Full Length Research Paper

ABSTRACT
Undernutrition is a leading cause of child mortality, especially among indigenous peoples worldwide. Understanding associated predictors is essential for mitigation strategies. This review was undertaken to identify existing literature on the determinants of undernutrition among under-five indigenous children in developing countries, and to reveal existing knowledge gaps. Using relevant terms, we searched for relevant literature from PubMed, Medline, Scopus, and Google scholar databases, WHO and UNICEF websites, and reference lists of included studies from 2009 to 2019. Of the 10 records that met the eligibility criteria, 4, 3, 2, and 1, were conducted in Brazil, India, Guatemala and Malaysia, respectively. Seven were cross-sectional, studies, 2 were population-based studies and 1 a mixed-method studies. All studies included under-five children, ranging in sample size from 74 to 6075. Regarding anthropometric indicators, study 1 focused on anaemia, 2 on wasting, 3 on underweight, and 8 focused on stunting. Factors associated with undernutrition were maternal educational status, maternal stunting, health care seeking behaviour, child age, child sex, child morbidity status, socio-economic status, inadequate water quality, hygiene and sanitation conditions. These results are relevant in informing undernutrition-reduction policies and interventions among indigenous populations in developing countries. The study revealed a paucity of research, particularly, in Africa where no study was identified.
Key words: Under nutrition, risk factors, under-five children, indigenous, developing countries.
Abbreviation: UNICEF, United Nations International Children’s Educational Fund; WHO, World Health Organization; SDG, sustainable development goals; CI, confidence interval; OR, odd ratio; AOR, adjusted odd ratio; PR, prevalence ration; WASH, water, sanitation and hygiene.INTRODUCTION
Worldwide, malnutrition accounts for more than 45% (Black et al., 2013)of an estimated 5.6 children who die before their fifth birthday annually, 80% of deaths occurring in sub-Saharan Africa (SSA) and Asia (Vakili et al., 2015).
Besides being a leading cause of child morbidity and mortality, malnutrition, especially undernutrition impairs child normal growth and development, school performance and economic productivity in adulthood (Victora et al., 2008). Hence, ending all forms of malnutrition by 2030 in resonance with the Sustainable Development Goal (SDG) 2.2 target (United Nations, 2017), will significantly contribute to the achievement of other related child health goals. Malnutrition reduction strategies targeting evidence-based high-risk groups (Sultana et al., 2019)are fundamental in attaining these goals.
Among nutritionally vulnerable population groups are the world’s indigenous peoples, numbering more than 370 million in some 90 countries, and over 14.2 million in 35 countries in the African region (Department of Economic and Social Affairs, United Nations, 2015). Compared to benchmark populations, indigenous peoples experience higher disease burden due to persistent socioâ€economic disadvantages, marginalization and limited access to health services (Department of Economic and Social Affairs, United Nations, 2015; Basnayake et al., 2017). Children in particular, tend to have worse health outcomes and die younger than their non-indigenous peers (Department of Economic and Social Affairs, United Nations, 2015; Anderson et al., 2016; Basnayake et al., 2017). Accordingly, improving the nutritional status of children, and overall health of the indigenous people is one of the global health priorities (Department of Economic and Social Affairs, United Nations, 2015).
Effective malnutrition prevention strategies among vulnerable populations hinge largely on reducing their exposure to contextual risk factors. According to the widely adopted (United Nations Children’s Fund, 1991)conceptual framework, the etiology of malnutrition is complex and multifactorial. In line with the framework, systematic reviews in sub-Saharan Africa (Akombi et al., 2017a)and Southern Asia (Akhtar, 2016)have adequately documented the principal factors that jointly explain malnutrition among under-five children. However, the magnitude and distribution of determinants vary across different geographical regions, populations, and various socio-cultural conditions, due to differences in patterns of food intake, cultural beliefs and access to health care services among others (Motedayen et al., 2019). Moreover, most reviews focused on non-indigenous populations, and related evidence for indigenous populations is scarce. Within this context, this review was undertaken to identify and map existing literature on factors that contribute to childhood anaemia, stunting, wasting and underweight among indigenous population groups in developing countries, and to identify knowledge gaps. This paper presents a narrative synthesis on the topic, drawn from 10 selected studies. To the best authors knowledge, this is the first and most current scoping review on the topic. The results will be relevant in informing undernutrition-reduction policies and interventions among various indigenous population groups. It is worth noting that this study is part of a wider PhD thesis titled “Assessing malnutrition and associated determinants among under-five Indigenous Mbororo children in two health districts of the West Region of Cameroon”.
METHODOLOGY
Information source and search strategy
The study initially highlighted the medical subject headings (MeSH) and text terms related to the concept, context and population to guide an extensive on-line search from PubMed, Scopus and Medline databases. The MeSH and free text terms were used to construct search strings for each database. For example, using the Boolean operators (AND, OR) the following strategy was used for PubMed (Malnutrition OR Undernutr* OR Stunt* OR Wast* OR Underweight OR Anaemia [MeSH]) and (Determinant* OR Predictor OR Risk factor OR Correlate OR Cause [MeSH]) AND (Child* OR Under-five OR Infant OR Pre-school [MeSH]) and Indigenous OR Tribal OR Minority [MeSH]) AND English [lang]. We equally searched for unpublished literature from Google Scholar, World Health Organization (WHO) and UNICEF websites. A manual search for additional literature from the reference lists of selected studies was conducted.
Study selection
Inclusion and exclusion criteria
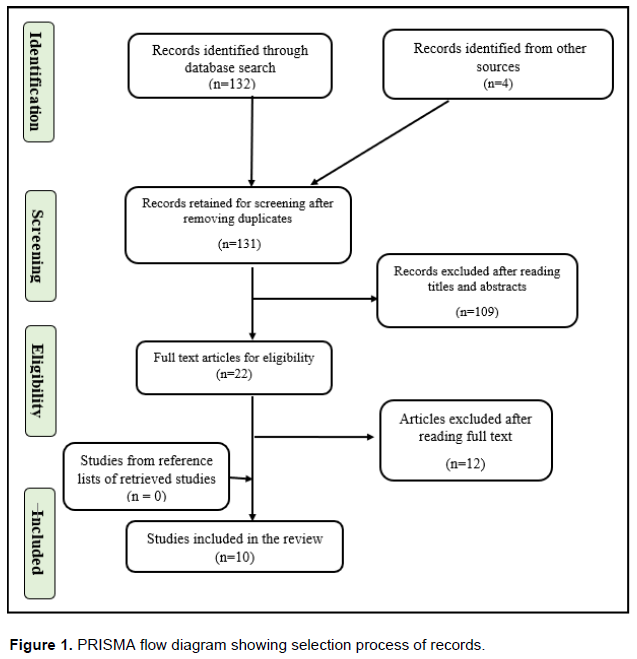
Full articles were considered for review if they reported the determinants of anaemia, stunting, wasting and underweight; focused on indigenous children under five years old were conducted in developing countries; were qualitative, qualitative or mixed-methods studies; and were published in English from 2009 to 2019. Records were excluded for the following reasons: Repeated publications; lack of access to full text of articles; lack of reference to the determinants of malnutrition; non-indigenous children; children above five years; published in languages other than English; books, policy briefs and conference papers; and studies conducted in affluent countries notably: Canada, United States of America and Australia. As presented in the PRISMA flow diagram (Figure 1), 10 of the 136 records which were retrieved met the priori eligibility criteria. Two review authors independently screened the abstracts and full articles using the eligibility criteria.
Data extraction
Data extraction was done using a data extraction template designed by the team and pilot tested on a representative sample of articles. The first author’s surname, year of publication, country, study design, sample size, age of study population, and determinants of anaemia, stunting, wasting and underweight were extracted from included studies. Only risk factors with reported p-values, odd ratios (OR), adjusted odd ratios (AOR) and prevalence ratios (PR) were considered. Data extraction was undertaken independently and in duplicate by two authors with disagreements resolved via consensus. A narrative approach was followed to synthesize the evidences from the reviewed studies.
RESULTS AND DISCUSSION
Characteristics of selected studies
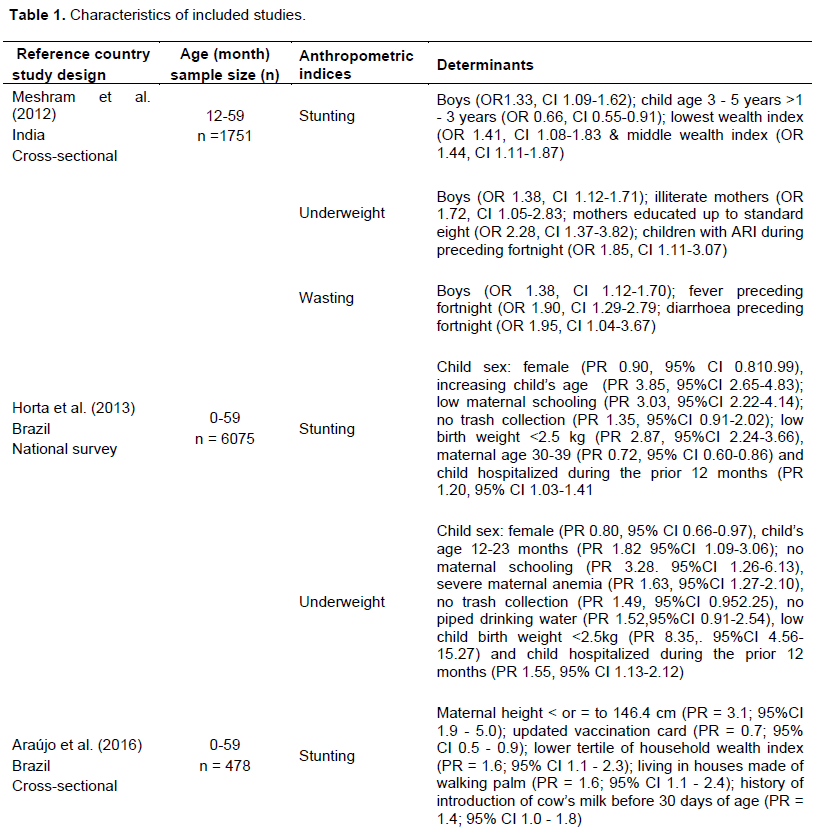
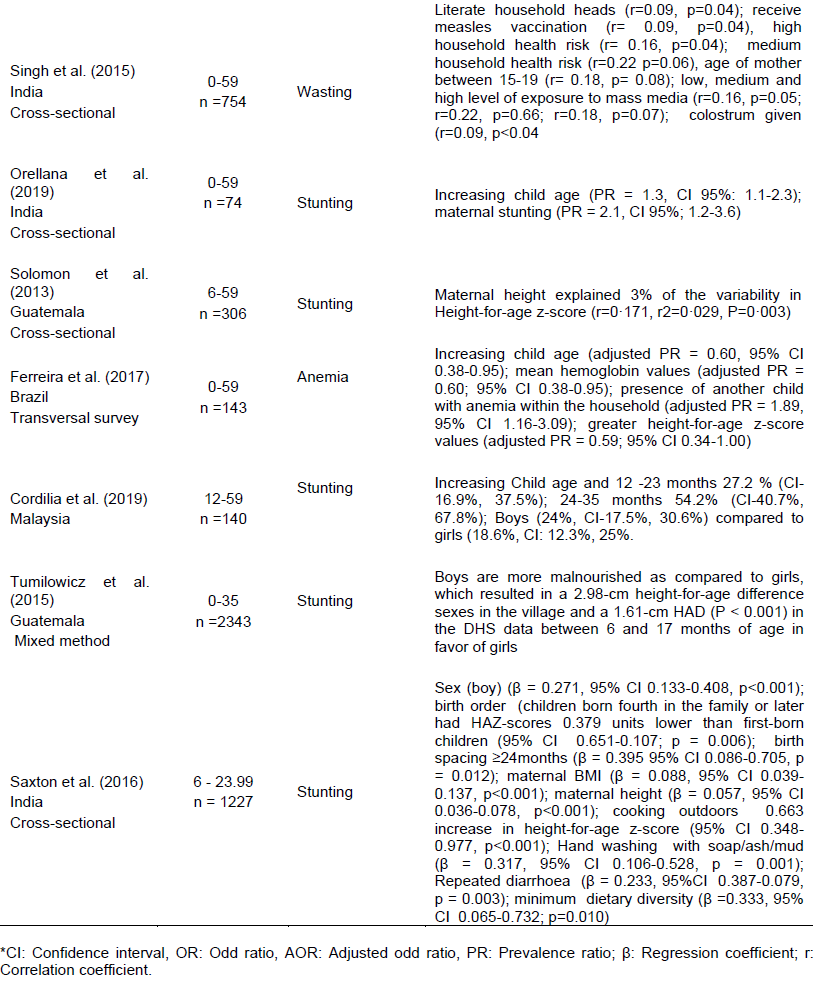
Table 1 presents the characteristics of 10 studies that were selected for the review. Of these, 4 were conducted in Brazil, 3 in India, 2 in Guatemala and 1 in Malaysia. Seven were cross-sectional studies, 2 were population-based studies, and 1 was a mixed method study. All studies focused on children under five years of age, ranging in sample size from 74 to 6075. As concerns anthropometric indicators, 1 study focused on anaemia, while, 2, 3, and 8 studies, respectively, reported on wasting, underweight and stunting.
Risk factors of under nutrition
Reported risk factors were grouped into three main categories namely: Maternal characteristics, child characteristics and household socio-economic characteristics.
Maternal characteristics
Maternal educational status
Low maternal educational status was significantly associated with underweight and stunting in India (Meshram et al., 2012)and Brazil (Horta et al., 2013). The odds of underweight were 1.7 times higher among children whose mothers were illiterates (Meshram et al., 2012), in agreement with a similar study in Ecuador (Walrod et al., 2018), and a systematic review in sub-Saharan Africa (Akombi et al., 2017). The association between maternal formal schooling and child nutritional status finds an explanation in the presumptions that, high maternal education attainment translates into greater health care utilization, adoption of modern medical practices, and child-centered caring practices that improve child nutritional outcomes (Abuya et al., 2012; Duah and Adisah-Atta, 2017). Additionally, maternal education enhances efficient management of limited household resources to provide adequate nutrition for children, and prevent childhood infectious diseases (Walrod et al., 2018). Otherwise, mothers with little or no formal education are more likely to have inadequate child feeding practices, and poor sanitation and hygiene practices (Adhikari et al., 2017). Hence, improvements in access to indigenous women’s education are likely to contribute to better child nutrition outcomes.
Maternal health care seeking behaviour
Maternal health care seeking behaviour which includes utilization of maternal and child health services was reported as a significant determinant of nutritional status of indigenous children. Inadequate pre-natal care significantly predicted stunting in Brazil (Araújo et al., 2016). Meanwhile, child growth monitoring and being up-to-date with the vaccination schedules were inversely associated with stunting (Araújo et al., 2016). In another study in India (Singh et al., 2015), immunization against measles reduced the risk of wasting among under-five children. These relationships are not unexpected, as access to primary health care has proven fundamental to the prevention of maternal and child deaths (Leite et al., 2013; Chomat et al., 2014; Basnayake et al., 2017; Dagnew et al., 2018). Regrettably, accessing health care services is a major problem for indigenous populations worldwide (Department of Economic and Social Affairs, United Nations, 2015). In Africa and Asia in particular, access to healthcare services is limited by several structural, social, economic, linguistic and cultural barriers (Chomat et al., 2014; Department of Economic and Social Affairs, Nations, 2015). Accordingly, mothers may tend to have low levels of health seeking behaviour which contribute to higher rates of child under nutrition, morbidity and mortality. This finding highlights the need to ensure maternal and child health care services that are accessible, affordable, acceptable, adaptable and adequate to meet the needs of the indigenous populations at large.
Maternal height
Low maternal stature (height <145 cm) was highlighted as a significant predictive factor for child stunting in Brazil (Araújo et al., 2016), India (Orellana et al., 2019)and Guatemala (Solomons et al., 2015). Children whose mothers were below 145 cm in height, were twice as likely to be severely stunted compared with their counterparts with taller mothers (Orellana et al., 2019). This finding is consistent with other studies among non-indigenous population groups (Khatun et al., 2018; Khan et al., 2019; Nshimyiryo et al., 2019). The positive association between maternal short stature and child stunting reflects an inter-generational problem (Orellana et al., 2019). Existing evidence suggest that, repeated height deficits for several generations, results in premature births, low birth weights and small-for-gestational age babies (Black et al., 2013; Orellana et al., 2019). The incidence of low birth weight and being small-for-gestational age babies is common among indigenous populations (Gracey and King, 2009). Thus, improving maternal nutritional status before and during pregnancy among the indigenous populations may significantly reduce child linear growth faltering.
Child characteristics
Child age
Child age was invariably associated with anaemia, stunting and underweight (Meshram et al., 2012;Orellana et al., 2019; Ferreira et al., 2017). An inverse relationship was shown between increasing child age and anaemia, as children less than 2 years were at greater risk of moderate and severe anaemia than their older counterparts (Ferreira et al., 2017). Whereas, children above 3 years were 0.66 times less likely to be stunted compared with those below 3 years of age (Meshram et al., 2012), similar to other studies in Malaysia (Anto Cordelia et al., 2019; Orellana et al., 2019), and India (Saxton et al., 2016).The positive correlation between stunting and increasing child age could possibly be attributed to an imbalance between the demand and supply of essential nutrients as children transit from infancy to childhood. This period is characterized by intense growth and physical activity, with correspondingly high needs for nutrients. Unmet nutritional needs during this critical period of growth could lead to poor nutrition outcomes. Additionally, young children unlike infants are more vulnerable to diarrhoea and other gastro-intestinal enteritis due to exposure to microbial contaminants in food and the immediate household environment (Budge et al., 2019). While child age is not a modifiable factor, ensuring adequate age-appropriate feeding, as well as food hygiene practices are crucial measures that could reduce under nutrition burden among indigenous children.
Child sex
Child sex (male) was highlighted as a significant risk factor for anemia in India (Meshram et al., 2012)and Brazil (Ferreira et al., 2017)underweight in Brazil (Horta et al., 2013)and Guatemala (Tumilowicz et al., 2015). Whereas, a study in India (Saxton et al., 2016)showed that girls had higher height-for-age scores than boys, male sex was a predictive factor for stunting in India (Meshram et al., 2012), Brazil (Horta et al., 2013)and Malaysia (Anto et al., 2019). These findings are consistent with a meta-analysis of 17 demographic health surveys in sub-Saharan Africa (Wamani et al., 2007). While this relationship may not be adequately explained, some authors (Akombi et al., 2017b)suggest that females are culturally expected to be less active and stay at home with their mothers near food preparation, while males engage in high physical activities that expend high amounts of energy that would have been channeled into increasing growth. Another school of thought (Singh et al., 2015)posits that, the sex of a child is significant only in settings where there is gender discrimination regarding access to food and other intra-household resources, hence the need for interventions to address such gender inequalities.
Child morbidity status
Fever, diarrhoea and acute respiratory infections (ARI) during the preceding fortnight were significantly associated with under nutrition (Meshram et al., 2012, Horta et al., 2013). Children with ARI were 1.85 times more likely to be underweight compared with their counterparts (Meshram et al., 2012). Similarly, children with fever and diarrhoea were twice at risk of wasting than their peers without any of the conditions. The role of infectious diseases on child nutritional status is well documented (Guerrant et al., 2008; Humphrey, 2009; UNICEF, 2013; Papier et al., 2014; Debnath et al., 2018). Persistent or repeated diarrhoea and infections cause loss of appetite, vomiting intestinal damage, decrease absorption of micronutrients, thereby, leading to under nutrition, which in turn impairs the immune system, thus, worsening the intensity of infections (Ibrahim et al., 2017). Moreover, the presence of infections may cause a shift in energy expenditure to combat the infectious process to the detriment of child growth.
Household socio-economic characteristics
Household income and wealth index
Two studies in India (Meshram et al., 2012; Saxton et al., 2016)revealed that stunting rates were lower among children from middle-income groups compared with those in the lower-income groups. Similarly, a study in Brazil (Horta et al., 2013)reported that children belonging to households with no regular source of income were more likely to be underweight and stunted. A plausible explanation for this relationship could be attributed to the fact that, adequate income increases the ability of households to purchase and access good quality food to meet children’s nutrition needs (Titaley et al., 2019). Thus, poor households are at higher risk of food insecurity and related child growth deficits (Bain et al., 2013). Furthermore, poverty drives families to reside in resource-limited rural and urban slum areas (Goudet et al., 2017)where childhood morbidities are higher (Singh et al., 2011). Globally, indigenous populations are more likely to reside under poor living conditions (Basnayake et al., 2017). Hence, policies and interventions that seek to improve the socio-economic status of poor indigenous households in a sustainable manner are likely to improve the nutritional well-being of their children.
Inadequate water, hygiene and sanitation conditions
Household environmental factors notably the unavailability of piped drinking water, absence of in-door sanitation facilities, and limited access to trash collection services correlated positively with child under nutrition in Brazil (Horta et al., 2013)and India (Singh et al., 2015). This could be explained by the fact that, most endemic diarrheal diseases, intestinal parasite infections, and environmental enteropathies that harm children’s nutritional status are transmitted under conditions of inadequate water, sanitation and hygiene (WASH) (Horta et al., 2013; World Health Organization, 2015; Adhikari et al., 2017; Fatihah et al., 2018). Although access to improved household WASH facilities remains a worldwide problem (World Health Organization, 2015), the issue is more pronounced among indigenous populations (Basnayake et al., 2017; Rajoo et al., 2017; Adhikari et al., 2017). Hence, they tend to have much higher rates of infections than do their non-indigenous counterparts (Gracey and King, 2009). Ensuring adequate access and use of safe drinking-water, personal and environmental hygiene services among indigenous populations are therefore likely to improve child nutritional status.
LIMITATIONS
The results of this study need to be considered in the light of a few limitations. First, the search identified only 10 eligible articles, and none from Africa. This was probably due to bias introduced by examining studies published in the English language only, and for a ten years period. Second, some other factors known to significantly predict child under nutrition such as maternal nutritional status, cultural child feeding practices, and household food security status were not included in the analysis because they were not reported in the reviewed articles.
CONCLUSION
This study reveals that indigenous populations groups share a wide range of interrelated maternal, child, socio-economic and environmental factors that contribute to child under nutrition. The most significant predictors are low maternal educational status, low maternal height, inadequate health seeking behaviour, child sex, child age, child morbidity status, poverty and inadequate water, sanitation and hygiene practices. These findings represent important prevention points, and support holistic multi-sectorial policies and interventions to combat child malnutrition among various indigenous populations groups. Such interventions should be aimed at addressing barriers to formal educational opportunities for the girl child and women, facilitating access to mother and child care health services, promoting adequate maternal nutrition, reducing childhood infectious disease, improving WASH conditions and access to income generating opportunities. The lack of related studies from the African region revealed by this study is equally of great concern. There is therefore need to address such knowledge gaps in order to foster child development and ensure sustainable socio-economic development particularly among the growing numbers of indigenous people in the region.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
This is part of a Ph.D. thesis by Florence Titu Manjong under the supervision of Associate Professors Nsagha Dickson Shey and Thomas Obinchemti Egbe, and Dr. Vincent Siysi Verla, of the Faculty of Health Sciences, University of Buea.
REFERENCES
|
Abuya BA, Ciera J, Kimani-Murage E (2012). Effect of mother's education on child's nutritional status in the slums of Nairobi. BMC Pediatrics 12:80. |
|
|
Adhikari D Khatri RB, Paudel YR, Poudyal AK (2017). Factors Associated with Underweight among Under-Five Children in Eastern Nepal: Community-Based Cross-sectional Study. Frontiers in Public Health 5:350.. |
|
|
Akhtar S (2016). Malnutrition in South Asia-A Critical Reappraisal. Critical Reviews in Food Science and Nutrition 56(14):2320-2330. |
|
|
Akombi, Blessing J, Agho KE, Hall JJ, Wali N, Renzaho AMN, Merom D (2017). Stunting, Wasting and Underweight in Sub-Saharan Africa: A Systematic Review. International Journal of Environmental Research and Public Health 14(8): |
|
|
Akombi BJ, Agho KE, Hall JJ, Merom D, Astell-Burt T, Renzaho AMA (2017). Stunting and severe stunting among children under-5 years in Nigeria: A multilevel analysis. BMC Pediatrics 17(15) |
|
|
Anderson I, Robson B, Connolly M, Al-Yaman F, Bjertness E, King A, Tynan M, Madden R, Bang A, Coimbra Jr CE, Pesantes MA (2016). Indigenous and tribal peoples' health (The Lancet-Lowitja Institute Global Collaboration): A population study. Lancet (London, England), 388(10040):131-157. |
|
|
Anto Cordelia TAD, Sylvia Subapriya M, Hnin PA (2019). Nutritional status and dietary intake of Semai Indigenous children below five years in Perak, Peninsular Malaysia. Malaysian Journal of Public Health Medicine 19(1):84-100. |
|
|
Araújo TS, Oliveira CSM, Muniz PT, Silva-Nunes M, Cardoso MA (2016). Child undernutrition in one of the cities with greater nutritional risk in Brazil: Population-based study in the Western Brazilian Amazon. Revista Brasileira de Epidemiologia 19(3):554-566. |
|
|
Bain LE, Awah PK, Geraldine N, Kindong NP, Sigal Y, Bernard N, Tanjeko AT (2013). Malnutrition in Sub-Saharan Africa: Burden, causes and prospects. Pan African Medical Journal 15. |
|
|
Basnayake LT, Morgan LC, Chang AB (2017). The global burden of respiratory infections in indigenous children and adults: A review. Respirology 22(8):1518-1528. |
|
|
Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, De Onis M, Ezzati M, Grantham-McGregor S, Katz J, Martorell R, Uauy R (2013). |
|
|
Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet (London, England) 382(9890):427-451. |
|
|
Budge S, Parker AH, Hutchings PT, Garbutt C (2019). Environmental enteric dysfunction and child stunting. Nutrition Reviews 77(4):240-253. |
|
|
Chomat AM, Solomons NW, Montenegro GC, Crowley CR, & Bermudez OI (2014). Maternal health and health-seeking behaviors among indigenous Mam mothers from Quetzaltenango, Guatemala. Revista Panamericana de Salud Publica = Pan American Journal of Public Health 35(2):113-120. |
|
|
Dagnew AB, Tewabe T, Murugan R (2018). Level of modern health care seeking behaviors among mothers having under five children in Dangila town, north West Ethiopia, 2016: A cross sectional study. Italian Journal of Pediatrics 44(1):61. |
|
|
Debnath SC, Haque ME, Hasan DMM, Samin S, Rouf MA, & Rabby MF (2018). Undernutrition and Morbidity Profile of Exclusively Breastfeeding Children: A Cross-sectional Study. International Journal of Preventive Medicine 9. |
|
|
Department of Economic and Social Affairs, United Nations (2015). State of the World's Indigenous Peoples, Indigenous Peoples' access to Health Services. |
|
|
Duah HO, Adisah-Atta I (2017). Determinants of health care decision making autonomy among mothers of children under five years in Ghana: Analysis of 2014 Ghana demographic and health survey. Research Journal of Women's Health 4(1):5. |
|
|
Fatihah MS, Gan WY, Sulaiman N, Mohd Shariff Z (2018). Factors associated with stunting among Orang Asli preschool children in Negeri Sembilan, Malaysia. Malaysian Journal of Nutrition 24:215-226. |
|
|
Ferreira AA, Santos RV, Souza JAM, Welch JR, Coimbra Jr CEA (2017). Anemia and hemoglobin levels among Indigenous Xavante children, Central Brazil. Revista Brasileira de Epidemiologia 20(1):102-114. |
|
|
Goudet SM, Kimani-Murage EW, Wekesah F, Wanjohi M, Griffiths PL, Bogin B, Madise NJ (2017). How does poverty affect children's nutritional status in Nairobi slums? A qualitative study of the root causes of undernutrition. Public Health Nutrition 20(4):608-619. |
|
|
Gracey M, King M (2009). Indigenous health part 1: Determinants and disease patterns. The Lancet 374(9683):65-75. |
|
|
Guerrant RL, Oriá RB, Moore SR, Oriá MO, Lima AA (2008). Malnutrition as an enteric infectious disease with long-term effects on child development: Nutrition Review. Nutrition Reviews 66(9):487-505. |
|
|
Horta BL, Santos RV, Welch JR, Cardoso AM, dos Santos JV, Assis AM, Lira PC, Coimbra Jr CE (2013). Nutritional status of indigenous children: Findings from the First National Survey of Indigenous People's Health and Nutrition in Brazil. International Journal for Equity in Health 12:23. |
|
|
Humphrey JH (2009). Child undernutrition, tropical enteropathy, toilets, and handwashing. The Lancet 374(9694):1032-1035. |
|
|
Ibrahim MK, Zambruni M, Melby CL, Melby PC (2017). Impact of Childhood Malnutrition on Host Defense and Infection. Clinical Microbiology Reviews 30(4):919-971. |
|
|
Khan S, Zaheer S, Safdar NF (2019). Determinants of stunting, underweight and wasting among children < 5 years of age: Evidence from 2012-2013 Pakistan demographic and health survey. BMC Public Health 19. |
|
|
Khatun W, Alam A, Rasheed S, Huda TM, Dibley MJ (2018). Exploring the intergenerational effects of undernutrition: Association of maternal height with neonatal, infant and under-five mortality in Bangladesh. BMJ Global Health 3(6). |
|
|
Leite MS, Cardoso AM, Coimbra CE, Welch JR, Gugelmin SA, Lira PC, Horta BL, Santos RV, Escobar AL (2013). Prevalence of anemia and associated factors among indigenous children in Brazil: Results from the First National Survey of Indigenous People's Health and Nutrition. Nutrition Journal 12:69. |
|
|
Meshram II, Arlappa N, Balakrishna N, Laxmaiah A, Mallikarjun Rao K, Gal Reddy C, Brahmam GNV (2012). Prevalence and Determinants of Undernutrition and its Trends among Pre-School Tribal Children of Maharashtra State, India. Journal of Tropical Pediatrics 58(2):125-132. |
|
|
Motedayen M, Dousti M, Sayehmiri F, Pourmahmoudi AA (2019). An Investigation of the Prevalence and Causes of Malnutrition in Iran: A Review Article and Meta-analysis. Clinical Nutrition Research 8(2):101-118. |
|
|
Nshimyiryo A, Hedt-Gauthier B, Mutaganzwa C, Kirk CM, Beck K, Ndayisaba A, Mubiligi J, Kateera F, El-Khatib Z (2019). Risk factors for stunting among children under five years: A cross-sectional population-based study in Rwanda using the 2015 Demographic and Health Survey. BMC Public Health 19(1):175. |
|
|
Orellana JDY, Marrero L, Alves CLM, Ruiz CMV, Hacon SS, Oliveira MW, Basta PC (2019). Association of severe stunting in indigenous Yanomami children with maternal short stature: Clues about the intergerational transmission. Ciência & Saúde Coletiva 24(5): 1875-1883. |
|
|
Papier K, Williams GM, Luceres-Catubig R, Ahmed F, Olveda RM, McManus DP, Chy D, Chau TN, Gray DJ, Ross AG (2014). Childhood Malnutrition and Parasitic Helminth Interactions. Clinical Infectious Diseases 59(2):234-243. |
|
|
Rajoo Y, Ambu S, Lim YAL, Rajoo K, Tey SC, Lu CW, Ngui R (2017). Neglected Intestinal Parasites, Malnutrition and Associated Key Factors: A Population Based Cross-Sectional Study among Indigenous Communities in Sarawak, Malaysia. PLOS ONE 12(1):e0170174. |
|
|
Saxton J, Rath S, Nair N, Gope R, Mahapatra R, Tripathy P, Prost A (2016). Handwashing, sanitation and family planning practices are the strongest underlying determinants of child stunting in rural indigenous communities of Jharkhand and Odisha, Eastern India: A cross-sectional study. Maternal and Child Nutrition 12(4):869-884. |
|
|
Singh A, Pathak PK, Chauhan RK, Pan W (2011). Infant and Child Mortality in India in the Last Two Decades: A Geospatial Analysis. PLoS ONE 6(11). |
|
|
Singh DK, Alagarajan M, Ladusingh L (2015). What Explains Child Malnutrition of Indigenous People of Northeast India? PLoS ONE 10(6). |
|
|
Solomons NW, Vossenaar M, Chomat AM, Doak CM, Koski KG, Scott ME (2015). Stunting at birth: Recognition of early-life linear growth failure in the western highlands of Guatemala. Public Health Nutrition, 18(10):1737-1745. |
|
|
Sultana P, Rahman MM, Akter J (2019). Correlates of stunting among under-five children in Bangladesh: A multilevel approach. BMC Nutrition 5(1):41. |
|
|
Titaley CR, Ariawan I, Hapsari D, Muasyaroh A, Dibley MJ (2019). Determinants of the Stunting of Children Under Two Years Old in Indonesia: A Multilevel Analysis of the 2013 Indonesia Basic Health Survey. Nutrients 11(5). |
|
|
Tumilowicz A, Habicht JP, Pelto G, Pelletier DL (2015). Gender perceptions predict sex differences in growth patterns of indigenous Guatemalan infants and young children. The American Journal of Clinical Nutrition 102(5):1249-1258. |
|
|
United Nations International Children's Educational Fund (UNICEF) (Ed.) (2013). Improving child nutrition: The achievable imperative for global progress. United Nations Children's Fund. |
|
|
United Nations (2017). Transforming Our World: The 2030 Agenda for Sustainable Development. In: A New Era in Global Health. Springer Publishing Company. |
|
|
United Nations Children's Fund (1991). Strategy for improved nutrition of children and women in developing countries. The Indian Journal of Pediatrics 58(1):13-24. |
|
|
Vakili R, Emami MZ, Khademi G, Vakili S, Saeidi M (2015). Child Mortality at Different World Regions: A Comparison Review. International Journal of Pediatrics 3(42):809-816. |
|
|
Victora CG, Adair L, Fall C, Hallal PC, Martorell R, Richter L, Sachdev HS (2008). Maternal and child undernutrition: Consequences for adult health and human capital. Lancet (London, England) 371(9609):340-357. |
|
|
Walrod J, Seccareccia E, Sarmiento I, Pimentel JP, Misra S, Morales J, Andersson N (2018). Community factors associated with stunting, overweight and food insecurity: A community-based mixed-method study in four Andean indigenous communities in Ecuador. BMJ Open 8(7):e020760. |
|
|
Wamani H, Astrøm AN, Peterson S, Tumwine JK, Tylleskär T (2007). Boys are more stunted than girls in sub-Saharan Africa: A meta-analysis of 16 demographic and health surveys. BMC Pediatrics 7:17. |
|
|
World Health Organization, UNICEF, United States, & Agency for International Development (2015). Improving Nutrition Outcomes with Better Water, Sanitation and Hygiene: Practical Solutions for Policies and Programs. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


