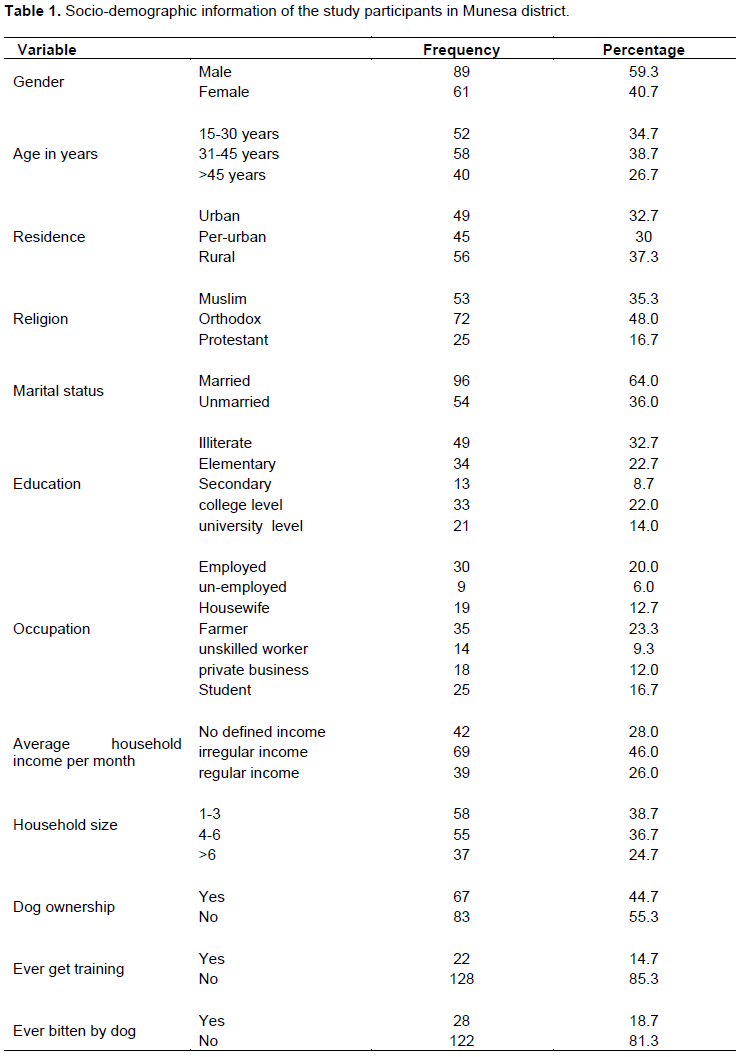
In this study a total of 150 communities in munesa district were interviewed. Table 1 shows the Socio-demographic information of the study participants. Out of 150 participants, 89 (59.3%) of them were males and 61 (40.7% were females and 34.7, 38.7 and 26.7% of the participants are in age group of 15-30 years, 31-45 years and >45 years old, respectively). Regarding the residence of the respondents, urban, peri-urban and rural residence comprises about 49(32.7%), 45(30%) and 56(37.3%) of total participants, respectively. Concerning the religion of participant’s majority was Orthodox 72 (48.0%) and followed by Muslim 53 (35.3%) and Protestant 25 (16.7%). Furthermore, the majority of study participants were married 96 (64.0%) and 69 (46.0%) had irregular average household income per month. Regarding the educational status of respondents, the number and percentage of illiterate, elementary, secondary, college level and university level were 49 (32.7%), 34 (22.7%), 13 (8.7%), 33 (22.0%) and 21 (14.0%), respectively. The frequency and percentages of participants with household size of 1-3, 4-6 and >6 were 58 (38.7%), 55 (36.7%) and 37 (24.7%). Moreover, 44.7% participants were dog owners and 18.7% had experienced dog bite one or more times in their life. Besides, from the whole community members 85.3% responded as they were not trained regarding this disease.
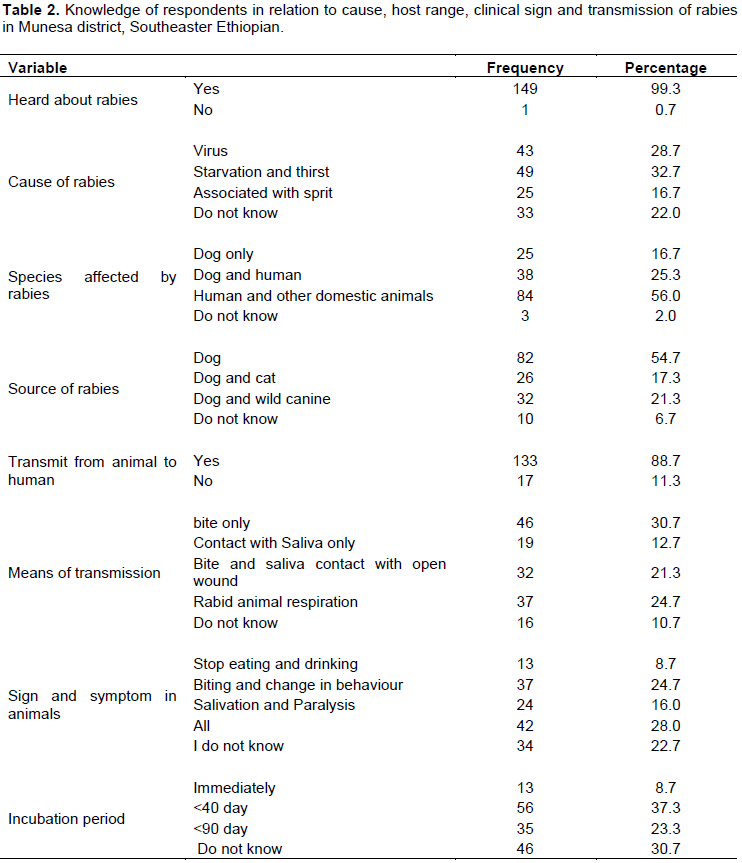
Knowledge of respondents in relation to cause, host range, clinical sign and transmission of rabies
In this study almost all (99.3%) participants had heard about rabies. However, 49 (32.7%) of respondent replied starvation and thirst as the causative agent of rabies. Moreover, more than half of the respondent (56.0%) mentioned as rabies can affect human and other domestic animals regarding source of rabies dog was responded by 54.7% of the participants. 133 (88.7%) knew the transmission of rabies from animal to human. However, only 32(21.3%) knew rabies transmission by bite and saliva contact with open wound and 12.7% of them believe as any type of contact (irrespective of the skin condition) with saliva of rabid individual can transmit the virus to human.
Furthermore, rabid animal respiration was replied by 37 (24.7%) of the participants as a means of transmission. The most common sign and symptom mentioned by 8.7, 24.7 and 16.0% were stop eating and drinking, biting and change in behaviour and salivation and paralysis, respectively (Table 2). Regarding the incubation period of rabies, 37.3% of the participant knew as it is less than 40 days. Knowledge of respondents in relation to cause, host range, clinical sign and transmission of rabies are summarized in Table 2.
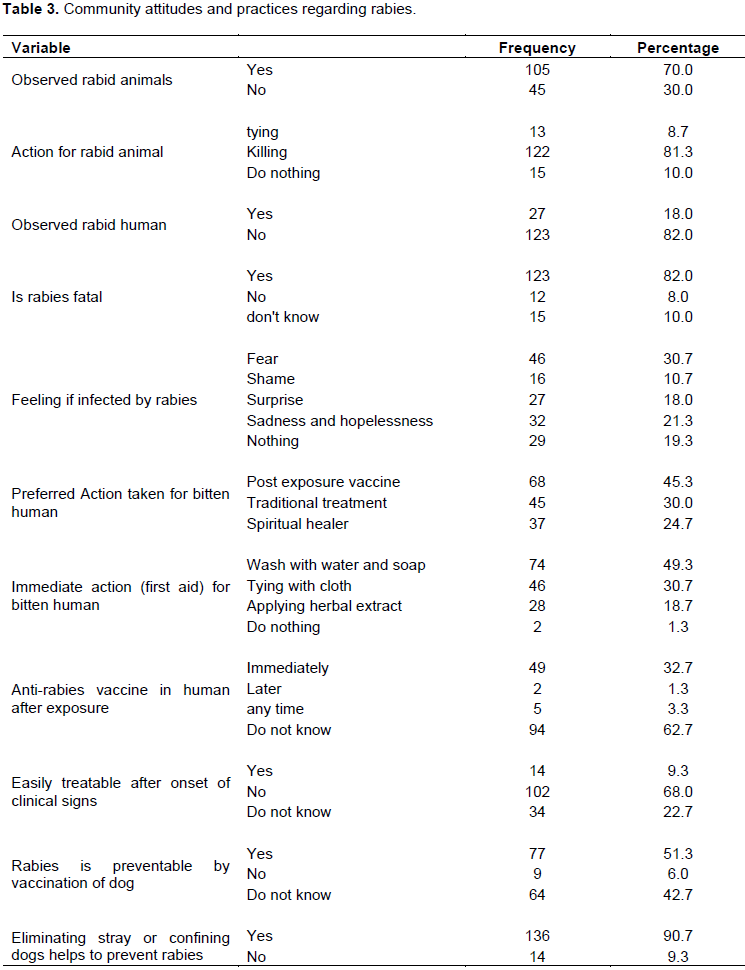
Community attitudes and practices regarding rabies
Out of total participants 70.0 and 18.0% of the participants had observed rabid animal(s) and humans(s), respectively. Furthermore, 81.3% respondents replied killing as the preferred method for rabid animal. Majority (82.0%) of the respondents considered rabies as fatal disease and 30.7% responded as they fear rabies. Regarding the preferred action taken for bitten human 68 (45.3%), 45 (30.0%) and 37 (24.7%) of participants responded post exposure vaccine, traditional treatment and Spiritual healer, respectively. Almost half (49.3%) participants wash the wound with water and soap as immediate action (first aid) for bitten human, whereas, 30.7 and 18.7% tying with cloth apply herbal extract, respectively. Moreover, 32.7% of the participants knew that anti-rabies vaccine after exposure should be immediately and out of total respondents 68.0% knew as rabies is not easily treatable after onset of clinical signs. 51.3% participants knew as rabies is preventable by vaccination of dogs and majority (90.7%) responded as eliminating stray dogs or confining dog helps to prevent rabies. The community attitudes and practices regarding rabies are summarized in Table 3.
Factors associated with knowledge, attitudes and practices (KAP) towards rabies
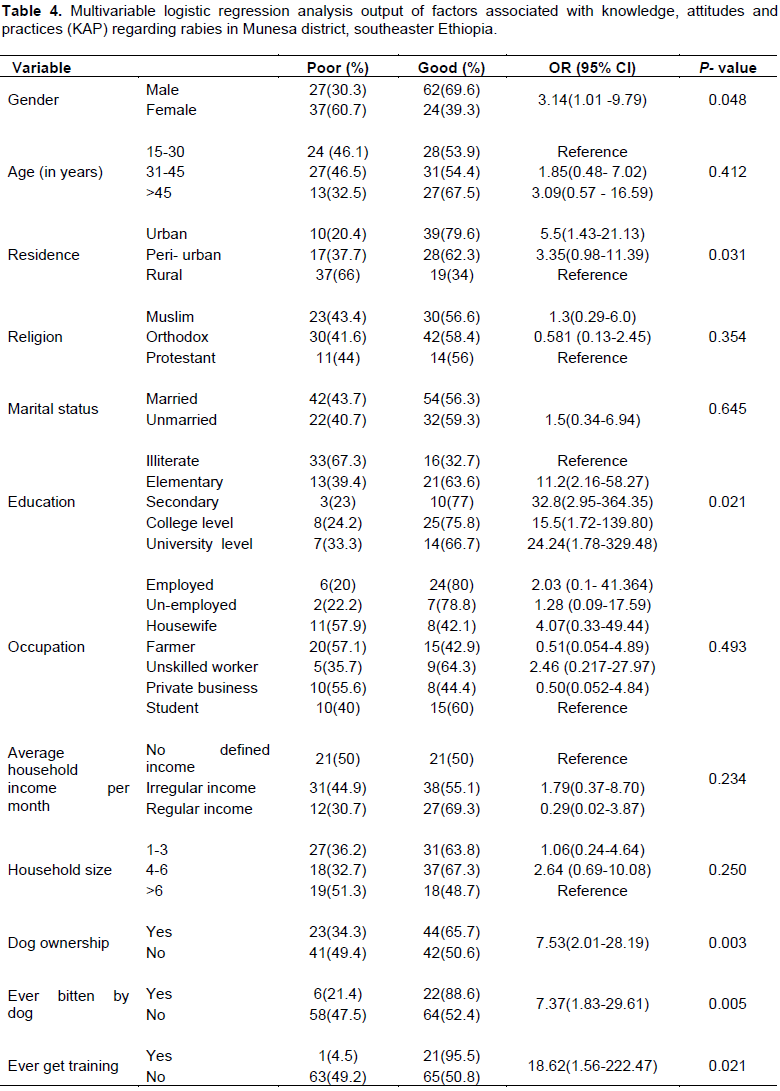
In this study the overall knowledge, attitude and practice (KAP) study revealed that 57.3% of participants had a good KAP, whereas 42.3% was found to have poor KAP score. Table 4 shows the multivariable logistic regression analysis output of factors associated with knowledge, attitudes and practices (KAP) regarding rabies. Accordingly the higher good KAP score was found to be significantly associated with gender in which higher good score was found in male (69.6%) than female (39.3). Males were about 3.14 times more likely to have higher good KAP score than males (OR=3.14, CI=1.01 -9.79, P=0.048). The residence of respondents was also found to be significantly associated with higher good KAP score in which respondents from urban were 5.5 time more likely to have higher good score than urban residents. Moreover, the odds of higher good KAP score in elementary, secondary, college level and university level were 11.2, 32.8, 15.5 and 24.24 times more likely than illiterate (Table 4). The participant who experience dog bite were 7.37 time more likely to have higher good KAP score than those did not experienced dog bite (OR=7.37,
CI=1.83-29.61, P=0.005). Moreover, dog owners and participants who were trained about rabies were 7.53 and 18.62 time more likely to have higher good KAP score than none dog owners and untrained participants, respectively (Table 4). Furthermore, insignificantly (0.645) higher good KAP score was recorded in married (56.3%) participants than unmarried (59.3%). Insignificantly higher good KAP score was also found in age group between 31 and 4 (53.9%) and above 45 years (67.5%) than respondents in age group of 15-30 years (54.4%). Those who were above 45 years are 3.09 times more likely to have higher good KAP score than 15-30 years participants. The odds of higher good KAP score in employed, un-employed, housewife, farmer, unskilled worker, and those having private business than students were 2.03, 1.28, 4.07, 0.51 2.46 and 0.50, respectively. However, this variation is not statically significant (p=0.493). The association household size with KAP score was also not significant (p=0.250) despite higher good KAP score in household size of 1-3 (63.8%) and 4-6 (67.3%) than above 6 (48.7%). The odds of higher good KAP score in household size of 1-3 and 4-6 than above 6 were 1.06 and 2.64, respectively. Regarding the association of average household income per month with KAP score multivariable logistic regression analysis output showed statically insignificant association (p = 0.250) (Table 4).
The result of current study revealed that rabies is an important disease of both human and animals in the study area. All most all (99.3%) had heard about rabies. In line with this finding several scholars from different area of Ethiopia (Digafe et al., 2015; Yalemebrat et al., 2016) and other country (Singh and Choudhary, 2005) reported a similar findings. Regarding the causative agent of rabies 32.7% of respondent were found to have misperception which was starvation and thirst. Similar misperception were reported by several scholars from different area of Ethiopia (Guadu et al., 2014; Gebeyaw and Teshome, 2016; Yalemebrat et al., 2016). The current finding is lower when compared with the result of study in and around Dessie town, Ethiopia which was 49.6% (Gebeyaw and Teshome, 2016) and the result of study in Debark District, North Gondar, Ethiopia 63.5% (Yalemebrat et al., 2016). However, this finding is higher when compared with the study conducted Bahir Dar town which was 24.1% (Guadu et al., 2014). This variation might be associated with difference in awareness of the community between different study areas.
In the current study 88.7% of participants knew the transmission of rabies from animal to human. This finding was in agreement with the result of Yalemebrat et al. (2016). However, Guadu et al. (2014) reported a lower result (21.4%) from Bahir Dar town and higher result (71.9%) was also reported in the city of New York, USA (Eidson et al., 2004). The possible reason for this could be due to the availability of different host range, level of awareness and educational status of community. Despite good knowledge of rabies transmission from animal to human, only 21.3% knew rabies transmission by bite and saliva contact with open wound and 12.7% of them believe as any type of contact (irrespective of the skin condition) with saliva of rabid individual can transmit the virus to human. Another important misperception regarding rabies transmission was rabid animal respiration as 24.7% of the participant responded rabid animal respiration as a transmission means of rabies from animal to human. Thus, the community deserve awareness in these regard as these are serious knowledge deficiency which interfere with rabies prevention and control program.
This study revealed that 37.3% of the participant knew incubation period of rabies as it is less than 40 days. This misperception is also in agreement with the report of several scholars from different area of Ethiopia (Digafe et al., 2015; Kabeta et al., 2015; Yalemebrat et al., 2016). This misunderstanding about the incubation period indicates that those who believe this incubation period do not seek post exposure prophylaxis once the perceived incubation period passed. This is serious for rabies infected individuals where mortality is 100% after development of clinical signs. The incubation period varies from 5 days to several years (usually 2 to 3 months; rarely more than 1 year) depending on the amount of virus in the inoculum, the density of motor endplates at the wound site and the proximity of virus entry to the central nervous system (WHO, 2013).
Majority (82.0%) of the respondents considered rabies as fatal disease and 30.7% responded as they fear rabies. Similarly a higher response rate regarding fatality was reported from different area of Ethiopia and other country. 94.5% reported in the study conducted in Bahir Dar town (Guadu et al. (2014). 94.1% was also reported in study conducted in New York, USA (Eidson et al., 2004). Furthermore, 99.0% was reported in Debark district (Yalemebrat et al., 2016). However, lower (30.97%) was also from Addis Ababa (Ali et al., 2013). This could be associated with sample size difference and awareness level of the community.
Among immediate action taken for bitten human, almost half (49.3%) participants wash the wound with water and soap as immediate action (first aid), whereas, 30.7 and 18.7% tying with cloth apply herbal extract, respectively. The 49.3% finding in this study is higher compared to the study conducted in Gondar zuria district (30.7%) (Digafe et al., 2015) and in a rural Community of Gujarat, India (31.1%) (Singhand Choudhary, 2005). The variation may be due to the study area and awareness level of the community. This treatment is cheap, readily available and feasible for all to apply. Washing of rabies-infected wounds with soap and water can increase survival by 50% (Radostits et al., 2007).
Regarding the preferred action taken for bitten human 45.3, 30.0 and 24.7% of participants responded post exposure vaccine, traditional treatment and Spiritual healer, respectively. Low level (45.3% of preference for post exposure vaccine was recorded in this study. Similar finding was also recorded in Debark district which was 42.1% preference (Yalemebrat et al., 2016). The preference for traditional treatment recorded in this study was low when compared to study conducted in Gondar zuria district, Ethiopia, which reported 62.2% preference for traditional medicine (Digafe et al., 2015) and study in Debark district which reported 54.8 preference for traditional medicine (Yalemebrat et al., 2016). Furthermore, a higher (84%) reliance of respondents on traditional treatment was also reported from Dabat and Gondar (Jemberu et al., 2013). The preference for traditional practices might be arise from many factors including easy access to traditional medicine, lack of awareness, long duration of treatment. Reliance on traditional medicines with unproven efficacy is very risky and nothing can be done to save one’s life after the first symptoms of the disease occur. In our study 32.7% of the participants knew that anti-rabies vaccine after exposure should be immediate. Similarly the study in Bahar Dar town reported 55.7% response for immediate post exposure vaccination (Guadu et al., 2014). The World Health Organization (WHO) also recommends wound washing and vaccination immediately after contact with a suspected rabid animal which can prevent almost 100% of rabies deaths (WHO, 2013).
In the current study the overall knowledge, attitude and practice (KAP) study revealed that 57.3% of participants had a good KAP, whereas 42.3% was found to have poor KAP score. This finding is lower when compared with Study by Guadu et al. (2014) who reported about 64.1% among the community of Bahir Dar town and Yalemebrat et al. (2016) who reported 60.3% in Debark District, North Gondar.
This difference could be due to his difference in sample size and level of awareness of community. Multivariable logistic regression analysis revealed higher good KAP score to be significantly associated with gender in which higher good score was found in male (69.6%) than female (39.3). Males were about 3.14 times more likely to have higher good KAP score than males. The same proportion of statistical difference on KAP score of male (53.4%) and female (10.75%) was reported in Bahirdar town by Guadu et al. (2014), in Addis Ababa (Male, moderate (77.09%) and good (10.55%), female, moderate (73.62%), good (5.08%) (Ali et al., 2013), in Debark District in males (64.6%) in females (54.5%) (Yalemebrat et al., 2016). This difference might be due to increased activity of males in their daily life compared with females and better chance of acquiring correct information about rabies.
The residence of respondents was also found to be significantly associated with higher good KAP score in which respondents from urban were 5.5 time more likely to have higher good score than urban residents. This could be explained by the fact that urban respondents have better information access than rural. Moreover, the odds of higher good KAP score in elementary, secondary, college level and university level were 11.2, 32.8, 15.5 and 24.24 times more likely than illiterate. This finding was also supported by a study conducted in Bahir Dar (Guadu et al., 2014), in Addis Ababa (Ali et al., 2013) and the studies conducted in Flagstaff, Arizona, USA (Andrea and Jesse, 2012). This could be due to the fact that educated person have better information access and can easily understand the disease.
The other factor significantly (P=0.005) associated with KAP score was dog bite experience The participant who experienced dog bite were 7.37 time more likely to have higher good KAP score than those did not experienced dog bite. The possible explanation for this could be that individual who experienced dog bite would seek for information regarding the consequences of dog to save him/or self. Moreover, dog owners and participants who were trained about rabies were 7.53 and 18.62 time more likely to have higher good KAP score than none dog owners and untrained participants, respectively. The statistical significant difference (p= 0.003) in KAP score between dog owners and non-dog owners could be attributed to the fact that dog owners has a better chance to know more about dog and dog disease. Furthermore, the statistical significant difference between trained and untrained could be attributed to significance of training in raising the community awareness. This finding was also supported by many scholars who mentioned awareness level as important tool to control rabies (Eshetu et al., 2002; Wudu et al., 2013).
This study revealed that rabies is a well-known and significant disease of both human and animals in the study area. Almost all (99.3%) participants had heard about rabies and 88.7% of them knew its zoonotic significance. 18.0 and 70.0% of the participants had encountered rabid human(s) and animal(s), respectively at least once in their life. Thus, rabies should be prioritized and targeted as a more serious public health burden and animals too. Even though the majority (57.3%) of the participants in this study have good KAP score about rabies there were some knowledge gap observed regarding the cause, transmission incubation period and prevention methods of rabies. This reflects the urgent need for rabies awareness programmes within the community. Increasing community knowledge is particular needed regarding wound washing after animal bite as first aid and seeking post-exposure prophylaxis other than traditional and spiritual healer. This study also demonstrates the need for awareness creation to the community regarding dog vaccination and implementation of dog vaccination with proper management. Above all to realize the available of preventative options, the close collaboration of public health and veterinary sector has a paramount role. Thus there should be strong linkage between all stake holders including local authority.
The authors have not declared any conflict of interests.
REFERENCES
|
Abera E, Assefa A, Belete S, Mekonen N (2015). Review on Rabies, with Emphasis on Disease Control and Eradication Measures. Int. J. Bas Appl. Vir. 4(2):60-70.
|
|
|
|
Ali A, Yimer EA, Sifer D (2013). A study on knowledge, attitude and practice of rabies among residents in Addis Ababa, Ethiopia. Ethiop. Vet. J. 17(2):19-35.
Crossref
|
|
|
|
|
Andrea M, Jesse D (2012). Community Survey after Rabies Outbreaks, Flagstaff, Arizona, USA. Emerg. Infect. Dis. 18(6):932-938.
|
|
|
|
|
Arsham H (2005). Questionnaire design and surveys sampling, 9th ed.
View (Retrieved 2017).
|
|
|
|
|
Blackmore C (2014). Rabies Prevention and Control in Florida, Division of Disease Control and Heal the Protection. P 122.
|
|
|
|
|
Chernet B, Nejash A (2016). Review of Rabies preventions and control. Int. J. Life Sci. 4(2):293-301.
|
|
|
|
|
CSA (2016). Federal Democratic Republic of Ethiopia Central Statistical Agency. Population Projection of Ethiopia for All Regions at Wereda Level from 2014 - 2017. Addis Ababa
|
|
|
|
|
Depani SJ, Kennedy N, Mallewa M, Molyneux EM (2012). Case report: Evidence of Rise in Rabies Cases in Southern Malawi – Better Preventative Measures Are Urgently Required. Malawwi Med. J. 24(3):61-64.
|
|
|
|
|
Dhand NK, Rai BD, Tenzin S, Tsheten K, Ugyen P, Singye K, Ward MP (2012). Community-based study on knowledge, attitudes and perception of rabies in Gelephu, south-central Bhutan. Int. Health 4(3):210-219.
Crossref
|
|
|
|
|
Digafe RT, Kifelew LG, Mechesso AF (2015). Knowledge, attitudes and practices towards rabies: questionnaire survey in rural household heads of Gondar Zuria District, Ethiopia. BMC Res. Notes 8(400):2-7.
Crossref
|
|
|
|
|
Eidson M, Kate S, Mary K, Charles T, Amy W (2004). Development and evaluation of bat rabies education materials. Evid. based Prev. Med. 1(2):85-91.
|
|
|
|
|
Eshetu Y, Bethelehem N, Girma T, Yared M, Yosef B, Badeg Z, Mekoro B, Abebe B (2002). Situation of rabies in Ethiopia: A retrospective study 1990-2000. Ethiop. J. Health Dev. 16(1):105-112.
|
|
|
|
|
Fekadu M (1997). Human rabies surveillance and control in Ethiopia. In: Proceedings of the Southern and Eastern Africa Rabies Group Meeting, Nairobi, Kenya.
|
|
|
|
|
Gebeyaw S, Teshome D (2016). Study on Community Knowledge, Attitude and Practice of Rabies in and Around Dessie City. Austin J. Vet. Sci. Anim. Husb. 3(1):1020.
|
|
|
|
|
Guadu T, Shite A, Chanie M, Bogale B, Fentahum T (2014). Assessment of knowledge, attitude and practices about rabies and associated factors: in the case of Bahir Dar town. Global Vet. 13(3):348-54.
|
|
|
|
|
Jemberu WT, Molla W, Almaw G, Alemu S (2013). Incidence of Rabies in Humans and Domestic Animals and People's Awareness in North Gondar Zone, Ethiopia. PLoS Negl. Trop. Dis. 7(5):e2216.
Crossref
|
|
|
|
|
Kabeta T, Deresa B, Tigre W, Ward MP, Mor SM (2015). Knowledge, attitudes and practices of animal bite victims attending an anti-rabies health center in Jimma Town, Ethiopia. PLoS Negl. Trop. Dis. 9(6):e0003867.
Crossref
|
|
|
|
|
Livestock Development and Health office of Munesa woreda (LDHOMW) (2012). Livestock Development and Health office of Munesa woreda.
|
|
|
|
|
Liu W, Liu Y, Liu J, Zhai J, Xie Y (2011). Evidence for inter- and intraclade recombinations in rabies virus. Infect. Gen. Evol. 11:1906-1912.
Crossref
|
|
|
|
|
Matsumoto T, Yamada K, Noguchi K, Nakajima K, Takada K, Khawplod P, Nishizono A (2010). Isolation and characterization of novel human monoclonal antibodies possessing neutralizing ability against rabies virus. Microb. Immunol. 54(11):673-683.
Crossref
|
|
|
|
|
Nilsson M (2014). Effect on rabies education program on rabies awareness, attitudes towards dogs and animal welfare among children in Lilongwe, Malawi. Epsilon, Examensarbete 2014:26.
|
|
|
|
|
OIE (2012). Manual of diagnostic tests and vaccines for terrestrial animals. OIE Rabies.
|
|
|
|
|
Pankhrust R (1990). An introduction to the medical history of Ethiopia. The Red Sea Press. Inc. Trenton, New Jersey. pp. 93-101.
|
|
|
|
|
Radostits OM, Gay CC, Hinchcliff KW, Constable PD (2007). Veterinary medicine: a textbook of the diseases of cattle, horses, sheep, pigs and goats.10thed. London. Saunders. pp. 1384-1394.
|
|
|
|
|
Rupprecht CE, J. Barrett D, Briggs F, Cliquet A, Fooks R, Lumlertdacha B, Tordo N (2007). Can rabies be eradicated? Dev. Biol. 131:95-121.
|
|
|
|
|
Sambo M, Lembo T, Cleaveland S, Ferguson HM, Sikana L, Simon C, Hampson K (2014). Knowledge, attitudes and practices (KAP) about rabies prevention and control: a community survey in Tanzania. PLoS Negl. Trop. Dis. 8(12):e3310.
Crossref
|
|
|
|
|
Schnell MJ, McGettigan JP, Wirblich C, Papaneri A (2010). The cell biology of rabies virus: using stealth to reach the brain. Nature Rev. Microbiol. 8:51-61.
|
|
|
|
|
Serebe SG, Tadesse KA, Yizengaw HA, Tamrat SM (2014). Study on community knowledge, attitude and practice of rabies in and nearby Gondar town, North West Ethiopia. J. Public Health Epidemiol. 6(12):429-435.
|
|
|
|
|
Singh SU, Choudhary SK (2005). Knowledge, attitude, behavior and practice study on dog-bites and its management in the context of prevention of rabies in a rural community of Gujarat. Indian J. Commun. Med. 30(3):81-83.
Crossref
|
|
|
|
|
Teklu GG, Hailu TG, Eshetu GR (2017). High Incidence of Human Rabies Exposure in Northwestern Tigray, Ethiopia: A Four-Year Retrospective Study. PLoS Negl. Trop. Dis. 11(1):e0005271.
Crossref
|
|
|
|
|
Tiembre I, Vroh BBJ, Kouassi P, Attoh-Touré H, Ekra KD, Diane A, Tagliante-Saracino J (2014). Knowledge, attitudes and practices of household heads regarding rabies in the Abobo district (Abidjan, Côte d'Ivoire) in 2008. Sante publique (Vandoeuvre-les-Nancy, France). 26(4):547-553.
|
|
|
|
|
Tschopp R, Bekele S, Aseffa A (2016). Dog demography, animal bite management and rabies knowledge-attitude and practices in the Awash Basin, Eastern Ethiopia. PLoS Negl. Trop. Dis. 10(2):e0004471.
Crossref
|
|
|
|
|
WHO (World Health Organization). (2013). WHO Expert Consultation on Rabies: second report (No. 982). World Health Organization.
|
|
|
|
|
Wudu T, Wassie M, Gizat A, Sefinew A (2013). Incidence of rabies in humans and domestic Animals and People's Awareness in North Gondar Zone, Ethiopia. J. PLOS Negle. Trop. Dis. 7(5):2216.
Crossref
|
|
|
|
|
Yalemebrat N, Bekele T, Melaku M (2016). Assessment of public knowledge, attitude and practices towards rabies in Debark Woreda, North Gondar, Ethiopia. J. Vet. Med. Anim. Health 8(11):183-192.
|
|
|
|
|
Yimer E, Neway B, Girma T, Mekonnen Y, Yoseph B, Badeg Z (2002). Situation of rabies in Ethiopia: a retrospective study 1990-2000. Ethiop. J. Health Dev. 16(1):105-112.
Crossref
|
|
|
|
|
Yin CP, Zhou H, Wu H, Tao XY, Rayner S, Wang SM, Liang GD (2012). Analysis on factors related to rabies epidemic in China from 2007.2011. Virol. Sci. 27(2):132-143.
|
|
|
|
|
Yousaf M, Qasim M, Zia S, Khan MR, Ashfaq UA, Khan S (2012). Rabies molecular virology, diagnosis, prevention and treatment. Virol. J. 9(1):1.
Crossref
|
|
|
|
|
Zhao XL, Yin J, Chen WQ, Jiang M, Yang G, Yang ZH (2008). Generation and characterization of human monoclonal antibodies to G5, a linear neutralization epitope on glycoprotein of rabies virus, by phage display technology. Microb. Immunol. 52:89-93.
Crossref
|
|