Full Length Research Paper

ABSTRACT
Pre-eclampsia/Eclampsia has significant impact on maternal and perinatal health. Little is known about prevalence and risk factors for pre-eclampsia/eclampsia in Tanzania. This study aimed to determine prevalence and risk factors for pre-eclampsia/eclampsia among women who delivered at KCMC hospital between 2000 and 2014. Retrospective cross-sectional study was conducted at KCMC medical birth registry. Multivariable logistic regression models were performed to obtain odds ratios with 95% CI for factors associated with pre/eclampsia. P-value<0.05 was considered statistically significant. A total of 40,176 mothers were analysed. The prevalence of pre/eclampsia was 4.2%. Factors such as maternal age (≥35) years (AOR = 1.73), ≥12 years of schooling (AOR=1.29), being unmarried (AOR=2.03), overweight (AOR=1.99), obesity (AOR=5.52), hypertension (AOR=18.66), anaemia (AOR=3.53), and multiple pregnancy (AOR=6.58), were associated with higher risk of pre-eclampsia/eclampsia while ANC visits (≥4) reduced the risk of pre-eclampsia (AOR= 0.78). This study provides an estimate of prevalence of pre-eclampsia at KCMC hospital in Northern Tanzania. Factors such as advanced maternal age (≥35 years), ≥12 years of schooling, being unmarried, overweight, obesity, hypertension, anaemia and multiple pregnancy were associated with higher risk of pre-eclampsia while having ≥4 ANC visits reduced the risk of pre-eclampsia at KCMC.
Key words: Prevalence, pre-eclampsia, eclampsia, risk factors, Tanzania.
INTRODUCTION
Pre-eclampsia is defined as multisystem disorder characterised by high blood pressure (≥140/90 mmHg) and increased proteinuria (≥0.3 g/day) in previous normotensive women, while eclampsia is defined as the occurrence of one or more convulsions preceded by changes in cardiac structure and function in association with the pre-eclampsia syndrome(WHO, 2011).Pre-eclampsia is the second leading cause of maternal death,and it has been associated with maternal morbidity and adverse perinatal outcomes globally (Firoz et al., 2011).
The global prevalence of pre-eclampsia has beenestimated to be 4% (Bilano et al., 2014). The prevalence of pre-eclampsia in sub Saharan African has been reported to be high as up to 16% (Guerrier et al., 2013). In low and middle income countries, pre-eclampsia has been reported to cause almost a third of a million maternal deaths (Lozano et al., 2011). Hypertensive disorders of pregnancy including pre-eclampsia/eclampsia accounts for about 18% of all maternal deaths globally, with an estimate of sixty two to seventy seven thousand deaths per year (Khan et al., 2006). In Nigeria, pre-eclampsia is reported to be associated with 5.84/1000 births perinatal mortality rate (Makinde, 2012). Locally in Tanzania, eclampsia is associated with 11% case fatality rate and 30% mortality rate (Mooij et al., 2015).
Several studies have documented risk factors for pre-eclampsia. A global survey involving low and middle income countries (WHO secondary analysis) revealed that advanced maternal age, low maternal education prim parity, high maternal body mass index (BMI), chronic hypertension, cardiac or renal disease, gestational diabetes mellitus, lack of antenatal visits, urinary tract infection, and severe anaemia were associated with increased risk of pre-eclampsia (Bilano et al., 2014).
A systematic review and meta-analysis of large cohort studies aiming to determine clinical risk factors for pre-eclampsia in early pregnancy reported that women with antiphospholipid antibody syndrome, history of pre-eclampsia, chronic hypertension, pre-gestational diabetes, high body mass index and those who use assisted reproductive technology have high risk of pre-eclampsia (Fang et al., 2009; Kiondo et al., 2012; Aksornphusitaphong and Phupong, 2013; Bartsch et al., 2016).
In this paper, the term pre-eclampsia/eclampsia is used to refer to both conditions (having pre-eclampsia either with or without progressing to eclampsia).
Despite the advance understanding of the adverse impact of pre-eclampsia on maternal and perinatal health, there remains limited information regarding the prevalence and risk factors for pre-eclampsia/eclampsia in Tanzania. Understanding the prevalence and associated risk factors of pre-eclampsia/eclampsia is important for the clinical management of preconception and pregnant women to enable development of strategies and interventions to prevent complications attributed to preeclampsia. This study aimed to determine prevalence and risk factors associated with pre-eclampsia in Northern Tanzania.
METHODOLOGY
Study designs and settings
A retrospective cross-sectional study was performed using Kilimanjaro Christian Medical Centre (KCMC) medical birth registry for all women who delivered at the department of obstetrics and gynaecology at KCMC for the period of 2000 to 2014. Kilimanjaro Christian Medical Centre is one of four referral hospitals in Tanzania located in Moshi, Kilimanjaro region in North of Tanzania. The hospital receives women from nearby communities and referrals from the nearby regions such as Arusha, Manyara and Tanga. The hospital has an average of 4000 deliveries per year. By the end of December 2014, a total of 40,176 women were recorded to have delivered at KCMC medical birth registry. These women contributed to 50,807 deliveries in total. Of these, 133 (0.3%) deliveries were excluded from the analysis due to missing record on pre-eclampsia/eclampsia status. Thus the remaining 50,807 deliveries were analysed.
Data source
The KCMC medical birth registry has been operating since July 2000. The detail of the medical birth registry has been well described elsewhere (Mahande et al., 2013). In short, all women who give birth at KCMC were assigned with a unique hospital identification number which is constant for subsequent births that occur at KCMC for each woman. This enables us to link each woman with their respective siblings in subsequent pregnancy/birth.
Trained midwives collected all information of mothers using a standardized questionnaire within 24 h of hospital delivery, or as soon as a mother has recovered from birth. Furthermore, additional information are extracted from patient files and mothers are also asked to bring their antenatal cards for more clarification on prenatal information such as antenatal care visits, maternal weight, and blood pressure measurements. Finally, all data were entered and stored in a computerised data base system at the birth registry.
Study variables
Pre-eclampsia and eclampsia were the dependent variable and were combined into a single dependent variable. The dependent variable was based on having the recorded diagnosis (1 for those with the outcome and 0 for those without the outcome).
Independent variables
Independent variables included maternal socio-demographic characteristics such as maternal age at the time of birth which was recorded as continuous, then was classified into three categories ( ≤19, 20-34 and ≥35 years), marital status was dichotomized into married and unmarried, maternal educational level based on the number of years of schooling, maternal body mass index (BMI) was computed as the ratio of maternal weight in kilograms divided by maternal height in meters, number of antenatal care visits recorded as continuous which was then categorized into less than 4 and ≥4 ANC visits (as per World Health Organization recommendation) and it was determined based on the clinical records as indicated on the ANC card and patient file. Maternal clinical conditions included chronic hypertension, gestational diabetes, renal disease, and anaemia based on the recorded diagnosis (yes or no).
Ethical consideration
This study was approved by Kilimanjaro Christian Medical University College Research and Ethics Review Committee (CRERC) with certificate number 734. Permission to conduct the study was obtained from Kilimanjaro Christian Medical Centre administrative authority. Written consents were obtained from all mothers prior to the interview after they had been fully explained about the objectives of the medical birth registry project. Participants were also informed that participation in the study was on voluntary basis and the refusal to participate had no impact to their hospital care. Both confidentiality and privacy were ensured where participant hospital identification numbers were used instead of names. Interviews were conducted in a privacy room.
Statistical analysis
Data analysis was performed using STATA version 13 (www.stata.com). Descriptive statistics were summarized using frequencies and proportion. To determine the potential risk factors for pre-eclampsia, multivariable analysis was performed to calculate odds ratio (ORs) and 95% confidence intervals (CIs). A p-value of less than 0.05 was considered statistically significant. Confounding was assessed by entering potential confounders into a logistic model one at a time, and by comparing the adjusted and crude odds ratios. A variable was considered to be confounder if its inclusion in the model changed ORs for the outcome variables (pre-eclampsia/eclampsia) associated with risk factors by at least 10%. Considering the relationship between BMI and other variables (maternal age, chronic hypertension and gestational diabetes), the effect of BMI on pre-eclampsia/eclampsia was adjusted for maternal age, chronic hypertension and gestational diabetes.
RESULTS
Demographic characteristics of the study participants
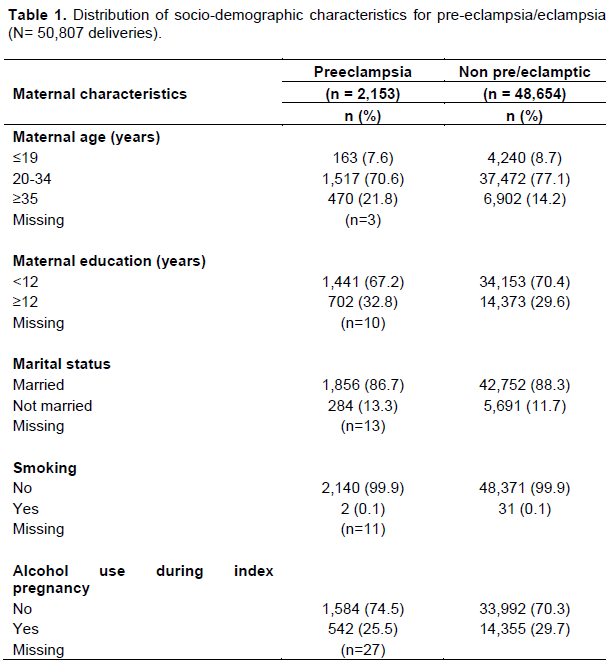
A total of 40,176 women were studied. These women contributed to a total of 50,807 deliveries. Socio-demographic characteristics of the study participants are shown in Table 1. The prevalence of pre-eclampsia was 4.2% (2,153/50,807). Compared to women with normal pregnancy, those who have pre-eclampsia were more likely to have >35 years (21.8% vs. 14.2%), respectively, less than twelve years of education (67.2% vs. 70.4%), being unmarried (13.3% vs. 11.7%) and not using alcohol during the current pregnancy (25.5% vs. 29.7%).
The clinical characteristics of women with pre-eclampsia and those without are summarised in Table 2.
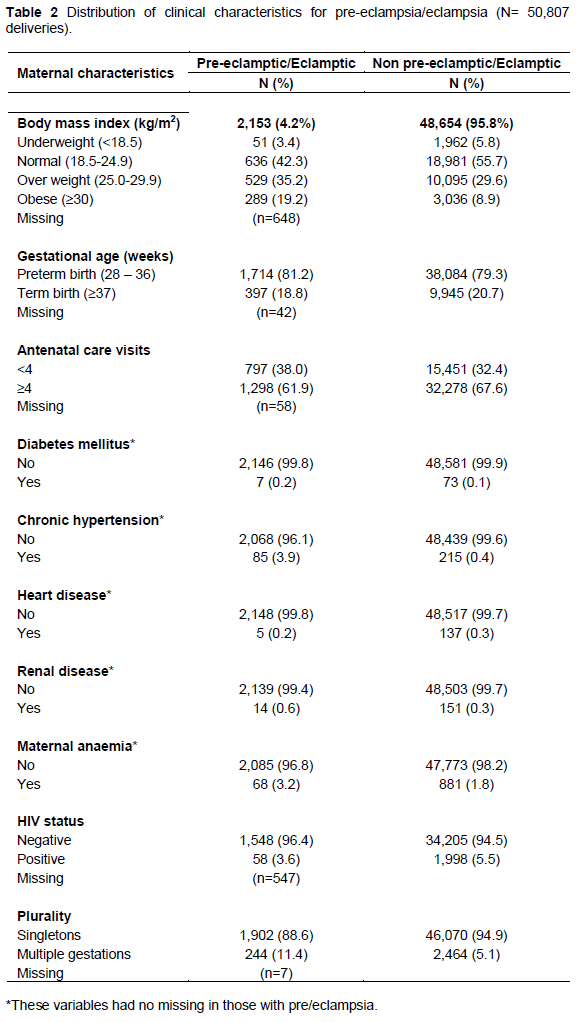
Compared to non-pre-eclamptic/eclamptic women, women with pre-eclampsia were more likely to be overweight (35.2% vs. 29.6%), obese (19.2% vs. 8.9%), have chronic hypertension (3.9% vs. 0.4%), have gestational diabetes (0.2% vs. 0.1%), have renal disease (0.6% vs. 0.3%), have maternal anaemia (3.2% vs. 1.8%) and to have multiple pregnancy (11.4% vs. 5.1%).
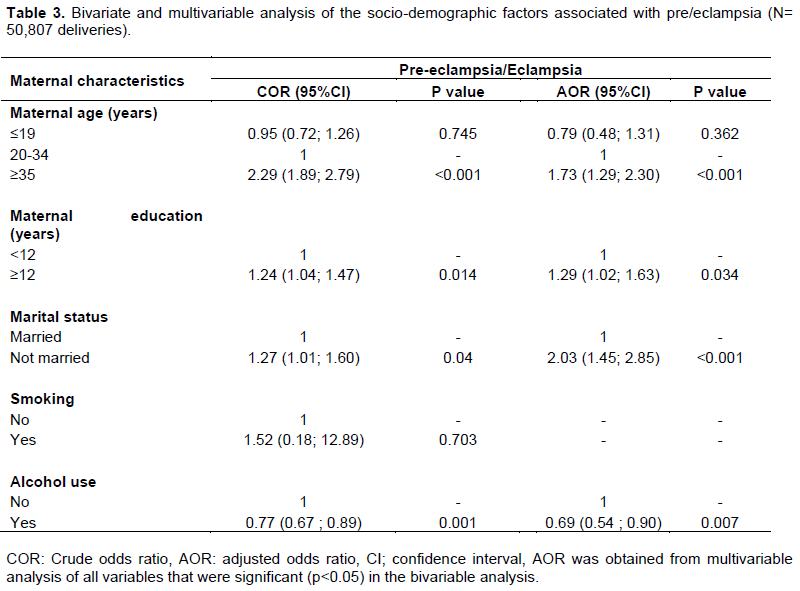
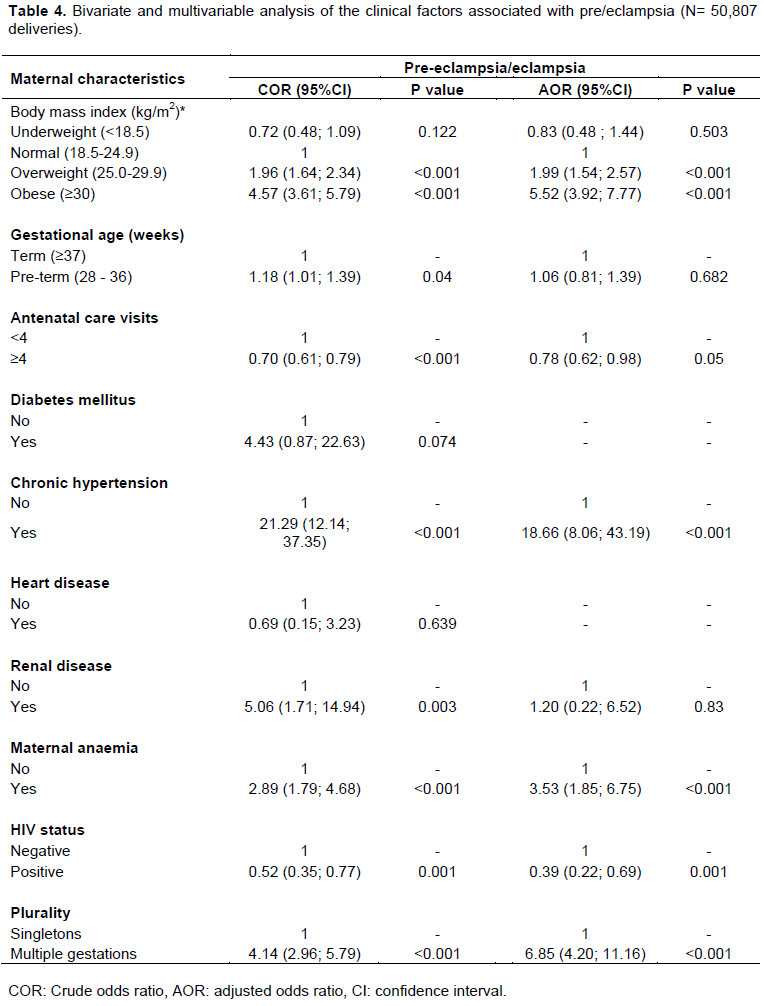
Risk factors for pre-eclampsia
The risk factors associated with pre-eclampsia/eclampsia were estimated in a multiple logistic regression models (Tables 3 and 4). Some sociodemographic variables such as advanced maternal age of >35 years (AOR=1.73, 95% CI: 1.29-2.30), having 12 or more years of education (AOR=1.29, 95% CI: 1.02-1.63), and being unmarried (AOR=2.03, 95% CI: 1.45-2.85) were significantly associated with an increased risk of pre-eclampsia/eclampsia (Table 3). Regarding clinical factors, overweight (AOR=1.99, 95% CI: 1.54- 2.57), or being obese (AOR=5.52, 95% CI: 3.92-7.77), chronic hypertension (AOR=18.66, 95% CI: 8.06-43.19), maternal anaemia (AOR=3.53, 95% CI: 1.85-6.75), nd multiple pregnancy (AOR=6.85, 95% CI: 4.20-11.16) were also associated with an increased risk of pre-eclampsia/eclampsia (Table 4).
DISCUSSION
In this study, it was found that the prevalence of preeclampsia was 4.2%. Advanced maternal age (≥ 35 years), maternal low education, being unmarried, maternal overweight, obesity, chronic hypertension, maternal anaemia and multiple pregnancy all were associated with an increased risk of developing pre-eclampsia/eclampsia.
The prevalence of pre-eclampsia/eclampsia in this study is consistent with the global prevalence of 4.0% (Bilano et al., 2014). This rate was higher than 1.2% that was reported among Nigerian women (Kooffreh et al., 2014). But it is within the range of prevalence of pre-eclampsia/eclampsia in developing countries of 1.8 to 16.7% (Kayode et al., 2011). A multicounty survey involving 29 countries from Africa, Asia, Latin America and Middle East reported that 2.73% women suffer pregnancy hypertensive disorders whereby 0.29% had chronic hypertension, 2.73% had pre-eclampsia and 0.28% had eclampsia (Abalos et al., 2014). In Tanzania, little is documented about prevalence of pre-eclampsia. However, it is associated with 11% case fatality rate (Mooij et al., 2015). The difference in prevalence of pre-eclampsia/eclampsia between this study and that of others could be explained by the difference in risk factors between the studied populations or it could be due to the difference in management of the women at risk of pre-eclampsia/eclampsia between settings. The high prevalence of pre-eclampsia/eclampsia highlights the needs for appropriate intervention such as early identification of high risk women and provision of pre-pregnancy counselling for early identification of modifiable risk factors for pre-eclampsia/eclampsia.
In this study, it was found that chronic hypertension, being overweight or obese were significantly associated with increased odds of having pre-eclampsia/eclampsia. Similar findings have been reported elsewhere (Guerrier et al., 2013; Bilano et al., 2014) and this relationship could be due to the mechanical vasoconstriction of the uterine arteries causing increased blood pressure hence development of pre-eclampsia. Obese women are likely to be hypertensive and hence increased risk of developing pre-eclampsia. The association between overweight and obese with pre-eclampsia remained significant even after controlling for potential confounder such as maternal age, chronic hypertension and gestational diabetes. The possible explanation for this may be that overweight and obese mothers could have placental endothelial dysfunction and thus could lead into development of pre-eclampsia as it has been reported by previous investigators (Ganesh et al., 2010).
In the present study, mothers with multiple pregnancies were found to have 7-fold increased odds of having pre-eclampsia as compared to those who had singleton delivery. This could be explained by the fact that mothers with multiple pregnancies have increased placental mass that may relatively cause placental hypoxia hence development of pre-eclampsia (Wong et al., 2007; Bdolah et al., 2008). Also, maternal anaemia was found to be associated with higher odds of having preeclampsia/eclampsia; this could be due to deficiency of micronutrients and antioxidants. The reduction in serum levels of calcium, magnesium and zinc during pregnancy might contribute to development of pre-eclampsia (Ali et al., 2011; Bilano et al., 2014).
Being not married was found to have increased odds of pre-eclampsia/eclampsia; being unmarried could be associated with change of partner or increased interpregnancy interval which may lead to the development of pre-eclampsia/eclampsia (Bilano et al., 2014). Unfortunately, these factors were not assessed in the present study. Advanced maternal age (≥35 years) was found to be associated with increased odds of having pre-eclampsia/eclampsia. This finding is consistent with previous study (Bilano et al., 2014). The increased risk of pre-eclampsia with higher maternal age could be due to maternal immune mal-adaptation and aging-mediated vascular damage or could be attributed by chronic hypertension.
In this study, it was found that women with high education level (12 or more years of schooling) had increased odds of having pre-eclampsia/eclampsia than their counterparts with lower education. The increased risk of pre-eclampsia among women with high education level could be due to the fact that, in Tanzania, people with high income are more likely to fall into those people with moderate/middle income to high income. Individuals in this group are practicing poor life style practices including lack of physical exercise and poor eating habits such as eating/access to unhealthy foods that could lead to overweight or obese which increases the risk of developing pre-eclampsia/eclampsia. In the other hand, the increased risk of preeclampsia among women with high education could be attributed by increased maternal age, as women with higher education achievement are more likely to have their child at advanced maternal age. However, a study conducted in Uganda has reported higher education to be protective against pre-eclampsia/eclampsia (Kiondo et al., 2012).
The association between fewer antenatal care visits and an increased risk of pre-eclampsia/eclampsia could be explained by the fact that, most women with pre-eclampsia are more likely to be admitted/hospitalized thereby reducing their chances to attend the ANC clinics. Their clinical encounter would therefore more likely to be through in-patient services rather than out-patients services (ANC clinics). It was also found that being HIV positive was protective against pre-eclampsia/eclampsia; HIV has been shown to inhibit maternal inflammatory response and thus prevent development of pre/eclampsia. Similar findings have been reported elsewhere (Landi et al., 2014). Knowing the factors associated with pre-eclampsia will be very useful to the clinicians, thus during the antenatal clinics all pregnant mothers should be screened for the risk factors and be managed accordingly.
However, in Tanzania, pre-eclampsia is associated with abruption placentae, high maternal mortality rate leading to adverse perinatal outcomes (Illah et al., 2013; Macheku et al., 2015). Management of pre-eclampsia includes provision of MgSO4 and close follow up during antenatal clinics. Despite availability of these services, pre-eclamptic mothers need extra care in order to control the disease and its associated adverse perinatal outcomes (Urassa et al., 2006; Muganyizi and Shagdara, 2011).
This study has a number of limitations which needs to be taken into account while interpreting our results. Hospital based data was used; this may result to selection bias. Therefore, the present findings may not be generalized to the general population. Furthermore, KCMC is a referral hospital so there is greater number of referred complicated deliveries which may lead to overrepresentation of high risk group of pregnancy women. In addition, some risk factors for pre-eclampsia such as family history of pre-eclampsia, history of pre-eclampsia, interpregnancy interval and paternity change between pregnancies were not assessed in this study.
Therefore, the overall effects of these factors on the observed finding were not quantified.
Despite these limitations, the medical birth registry has detailed information on pregnancy and delivery as well as mothers’ reproductive history. This information enabled us to study the most important risk factors for the outcome of interest and we were able to adjust some potential confounders. The use of linked data minimized the effect of recall bias. The large sample size allowed us to estimate significantly the prevalence of pre-eclampsia/eclampsia and associated factors with a higher precision.
CONCLUSION
Prevalence of pre-eclampsia in Northern Tanzania is 4.2%. Factors such as advanced maternal age (≥35 years), ≥12 years of schooling, being unmarried, overweight, obesity, chronic hypertension, anaemia and multiple pregnancy were significantly associated with higher risk of pre-eclampsia while having ≥4 ANC visits reduced the risk of pre/eclampsia in Northern Tanzania. Therefore, pre-eclampsia/eclampsia remains a significant concern for women in this region. Early identification of these factors and providing targeted interventions to at-risk women may reduce the prevalence and subsequent maternal and neonatal mortality and morbidity.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abalos E, Cuesta C, Carroli G, Qureshi Z,Widmer M, Vogel JP, Souza JP (2014). On behalf of the WHO Multicountry Survey on Maternal and Newborn Health Research Network. Pre-eclampsia, eclampsia and adverse maternal and perinatal outcomes: a secondary analysis of the World Health Organization Multicountry Survey on Maternal and Newborn Health. International Journal of Obstetrics and Gynaecology 121(1):14-24. |
|
|
Aksornphusitaphong A, Phupong V (2013).Risk factors of early and late onset pre-eclampsia. Journal of Obstetrics and Gynaecology Research 39(3) 627-631 |
|
|
Ali AA, Rayis DA, Abdallah TM, Elbashir MI, Adam I (2011). Severe anaemia is associated with a higher risk for preeclampsia and poor perinatal outcomes in Kassala hospital, eastern Sudan. BMC Research Notes 4(1):311. |
|
|
Bartsch E, Medcalf KE, Park AL, Ray JG (2016). On behalf of the High Risk of Pre-eclampsia Identification Group Clinical risk factors for pre-eclampsia determined in early pregnancy: systematic review and meta-analysis of large cohort studies. British Medical Journal 353:1753 |
|
|
Bdolah Y, Lam C, Rajakumar A, Shivalingappa V (2008). Twin pregnancy and the risk of preeclampsia: bigger placenta or relative ischemia? American Journal of Obstetrics and Gynecology 198(4)428-431. |
|
|
Bilano VL, Ota E, Ganchimeg T, Mori R, Souza JP (2014). Risk Factors of Pre Eclampsia/Eclampsia and Its Adverse Outcomes in Low- and Middle-Income Countries:A WHO Secondary Analysis. PLoS ONE 9(3):198. |
|
|
Fang R, Dawson A, Lohsoonthorn V and Williams MA (2009).Risk Factors of Early and Late Onset Preeclampsia among Thai Women. Asian Biomedicine Research, Reviews and News 3(5):477-486. |
|
|
Firoz T, Sanghvi H, Merialdi M, von Dadelszen P (2011).Pre-eclampsia in low and middle income countries. Best Practice and Research Clinical Obstetrics and Gynaecology 25(4):537-48. |
|
|
Ganesh KS, Unnikrishnan B, Nagaraj K, JayaramS (2010).Determinants of pre-eclampsia: a case control study in a district hospital in South India. Indian Journal Community Medicine 35(4):502-505 |
|
|
Guerrier G, Oluyide B, Keramarou M, Grais RF (2013). Factors associated with severe pre-eclampsia and eclampsia in Jahun, Nigeria. International Journal of Women's Health 5:509-513. |
|
|
Illah E, Mbaruku G, Honorati M, Kathleen K (2013).Causes and Risk Factors for Maternal Mortality in Rural Tanzania - Case of Rufiji Health and Demographic Surveillance Site (HDSS). African Journal of Reproductive Health September 17(3):119-130 |
|
|
Kayode O, Osungbade, Olusimbo K, Ige OK (2011). Public Health Perspectives of Preeclampsia in Developing Countries: Implication for Health System Strengthening, Journal of Pregnancy 6 p. |
|
|
Khan KS, Wojdyla D, Say L, Gulmezoglu AM, Van Look PF (2006). WHO analysis of causes of maternal death: a systematic review. Lancet 367:1066-1074. |
|
|
Kiondo P, Wamuyu-Maina G, Bimenya GS, Tumwesigye NM, WandabwaJ and Okong P (2012). Risk factors for pre-eclampsia in Mulago Hospital, Kampala, Uganda. Tropical Medicine and International Health 17(4):480-487 |
|
|
Kooffreh ME, Ekott M, Ekpoudom DO (2014). The prevalence of pre-eclampsia among pregnant women in the University of Calabar Teaching Hospital, Calabar. Saudi Journal of Health Science 3:133-136 |
|
|
Landi B, Bezzeccheri V, Guerra B , Piemontese M (2014). HIVInfection in Pregnancy and the Risk of Gestational Hypertension and Preeclampsia. World Journal of Cardiovascular Diseases 4:257-267. |
|
|
Lozano R, Wang H, Foreman KJ (2011). Progress towards Millennium Development Goals 4 and 5 on maternal and child mortality: an updated systematic analysis. Lancet 378 (9797):1139-1165. |
|
|
Macheku GS, Philemon RN, Oneko O, Mlay PS, Masenga G, Obure J, Mahande MJ (2015). Frequency, risk factors and feto-maternal outcomes of abruptio placentae in Northern Tanzania: a registry-based retrospective cohort study. BioMed Central Pregnancy and Childbirth 15:242 |
|
|
Mahande MJ, Daltveit AK, Mmbaga BT, Masenga G, Obure J, et al. (2013). Recurrence of Preeclampsia in Northern Tanzania: A Registry-Based Cohort Study. PLoS ONE 8(11):79116. |
|
|
Makinde ON (2012). The Contribution of Severe Pre-Eclampsia and Eclampsia to Perinatal Mortality in a Nigerian Teaching Hospital, Perinatal Mortality Dr. Oliver Ezechi (Ed.),ISBN: 978-953-51-0659-3. |
|
|
Mooij R, Lugumila J, Mwashambwa MY, Mwampagatwa IH, Van Dillen J, Stekelenburg J (2015). Characteristics and outcomes of patients with eclampsia and severe pre-eclampsia in a rural hospital in Western Tanzania: retrospective medical record study. BMC Pregnancy and Childbirth 15(1):213 |
|
|
Muganyizi P, Shagdara M (2011). Predictors of extra care among magnesium sulphate treated eclamptic patients at Muhimbili National Hospital, Tanzania. BioMed Central Pregnancy and Childbirth 11:41. |
|
|
Urassa DP, Carlstedt A, Nyström L, Massawe SN, Lindmark G (2006). Eclampsia in Dar es Salaam, Tanzania -- incidence, outcome, and the role of antenatal care. Acta Obstetricia et Gynecologica Scandinavica 85(5):571-578. |
|
|
World Health Organization (2011). WHO recommendations for prevention and treatment of pre-eclampsia and eclampsia. Geneva: World Health Organization. |
|
|
Wong LF, Stuart B, Gleeson N (2007). Triploidy partial mole and proteinuric hypertension. Journal of Obstetrics and Gynaecology 27(4):424-5 |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


