Full Length Research Paper

ABSTRACT
Child malnutrition is a public health problem in Côte d’Ivoire. The persistence of malnutrition, sometimes looking like an epidemic, seems contradictory in view of the many natural potentialities available in the Health Care District of Danané. The level of rainfall conducive to cereal production is satisfactory; this should normally guarantee minimum food availability. Through this work, we aim to understand the factors associated with malnutrition among children under five in the Health Care District of Danane in order to identify and implement the best prevention and control strategies. Using a case-control study (n =109 cases and n =218 controls), we performed a logistic regression model to identify factors associated with child malnutrition (z-score < -2) at the level of child, households, and of person in charge of the child, in the Health Care District of Danané from January 1st to March 31st, 2017. Odds ratio (OR) of child malnutrition were significantly high in the presence of over one child under 5 in a household (OR=3.05, 95%CI [1.34-6.91]; p ?0.01), of influenza episodes (OR=3.48, 95%CI [2.10-6.80], p ?0.01), of diarrhea (OR=2.56, 95%CI [1.30-5.05]; p ?0.01), and non-drinking water consumption OR=1.37, 95%CI [1.17-2.48]; p ?0.01). The care of the child by his/her biological mother, progressive weaning, exclusive breastfeeding, deworming, age of the person in charge of the child (≥25 years), were significantly protective factors. Promoting family planning, hygiene, and the strengthening of gradual weaning, exclusive breastfeeding and deworming could help reduce child malnutrition in Health Care District of Danané.
Key words: Infant malnutrition, odds ratio, logistic regression, case control.
INTRODUCTION
Malnutrition is characterized by insufficient or excessive intake of protein, energy and micronutrients. According to united nation inter-agency Group for Child mortality estimation (UN-IGME), nearly half of deaths in under five children are associated to undernutrition (United Nations Inter-agency Group for Child Mortality and IGME), 2017).
Severe acute malnutrition affects nearly numerous children, the majority of whom live in sub-Saharan Africa and South-East Asia. It is a major factor in a third of the deaths occurring in children under 5 worldwide, the number of which reaches almost 8 million each year (UNICEF et al., 2020).
Côte d'Ivoire, like other sub-Saharan countries, is not an exception. Indeed, surveys conducted in the country have shown that malnutrition is ubiquitous (Ernest et al., 2016; Tano et al., 2010). In 2016, according to World Health Organization (WHO), 20.9% of children under 5 were underweight, while 14% were wasted in Côte d'Ivoire (Organisation Mondiame De La Santé, 2016).
To fight against this scourge, the country political leaders have set up since 2001, a national nutrition Program. Despite efforts made by the program, malnutrition remains a public health problem in Côte d'Ivoire. In fact, according to the 2011-2012 Demographic and Health Surveys Multiple Indicators Cluster Surveys (DHS-MICS), the prevalence of growth stunting went from 34% (UNICEF Côte D’Ivoire, 2006) to 29.8% (Mosso et al., 2012). Despite the nearly 4-point percent decline, this figure can be deemed "critical" especially in the northern and western areas where the prevalence reached 40% (MSLS, 2013).
Unfortunately, the Health Care District of Danané is concerned by this situation. Indeed, Danané is one of the districts of the Tonpki Health Region most affected by malnutrition with an incidence of 24.2% in 2012, 11.4% in 2013, 29% in 2014, and 35 % in 2015 (Ministère de la santé et de l’hygiène publique, 2017). However, the rainfall favorable to cereal production is satisfactory (République de Côte d’Ivoire, 2015); this should normally guarantee minimum food availability. This is not always the case because according to World Food Program (WFP) and Food and Agriculture Organization (FAO), the prevalence of global food insecurity (moderate and severe) is 20% in this area (République de Côte d’Ivoire, 2015).
For many children, the lack of access to food is not merely the cause of malnutrition. Poor dietary practices and infections, or even the combination of both, also contributes to this phenomenon. Infections, including persistent or frequent diarrhea, pneumonia, measles and malaria, compromise the nutritional status (WHO, 2016). To our knowledge, no study on this specific aspect has been carried out in the Health Care District of Danané. Through this work, Health Care District of Danane aim to understand the factors associated with malnutrition among children under five in order to identify and implement the best prevention and control strategies.
MATERIALS AND METHODS
Study design
A case-control study was conducted from January 1 to March 31, 2017 in the Health Care District of Danané in Côte d’Ivoire. The District is located in the western part of Côte d'Ivoire, more than 650 km from Abidjan. It is bordered to the East by the health care districts of Man and Bangolo, Guinea and Liberia to the West, Health District of Biankouma to the North and the Health District of Zouan Hounien to the South. The study was conducted in 18 out of the 21 public health institutions in the Health Care District of Danané involved in nutrition activities.
Definition of cases and controls
Inclusion criteria
We considered as a case : i) any child under 5 years old residing for more than one month in the Health Care District of Danané; ii) those who were received in the health centre (either for a consultation or referred by an CHW, for vaccination or weighing), and diagnosed with malnutrition with a z-score < -2 standard deviations (SD) of WHO reference median for weight-for-height and accompanied by his mother or caregiver (WHO Expert Committee on Physical Status, 1995; World Health Organization, 1997).
We considered the controls: i) as any child under 5 years old residing for more than one month in the Health Care District of Danané; ii) those who were received in the health Centre (either for a consultation or referred by a CHW, for vaccination or weighing), with z-scores ≥ -2 SD for the weight-for-height of children (WHO Expert Committee on Physical Status, 1995; World Health Organization, 1997).
Given the short period of the study that did not correspond to the peak of onset of malnutrition cases, one case for two controls was not only considered but also, did not match the controls with cases. The sample size was calculated using the Open Epi software (version 3). For a 95% confidence level, 80% power, an extreme minimum odds ratio of 2, a hypothetical proportion of controls with 40% exposure, 323 individuals was computed (108 cases and 216 controls) using Fleiss’ method and applied a continuity correction. Sample was done by convenience. Cases and controls were included progressively according to the availability of the investigators. For each centre, two recruitment positions were set up (consultation and vaccination). At each level, children are weighed first. As a result of weighing, any child with a Z-score ? -2 SD is considered as a case (WHO and UNICEF, 2009). His/her controls were identified by considering the first two children with a Z score ≥ 2 SD among the children who were received following the case.
Tools, data collection technique and data analysis
Variables was collected related to the characteristics of the child (age, sex, weight, height, living environment, breastfeeding, type of weaning, vaccination status, history of diarrhea, influenza, fever, deworming, vitamin A supplementation), the characteristics of the person in charge of the child (biological mother, adoptive mother, other person and for each age, level of education, occupation, marital status), and household characteristics (number of persons in the household, number of children under 5 in the household, presence of latrines, source of water supply, number of daily meals in the household). Face-to-face interviews were conducted with the parents of the children using a standardized questionnaire.
The data were entered into the Epi info 7.2 software. Descriptive analyses was conducted (by calculating frequencies, proportions and the median), a bivariate analysis (by calculating odds ratios and their confidence intervals), and a multivariate analysis by performing a simple and multiple logistic regression model. Variables for which p-values of association with malnutrition were ? 0.20 were included in the multivariate model. Finally, a threshold of significance p ? 0.05 was considered for all statistical analyses. The Ministry of Health of Côte d'Ivoire approved the study protocol (007/MSHP/DGS/INHP/BBVJ-KMM). Informed consent was obtained from parents or guardians of children before each interview. Confidentiality was ensured by the storage of data obtained in a password protected computer; only de-identified data was analyzed and disseminated.
RESULTS
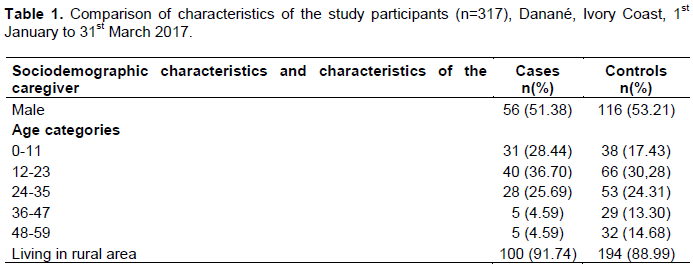
In our study, the median age (interquartile range) of malnourished children is 18 months (14 - 24). For controls, the median age is 23 months (11 - 36). The median age of person in care of the child was 28 (21-35) and 27-year-olds (24-32) for cases and controls respectively (Table 1).
Factors associated with malnutrition
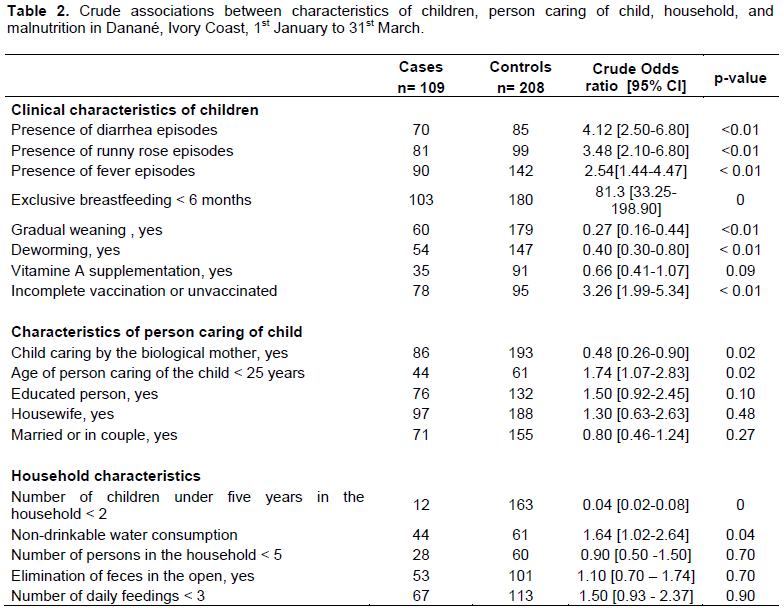
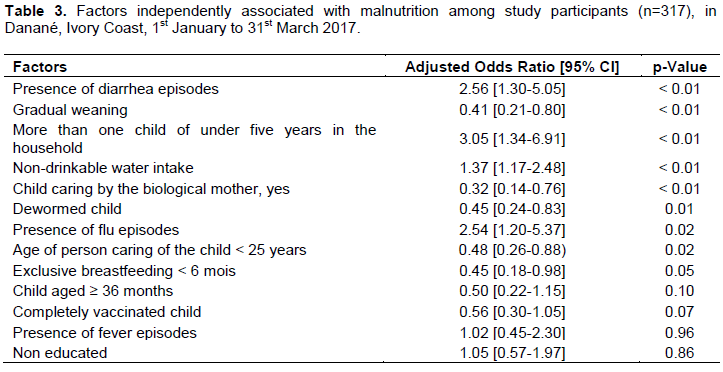
Table 2 shows that incompletely or unvaccinated children are associated with malnutrition (OR= 3.26, 95%CI [1.99-5.34]; p ?0.01. Also, deworming, being cared for by the biological mother or a person of at least 25 years of age were protective against malnutrition (Table 2). In terms of household characteristics, the presence of less than one child under 5 years compared to more than one child protected against malnutrition in univariate analysis (Table 2) and this was confirmed in the multivariate analysis (3.05 [1.34-6.91] p ?0.01 Table 3). In addition, the crude and adjusted analyses show caring by the biological mother, progressive weaning, exclusive breastfeeding of at least 6 months, child deworming or caring by a person of at least 25 years old, significantly protected against malnutrition (Tables 2 and 3). In contrast, consumption of non-drinking water is independently associated with malnutrition (OR=1.37, 95%CI [1.17-2.48]; p ?0.01) (Table 3). Similarly, influenza episodes (OR=3.48, 95%CI [2.10-6.80], p ?0.01), and diarrhea (OR=2.56, 95%CI [1.30-5.05]; p ?0.01), were associated to malnutrition (Table 3).
DISCUSSION
This study showed that the repeated presence of flu and diarrhea were statistically significantly factors associated with malnutrition among children of under five years old. Regarding infectious diseases, the current results corroborate those of studies carried out in Malaysia, India, Burkina Faso, Senegal (Aouehougon, 2007; Basit et al., 2012; LO, 2011; Wong et al., 2014). This could be explained by throat irritation during flu with consequent difficulty of feeding in children (World Health Organization, 2017a). Episodes of diarrhea also deprive children from nutrients required for their growth (World Health Organization, 2017b).
Non-potable water consumption was associated with child malnutrition. Consumption of non-potable water could increase the occurrence of infections, including diarrhea. This result is similar to those found in cross-sectional studies conducted in Côte d'Ivoire, Senegal, and in the Democratic Republic of Congo respectively, in children under five years (Tano et al., 2010; LO, 2011; Mukalay et al., 2010). In Ethiopia, a study (Soboksa et al., 2019) found that the occurrence of childhood diarrhea, increased among children whose families did not treat drinking water at home. However, a study carried out in Ethiopia revealed, "That a source of potable water for consumption was not significantly associated with acute malnutrition» (van Cooten et al., 2019).
Our study showed that deworming protects children against malnutrition. According to Stephenson (1994), treatment of children with whipworm improves hematocrit, growth rates and anthropometry, and serum albumin, and reduces diarrhea and bacterial and protozoan infections in the bowel (Stephenson, 1994). A systematic and regular deworming program must be done for children under 5 years old.
Exclusive breastfeeding was a protective factor for malnutrition in children. This result is in line with the studies conducted respectively in Côte d'Ivoire, India and Morocco, which showed that the lack of exclusive breastfeeding was associated with malnutrition (Basit et al., 2012; Tano et al., 2010; Triki, 2013). Exclusive breastfeeding protects children against infectious and chronic diseases. It speeds up recovery in case of disease (Kramer et al., 2015). According to Jarpa et al. (2015) it was found that predominantly breastfeeding during the first 6 months of life acted as a protective factor against malnutrition (Jarpa et al., 2015). For Uwaezuoke, the preponderance of current evidence strongly suggests that exclusivity in breastfeeding can prevent the development of obesity in children (Uwaezuoke et al., 2017).
All families should adopt exclusive breastfeeding up to 6 months in order to reduce infant morbidity and mortality.
This study showed that progressive weaning was a protective factor against malnutrition. This result is in line with that of the study conducted by Senegalese author (LO, 2011). Progressive weaning of children would give them enough time to adapt to the new diet. Our study showed the presence of more than one child under five years in the household was associated with malnutrition. This result is compliant with other findings from studies in Côte d'Ivoire and Burkina-Faso(Aouehougon, 2007; Ernest et al., 2016). While caring for a child under five is difficult, caring for more than one child under five years old in the context of widespread poverty will be much more difficult and could lead to poor care.
The age of at least 25 years of the caregiver is a protective factor of malnutrition. This result is in line with the studies conducted by Ernest et al. (2016), Owor et al. (2000) and Remonja et al. (2016) in Côte d'Ivoire, Uganda and Madagascar (Ernest et al., 2016; Owor et al., 2000; Remonja et al., 2016). The older mother would be more experienced in caring for children than young mothers. In addition, this study shown being biological mother is a protective factor against malnutrition. Biological mother would be physiologically, psychologically and economically more prepared for the reception and care of the child.
Limitations
The difficulty to match cases to controls which may have resulted in a selection bias was the major limitation of our study. Three from the expected 21 centers did not participate in the study. Two out of the three were not able to collect data and one out of the three were not able to send the data in time for this analysis. Possible influence on the findings could not be excluded. However, as the majority of the centers were included, the influence of the three centres on the findings could be mitigated. Similarly, the reasoned sampling makes that we cannot generalize our results to the entire population of the Health Care District of Danané.
CONCLUSION
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Aouehougon O (2007). La malnutrition proteino-energetique et ses facteurs de risque chez les enfants de moins de 5 ans dans le district sanitaire de Tougan. |
|
|
Basit A, Nair S, Chakraborthy KB, Darshan BB,Kamath A (2012). Risk factors for under-nutrition among children aged one to five years in Udupi taluk of Karnataka, India: A case control study. The Australasian medical journal 5(3):163-167 |
|
|
Ernest AK, Sonia-estelle E, Gustave KK, Guy-alexandre ZBF (2016). Facteurs socio-démographiques et risque de la malnutrition protéino-énergétique chez les enfants , de 0 à 59 mois , fréquentant l ' Hôpital |
|
|
Général de Bingerville ( Côte d ' Ivoire ) [Socio-demographic factors and risk of protein energy malnutrition in c. International Journal of Innovation and Applied Studies 17(3):884-892. |
|
|
Jarpa MC, Cerda LJ, Terrazas MC, Cano CC (2015). [Breastfeeding as a protective factor against overweight and obesity among pre-school children]. Revista Chilena De Pediatria 86(1):32-37. |
|
|
Kramer MS, Chalmers B, Hodnett ED, Vanilovich I, Mezen I (2015). Promotion of Breastfeeding. JAMA - Journal of the American Medical Association 285(4). |
|
|
Lo AF (2011). Facteurs explicatifs de la fréquence de la malnutrition chez les enfants à¢gés de 0 à 5 ans dans la communauté rurale de |
|
|
Nguène Sarr au Sénégal-Amadou Fall LO. Memoire Online. |
|
|
Ministère de la santé et de l'hygiène publique. (2017). Rapport annuel sur la situation sanitaire 2016. |
|
|
Mosso RA, Dore EDA, Kouakou HA, Assi SB, Bakayoko M, Bakayoko Y, Coulibaly M, Gbane M, N'Zi E, Salam G, Sika L, Yao EK, Busangu MF(2012). Enquête démographique et de santé et à indicateurs multiples (eds-mics). 591. |
|
|
Mukalay AW, Kalenga PM, Dramaix M, Hennart P, Schirvel C, Kabamba LM, Donnen P (2010). Facteurs prédictifs de la malnutrition chez les enfants âgés de moins de cinq ans à Lubumbashi (RDC). Santé Publique 22(5):541-550. |
|
|
M. de la S. et de la L. contre le S, MSLS (2013). Enquête Démographique et de Santé à indicateurs Multiples (EDS-MICS) 2011-2012. |
|
|
Organisation mondiame De La Santé, B. Régional De l'Afrique. (2016). Atlas of African Health Statistics. WHO regional Office for Africa. |
|
|
Owor M, Tumwine JK, Kikafunda JK (2000). Socio-economic risk factors for severe protein energy malnutrition among children in Mulago Hospital, Kampala 77(9):471-475. |
|
|
Remonja C, Rakotonirainy N, Mangahasimbola R, Piola P, Randremanana R (2016). Déterminants de la malnutrition chronique à Moramanga, Madagascar. Revue d'Epidémiologie et de SantécPublique, 64:S209. |
|
|
République de Côte d'Ivoire. (2015). Analyse de la situation nutritionnelle en côte d'Ivoire, Rapport Juillet 2015. |
|
|
Soboksa NE, Hailu AB, Gari SR, Alemu BM (2019). Water supply, sanitation and hygiene interventions and childhood diarrhea in Kersa and Omo Nada districts of Jimma Zone, Ethiopia: A comparative cross-sectional study. Journal of Health, Population and Nutrition 38(1):45. |
|
|
Stephenson LS (1994). Helminth parasites, a major factor in malnutrition. World Health Forum 15(2):169-172. |
|
|
Tano OA, Tiembré I, Konan YE, Donnen P, Dagnan S, Koffi K, Diarra-nama A, Dramaix M, Publique SFSPS (2010). Malnutrition chronique chez les enfqnts de moins de cinq ans au Nord de la Côte d'Ivoire. Santé Publique 22(2):213-220. |
|
|
Triki S (2013). Mémoire de fin d ' études Etude de prévalence et des déterminants de la préscolaire de la ville de Kenitra. |
|
|
UNICEF Côte D'Ivoire. (2006). Enquête par grappes à indicateurs multiples Côte D'Ivoire. |
|
|
UNICEF, WHO, WB (2020). Levels and trends in child mortality. https://www.unicef.org/media/79371/file/UN-IGME-child-mortality-report-2020.pdf.pdf |
|
|
United Nations/Inter-agency Group for Child Mortality (IGME/UN) (2017). 'Levels & Trends in Child Mortality: Report 2017, Estimates Developed by the UN Inter-agency Group for Child Mortality Estimation. |
|
|
Uwaezuoke SN, Eneh CI, Ndu IK (2017). Relationship Between Exclusive Breastfeeding and Lower Risk of Childhood Obesity: A Narrative Review of Published Evidence. Clinical Medicine Insights. Pediatrics 11, 1179556517690196. |
|
|
van Cooten MH, Bilal SM, Gebremedhin S, Spigt M (2019). The association between acute malnutrition and water, sanitation, and hygiene among children aged 6-59 months in rural Ethiopia. Maternal and Child Nutrition 15(1), e12631. |
|
|
WHO Expert Committee on Physical Status (1995). The use and interpretation of anthropometry Physical Status: Report of a WHO Expert Committee. WHO Technical Report Series No. 854. |
|
|
WHO, UNICEF (2009). Normes de croissance OMS et identification de la malnutrition aiguë sévère chez l'enfant: Déclaration commune de l'Organisation mondiale de la Santé et du Fond des Nations Unies pour l'Enfance. |
|
|
World Health Organization (WHO) (2016). Santé de la mère, du nouveau-né, de l'enfant et de l'adolescent: Malnutrition. |
|
|
World Health Organization (WHO) (1997). WHO Global Database on Child Growth and Malnutrition. |
|
|
World Health Organization (WHO) (2017a). Grippe Saisonnière. |
|
|
World Health Organization (WHO). (2017b). maladies Diarrhéiques: Prinicoaux faits. |
|
|
Wong HJ, Moy FM, Nair S (2014). Risk factors of malnutrition among preschool children in Terengganu, Malaysia: A case control study. BMC Public Health 14(785):1-10. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


