Full Length Research Paper

ABSTRACT
Tinea capitis is a common infection among children in Nigeria and appropriate management will reduce its incidence among the pediatric population. The study assessed the opinions of mothers on the local and orthodox management of children infected with Tinea capitis. The study adopted a cross-sectional descriptive survey design and was conducted among 390 women in two states in Southern Nigeria. Pretested, translated questionnaires were administered to them in their various houses, and data analysis was done with SPSS version 20. Findings from the study showed that the majority of the mothers were older adults (42%). Higher percentages of the mothers reported choice of local products for management of Tinea capitis which includes toothpaste (60%), black soap (61%), lime (49%), and herbal cream (41%). However, 66 mothers reported the use of orthodox medication out of which Fulcin (52%) had the highest percentage with wrong prescriptions. In conclusion, mothers used more local products compared to orthodox medication in managing Tinea capitis among children and the effectiveness of such products, in the management of Tinea capitis have not been confirmed. Orthodox medicines were also used inappropriately. Public Health professionals should create awareness among mothers on the proper management of Tinea capitis.
Key words: Tinea capitis, local management, orthodox management, mothers.
INTRODUCTION
Tinea capitis (TC) is a dermatophyte of the scalp, found in many countries of the world and it mostly affects children. It inflicts a lot of psychosocial trauma due to attached social stigma, ulceration, and sometimes, irritation. It also hampers the pupil's concentration in class and it represents a potential source of secondary bacterial infection (Atraide et al., 2011). Researchers have documented the prevalence of TC in various countries (Pai et al., 2013; Zhan et al., 2015; Veasey et al., 2017; Lopez et al., 2018), with the highest number of cases found in Africa and Southern Europe (Oguzkaya Artan et al., 2013; Yehia et al., 2010). However, the prevalence of TC among children in Nigeria, most especially those attending public elementary schools is worrisome. The study by Adesiji et al. (2019) on TC among school children revealed that children between the ages of 4 and 7 years had the highest distribution of TC (67%), followed by those between the ages of 8 and 11 years (39%). In a study conducted by Afolabi et al. (2018) in Osun State, Nigeria, revealed 21.7% overall prevalence rate of TC among school children with the etiological agents consisting of Epidemophyton floccosum (12.0%), Microsporum gypseum (7.7%), Trichophyton mentagrophytes (7.7%) and Aspergillus niger (33%). Olarinoye et al. (2020) study found both non-inflammatory and inflammatory clinical types of TC among school children in North Central Nigeria.
Despite the overwhelming prevalence of TC in African nations, management practices remain a critical challenge. In the past, radiation therapy was used as a form of treatment before the advent of oral antifungal drugs. The children who were irradiated eventually developed brain cancer, despite their low-dose radiation exposure (Lubin et al., 2017). Currently, there are scientific and orthodox ways of treating TC which has been documented in the literature. Alkeswani et al., (2019) documented the use of Selenium sulfide for topical application and Grisofulcin for systemic application. The effectiveness of some of these drugs has also been confirmed in the literature (Gupta et al, 2018). In developed and developing countries, the management of the diseases includes both local and orthodox protocols. This has been documented by researchers and program planners (Anquez-Traxler, 2011; Asare, 2016; Ameade et al., 2018; World Health Organization, 2019). The literature has confirmed the use of many orthodox drugs in disease management, but many local products for disease management have not been proven scientifically. In Botswana, it has been documented that parents used local substances to manage skin infections (Ifebuzor et al., 2013). Li et al., 2020) reported that there is an increasing shift to local products in the management of disease conditions in Nigeria, where citizens have adopted local methods in the management of diseases such as diarrhea (Nwankwo, 2014), measles (Fatoba et al., 2019), and malaria (Ajayi et al., 2018).
The treatment of TC over the years has involved both systemic and topical applications. This is because, the pathogenic fungi are located within the hair and the combined effect of both systemic and topical drugs has been proven effective (Handler, 2018). The allylamines such as terbinafine and azoles group (ketoconazole, itraconazole, and fluconazole) have been recommended in the management of TC (El-Gohary et al., 2014).
These drugs have also been approved by the Nigeria Federal Ministry of Health (Federal Ministry of Health Nigeria, 2008). The FDA-approved pediatric treatment options for TC are griseofulvin and terbinafine (Brooks, 2013). In spite of the availability of these drugs in the country, anecdotal evidence has shown that TC is a chronic infection among children who also have the affected part exhibiting secondary bacteria infections.
In Nigeria, many studies conducted on TC have been on the prevalence of the disease (Adesiji et al., 2019; Afolabi et al., 2018), identifying causative organisms (Olarinoye et al., 2020), and exploring the burden and psychological impact of the disease (Fienemika and Okeafor, 2018). However, there is little or no effort in identifying the management strategy for the disease in children most especially at the community level. This study, therefore, aimed at assessing the opinions of mothers on the local and orthodox management strategy for Tinea capitis of children in two communities in Southern Nigeria. It also determined the association between their sociodemographic variables and the use of local and orthodox products in the management of TC.
MATERIALS AND METHODS
Design and setting
The study adopted a cross-sectional descriptive survey design and it was conducted in Edo and Osun States, Nigeria. Ife Central and Ife East Local Government Areas of Osun State as well as Oredo and Egor Local Government Areas (LGAs) of Edo State were purposively selected for the study. These LGAs are where indigenes, mostly reside and 10 communities were purposively selected for the study (Figures 1). The residents of the communities are also known for holding tenaciously to old traditions and for enforcing local practices on their inhabitants.
Sample and sampling
The sample size for the study was determined using Pagano and Gauvreau (2000) formula for calculating sample size

The prevalence of TC among school children in Osun State was 35% (Oke et al., 2014) while that of Benin in Edo State was 13.4% (Enweani et al., 1996). Based on these values the difference (P1-P2) in this proportion was calculated to be 21.6%. P = Pooled or weighted average of P1and P2,= 24.2%;n1= mothers’ sample from Osun State. n2 = mothers’ sample from Edo State with n1 = n2. Z crit= (Standard Normal Deviate) corresponding to selected Significance Criteria at 0.05 and Confidence Intervals of 95%. Z pwr= (Standard Normal Deviate) corresponding to selected Statistical Powers of 0.80. Therefore n = 354.89 and after adding a 10% non-response rate, a total sample size of 390 was obtained. Therefore, 195 mothers from each of the two states were selected.
Instruments
A semi-structured questionnaire which consisted of two sections was used for data collection.
Section A contained 10 listed local products commonly used for management of skin infections in Nigeria, on a dichotomous scale of Yes and No, and elicited responses on local management of TC. The section also contained open ended questions on other local management choices that were not captured on the list. Section B contained open ended questions asking the mothers to list the orthodox drugs commonly used in managing TC of children and the methods of use. The questionnaire was translated into local languages for those who could not read or write in English.
Pilot study and pretest of instrument
The pilot study was conducted in Ile Ife among 20 non-indigenous mothers to determine the feasibility of the study and to also pretest the questionnaire. The pilot study revealed that the majority of the mothers used local methods of management. Questions that appeared to be ambiguous were reworded for clarity. Richardson formula for determining reliability for dichotomous variables was used and a reliability coefficient of 0.7 was obtained.
Research assistants
Two research assistants who could read and write the indigenous languages were recruited for the study. The assistants were trained on the recruitment of participants, obtaining informed consent from them, and administration of the questionnaire using interviewer-administered mode.
Sampling and data collection
The research team went from house to house to recruit the mothers using purposive sampling technique. The inclusion criteria for recruitment were that mothers should be indigenes of the communities and must have at least nursed a child up to the elementary school level. The questionnaire was administered in the evening and weekends when the mothers were back from their workplaces. The interviewer-administered mode was adopted for those who could not read or write English.
Ethics
Ethical approval for the study was obtained from the Health Research and Ethics Committee of the Institute of Public Health, Obafemi Awolowo University, and also from the Research Ethics Committee, College of Medical Sciences, University of Benin. Letter of introduction from the Department of Nursing Science, OAU seeking permission to collect data were given to the traditional rulers in the study settings, and permission to enter the communities was obtained from them. Translated Informed Consent Form was administered to the participants before data collection.
Data analysis
The dichotomous scale was scored as Yes (1) and No (2). Responses to the open ended questions were converted to frequencies and percentages while methods of use of orthodox drugs were presented in prose. Pearson Chi-square test was conducted to determine the association of education and occupation of mothers with the use of local and orthodox products.
RESULTS
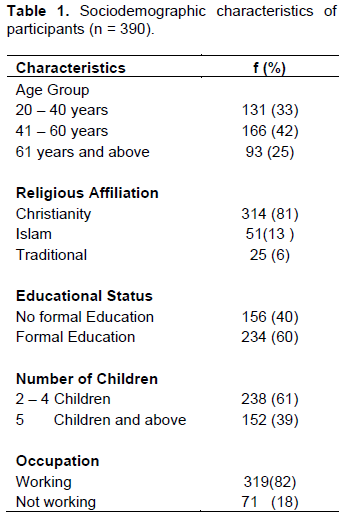
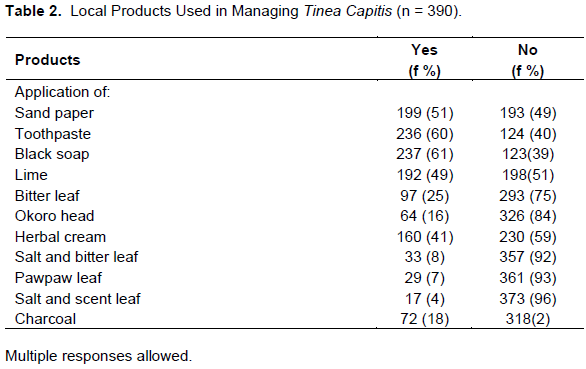
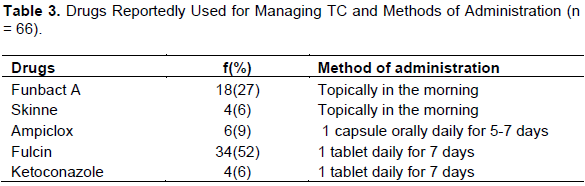
The majority of the mothers had formal education, 60 and 82% of the participants were working, 42% of them were between the ages of 41 and 60 years (Table 1). Higher percentages of the mothers that indicated their choice of management for TC reported local products which include the use of black soap (61%), toothpaste (60%), sandpaper (51%), lime (49%), and herbal cream (41%) (Table 2). A significant association was not found between the use of local products and education of mothers (x2 = 2.19; p = 0.14; df = 1) as well as their occupation (x2 = 0.16; p = 0.69; df = 1). The open ended questions revealed the following responses on other local products used for TC which are: Gbogbonise (concoction claimed to cure all diseases) (12%); garlic (3%); motor brake oil (10%), used engine oil (4%); charcoal (3%); cigarette ash (3%); potash (6%); camphor (4%); kitchen cobwebs (17%); candle bush (Araghomiasol) leaves (13%); torchlight battery (2%); stale soup (1%); corn cob (1%); ground broken plate (3%); and salt (1%). Of the 390 participants, only 66 of the mothers listed drugs used by them in the treatment of TC. The most reported drugs used by the 66 mothers who administered drugs to their children are Fulcin (52%) and Funbact A (27%) (Table 3). A significant association was not found between the use of orthodox products and education of mothers (x2 = 1.19; p = 0.28; df = 1) as well as their occupation (x2 = 2.42; p = 0.12; df = 1).
DISCUSSION
The present study demonstrated that mothers reported use of local and orthordox products for managing TC which are unique findings different from previous African studies on prevalence of Tinea capitis and its aetiological agents (Thakur, 2013; Moto et al., 2015; Veasey et al., 2017; Lopez et al., 2018). There are limited studies on mothers’ opinions on the management of TC of infected children.
The sociodemographic characteristics of the mothers showed that the education and occupation of the mothers were not significantly associated with the use of both local and orthodox products for managing TC. This is not in line with the study of Yuan et al. (2015) which was conducted in rural China indicated that education influences health knowledge as well as health promotion activities. In this study, it can be inferred that treatment choices adopted by mothers for TC of their children are acquired from the society which must have been passed down from generation to generation. The socio-demographic characteristics of the mothers are not factors to be reckoned with in determining the treatment choices for TC.
The study revealed that higher percentage of mothers reported the use of local products for the treatment of TC.
This is in consonance with the findings of Li et al. (2020) who reported high prevalence of use of herbal medicine among adult women in Nigeria. This might explain why there are many chronic cases of TC among children because the skin condition would not have been treated with appropriate medicine. Aside from this, some of these products such as torchlight batteries, camphor, and used engine oil may be very harmful to health. However, those that seem not to be harmful are also not appropriate for use as those products’ dosages, and effectiveness have not been reported to be scientifically proven for the treatment of TC. Nevertheless, it is important to expose these products to scientific inquiry and testing to determine which of them is effective in managing TC, and such should be officially recommended to mothers and other stakeholders. Also, local products such as bitter leaf, black soap, and pawpaw leaves are effective medicinal products for some disease conditions (Alabi and Adeyemi, 2021; Ogunbiyi and Enechukwu, 2021) but their efficacy in TC management has not been ascertained. The use of these local products in managing TC may be a contributory factor for the chronicity of the condition among children. Therefore, an urgent community health intervention is paramount for the proper management of the disease condition.
The study showed that mothers reported low use of scientifically approved drugs for the treatment of Tinea capitis of infected children. This is a cause for concern. This finding is contrary to the study done in Nigeria by Mustapha et al. (2016) which revealed that participants preferred orthodox medicine for treating disease conditions. In this study, the mothers who reported the use of drugs use them inappropriately and also use drugs not recommended for the treatment of TC. For example, the use of Fulcin which is an antifungal drug was reported to be used as one tablet, daily for 7 days. Fulcin is a drug used for weeks for effective results (Mayser et al., 2020). Some other antifungal drugs were also reported to be used by the mothers (Table 3) but all the drugs were inappropriately used for their children. In addition, the antibiotic that was reported, (Ampiclox) could have been used in a case of bacterial infected TC or used directly to manage TC. Whichever case the drug was used, Ampiclox is not the drug of choice for TC and if it was used to treat a bacterial infection, the dose and dosages reported were inappropriate. The use of orthodox drugs in managing TC most especially antifungal drugs are effective and mothers should be encouraged to patronize health care facilities to receive appropriate treatment for managing TC of their infected children. Appropriate treatment will also reduce the psychological impacts that children infected with TC usually expérience as documented in previous study (Fienemika and Okeafor, 2018).
CONCLUSION
The study concluded that mothers reported the use of both local and orthodox medicine for the treatment of TC of infected children. The local products used have not been scientifically proven for managing TC while the orthodox medicines used were inappropriately administered.
Implications for public health professionals
Public Health professionals have significant responsibilities in reducing the occurrence of TC among children in their communities. They can do this by creating awareness on the appropriate management of TC among mothers either at the primary health care centers during infant welfare clinic or antenatal clinic. They can also integrate the awareness program as part of their intervention programs for parents at various settings such as schools, market places, religious places, and other settings where mothers can be located. Children infected with TC can also be identified at schools and other settings, while mothers of such children are assisted to access adequate treatment for the skin disease.
LIMITATIONS
The area of study was large hence, accessing some of these mothers was difficult because, most of the time, they were away to their business locations during work hours hence, these mothers were contacted during weekends. Given that the study was only carried out in two states in Nigeria, the findings cannot be generalized as being representative of what obtains in the entire country.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adesiji YO, Omolade FB, Aderibigbe IA, Ogungbe O, Adefioye OA, Adedokun SA, Adekanle MA, Ojedele R (2019). Prevalence of Tinea Capitis among Children in Osogbo, Nigeria, and the Associated Risk Factors. Diseases 7(1):13. |
|
|
Afolabi OT, Oninla O, Fehintola F (2018). Tinea capitis: A tropical disease of hygienic concern among primary school children in an urban community in Nigeria. Journal of Public Health and Epidemiology10(9):313-319. |
|
|
Ajayi CO, Elujoba AA, Adepiti AO (2018). Preliminary phytochemical investigation on Mama powder - An approved herbal antimalarial in Nigeria. American Journal of Ethnomedicine 5(12):64-66. |
|
|
Alabi QK, Adeyemi WJ (2021). Vernonia amygdalina (Del) as an antioxidant, aspirin toxicity, and oxidative stress. In: V. B. Patel & V. R. Preedy (Eds.), Toxicology (pp. 491-504). Academic Press. |
|
|
Alkeswani A, Cantrell W, Elewski B (2019). Treatment of Tinea Capitis. Skin Appendage Disorders 5(4):201-210. |
|
|
Ameade P, Kwame Baba, MM, Iddrisu NU, Musah AA, Gbe SY (2018). Herbal Pharmacovigilance?: Are Ghanaian Herbal Medicine Practitioners Equipped Enough to Assist in Monitoring the Safety of Herbal Medicines? - A Survey in Tamale, Ghana. Chronicles of Complementary, Alternative and Integrative Medicine 2018(1):1-10. |
|
|
Anquez-Traxler C (2011). The Legal and Regulatory Framework of Herbal Medicinal Products in the European Union: A Focus on the Traditional Herbal Medicines Category. Drug Information Journal 45(1):15-23. |
|
|
Asare B (2016). Developments made in herbal medicine practice in Ghana. Modern Ghana. |
|
|
Atraide DD, Akpa MR, George IO (2011). The pattern of skin disorders in a Nigerian tertiary hospital. Journal of Public Health and Epidemiology 3(4):177-181. |
|
|
Brooks M (2013). FDA Approves New Topical Antifungal Luliconazole 1%. Medscape Medical News. |
|
|
El-Gohary M, van Zuuren EJ, Fedorowicz Z, Burgess H, Doney L, Stuart B, Moore M, Little P (2014). Topical antifungal treatments for tinea cruris and tinea corporis. Cochrane Database of Systematic Reviews 8 p. |
|
|
Enweani IB, Ozan CC, Agbonlahor DE, Ndip RN (1996). Dermatophytosis in schoolchildren in Ekpoma, Nigeria. Mycoses 39(7-8):303-305. |
|
|
Fatoba PO, Adeyemi SB, Adewole AA, Fatoba MT (2019). Medicinal plants used in the treatment of infant diseases in south western Nigeria. Nigerian Journal of Basic and Applied Sciences 26(1):14. |
|
|
Federal Ministry of Health Nigeria (2008). Standard treatment guidelines. |
|
|
Fienemika AE, Okeafor CU (2018). The Identification and Grading of the Psychosocial Impact of Tinea capitis in Primary School Children in a Semi-urban Area of Rivers State, Nigeria. Nigerian Postgraduate Medical Journal 24(1):19-26. |
|
|
Gupta AK, May RR, Verstteeg SG, Piraccini BM, Tsti A, Friedland SF (2018). Tinea capitis in children: a systematic review of management. J Eur Acad Dermatoll Venenol 32(12):2264-2274. |
|
|
Handler MZ (2018). Tinea Capitis: Presentation and Management. Medscape Medical. |
|
|
Ifebuzor DC, Mabuza LH, Malete NH, Govender I (2013). The perceptions of parents about the skin conditions of their children presenting with comorbid fungal skin infections in Francistown, Botswana. African Journal of Primary Health Care and Family Medicine 5(1):1-6. |
|
|
Li S, Odedina S, Agwai I, Ojengbede O, Huo D, Olopade OI (2020). Traditional medicine usage among adult women in Ibadan, Nigeria: a cross-sectional study. BMC Complementary Medicine and Therapies 20(1):93. |
|
|
Lopez C, Marillo A, Trujillo P (2018). Cross sectional study: Superficial mycoses in school children of a rural Parish of Cuenca, Ecuador. Rev Med HJCA 9:249-254. |
|
|
Lubin JH, Adams MJ, Shore R, Holmberg E, Schneider AB, Hawkins MM, Robison LL, Inskip PD, Lundell M, Johansson R, Kleinerman RA, De Vathaire F, Damber L, Sadetzki S, Tucker M, Sakata R, Veiga LHS (2017). Thyroid cancer following childhood low-dose radiation exposure: A pooled analysis of nine cohorts. Journal of Clinical Endocrinology and Metabolism 102(7):2575-2583. |
|
|
Mayser P, Nenoff P, Reinel D, Abeck D, Brasch J, Daeschlein G, Effendy I, Ginter-Hanselmayer G, Gräser Y, Hipler UC, Höger P, Kolb-Mäurer A, Ott H, Schaller M, Zidane M (2020). S1 guidelines: Tinea capitis. Journal of the German Society of Dermatology 18(2):161-179. |
|
|
Moto JN, Maingi JM, Nyamache AK (2015). Prevalence of Tinea Capitis in school going children from Mathare, informal settlement in Nairobi, Kenya. BMC Research Notes 8(1):274. |
|
|
Mustapha KB, Kirim RA, Ibrahim JA, Onuche PU, Bakare-Odunola MT (2016). Perception of use of herbal and orthodox medicines in parts of Abuja: A pilot study. Journal of Applied Pharmaceutical Science 6(9):128-132. |
|
|
Nwankwo IU (2014). Resilience of Folk Medicine Among the Igbos of Southeast Nigeria. European Scientific Journal 10(36):177-187. |
|
|
Ogunbiyi A, Enechukwu NA (2021). African black soap: Physiochemical, phytochemical properties, and uses. Dermatologic Therapy 34(3):1-7. |
|
|
Oguzkaya Artan, M, Koc A, Baykan Z, Buldu H (2013). Prevalence of Tinea Capitis in Primary School Children. International Journal of Medical Investigation 1(2):104-110. |
|
|
Oke OO, Onayemi O, Olasode OA, Omisore AG, Oninla OA (2014). The prevalence and pattern of superficial fungal infections among school children in ile-ife, south-western nigeria. Dermatology Research and Practice2014. |
|
|
Olarinoye GM, Katibi OS, Ilesanmi ON, Fayemiwo SA, Ogunbiyi AO,George AO (2020). Trichoscopic features of tinea capitis among primary school children in north central Nigeria. International Journal of Dermatology 59(11):1346-1352. |
|
|
Pagano M, Gauvreau K (2000). Principles of Biostatistics (2nd ed.). Duxbury. |
|
|
Pai VV, Hanumanthayya K, Tophakhane RS, Nandihal NW, Naveen KNS (2013). Clinical study of Tinea capitis in Northern Karnataka: A three-year experience at a single institute. Indian Dermatology Online Journal 4(1):22. |
|
|
Thakur R (2013). Tinea capitis in Botswana. Clinical, cosmetic and investigational dermatology 3(6):37-41. |
|
|
Veasey JV, Miguel BAF, Mayor SAS, Zaitz C, Muramatu LH, Serrano J A (2017). Epidemiological profile of tinea capitis in São Paulo City. Anais Brasileiros de Dermatologia 92(2):283-284. |
|
|
World HealthOrganization (WHO) (2019). WHO global report on traditional and complementary medicine 2019. World Health Organization. |
|
|
Yehia MA, El-Ammawi TS, Al-Mazidi KM, El-Ela MAA, Al-Ajmi HS (2010). The spectrum of fungal infections with a special reference to dermatophytoses in the Capital area of Kuwait during 2000-2005: A retrospective analysis. Mycopathologia 169(4):241-246. |
|
|
Yuan F, Qian D, Huang C, Tian M, Xiang Y, He Z, Feng Z (2015). Analysis of awareness of health knowledge among rural residents in Western China. BMC Public Health 15(1):1-8. |
|
|
Zhan P, Geng C, Li Z, Jin Y, Jiang Q, Tao L, Luo Y, Xiong Z, Wu S, Li D, Liu W, De Hoog GS (2015). Evolution of tinea capitis in the Nanchang area, Southern China: A 50-year survey (1965-2014). Mycoses 58(5):261-266. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


