ABSTRACT
The prevalence of hepatitis B and C (HBV and HCV) among HIV infected persons is a major public health problem in Nigeria. The increasing number of people living with HIV in Nigeria has presented the health care system with new co-morbid infections such as HBV and HCV. This study was designed to investigate the prevalence of hepatitis B and C among HIV/AIDS patients attending Bingham University Teaching Hospital Jos Plateau State Nigeria. The study was a retrospective study that reviewed all clinical case records of HIV/AIDS patients seen from 1st January, 2012 to 31st December, 2016. Information such as age, sex, marital status, occupation, educational level, hepatitis B and C status, CD4 T lymphocyte count, signs and symptoms were retrieved using structured questionnaire. Data were analysed and presented in simple percentage while Chi-square test was used to test for associations between variables at P<0.05. According to the results, more than two-third of the patients (1051, 68.10%) were females and 576 (37.30%) were in the age group of 38-47 years with a mean age of 42.60±9.9 years. The prevalence of HBV was 56.70% while HCV was 30.30%. In addition, both HBV and HCV were significantly found among HIV infected females compared to HIV infected males. The mean CD4 cells/µl for HBV positive was 500.48±101.81 while HCV positive was 557.33±121.76. The study showed the prevalence of hepatitis B and C among the HIV infected patients. Therefore routine screening for hepatitis B and C markers among HIV patients should be carried out regularly.
Key words: Prevalence, HIV/AIDS patients, hepatitis B, hepatitis C, CD4 count, Bingham University.
Globally, an estimate of 36.7 million people was living with Human Immuno-Deficiency Virus (HIV) in 2016. Sub-Saharan Africa remains most severely affected with nearly 1 in every 25 adults (4.2%) living with HIV, accounting for nearly two-thirds of the people living with HIV worldwide (World Health Organisation, 2017). Furthermore, there were about 3.2 million people living with HIV as at 2016, with an estimated 160 000 Acquired Immune Deficiency Syndrome (AIDS) related death recorded (UNAIDS, 2017). These AIDS related death can be attributed to the increase in mortalities and morbidities from liver diseases amongst HIV patients which is partly due to co-infection with hepatitis B and C viruses (HBV and HCV) as these viruses promote liver fibrosis by increasing intra-hepatic apoptosis (Greub, 2000; Macias et al., 2005; Iser et al., 2011; Chiekulie Kevin Diwe et al., 2013). Hepatitis which refers to an inflammation of the liver is becoming a major public health concern in sub-Saharan Africa including Nigeria. For instance, Sub-Saharan Africa has been shown to be endemic for hepatitis B with an estimated >8% prevalence in the population or in some 65 million people (Sonderup and Spearman, 2017). Furthermore, hepatitis C infection is prevalence in about 36 million people and the rates of co-infection with hepatitis B is up to 36% with the highest rate recorded in West and Southern sub-Saharan Africa (Matthews et al., 2014). Similarly, record from Nigeria reveals that over 35 million people have been estimated to live with hepatitis B and C viruses (Modi and Feld, 2007; Tremeau-Bravard et al., 2012; Madhava et al., 2002) while a pooled prevalence of HBV in Nigeria from studies carried out between 2000 and 2013 was 13.6% (Musa et al., 2015). Thus, the study estimated the prevalence of HBV and HCV among HIV/AIDS patients as it remains the foundation for understanding the interrelationship between these viruses along with designing health promotion programs for the prevention and control of these epidemics. Therefore, the retrospective study investigated the prevalence of hepatitis B and C infection among HIV/AIDS patients seen from 1st January 2012 to 31st December 2016 at the Bingham University Teaching Hospital Jos, Plateau State, Nigeria.
Study design
This study was a retrospective study that reviewed all clinical case records of HIV/AIDS patients seen from 1st January, 2012 - 31st December, 2016.
Study area
The study was conducted in Bingham University Teaching Hospital in the Jos North Area of Plateau State in North Central Nigeria.
Study population
The study population consists of all HIV/AIDS patients seen at Bingham University Teaching Hospital from 1st January, 2012 to 31st December, 2016. Bingham University Teaching Hospital is the second largest Teaching Hospital in Jos metropolis and offers a range of health care services including diagnosis and treatment of HIV/AIDS patients. The population of HIV/AIDS cases for the stated period were 1,544.
Inclusion criteria
HIV/AIDS positive patients seen only within the period of 5 years (1st January, 2012 to 31st December, 2016) who attended Bingham University Teaching Hospital were included in the study.
Exclusion criteria
Excluded from the study, were HIV/AIDS patients not seen within the period under review.
Instrument and method of data collection
A checklist was designed to collect information on the demographic characteristics of patients, HBV and HCV status, CD4 count, signs and symptoms. The data was abstracted by the researcher and three research assistants from the record of diagnosed HIV/AIDS patients, who were coming to the hospital from 1st January, 2012 to 31st December, 2016. Clinical data were collected from HIV-positive patients coming for CD4 monitoring from 1st January, 2012 to 31st December, 2016. Overall, a total of 1544 entries were retrieved for the retrospective study on the prevalence of HBV and HCV infection among HIV/AIDS patients. Information in the records includes patients’ demographic information, HBV and HCV status, CD4 count, signs and symptoms the patients presented at the time of treatment. The data were sorted and extracted after obtaining approval from the ART clinic through the hospital management board. The CD4 count in micro litre (µl) was classified according to the CDC Classification System for HIV-Infected Adults and Adolescents. Thus T-cells ≥500 µl was classified as category 1, T-cells 200-499 µl classified as category 2 and T-cells <200 µl classified as category 3 (CDC, 1993).
Data analysis
The collected data were entered into the computer and analysed using Statistical Package for Social Sciences version 20 (IBM Corp., Chicago, USA). Simple percentage were used to describe the basic features of the retrieved data while inferences between variables of interest were drawn using Chi-Square test at P<0.05. The data were collected to ensure confidentiality of patients’ information as no identifiers were used and the results were used for research purpose only.
Ethical consideration
Ethical clearance was obtained from the Department of Public and Community Health, Novena University Ogume and from Bingham hospital management board to the ART clinic.
Socio-demographic characteristics of the respondents
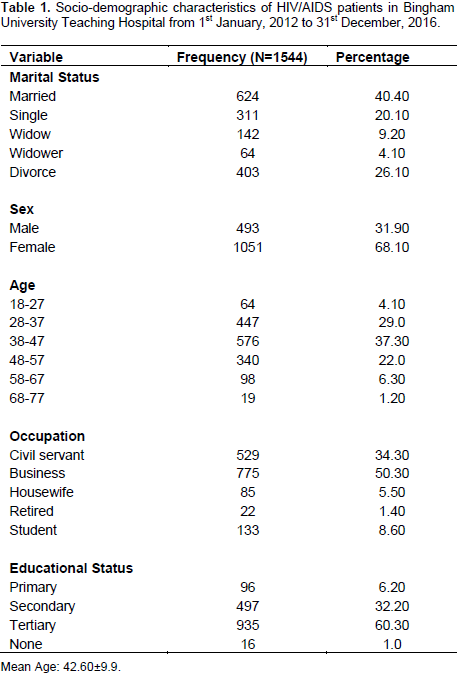
According to Table 1, 624 (40.40%) of the respondents were married and more than two third (1051, 68.10%) were females. Most (576, 37.30%) were between the age group of 38-47 years. Furthermore, almost half of the respondents (775,50.30%) were into business and 935(60.30%) attained secondary education.
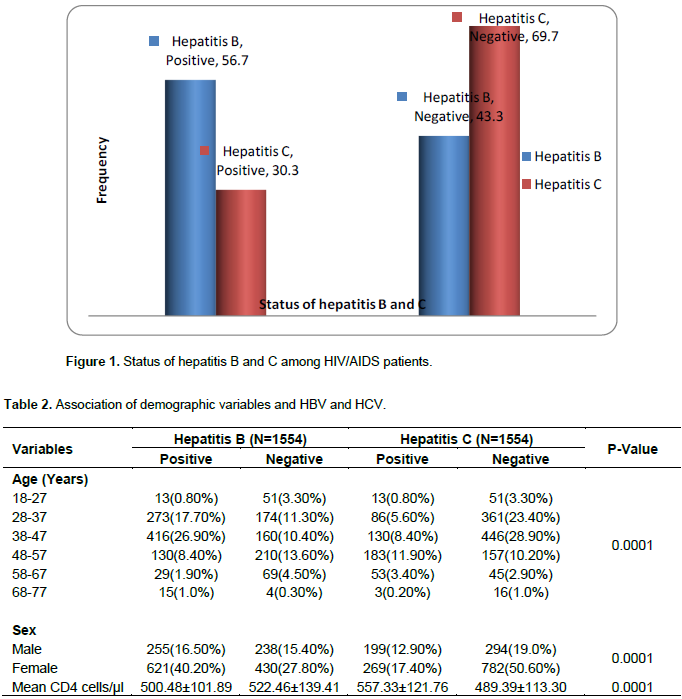
Status of hepatitis B and C
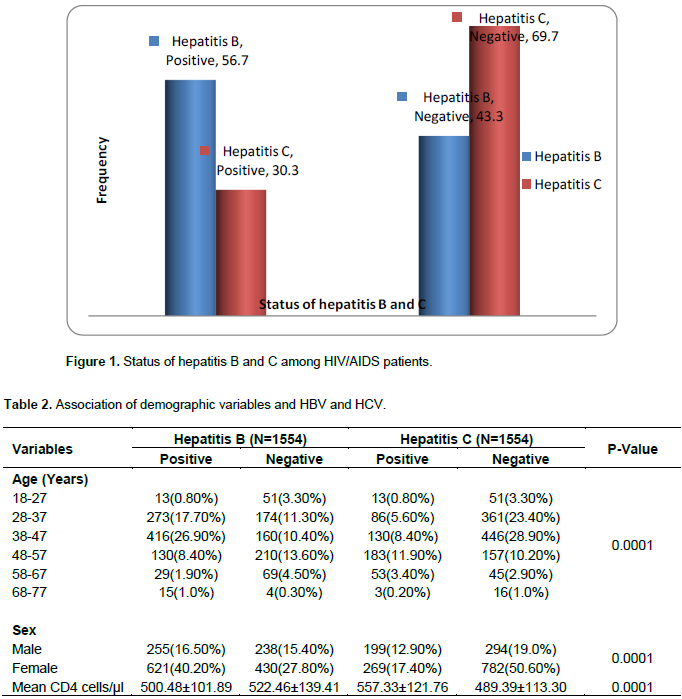
According to Figure 1, 876 (56.70%) of the respondents were positive to hepatitis B virus and 668 (43.30%) were negative to hepatitis B virus. Furthermore, more of the respondents (1076, 69.70%) tested negative to hepatitis C infection while (468, 30.30%) were hepatitis C positive. From Table 2, HBV were more common in patients aged 38-47 (26.90) and 28-37 (17.70%) years compared to patients in other age groups. Also, patients aged 48-57 years (183, 11.90%) were more positive to HCV than other age groups. Similarly, more females (621, 40.20%) than males (255, 16.50%) were HBV positive.
CD4 count of the patients
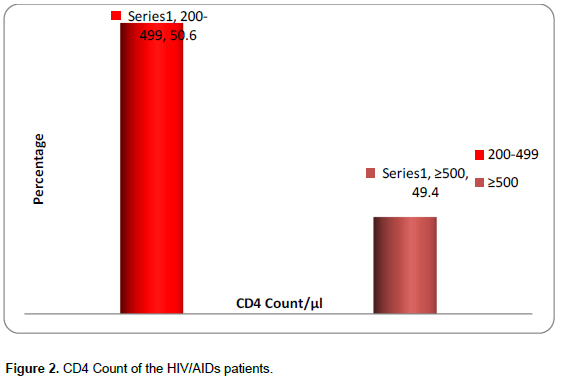
As shown in Figure 2, 781 (50.60%) of the patients were in category 2 as they had T-cells of 200-499 µl while 763 (49.40%) were in category 1 as they had T-cells of ≥500 µl and none of the patients recorded T-cells fell into category 3.
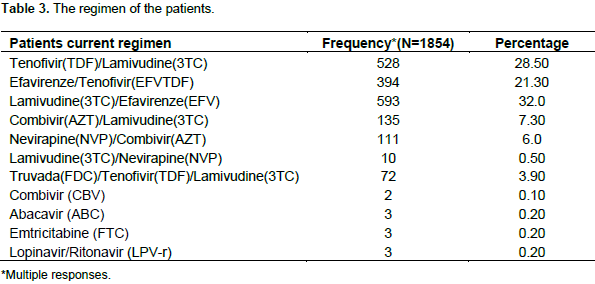
Patient current regimen
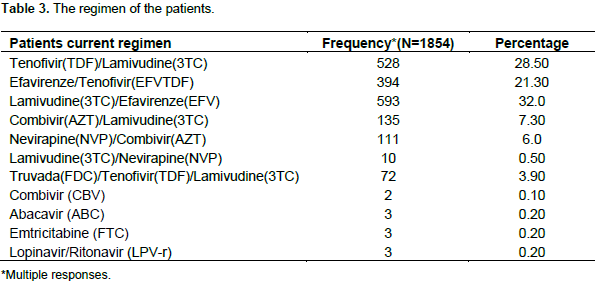
The regimen of the patients shows that more of them have a combination of lamivudine and Efavirenze (593, 32.0%) followed by a combination of Tenofivir and Lamivudine (528, 28.50%) while 394 (21.30%) had a combination of Efavirenze and Tenofivir (Table 3).
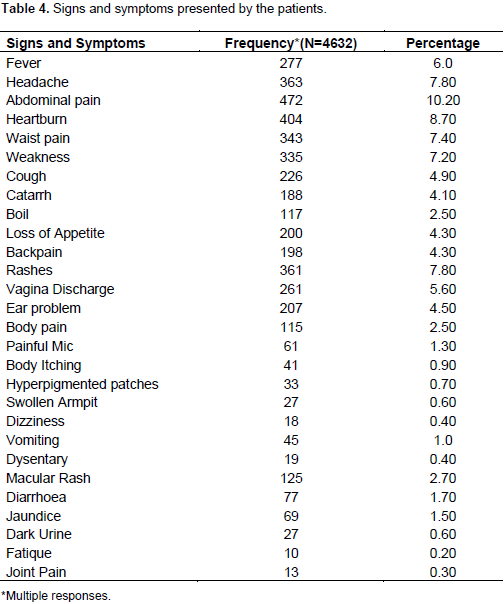
Signs and Symptoms of the patients
As shown in Table 4, more of the patients presented abdominal pain (472, 10.20%) at the hospital, followed by heartburn (40, 8.70%), headache (363, 7.80), rashes (361, 7.80), waist pain (343, 7.40) and weakness (335, 7.20%).
Viral hepatitis (HBV and HCV) has become a major public health concern worldwide especially among HIV patients (WHO, 2008; WHO, 2011). Furthermore, the relationship in the mode of transmission between the three viruses; HIV, HBV and HCV has made it more pertinent to assess the prevalence of HBV and HCV among HIV patients. The study reported the prevalence of both HBV and HCV among HIV/AIDS subjects. Furthermore, most of the respondents CD4 T lymphocyte were in Category 2 and 1 as their CD4 count was >200 µl above. The socio-demographic characteristics of the patients show that more of the patients were females representing more than two-third of the total cases of HIV patients reviewed in this study. This finding is similar to other studies which reported more females than males in their studies (Lacombe 2010; Muriuki et al., 2013; Tremeau-Bravard et al., 2012; Opaleye et al., 2014; Obadiah, 2011). The finding confirms previous assertions that women are more sexually vulnerable to HIV and other sexually transmitted infections than male (WHO, 2000). Furthermore, the majority of HIV infected patients were between the ages 28-57 years old with a mean age of 42.60±9.9 years. This signifies a higher HIV prevalence among adults and the age distribution is similar to previous studies (Balogun et al., 2012; Opaleye et al., 2014; Tremeau-Bravard et al., 2012). The prevalence of hepatitis B virus from the study shows that more of the patients tested positive to HBV. This prevalence of HIV/Hepatitis B co-infection (56.70%) was higher than previous studies from Ikole-Ekiti South-West Nigeria (Opaleye et al., 2014), Niger-Delta South-South Nigeria (Ejele and Ojule , 2004), Lagos South-West Nigeria (Balogun et al., 2012), Ibadan South-West Nigeria (Otegbayo et al., 2008), Jos North-Central Nigeria (Adekeye et al., 2013), Ilorin North-Central Nigeria (Olatunji and Iseniyi, 2008) and Maiduguri North-Eastern Nigeria (Baba et al., 1998).
Furthermore, other studies with lower prevalence outside Nigeria include a study in South-Africa (Parboosing et al., 2008), Senegal (Diop-Ndiaye et al., 2008), France (Larsen et al., 2008) and Thailand (Sungkanuparph et al., 2004). This observed difference of prevalence of HBV of the current study as compared with other studies might probably be due to varying sample size and the study design of the current study which reviewed a 5 years clinical records. In addition, the sex stratification prevalence of HBV shows that more females were HBV positive than males. This finding is similar to a previous study (Opaleye et al., 2014) but was however different from other studies (Mehmet et al., 2005; Muriuki et al., 2013). Furthermore, the statistically observed difference of HIV infection in both male and female in the current study reveals unequal exposure to HBV infection which is in line with previous studies (Opaleye et al., 2014; Agbede et al., 2007). In the same vein, the prevalence of 30.30% for HCV reported in the current study was higher than that reported in previous studies (Tremeau-Bravard et al., 2012; Muriuki et al., 2013; Forbi et al., 2007). Similarly, more females were positive to HCV than their male counterpart which is in line with result from previous studies (Muriuki et al., 2013; Lesi et al., 200); but at variance with other studies (Forbi et al., 2007; Agwale et al., 2004). Furthermore, there was a significant relationship between the sex of the patients and their HCV status.
This was slightly different from a previous study (Muriuki et al., 2013). Based on the Centre for Disease Control classification system for HIV infection which was used to categorise the severity of the HIV infection of the patients shows that almost all of the patients were in category 1 (T-cells of ≥500 µl) and 2 (T-cells of 200-499 µl). This result shows that the patients were still in the asymptomatic, acute HIV or persistent generalized lymphadenopathy stage of the infection. Although, the patients displayed some signs and symptoms consistent with category B symptomatic conditions and category C which is the AIDS-indicator conditions; it can be probably deduce that the various combination of antiretroviral drug regimen the patients were currently taking might have help to improve their CD4 count and also help in suppressing the manifestation of the full blown AIDS. This finding is slightly different from the study in Ikole-Ekiti South-Western Nigeria where almost one third of the patients from that study were in category 3 (Opaleye et al., 2014). Furthermore, the mean CD4 count was higher in HBV negative patients as compared with HCV patients which were higher in positive patients. The finding was also slightly different from the study in Ikole-Ekiti (Opaleye et al., 2014). The main limitation of the study is that the study was solely depended on the clinical records of the ART clinic at the Bingham University Teaching Hospital in identifying HIV, HBV and HCV patients without carrying out any confirmatory clinical laboratory test.
In conclusion, the study shows the prevalence of hepatitis B and C among the HIV infected patients. Therefore, we recommend that HIV patients should be routinely screened for hepatitis B and C markers. Also, intervention should be directed at implementing hepatitis B and C prevention strategies as part of HIV routine education among HIV patients. This will help reduce the severity of morbidity such as exposure to cirrhosis and mortality rate associated with hepatitis B and C infection including antiretroviral drug associated hepatoxicity among these patients.
The authors have not declared any conflict of interests.
REFERENCES
|
Adekeye AM, Chukwuedo AA, Zhakom PN, Yakubu RS (2013). Prevalence of Hepatitis B and C among Blood Donors in Jos South LGA, Plateau State, Nigeria. Asian Journal of Medical Sciences, 5(5):101-104.
|
|
|
|
Agbede OO, Iseniyi JO, Kolawole MO, Ojuawo A (2007). Risk factors and seroprevalence of hepatitis B surface antigenaemia in mothers and their pre-school age children in Ilorin. Niger. Ther. 4(1):67-72.
|
|
|
|
Agwale SM, Tanimoto L, Womack C, Odama L, Leung K, Duey D (2004). Prevalence of HCVcoinfection in HIV-infected individuals in Nigeria and characterization of HCV genotype. Journal of Clinical Virology Supplement, 1:S3-6.
Crossref
|
|
|
|
Baba MM, Gushau W, Hassan AW (1998). Detection of hepatitis-B surface antigenaemia in patients with and without the manifestations of AIDS in Maiduguri, Nigeria. Postgraduate Medical Journal, 5(3):125-127.
|
|
|
|
Balogun TM, Emmanuel S, Ojerinde EF (2012). HIV, Hepatitis B and C viruses' co-infection among patients in a Nigerian tertiary hospital. Pan African Medical Journal, 12:100.
|
|
|
|
Centre for Disease Control (1993). 1992 revised classification system for HIV infection and expanded surveillance case definition for AIDS among adolescents and adults. MMWR 41(RR–17):961-962.
|
|
|
|
Diopâ€Ndiaye H, Touréâ€Kane C, Etard JF, Lo G, Diaw PA, Ngomâ€Gueye NF, Gueye PM, Baâ€Fall K, Ndiaye I, Sow PS, Delaporte E (2008). Hepatitis B, C seroprevalence and delta viruses in HIV-1 Senegalese patients at HAART initiation. Journal of Medical Virology, 80(8):1332-1336.
Crossref
|
|
|
|
Diwe CK, Okwara EC, Enwere OO, Azike JE, Nwaimo NC (2013). Sero-prevalence of hepatitis B virus and hepatitis C virus among HIV patients in a suburban University Teaching Hospital in South-East Nigeria. Pan African Medical Journal, 16:7.
Crossref
|
|
|
|
Ejele OA, Ojule AC (2004). The prevalence of hepatitis B surface antigen (HBsAg) among prospective blood donors and patients in Port Harcourt, Nigeria. Nigerian Journal of Medicine, 13(4):336-8.
|
|
|
|
Forbi JC, Gabadi S, Alabi R, Iperepolu HO, Pam CR, Entonu PE, Agwale SM (2007). The role of triple infection with hepatitis Bvirus, hepatitis C virus, and human immunodeficiency virus(HIV) type -1 on CD4+ lymphocyte levels in the highly HIV infected population of North Central Nigeria. Mem. Inst. Oswaldo Cruz. 102(4):535-537.
Crossref
|
|
|
|
Greub G (2000). Clinical progression, survival and immune recovery during antiretroviral therapy in patients with HIV-1 and hepatitis C co infection, Swiss HIV cohort study. Lancet 356:1800-1805.
Crossref
|
|
|
|
Iser DM, Avihingsanon A, Wisedopas N, Thompson AJ, Boyd A, Matthews GV, Locarnini SA, Slavin J, Desmond PV, Lewin SR (2011). Increased intrahepatic apoptosis but reduced immune activation in HIV-HBV co-infected patients with advanced immunosuppression. AIDS 25(2):197-205.
Crossref
|
|
|
|
Lacombe K, Boyd A, Gozlan J, Lavocat F, Girard PM, Zoulim F (2010). Drug resistance and immune escape HBV mutants in HIV-infected hosts. Antiviral Therapy, 15:493-497.
Crossref
|
|
|
|
Larsen C, Pialoux G, Salmon D, Antona D, Le Strat Y, Piroth L, Pol S, Rosenthal E, Neau D, Semaille C, Astagneau ED (2008). Prevalence of hepatitis C and hepatitis B infection in the HIV-infected population of France. Euro. Surveill. 13(22):18888.
|
|
|
|
Lesi OA, Kehinde MO, Oguh DN, Amira CO (2007). Hepatitis B and C virus infection in Nigerian patients with HIV/AIDS. Niger. Postgraduate Medical Journal,14(2):129-33.
|
|
|
|
Macias J, Japón MA, Sáez C, Palacios RB (2005). Increased hepatocyte fas expression and apoptosis in HIV and hepatitis C virus coinfection. Infectious Diseases, 192(9):1566-1576.
Crossref
|
|
|
|
Madhava V, Burgess C, Drucker E (2002). Epidemiology of chronic hepatitis C virus infection in subSaharan Africa. Lancet Infectious Diseases, 2(5):293-302.
Crossref
|
|
|
|
Matthews PC, Gerettic AM, Gouldera PJR, Klenermana P (2014). Epidemiology and impact of HIV coinfection with Hepatitis B and Hepatitis C viruses in Sub-Saharan Africa. Journal of Clinical Virology, 61:20-33.
Crossref
|
|
|
|
Mehmet D, Meliksah E, Serif Y, Gunay S, Tuncer O, Zeynep S (2005). Prevalence of hepatitis B infection in the southeastern region of Turkey: comparison of risk factors for HBV infection in rural and urban areas. Japanese Journal of Infectious Diseases, 58(1):15-9.
|
|
|
|
Modi AA, Feld JJ (2007). Viral hepatitis and HIV in Africa. AIDS Rev. 9(1):25-39.
|
|
|
|
Muriuki BM, Gicheru MM, Wachira D, Nyamache AK, Khamadi SA (2013). Prevalence of hepatitis B and C viral co-infections among HIV-1 infected individuals in Nairobi, Kenya. BMC Research Notes 6:363.
Crossref
|
|
|
|
Musa BM, Bussell S, Borodo MM, Samaila AA, Femi OL (2015). Prevalence of hepatitis B virus infection in Nigeria, 2000-2013: a systematic review and meta-analysis. Nigerian Journal of Clinical Practice, 18(2):163-172.
Crossref
|
|
|
|
Olatunji OP, Iseniyi JO (2008). Hepatitis B and C viruses' co-infection with human immunodeficiency virus infected patients at UITH, IIorin. Nigerian Medical Practitioner, 54(1):8-10.
Crossref
|
|
|
|
Opaleye OO, Oluremi AS, Ogbolu DO, Babalola BA, Shittu T, Adesiyan AA (2014). Prevalence of hepatitis- B virus infection among HIV patients in Ikole Ekiti, South–Western, Nigeria. Asian Pacific Journal of Health Sciences, 1(4):507-511.
|
|
|
|
Parboosing R, Paruk I, Lalloo UG (2008). Hepatitis C virus seropositivity in a South African cohort of HIVinfected, ARV naive patients is associated with renal insufficiency and increased mortality. Journal of Medical Virology, 80(9):1530-1536.
Crossref
|
|
|
|
Sonderup MW, Spearman W (2015). HIV/HBV and HIV/HCV Co-infection in Sub-Saharan Africa: Transmission, Disease Outcomes, and Treatment Options.
View
|
|
|
|
Sungkanuparph S, Vibhagool A, Manosuthi W, Kiertiburanakul S, Atamasirikul K, Aumkhyan A, Thakkinstian A (2004). Prevalence of hepatitis B virus and hepatitis C co infection with human immunodeficiency virus in Thai patients: a tertiary case based study. Journal of the Medical Association of Thailand, 87(11):1349-1354.
|
|
|
|
Tremeau-Bravard A, Ogbukagu IC, Ticao CJ, Abubakar JJ (2012). Seroprevalence of hepatitis B and C infection among the HIV-positive population in Abuja, Nigeria. African Health Sciences, 12(3):312-317
|
|
|
|
Joint United Nations Programme on HIV and AIDS (UNAIDS) (2017). An overview of HIV/AIDS in Nigeria.
|
|
|
|
World Health Organization (WHO) (2000). Women and HIV/AIDS: Key Facts and Issues Fact Sheet No. 242.
|
|
|
|
World Health Organisation (WHO) (2008). Hepatitis B [database on the Internet] World Health Organization.
View
|
|
|
|
World Health Organisation (WHO) (2011). Hepatitis C [database on the Internet] World Health Organization.
View
|
|
|
|
World Health Organisation (WHO) (2017). Global Health Observatory (GHO) data on HIV/AIDS. Geneva Switzerland.
|