ABSTRACT
Throughout the world, occupational exposure in cement factories continue to cause serious public health problems and are leading cause of disability and disease among workers. Since there has not been any study on the prevalence and associated factors of occupational injury in cement factory, this study investigates the prevalence and associated factors of occupational injuries among cement factory workers in Mugher. An institution based cross-sectional study was conducted using stratified random sampling by job category. The study participants were selected using simple random sampling technique and data collected by trained data collectors using pretested questionnaire. The data was edited, entered into a computer using Epi Info version 3.5.0 then exported to IBM SPSS version 21 and cleaned. Bivariate and multivariate analyses were done. The prevalence of occupational injury in one year was 10.4%. In addition, 1356 working days were lost as a result of 52 work related injuries. Thirty-seven (71.2%) were hospitalized, accounting for 51.4% hospitalization for more than 24 h, 18(34.6%) were absent from work for 15 to 30 days. Job category was the significant contributing factor for occupational injuries with workers in the cement production factory 74.7% less likely to experience occupational injury than workers in clinker production [AOR= 0.25, CI: (0.100-0.639)]. The prevalence of occupational injury was high, hence focus should be on preventive measures like timely provision of adequate and quality safety materials along with workplace supervision.
Key words: Occupational injury, cement factory workers, disability, disease and safety materials.
According to Labor Proclamation No. 377/2003 of Ethiopia, "Occupational injury" means any organic injury or functional disorder sustained by a worker as a result of any cause extraneous to the injured worker or any effort he makes during or in connection with the performance of his work and includes:
1. Any injury sustained by a worker while carrying out the employer's order, even away from the work place or outside his normal hours of work;
2. Any injury sustained by a worker before or after his work or during any interruption of work if he is present in the work place or the premises of the undertaking by reason of his duties in connection with his work;
3. Any injury sustained by a worker while he is proceeding to or from place of work in a transport service vehicle provided by the undertaking which is available for the common use of its workers or in a vehicle hired and expressly destined by the undertaking for the same purpose;
4. Any injury sustained by a worker as a result of an action of the employer or a third party during the performance of his work (Labour Proclamation No.377/2003, 2004).
Occupational injuries are injuries that occur at the location of a person's employment which can include exposure to chemicals or other substances as well as accidents. Occupational accidents, work injury, work-related injury, work accidents, work-related accidents are other names for occupational injuries (
http://www.rightdiagnosis.com/o/occupational_injuries/subtypes.htm). The primary cause of occupational injuries is the result from exposure to deleterious agents usually toxins, gases, inhalants, etc. while working (Andrina, 1998). According to International Labor Organization (ILO) projections for the year 2000, based on 1998 statistics there were two million work-related deaths annually worldwide of these accidents contribute 19%. The ILO estimated that the total costs of occupational accidents and work-related diseases are 4% of the gross national product. Most of the world's work-related deaths, injuries and illnesses are preventable (International Labour Organization, 2003). According to results from the Census of Fatal Occupational Injuries conducted by the U.S. Bureau of Labor Statistics, a preliminary total of 4,383 fatal work injuries were recorded in the United States in 2012 (Bureau of Labor Statistics U.S Department of Labor, 2013).
According to Centers for Disease Control and Prevention, 7.9 million nonfatal injuries to younger workers were treated in U.S. hospital emergency departments in 10 years (Centers for Disease Control Prevention, 2010). A global burden of about 10.5 million DALYs is estimated due to both fatal and non-fatal occupational injuries (Marisol et al., 2005). In Ethiopia, in an accident report by Ministry of Labor and Social Affairs (MOLSA) taken from 66 establishments during 2008/2009, a total of 1968 work accidents were reported of which the 9 were fatal. Among the reported work accidents 56.05% occurred in the manufacturing industries. According to the same report taken from 220 establishments in 2009/2010, 29 fatal and 6127 non-fatal work accidents were reported totally. Among the total 41.64% occurred in the manufacturing industries. Similarly in an accident report by MOLSA taken from 248 establishments in 2010/2011 showed that there were 16 fatal and 6990 non-fatal work accidents. Among the reported 51.78% taken place in agricultural, hunting, forestry and fishing sector followed by 42.95% in the manufacturing industries (Ethiopian Ministry of Labour and Social Affairs, 2008-2011).
Occupational injuries may occur in the production process of cement factory as a result of unsafe working condition, unsafe acts, personal failure and lack of awareness on the side of both employers and employees. The failure on the part of the management in realizing and applying properly guarded machine, proper illumination and ventilation, non-defective tools etc could be considered as one of the causes of work accidents. Occupational injuries may result in loss of life, physical impairment, material damage and termination of work that might claim very large financial loss (Ethiopian Ministry of Labour and Social Affairs, 2008-2011). Sex, age (Aderaw et al., 2011; Yiha and Kumie, 2010; Tadesse and Kumie, 2007), educational status (Serkalem et al., 2014; Kifle et al., 2014), marital status (Serkalem et al., 2014), job category, lack of experience, workplace supervision, job satisfaction (Tadesse and Kumie, 2007), working hour per week (Yiha and Kumie, 2010; Tadesse and Kumie, 2007; Serkalem et al., 2014) health and safety training (Aderaw et al., 2011), alcohol use (Yiha and Kumie, 2010; Kifle et al., 2014), sleeping disorder (Yiha and Kumie, 2010; Tadesse and Kumie, 2007; Serkalem et al., 2014), manual handling of very heavy objects (>20 kg), need for visual concentration for the task, and maintenance of machine (Serkalem et al., 2014), job stress (Aderaw et al., 2011; Kifle et al., 2014), non PPE use (Yiha and Kumie, 2010; Kifle et al., 2014) were factors associated with occupational injury in a study done in Ethiopia.
Most of the world's work-related deaths, injuries and illnesses are preventable. Worldwide occupational exposure to cement dust and other hazards is the cause for skin allergies, eye irritation and other work related injuries (Sana et al., 2013). Job category, work experience and use of personal protective equipments are the associated factors (Iqbal et al., 2010).Different investigations in Africa reported that cement industry is responsible for many type of injuries like burn injury in different part of the body, fracture, falling and responsible for hospitalization, high cost for treatment and loss of productivity due to absence from workplace (Shafik and El-Mohsen, 2012). Studies done in different parts of Ethiopia reported occupational injury is prevalent in different industries. Occupational injury caused many types of injuries, affect different parts of the body and it is the cause for hospitalization, working days lost (Yiha and Kumie, 2010; Kifle et al., 2014) and death (Tadesse and Kumie, 2007; Serkalem et al., 2014).
Studies done in different industry sector (even though they are different sectors they use similar machineries) of Ethiopia reported that age, working hour in a week, health and safety training, alcohol consumption and sleep disorder (Tadesse and Kumie, 2007), educational status, marital status, manual handling of heavy objects, maintenance of machine (Kifle et al., 2014), work stress (Aderaw et al., 2011; Kifle et al., 2014), work experience, job category, work place supervision (Tadesse and Kumie, 2007), use of personal protective equipment (PPE) (Kifle et al., 2014) were associated factors of occupational injury. While some of them reported that sex, educational level, monthly salary, job category, work experience, job satisfaction and use of PPE (Yiha and Kumie, 2010; Tadesse and Kumie, 2007), age, sex, employment pattern, work place supervision, health and safety training and sleep disorder (Kifle et al., 2014) were not associated with occupational injury.
Work, when it is well-adjusted and productive can be an important factor in health promotion, e.g. partially disabled workers may be rehabilitated by undertaking tasks suited to their physical and mental limitations and in this way, may substantially increase their working capacity (Occupational Health, 2001).There is a great discrepancy in the studies explained above in relation to the associated factors of occupational injuries in different industry sectors. In addition there is no study carried out on the prevalence and associated factors of occupational injury in cement factory. Occupational health and safety affect not only the worker but also his/her family and significant others and his community. There is rapid industrialization due to favorable investment policy, which may result in an increased number of industries and employment in Ethiopia, placing a greater number of people at risk from cement dust exposure and other hazards Therefore, it is important to know the prevalence and determinants of occupational injuries among cement factory workers.
Study area
According to Ministry of Industry there are around 10 cement factories in Ethiopia. Mugher Cement Enterprise is a state owned plant constructed in 1984. Mugher Cement Enterprise’s first production line was commissioned and officially inaugurated in 1984 with a capacity of 300,000 tons of clinker per annum, near Mugher River, located 90 km west of Addis Ababa. The enterprise doubled its capacity to 600,000 tons per annum of clinker production in 1990 with the construction of a second plant. The 3rd line cement expansion project was commissioned in 2011. It is the largest cement producer in Ethiopia with a production capacity of 900,000 tones and a 35% market share and has a total workforce of 1,488. The head office is based just outside the capital and its quarrying sites are spread across the country. Mugher Enterprise produces two main products OPC (Ordinary Portland cement) and PPC (Poslana Portland Cement). Sulphate resistance cement is sometimes produced on demand.
The firm produces about 60 million packaging sacs for its own consumption in Addis Ababa branch. Mugher also extracts and sells natural resource minerals such as gypsum, limestone and silica to other manufacturing companies and farms. Mugher uses an outdated production technology from Germany which has high energy consumption and dust emission (Yessuf et al., 2013). There were around 1488 workers in Mugher cement Enterprise in all branches (Mugher, Addis Ababa, Derba, Tatek and Nazreth). Out of the 1488 workers, 955 were working on the cement production process which includes raw material, clinker production, cement production and engineering processes. There were around 690 workers with greater than one year work experience in the production process of Mugher which was selected as a study area.
Study design
An industry based cross sectional study complemented with observation checklist and record review was conducted.
Source population
All workers in the production process of the cement factory. The production process consists of four main sections clinker production, cement production, raw material production and preparation and engineering team because they are considered as exposed to occupational health and safety hazards that leads to occupational injury.
Study population
All workers are randomly selected from the production process of the cement factory.
Inclusion criteria
All employees who were directly engaged in the production process within the study period and who have been working at least for one year in the selected factory irrespective of sex were included in the study.
Exclusion criteria
Workers less than 18 years old were excluded. Workers who were absent from work for more than 3 times of visit at the time of data collection were not included.
Sample size determination
The total sample size was calculated for each specific objective by using Epi Info version 7 and considering different parameters, and the largest sample size was taken. Considering 95% confidence level, 90% Power (1-ß), odds ratio of 1.9 (Shafik and El-Mohsen, 2012) and adding 5% non-response rate, a sample size of 500 was calculated.
Sampling procedures
Stratified random sampling was applied to get the desired sampling unit. It was stratified by job category. The calculated sample size was allocated to each stratum using probability proportional to size (PPS). The sampling frame was obtained from Mugher Cement Factory, Human Resource Management Office. A total of 500 study participants were selected using simple random sampling technique from the sampling frame using lottery method.
Data collection procedures
Data was collected using pretested and structured Amharic version questionnaire via face to face interview of the study participants after getting ethical clearance from responsible bodies and informed verbal consent from study participants. Before the actual data collection the questionnaire was pretested in 5% (25 workers) outside the study area; in Addis Ababa (Ethiopian Iron and steel factory). Based on the pretest necessary modification was done on the questions and participants who were involved in the pretest were excluded in the actual data analysis. The questionnaire was prepared in English and translated to Amharic and later translated back to English. The questionnaire was adopted from previous researches (Tadesse and Kumie, 2007).
The questionnaire focused on socio demographic, behavioral, and environmental variables and occupational injury characteristics. Work place observation checklist, record reviews were done and sick leaves were checked to supplement the quantitative data. Data collection was administered by four persons, one who have bachelor degree and the rest 10 complete and two supervisors with B.Sc degree in occupational health and MPH degree, respectively after two-day training. In case the selected respondents were absent, the data collectors tried to visit three times.
Study variable
Dependent variable
This includes occupational injury.
Independent variables
This includes the following:
1. Socio demographic factors: Sex, age, educational level, monthly salary, service duration, job category.
2. Work environment factors: Hours worked per week, workplace supervision, health and safety training.
3. Behavioral factors: Alcohol use, chat chewing, sleep disorder, job satisfaction, and use of personal protective equipment.
Operational definition
Occupational Injury-an injury sustained on worker in connection with the performance of his or her work in cement factory within one year that causes hospitalization, working days lost or disabilities and death as reported by the worker, confirming clinical records and sick leave.
Data management
After the completion of data collection, the raw data was edited, entered in to a computer using Epi Info version 3.5.0 then exported to IBM SPSS version 21. Data was cleaned in Epi Info version 3.5 as well as IBM SPSS version 21 by running frequencies and cross tabulations. Preliminary frequencies were run to identify missing variables. Data was backed up by saving it in different folders in the computer, removable flash disk and email. Continuous variables were coded and some coded variables were recoded.
Data analysis procedures
Data was analyzed using IBM SPSS version 21 and used to display percentages, graphs and tables. Descriptive statistics of the collected data was done for all variables in the study using standard statistical parameters: Percentages, means and standard deviations. Bivariate analysis (Cross tabulation and chi square, Crude OR with 95% confidence interval) were done for the independent variables with the outcome variable to select candidate variables for the multivariate analysis (Adjusted OR). Variables which showed significant association with the outcome variable on the bivariate analysis were entered in to multivariate logistic regression analysis to identify their independent effects on the outcome variable. 95% confidence interval and p-value <0.05 was used. To avoid an excessive numbers of variables and unstable estimates in the multivariate analysis variables reached a p-value less than 0.2, variables which become significant and those variables that were considered as determinants were kept. The variables which showed significant association in the bivariate and continue in the multivariate were the determinants of occupational injury. The overall effect of socio demographic variables on the occurrence of occupational injury was assessed in the first step. In the second step of the analysis, the work environment variables were added, and their effect was assessed. Behavioral factors were entered in the third step. In the fourth step selected socio demographic factors, work environment and behavioral factors together was assessed to see the overall effect on the occurrence of occupational injury.
Data quality assurance
Training of the data collection team with pretesting in 5% of the sample size before the actual survey was conducted for two days to ensure the possible quality of the data. Based on the pretest results, the questionnaire was additionally adjusted quantitatively, contextually and terminologically, and administered on the study population. Every day the completed questionnaires were handled to the supervisor on each day of data collection. The data collected in the cement factory was checked daily for completeness, clarity and logical consistency by the investigator and supervisor. Incorrectly filled or missed ones were sent back to data collectors for correction. Anything, which was unclear and ambiguous were corrected on the next day. Five percent of the samples were rechecked by the supervisors whether the interviewers have done their job correctly or not. Five percent of the collected data was entered twice by the investigators to verify whether the data was properly entered or not.
Ethical consideration
The study was approved by Addis Ababa University, School of Public Health Ethical Clearance Committee. A letter obtained from Addis Ababa University, School of Public Health Ethical Clearance Committee was submitted to the relevant and concerned bodies in the cement factory before starting the study. The information sheet and consent was provided for respondents to read for those who can read and the interviewer read the consent form for those respondents who cannot read. Finally the respondents were asked the agreement to participate in the study. The respondents were informed about the objective of the study. Confidentiality was maintained by omitting their names and personal identification, never be used in connection with any information and it was not revealed to anyone except the principal investigator and assistants and was kept locked with key in the entire study period.
Privacy was maintained by arranging quite place for interviewer and study participant to protect them exposing other parties according to the choice of the respondent ensuring visual and auditory privacy throughout the data collection. Study participants had the right to participate on the study or not and they can withdraw at any time of the study they wish. There was no benefit the study participants can get in terms of money or other item but they can get benefit in the future if there is a change of policy and strategies by considering this study, the benefit is to improve occupational safety, health and working environment services provided based on their answers to the questions. There was no risk to the study participants because of this study.
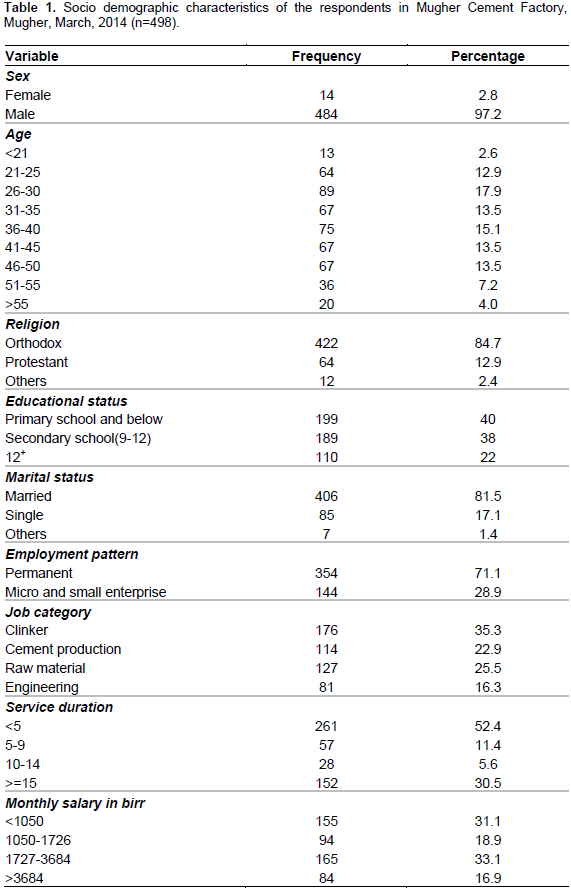
A total of 498(99.6%) respondents were included in the study and interviewed if they had experienced work related injury in the last 12 months.
Socio demographic characteristics of the respondents
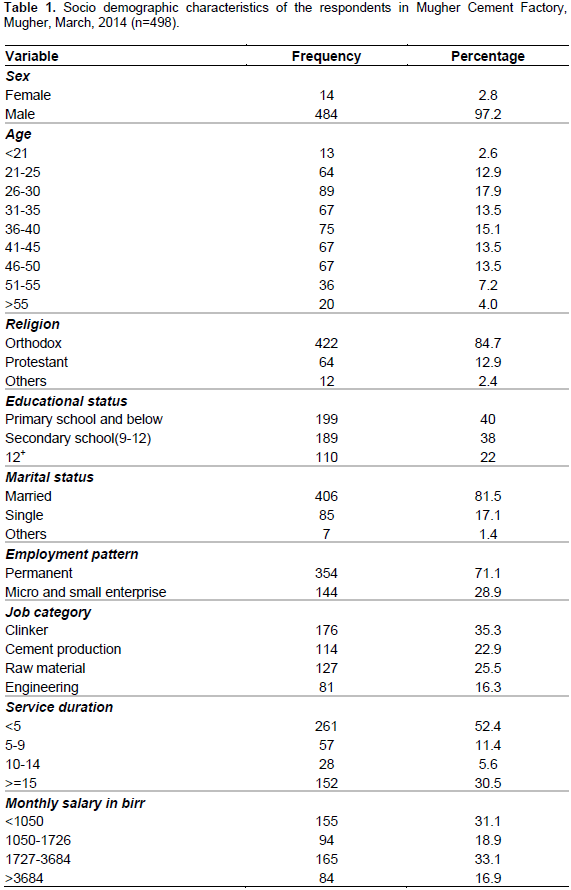
The 498 respondents included 484 males. The mean age (SD) 37.36±10.32 was years. About 89(17.9%) of the respondents were in the age group 26 to 30 years. The majority 422 (84.7%) of study participants were orthodox Christian religion followers. About 189(38%) of the respondents have attended secondary school. Regarding marital status of the respondents, the majority 406 (81.5%) was married. Out of 498 study participants, 354 (71.1%) were permanent and 144 (28.9%) were from micro and small enterprise. One hundred seventy six (35.3%) of the respondents were from clinker production. 165(33.1%) of the respondents had 1727 to 3684 monthly salary in birr. Most, [261 (52.4%)] of the respondents had working experience of five years or below (Table 1).
Occupational injury characteristics
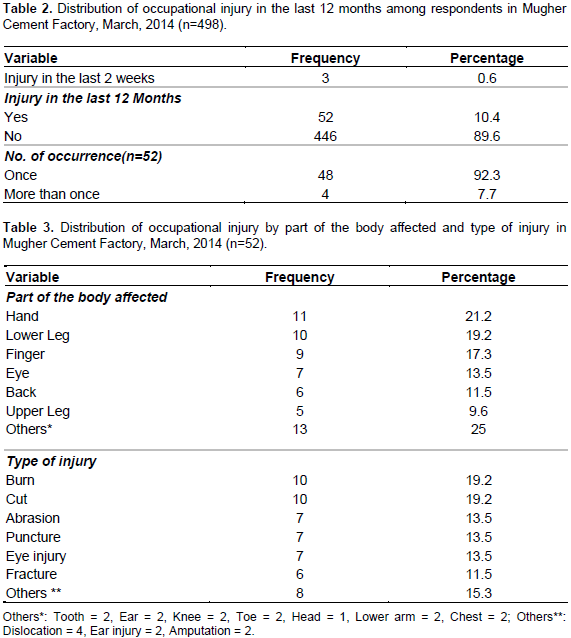
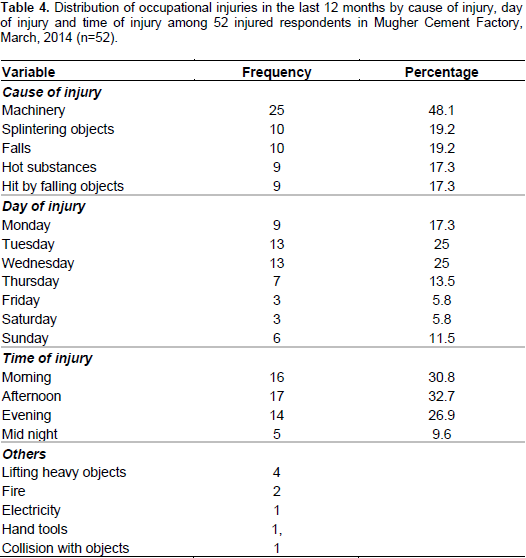
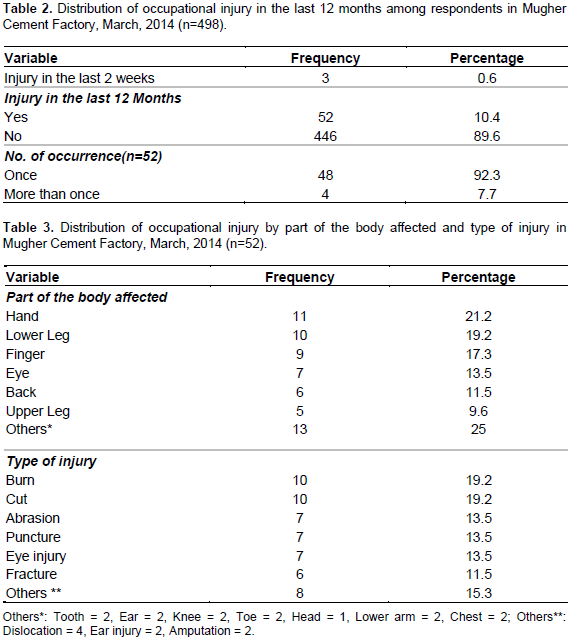
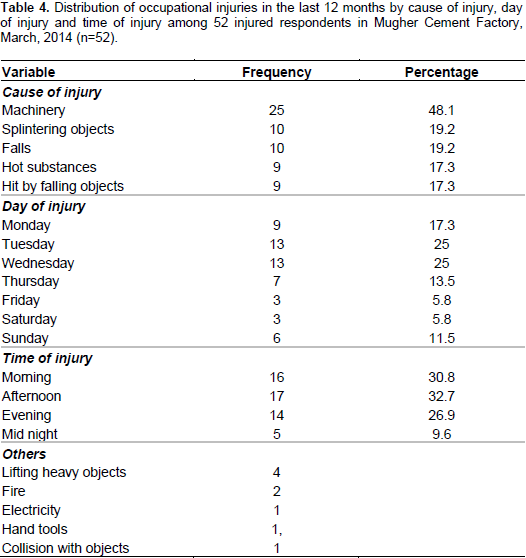
A total of 63(12.7%) respondents reported occupational injuries during the last 12 months. Due to the definition of occupational injury in this study and after reviewing records the overall prevalence during the last 12 months was 52(10.4%) and 48 92.3%) of the injured respondents reported they had sustained occupational injury once. The two week prevalence was 3(0.6%). Of this case all reported that they had sustained occupational injury once (Table 2). Hands were the body part with the highest frequency of occupational injuries 11(21.2%), lower leg 10(19.2%), finger 9(17.3%) and eye 7(13.5%) were other sites frequently affected. The main types of injuries reported were cuts, 10(19.2%), burn, 10(19.2%), abrasions, 7(13.5%) and eye injury, 7(13.5%) (Table 3). In this study the most common agent stated as cause was machinery 25 (48.1%), splintering objects 10 (19.2%) and falls 10 (19.2%) followed by hot substances 9(17.3%). Thirteen (25%) of the occupational injuries occurred on Tuesday and Wednesday 13(25%) followed by Monday [9(17.3%)]. The most 17(32.7%) common time of injury was in the afternoon followed by morning [16(30.8%)] (Table 4).
Severity of occupational injuries
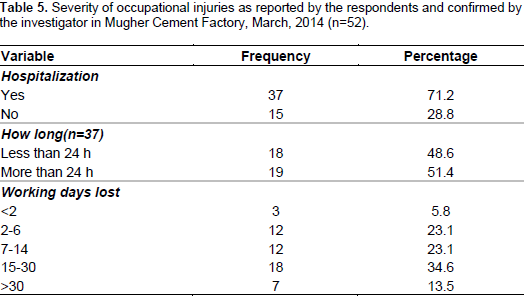
Of the total 52 injured respondents, 37(71.2%) were hospitalized, accounting for 51.4% hospitalization more than 24 h. 18(34.6%) were absent from work for 15 to 30 days There was one report with disability (total disability was 10% from the whole man) resulted in lumbar contusion and mild difficulty of walking which is decided by medical board of St. Paul hospital. In addition, 1356 working days were lost as result of 52 occupational injuries (Table 5).
Work environment characteristics
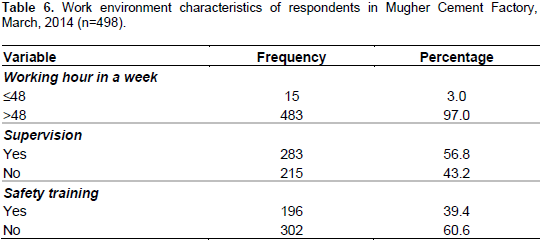
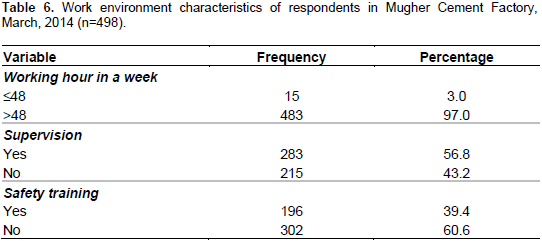
Four hundred eighty three (97%) respondents worked more than 48 h per week. Two hundred and fifteen (43.2%) of the respondents reported that their workplaces were not supervised regularly. Majority (60.6%) of the respondents were not taken any health and safety training (Table 6).
Behavioral characteristics
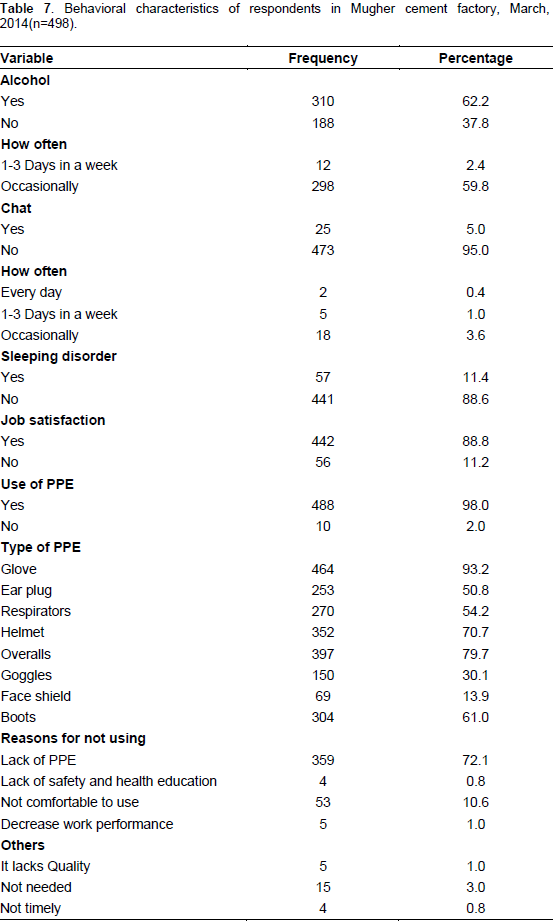
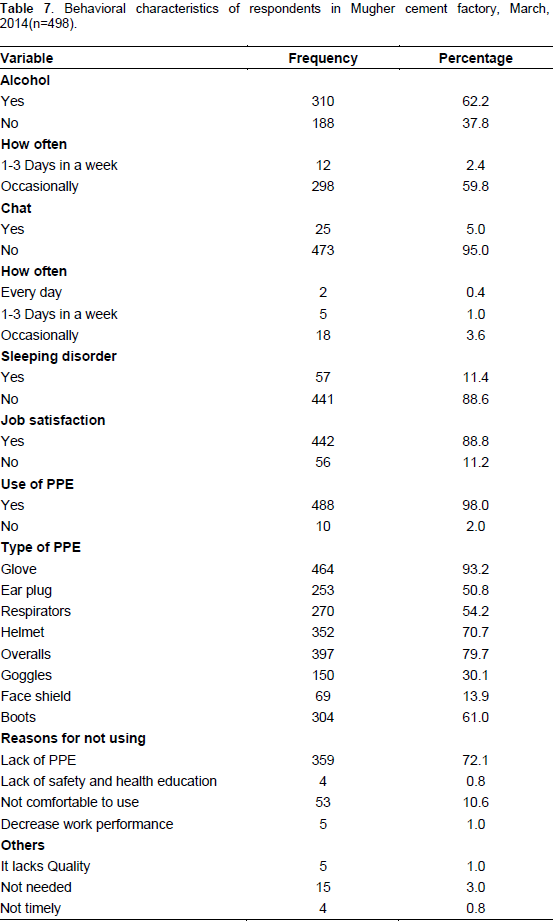
310 (62.2%) and 25(5%) of the respondents consumed alcohol and chewed chat, respectively. Tela was consumed by majority of them [231(46.4%)]. 298(59.8%) consumed occasionally. About 57 (11.4%) of the respondents reported that they had sleep disorder. The majority 442 (88.8%) of the respondents were satisfied by their current job. 488 (98.0%) of the respondents used personal protective equipment at their workplace, while 10 (2.0%) did not used any type of personal of protective equipment. Glove was used by majority of the respondents [464(93.2%)]. All of the study participants were interviewed for non-use of protective equipment and reported the most frequent reasons were lack personal protective equipment [359 (72.1%)], and not comfortable to use [53 (10.6%)] (Table 7).
Workers health information on illness symptoms
Eighty-four (16.9%) of the respondents reported that they are exposed to eye irritation 15 days prior to the data collection followed by skin allergy [51(10.2%)]. General weakness [34(6.8)], wheezing [18(3.6)], cough longer than 3 weeks [6(1.2)] and cough with sputum 1(0.2) were also reported.
Work environment observation
According to the observation workers around the kiln were exposed to heat, noise and splintering objects that pass through the conveyer belt without cover. Workers in cement packing were exposed to excessive dust, radiation and there was no adequate light. Some of the control rooms and cement packing room were not properly ventilated; some of the ventilators were not functional at the time of data collection. There was dust in the raw mill when the electro filter (conditioning tower) was not functioning. It pollutes the environment by changing its direction to different areas, sometimes it goes also to residential area of the workers that can cause many health problems and it is the cause for wastage of the raw material up to 9 tons per hour so that we can see that there is economical loss. No enough safety precautions were observed.
There were some directives and fire extinguishers in most of the work areas but the instructions are written in English that all workers may not read it. Some of the permanent workers use necessary PPE but they complained that they lack quality and were not provided timely. For example safety shoes provided cannot prevent foot where there is the risk of foot injuries from hot substances. Workers from the micro and small enterprises were not provided PPE by the organization, they bought by themselves. There was occupational health and safety officer but there was no adequate supervision from our observation. Training was given for some of the workers. There were two cafeterias near the plant which was patronized by many people and this may cause many health hazards. First Aid facilities were available but not functional in their workplace, but there was a health center in the compound.
Socio demographic factors
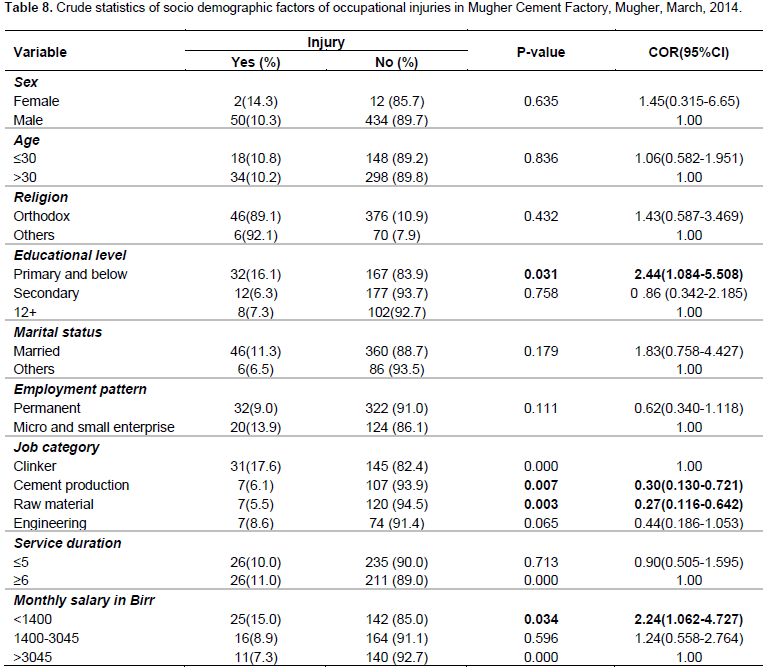
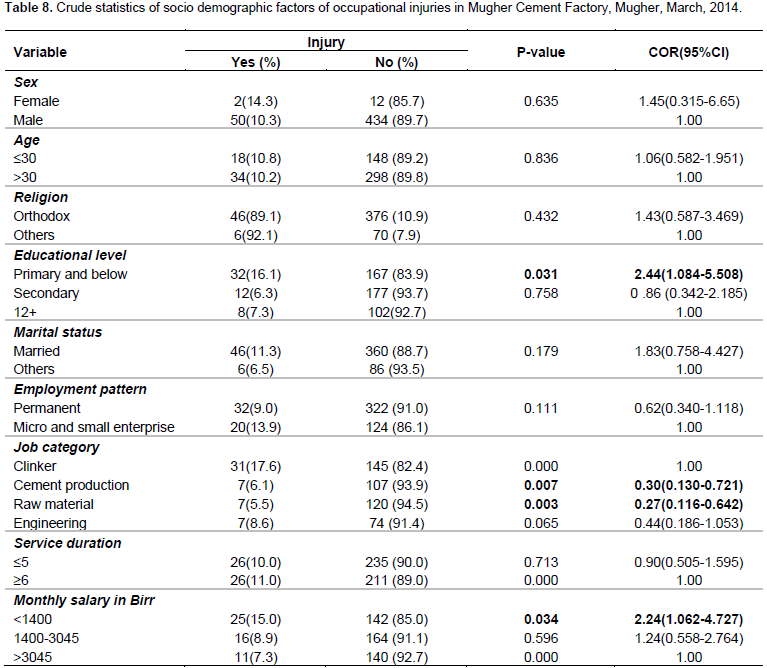
Educational level, job category, and monthly salary were identified as the major socio demographic determinant of occupational injury. When comparing workers who attended primary school and those below with workers who attended higher education, the difference was statistically significant. Workers who attended primary school had 2.44 times more odds of occupational injuries than workers who attended high school and colleges [OR=2.44, 95% CI: 1.084-5.508]. Occupational injury was statistically associated with job category. Workers who were working in cement production, raw materials preparation and production respectively were 69 and 73% less likely to report occupational injury than clinker production. Monthly salary was also another variable that showed association with prevalence of occupational injury. Workers who were paid less during the interview were more likely to report occupational injury [OR=2.24, 95 CI: 1.062-4.727] compared to those who were paid relatively higher. However, in this study occupational injury was not associated with sex, age, religion, marital status and service duration of the respondents (Table 8).
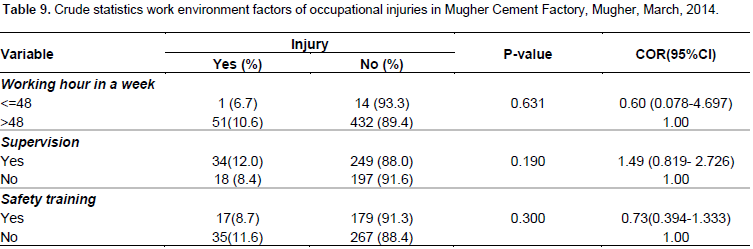
Work environment factors
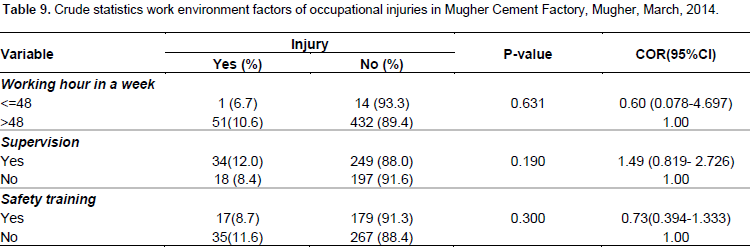
Hours worked per week, workplace supervision, health and safety training showed no association with the prevalence of occupational injuries (Table 9).
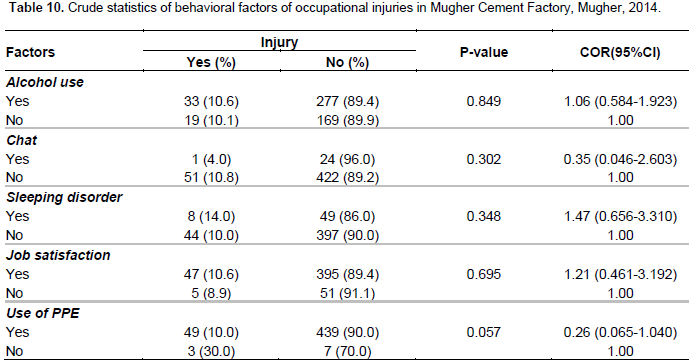
Behavioral factors
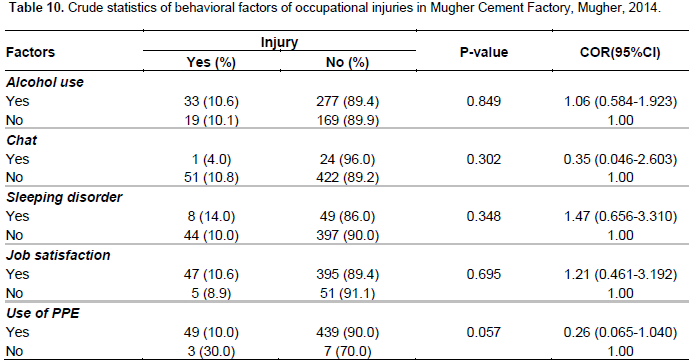
Alcohol use, chat chewing, sleeping disorder, job satisfaction and use of personal protective equipments did not show significant association (Table 10).
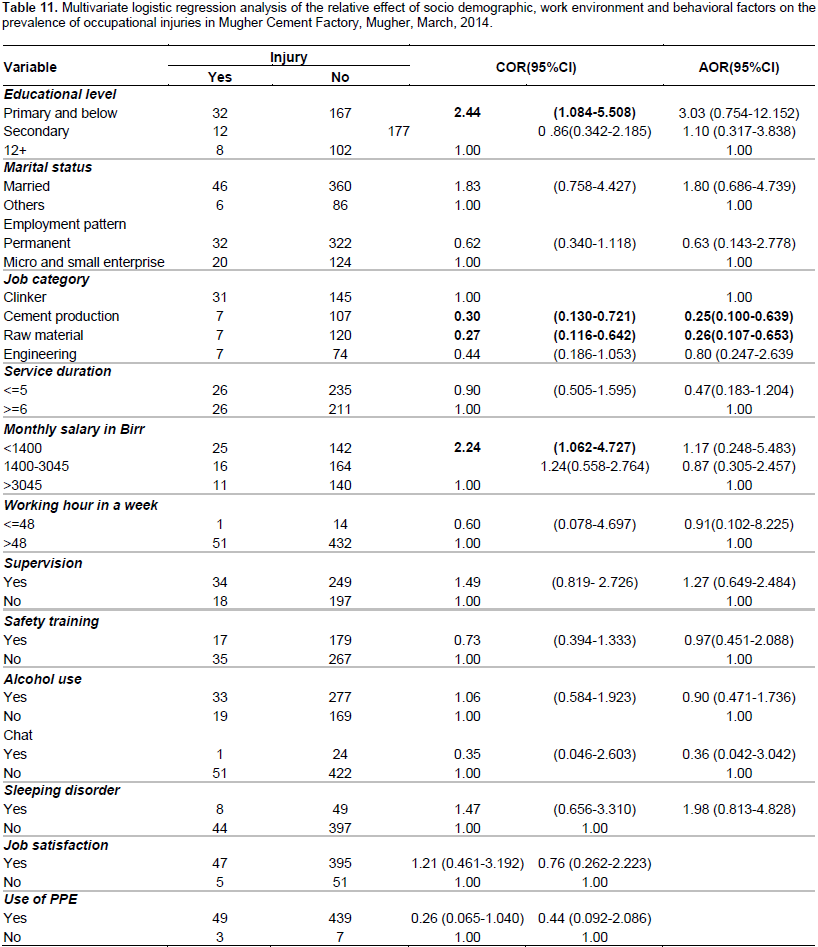
Multivariate logistic regression analysis
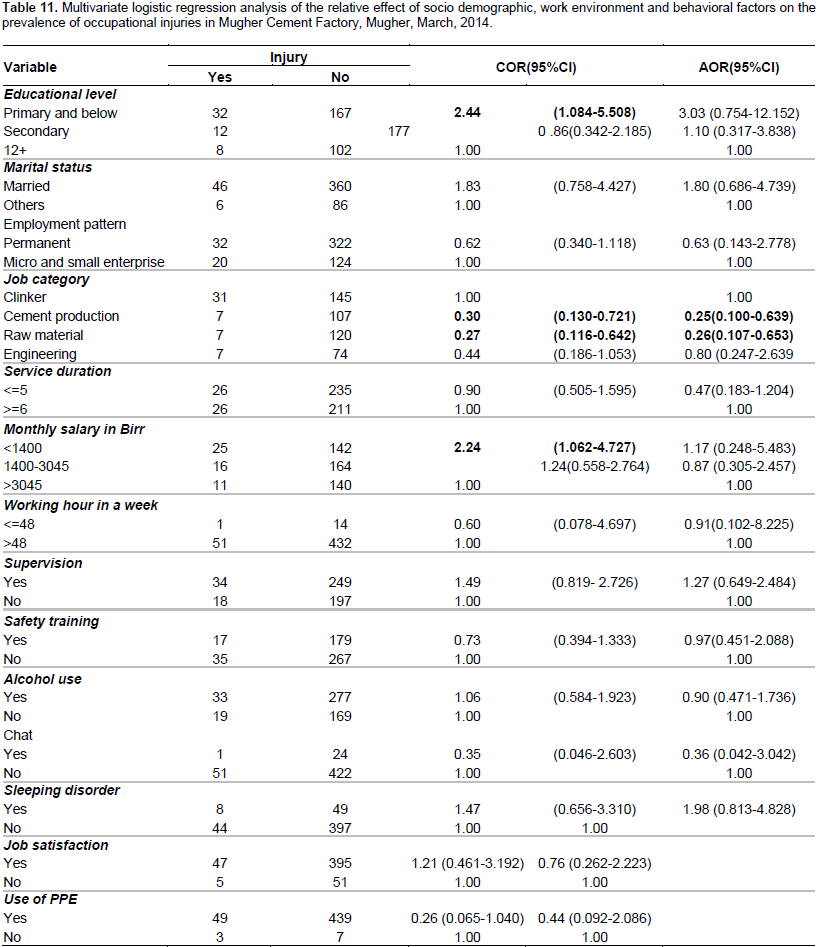
The overall effect of socio demographic variables on the occurrence of occupational injury was assessed in the first step. In the second step of the analysis, the work environment variables were added, and their effect was assessed. Behavioral factors were entered in the third step. In the fourth step selected socio demographic factors, work environment and behavioral factors together was assessed to see the overall effect on the occurrence of occupational injury. Among the mentioned socio demographic variables computed in the first step, job categories in cement production and raw material remained significant. Workers in the cement production were 74.3% less likely to experience occupational injury than workers in clinker production [OR=0. 26, 95% CI: 0.105-0.628], workers in the raw material production had 75.2% less than lower odds of having occupational injury than workers in the clinker production [OR=0.25 ,CI 95%:0.102-0.607].
From work environment variables analyzed hours worked per week, supervision of workplace and health and safety training were not statistically significant. From the behavioral factors, the use of PPE was found to be significant. Workers who used PPE were 0.24 less likely to experience occupational injury than who did not use PPE [OR=0.24, 95% CI ;( 0.058-0.973)]. From the variables computed in the fourth step only job category was found to be significant. Workers in the cement production were 74.7% less likely to experience occupational injury than workers in clinker production [OR= 0.25, CI: (0.100-0.639)]; workers in the raw material production had 73.6% less likely to experience occupational injury than workers in the clinker production [OR = 0.26, CI: (0.107-0.653)] (Table 11).
The 12 months prevalence was 52(10.4%) and 48 (92.3%) of the injured respondents reported they had sustained occupational injury once. The two week prevalence was 3(0.6%). Of this case all reported that they had sustained occupational injury once. The overall prevalence was relatively low compared with other studies (Yiha and Kumie, 2010; Tadesse and Kumie, 2007; Kifle et al., 2014; Yessuf et al., 2013). Of the total 52 injured respondents, 37(71.2%) were hospitalized, accounting for 51.4% hospitalization more than 24 h. 18(34.6%) were absent from work for 15 to 30 days. There was one report with disability (total disability was 10% from the whole man) resulted in lumbar contusion and mild difficulty of walking which is decided by medical board of St. Paul hospital. In addition, 1356 working days were lost as result of 52 occupational injuries. Hospitalization and working days lost can result to increase in medical cost, compensation cost, absenteeism and loss of working capacity which adversely affects productivity of the employees as well as the employer so we can see it economically. Work that resulted in production loss and disregard the safety and health of workers cannot be the basis of sustainable development.
In a study done in Afar, 70 (11.0%) were hospitalized. Regarding the length of hospitalization, 7 (10.0%) were for 1 day, 25 (35.7%) were between 24 h and 4 days, 25(35.7%) were 5 to 10 days, and 13(18.6%) were admitted for more than 10 days. One death was also reported due to severe head injury while working in the ginning section in the past 12 months. A total of 6153 work days were lost among 634 injured respondents (Yiha and Kumie, 2010). A study done in Kombolcha textile factory revealed that 73(43.45%) were hospitalized where 67% of the hospitalization were for more than 24 h. 137 working days were lost as result of work related injuries in the last 12 months (Yessuf et al., 2013).
Fifty five (17.1%) were hospitalized, accounting for 40% hospitalization more than 24 h. One hundred and three (53.9%) were absent from work for more than 4 days. In addition, 191 working days were lost as result of 322 work related injuries. There were 2 reported deaths as result of work related injuries in a study done in North Gondar (Tadesse and Kumie, 2007).
Hands were the body part with the highest frequency of occupational injuries 11 (21.2%), lower leg 10 (19.2%), finger 9 (17.3%) and eye 7(13.5%) were other sites frequently affected. The possible explanation is due to more involvement in work which has direct exposure to machines, hot materials and can be affected more by injuries. Non-use of PPE can also be the reason. This is consistent with a study done in Kombolcha (Yessuf et al., 2013) and North Gondar (Tadesse and Kumie, 2007) and inconsistent with a study done in Bangladesh (Iqbal et al., 2010), Afar (Yiha and Kumie, 2010) and Addis Ababa (Kifle et al., 2014) this might be due to use of adequate PPE in this studies. The main types of injuries reported were cuts 10(19.2%), burn 10(19.2%), abrasions 7(13.5%) and eye injury 7(13.5%). This is inconsistent with findings in Ethiopia (Yiha and Kumie, 2010; Tadesse and Kumie, 2007; Kifle et al., 2014; Yessuf et al., 2013); this could be due to the difference in the nature of the work, the type of machineries used in this different industries are not similar.
In this study the most common agent stated as cause was machinery 25 (48.1%), splintering objects 10 (19.2%) and falls 10 (19.2%) followed by hot substances 9(17.3%). This could be due to presence of unguarded machine parts and nonuse of PPE. This is in agreement with (Tadesse and Kumie, 2007; Yessuf et al., 2013) and inconsistent with Yiha and Kumie (2010) and can be explained by the difference in materials they used for work. Thirteen (25%) of the occupational injuries occurred on Tuesday and Wednesday 13(25%) followed by Monday 9(17.3%).The most 17(32.7%) common time of injury was in the afternoon followed by morning 16(30.8%). This is inconsistent with Tadesse and Kumie (2007); the reason could be the difference of work shifts. There are three working shifts with 8 working hour interval in the cement factory. The possible explanation for the high frequency of injury in the afternoon could be due to speeding up of the production by the second round shift workers to meet the target before it becomes dark. In this study, eighty four (16.9%) of the respondents reported that they are exposed to eye irritation 15 days prior to the data collection followed by skin allergy 51(10.2%).
Findings from India (Sana et al., 2013) and Cairo (Shafik and El-Mohsen, 2012) reported similarly. The use of personal protective equipment (PPE) is found to be significant when the effect of behavioral factors on occupational injury detected alone. Workers who used PPE were 0.238 less likely to experience occupational injury than those who did not use PPE [AOR=0.24, CI: (0.058-0.973)], but did not show significant association when socio demographic and work environment factors were added. Even though use of PPE did not show in the bivariate and multivariate analysis when added with the other factors in this study 72.1% of the workers reported there was lack of PPE and it was not provided timely and did not have quality. From the variables computed in the multivariate analysis job category was found to be significant which is consistent with a study done in North Gondar (Tadesse and Kumie, 2007). This can be explained by the work environment in clinker production is very hazardous, most of the workers in clinker production are from micro and small enterprises from which they are not provided adequate and quality PPE, lack of safety and health training and lack of regular workplace supervision.
Some studies revealed that increasing educational levels have been associated with decreasing work related injuries. This may be explained that education is likely to enhance workers health and safety practice that prevent them from work-related injuries. However, in our study educational level was not associated with occurrence of work-related injuries. This could be explained education only cannot eliminate injury when the level of hazards is high and when the use of adequate PPE and safe work organization are limited. However, in this study occupational injury was not associated with marital status, employment pattern, service duration, monthly salary, hours worked per week, workplace supervision, health and safety training, alcohol use, chat chewing, sleeping disorder, job satisfaction and use of PPE of the respondents. This study was not free of limitations. Since the study was a one year cross sectional study, the possibility of recall bias may result in under reporting and misreporting of events. Moreover, lack of studies with similar methodology and similar topic particularly in Ethiopia context made it difficult to compare results.
CONCLUSION AND RECOMMENDATIONS
The prevalence of occupational injury was 10.4%. Job category increased the risk of work related injuries. Taking modifiable and preventable factors that affect occupational injury occurrence into consideration, the following recommendations are forwarded to Mugher Cement Factory based on the findings of the study. Provision and supervision of adequate and quality safety materials timely and their appropriate use should be done. Besides, regular work place supervision should be focused upon.
The authors have not declared any conflict of interests.
The authors are very grateful to Addis Ababa University, College of Heath Science, School of Public health and “Reduction of the burden of injuries and diseases due to occupational exposures through capacity building in low income countries” project for the financial support that enabled us to conduct this research. Their heartfelt thanks goes to Mugher Cement Factory workers who participated in this study for their willingness and active participation and the administrative staffs for their unreserved support. They extend their thanks to the data collectors and supervisors.
REFERENCES
|
Aderaw Z, Engdaw D, Tadesse T (2011). Determinants of occupational injury: A case control study among textile factory workers in Amhara Regional State, Ethiopia. J. Trop. Med.
Crossref
|
|
|
|
Andrina L (1998). Sixteenth International Conference of Labour Statisticians (ICLS). Geneva: International Labour Organization. International Labour Organization. Safety in numbers. Geneva (2003).
|
|
|
|
|
Bureau of Labor Statistics U.S Department of Labor (2013). National Census of Fatal Occupational injuries in 2012 (Preliminary Results).
|
|
|
|
|
Centers for Disease Control Prevention (2010). Occupational injuries and deaths among younger workers--United States, 1998-2007. Report No.: 1545-861X Contract No: 15. Ethiopian Ministry of Labour and Social Affairs (2008-2011).
|
|
|
|
|
Iqbal SA, Iqbal M, Taufiq MZ, Ahmed MS (2010). Identification of Occupational Injury among the Workers of Selected Cement Industries in Bangladesh-A Case Study. J. Chem. Eng. 25:22-28.
|
|
|
|
|
Kifle M, Engdaw D, Alemu K, Sharma HR, Amsalu S, Feleke A (2014). Work related injuries and associated risk factors among iron and steel industries workers in Addis Ababa, Ethiopia. Saf. Sci. 63:211-216.
Crossref
|
|
|
|
|
Labour Proclamation No.377/2003 (2004). Federal Negarit Gazeta of the Federal Democratic Republic of Ethiopia. February26:2453-504.
|
|
|
|
|
Marisol C, Deborah IN, Marilyn F, Timothy D, James L (2005). The Global Burden Due to Occupational Injury. Am. J. Ind. Med. 48:470-481.
Crossref
|
|
|
|
|
Occupational health (2001). A manual for primary health care workers. World Health Organization Regional Office for the Eastern Mediterranean, Cairo.
|
|
|
|
|
Sana S, Bhat G, Balkhi HM (2013). Health risks associated with workers in cement factories. Int. J. Sci. Res. Pub. 3(5):1-5.
|
|
|
|
|
Serkalem SY, Haimanot GM, Ansha NA (2014). Determinants of Occupational Injury in Kombolcha Textile Factory, North-East Ethiopia. Int. J. Occup. Environ. Med. 5(2):327-384-393.
|
|
|
|
|
Shafik SA, El-Mohsen ASA (2012). Occupational health: Health promotion program to improve health workers in Tourah Cement Factory. J. Am. Sci. 8(3):486-496.
|
|
|
|
|
Tadesse T, Kumie A (2007). Prevalence and factors affecting work-related injury among workers engaged in small and medium-scale industries in Gondar woreda, North Gondor zone, Amhara Regional State, Ethiopia. Ethiop. J. Health Dev. 21(1):25-34.
Crossref
|
|
|
|
|
Yessuf SS, Moges HG, Ahmed AN (2013). Magnitude and characteristics of occupational injury in Kombolcha Textile Factory, North East Ethiopia. Int. J. Occup. Safety Health 2:25-29.
|
|
|
|
|
Yiha O, Kumie A (2010). Assessment of occupational injuries in tendaho agricultural development SC, Afar Regional State, Ethiopia. J. Health Dev. 24(3).
|
|