Full Length Research Paper

ABSTRACT
On January 30, 2020, the World Health Organization designated the outbreak as a Public Health Emergency of International Scope (USPPI). The purpose of this study was to assess the knowledge, attitudes and practices of medical personnel on the prevention of Covid-2019. A cross-sectional study among front-line health workers in the health facilities in the city of Conakry was carried out. The knowledge and attitude score were performed and categorized in 2: Good if ≥ at the average score and bad if < 50%. Logistic regression models were conducted to identify factors associated with knowledge and attitude. Among 548 health workers surveyed, 70.6% had a good knowledge of Covid-19. Among the health personnel interviewed, 57.7% had a good attitude towards a suspected case of Covid-19. Independent factors associated with poor knowledge of Covid-19 prevention were sex, health facility, and staff grade. As for poor attitude, the associated factors were knowledge of Ebola cases reported in the facility and the rank of the health staff. The health personnel have good knowledge of the virus but the attitudes are not related to knowledge. This study could serve as a basis for reorienting interventions involving front-line staff.
Key words: COVID-19, health facilities, knowledge, attitudes, professional practice, Guinea.
INTRODUCTION
On the 9th of January 2020, following reports of a series of unexplained cases of Pneumonia, China announced that the city of Wuhan - capital of Hubei Province-was facing an outbreak linked to a new type of coronavirus, known as SARS- coV-2. The World Health Organization (WHO) qualified this epidemic on Thursday, January 30, 2020, as a Public Health Emergency of International Concern (PHEIC). The epicentre of the epidemic has moved from China to Europe, before reaching America and Africa. This situation demonstrate the rapid spread of the epidemic through the circulation of goods and people (Chen et al., 2020; “Coronavirus disease 2019,” n.d.). To date, almost all the countries have reported cases of SARS-CoV-2 infection. According to the World Health Organization's current assessment of the epidemic, over 20 millions people have been infected, with nearly 1 million deaths (“Novel Coronavirus (2019-nCoV) situation reports,” n.d.). As on the 14th August 2020, a total of 1 096 951COVID-19 cases and 25,096 deaths have been reported in 55 African countries. This is 5% of all cases reported globally. Data from Africa Center for Diseases Control (Africa CDC) show an increase of 13% in a week. In Guinea, cases are reported in all health districts with strong community transmission.
Despite the impact of the preparedness policies put in place on the continent over the past several years (reflected in particular in the capacity of national laboratories to carry out diagnosis), the Covid-19 epidemic highlights the weakness of coordination among countries in their response and the impact of budget cuts on health systems. Everywhere the epidemic reveals the weaknesses of health systems (limited capacity in intensive care units, lack of health personnel). Low-Middle income countries (underdeveloped countries) with known weak health systems will therefore find it difficult to respond effectively to the predicted epidemic. This is the case in the Republic of Guinea, where the already weak health system was severely impacted by the Ebola epidemic between 2013 and 2016 (Delamou et al., 2017; Elston et al., 2017; Leno et al., 2018).
The epidemic of COVID-19 disease is an "extraordinary" pandemic because of its global scale and the speed of its spread. Despite the collective trauma it is causing worldwide, it is important to recognize the contexts in which it is occurring. While in all countries medical personnel remain at the heart of the response mechanism, their level of knowledge and experience of the epidemic is context specific. If the legacy of the previous Ebola epidemic among certain Guinean health workers (in terms of knowledge and practices) was observe, significant gaps remain and are the subject of a demand for training on the part of the actors.
Training of health workers is an integral part of the pandemic response. Thus, to guide health authorities on the need for training and to direct the response towards targeted actions, a few weeks before the notification of the first case of COVID-19, a survey among health personnel to assess knowledge, attitudes and practices to prevent coronavirus was organized in February 2020. The current study aimed to describe the knowledge and attitudes as well as analysed the factors influencing the knowledge and attitudes of the health personnel on COVID-19 at Conakry.
METHODOLOGY
Study design and setting
This was a cross-sectional study conducted between 1st and 29th of February 2020 among frontline health personnel in the health structures of the city of Conakry. The study was conducted in five communal medical centres (Coleah, Ratoma, le Flamboyant, Matam and Bernard KOUCHNER), three national hospitals (Donka and Ignace Deen and Sino-Guinean) and three health centres (Maciré, Dixinn and Madina). These hospitals are all located in the city of Conakry, the capital of the Republic of Guinea, which has an estimated population of 1,930,838 (“Rapports d’enquêtes - RGPH 2014 - stat-guinee.org,” n.d.).
Study Population and data collection
The study focused on front-line health workers in health facilities were included in this study, all health care workers of all ranks, and someone chose the number of years of experience that were present on the day of the survey and who agreed to participate in the survey. All health workers present on the day of the survey who gave their verbal consent were eligible for the survey. This is a face-to-face verbal interview with the respondent. The selection of health services was sampled for convenience. This type of sampling was used to select those health services in which staffs are considered convenient data sources for this study. Convenience sampling is a type of non-probability sampling in which individuals are sampled simply because they are "convenient" data sources for researchers (“Convenience Sampling,” 2008). The number of health personnel expected in the health facilities in Conakry was 900. The respondent was asked about those present in the services and with a verbal agreement to participate in the study.
Data were collected by interviewers using a standardized questionnaire with 4 sections: socio-demographic characteristics, knowledge about the coronavirus, attitudes to prevention and control of infection, and practices. The Kobocollect application was used to collect the data. The questionnaires were pre-tested for validation purposes. In order to carry out this survey as quickly as possible because of the public health emergency it represented, the study adapted the questionnaire used to assess health workers' knowledge of Ebola to Covid-19 (Iliyasu et al., 2015)completed it using information provided by the Center for Disease Control and Prevention (CDC) and WHO on the epidemic (“Novel Coronavirus (2019-nCoV) situation reports,” n.d.; “Transmission of Novel Coronavirus (2019-nCoV) | CDC,” 2020).
Knowledge and attitudes were assessed using structured questions on the virus, symptoms, care, prevention, and response activities undertaken by the State. A total of seventy questions to assess knowledge and six attitudes question questions were asked. Each correct answer was scored as 1, while the incorrect answer was scored as 0. Good knowledge was defined as a score ≥ at the overall average and poor knowledge was defined as a score < at the overall average. The same method was used to identify good and bad attitudes towards COVID-19. A 5-level likert scale was constructed to assess the infection prevention and control attitudes of health workers.
Data analysis
The data collected were extracted and cleaned before being analysed int the STATA 14 software (STATA Corporation, College Station, TX, USA). The study used the whole sample to summarise data with proportions (%) and mean (with standard deviation). The Chi2 or fisher exact test was used for the comparison. Logistic regression models derived the unadjusted and adjusted odds ratios were constructed to identify independent factors associated with poor knowledge and COVID-19’s poor attitude to prevention. All study variables with a p-value < 0.20 in the bivariable analysis were considered for inclusion in the logistic regression model. The significance level for the logistic regression model was set at 5% with a 95% confidence interval. The goodness of fit of the final model was tested by the Hosmer and Lemeshow test.
Ethical considerations
The study was approved by the Ethics and Scientific Committee of the Public Health department of the Faculty of Health Sciences and Technology of Gamal Abdel Nasser University, Conakry.
RESULTS
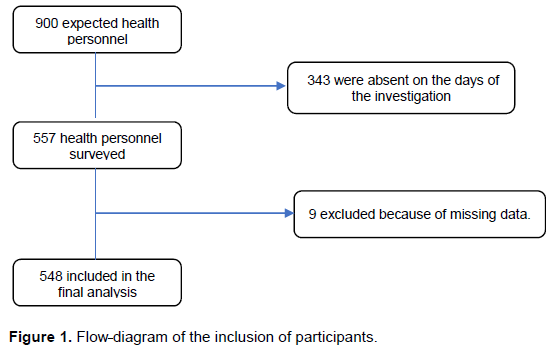
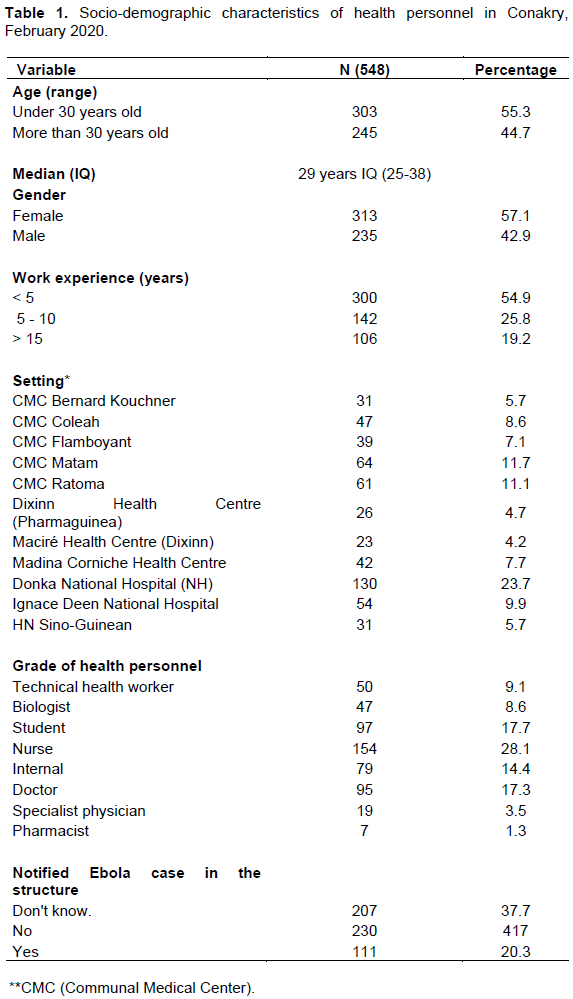
From 900 expected health workers, a total of 557 were included in this study of which 9 were excluded from the final analysis (Figure 1). More than half of the respondents were under the age of 30 with a median age of 29 years IQ (25-38). The majority of the agents interviewed were women (57.1%) and had less than 5 years’ experience in the field (54.9%) and were nurses in 28% of cases. The majority of the participants were surveyed at Donka National Hospital (NH) 130/548 or 23.7%. Nurses were the most represented in the study (28.1%) (Table 1).
Knowledge and attitudes of health care personnel about COVID-19
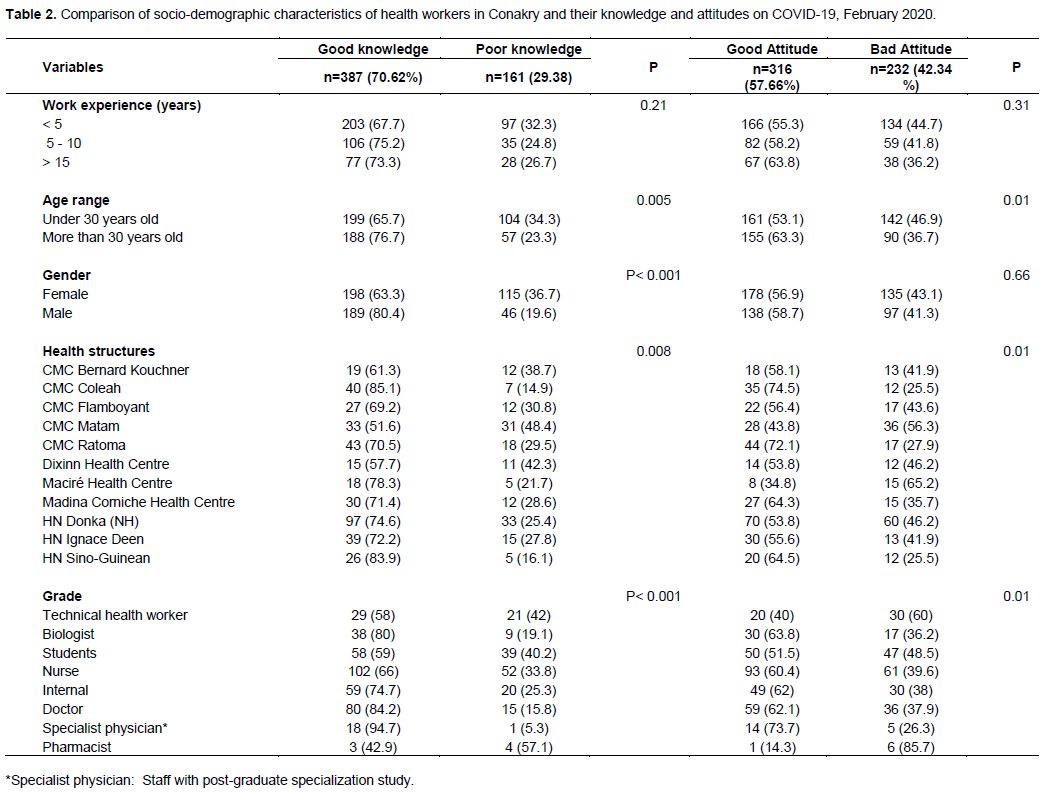
The mean knowledge score on COVID-19 was 54.81 ± 9.71 (Table 2). Majority of respondents (70.6%) had a score above 54.8% [95%CI: 66.6-74.4], that is good knowledge of COVID-19.
The mean attitude score was 62.3 ± 27.2, on this basis, 57.7% [CI95%: 53.4-61.5] of the study participants had a good attitude towards a suspected case of COVID-19 (Table 2). Almost all, 546/548 (99.6%) of the interviewees did not know the emergency number in case of a suspected case and about 50% did not know the incubation period of COVID-19. Indeed, a large majority (53.8%) of staff reported wanting to consult and prescribe medication for a patient with signs related to COVID-19. In this survey, doctors and biologists had a good knowledge of the virus with 84.2 and 80% respectively.
Prevention and control infection practices and information sources
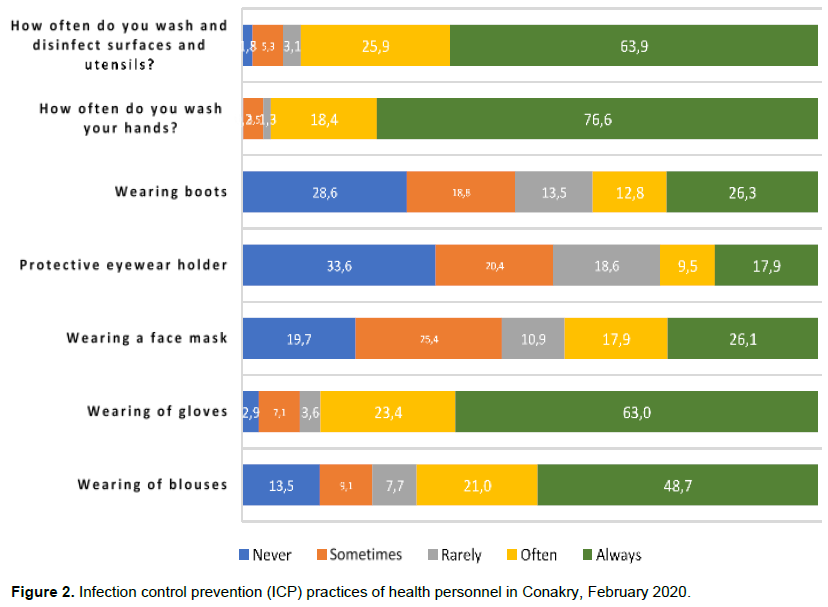
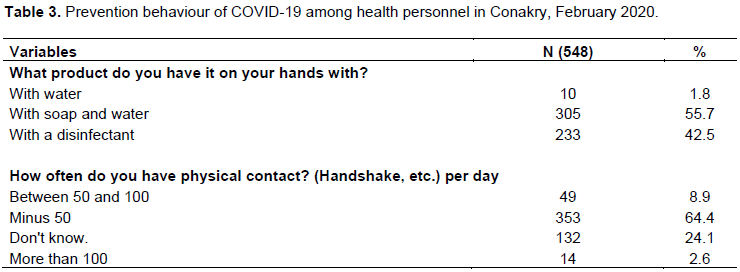
Participants' infection prevention and control practices were assessed using a Likert scale (Figure 2). Study participants reported that they always disinfected surfaces, utensils and work equipment (69.9%) and then washed their hands after a medical procedure (76.6%). They also reported that they always wore boots (26.3%), gloves (63%) and gowns (48.7%) during a medical procedure. Soap and hydro-alcoholic solutions were the most commonly used by staff, with proportions of 55.7 and 42.5% respectively (Table 3). It should be noted, however, that infection prevention and control (ICP) was not systematically applied by all staff. Thus, preventive gestures were not systematically applied (the rate of application did not even reach 80% for each gesture).
Sources of information on COVID-19 for health care personnel-19
The media was the main source of information about COVID-19 for health care workers (81%), both online and offline. The professional and family network was the main source of information for staff, with 65 and 35% respectively. Most health personnel (57.5%) had already received training in infection prevention and control and wanted more information on COVID-19 (98%).
Factors associated with poor knowledge of COVID among health care personnel-19
The logistic regression models showed that the independent factors associated with poor knowledge were gender, the structure where the respondent worked, the fact of having trained in ICP (Infectious pre in the past) and rank. Indeed, women, compared to men, are 2.46 95% CI [1.62 - 3.74] times more likely to have a poor knowledge of COVID-19, all other things being equal with p=0.001.
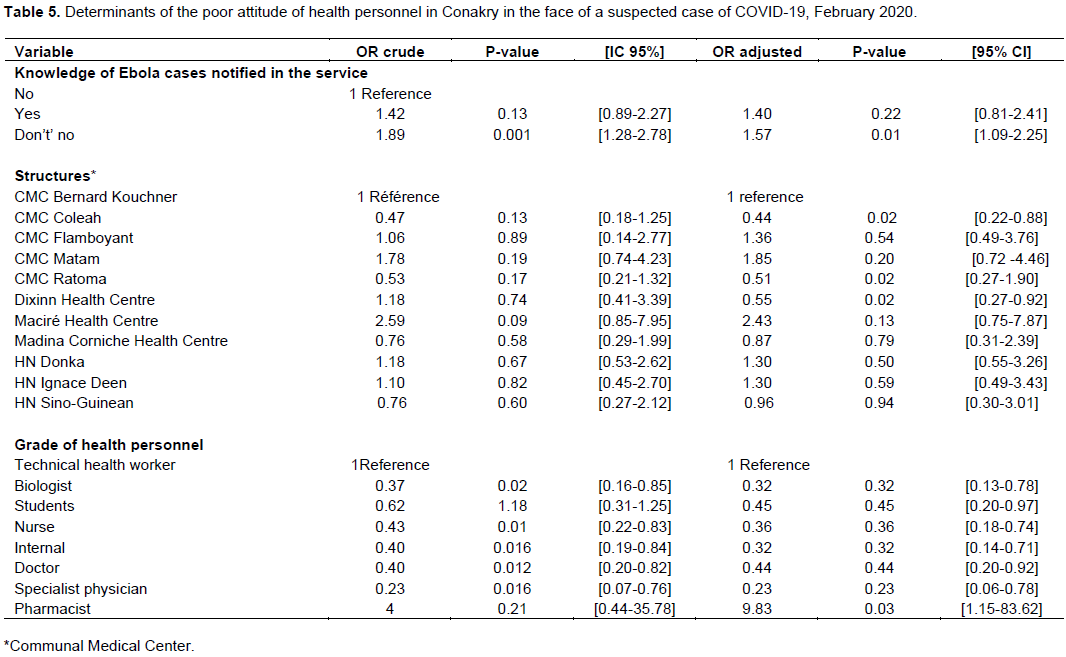
Healthcare workers who have had ICP training in the past compared to those who have not, are 40% less likely to have poor knowledge of COVID-19 (OR=0.61 CI [0.40-0.89], P=0.01. Pharmacists compared to health technical officers (HTAs) are more likely to have poor knowledge of COVID-19. (P=9.83 95% CI [1.09-38.44]) (Table 4). Data of the models also showed that the independent factors associated with poor attitudes were poor attitude, the associated variables where: Knowledge of Ebola cases reported in the department, health facility and grade of health worker (Table 5).

DISCUSSION
This study aimed to analyze the attitudes, knowledge and practices of health personnel in Conakry on COVID-19 and identify factors associated with poor knowledge and attitude of these practitioners.
The choice for convenience is a limit of the study, but the results of this study in this context have undoubtedly made it possible to adapt the strategies for minimizing the risks of COVID-19 contamination among health personnel. It could serve as a basis for the training of this socio-professional layer.
This study shows us that there are still some gains from the previous Ebola epidemic in terms of knowledge, attitudes and infection prevention and control practices. Indeed, it was observed that the majority of health workers have a good knowledge of Covid-19 (70% of the sample). However, the overwhelming majority of health workers, all statuses and structures combined (99.6%) were unaware of the existence of a toll-free number to alert on the presence of a suspected case of coronavirus and only 42.3% knew the incubation period of the virus. In a similar study of Ebola in Guinea, 95.2% of the health workers were knowledgeable and could identify an Ebola suspect (Sidibé et al., 2018). Although this is not the same context, nor the same pathogen, there is an effort on the part of health workers to learn about public health threats. This is reflected in the sources of information consulted: 81% of them obtained their information from the media (Internet, radio). The same sources were reported in the final report of a study to assess the knowledge and attitudes of health workers about Ebola disease in Sierra Leone (“Ebola-Virus-Disease-National-KAP-Study-Final-Report_-final.pdf,” n.d.). With a gradual increase in media penetration and coverage rates in Guinea, new information and communication technologies will play an important role in the detection and management of epidemics.
The attitude of the health staff when confronted with a case of a patient suspected of having COVID-19 is in contradiction with the response measures issued by the Ministry of Health, which require that suspicious cases be isolated and referred for management in a specialized environment. Even if the wearing of personal protective equipment is systematic for most agents, keeping a potentially infected patient would be a risk for other patients and the staff themselves. This proportion of staff using personal protective equipment is almost equal to the proportion reported in Nigeria for assessing the PPE of health workers in the Ebola context (Iliyasu et al., 2015). From the point of view of attitude in the face of a suspected case, the staff tends to opt to isolate patients even in health structures. There is a lack of place to isolate patients; these attitudes contained a significant desirability bias, since all the agents admitted that they were unaware of the existence of the toll-free number that would allow them to do so.
Systematic hand washing (76.6% of respondents) and glove wearing (63%) seemed to be relatively practiced but remain too weak to ensure effective protection for all agents and patients. The wearing of masks (26.1%) is largely insufficient, as is the wearing of gowns (48.7%). Concerning the literature on Haemorrhagic Fevers, the literature shows that the practice of handwashing varies according to whether health workers are practicing in a declared epidemic context or in an alert context. The practice was observed in the first case, around 80 to 85% in Sierra Leone and Nigeria (“Ebola-Virus-Disease-National-KAP-Study-Final-Report_-final.pdf,” n.d.; Iliyasu et al., 2015)but was very low in the second, as in Iran during the Crimean-Congo fever alert (Rahnavardi et al., 2008). This issue is crucial for the implementation of infection prevention and control measures among health workers in the context of the COVID epidemic [19] where the feeling of health actors seems to be that if the epidemic is present, it is confined to a limited fringe of the population (elites and foreigners).
In this period of pandemic, health personnel remain very exposed, especially at the start of outbreaks. Cascading training is often recommended to help them prevent the risk of contamination. It would also be advisable to identify, through the observation of practices, which types of actors are mainly exposed due to their contact with patients in order to prioritize their training (we can think of actors developing frequent physical contact with patients: care assistants, nurses, but also wardens or reception agents, etc.), but also how the application of ICP impacts on the quality of care produced (in particular by the absence of palpation-type contact).
The agents in the health centres and National Hospitals (NH), a large proportion of whom have less than 5 years of seniority (Health Centre: 47%, HN 38%) compared to the communical medical centre (CMC) 15% had on average a better knowledge of the coronavirus (Health Centre and National Hospital 41.9%, CMC 16.3). This could be explained by the fact that the issue of zoonoses and ICP is now part of the training curriculum for health workers (Faculty of Health Sciences and Techniques and Nursing School), in which they have participated. This therefore calls for priority to be given to upgrading the skills of health professionals with more than five years' seniority.
There is no strong correlation between level of knowledge of Covid-19 and expression of intention to advice isolation in case of symptoms, systematic mobilization of barrier gestures. This bids the authors to go beyond the cognitive question of knowledge of the risk to question both its perceptions, in particular the conviction of the actors to be concerned by the risk of the Coronavirus and the factors which do not come under the purely biomedical register which influences it (risk scales, rumours). This is not only the political context which gives rise to concern, putting the question of viral risk in the background), but also the conditions for appropriating the knowledge acquired in ordinary practice (conditions of practice, presence of protective equipment or disinfectant products, influx of patients, leadership role of the medical hierarchy in the establishment). Particular attention should be paid to the impact of discourse on the extraneity of viral risk on the management of national patients. Until now, prevention measures have focused on airports and the figure of the virus carrier has been embodied by the Asian or European traveller. This figure has not been contradicted by the first proven cases. However, as we enter a phase of local transmission of the virus, it is extremely important to alert health workers to the presence of the virus on national territory and to the fact that it is not limited to a section of the population of non-African origin.
The female sex, being a pharmacist, having benefited from training in ICP in the past and working in the communal medical centre of Matam were 2.46 at risk of having poor knowledge of COVID-19 compared to men. This result could be explained by the gendered distribution of roles in the Guinean health system. The majority of men occupy positions of responsibility, which allows them to have easier access to information at the central level. On the other hand, they occupy a greater number of administrative positions that allow them to search for information, whereas women, who are mostly confined to care functions, have fewer opportunities. In the context of the Ebola fever epidemic on the African continent, the lack of time that women could devote to information seeking and their high exposure to risk due to their care functions has been put forward to explain their high lethality (“OMS | Maladie à virus Ebola – République démocratique du Congo,” n.d.). With regard to the pharmacy profession (OR=9.83 CI [1.09-38.44], p=0.03), it is possible that pharmacists working in health facilities or pharmacies may suffer from a lack of access to training and workshops on infection prevention and control compared to health care workers. Staffs who have received ICP training in the past, the medical profession and biologists are likely to be knowledgeable about COVID.19
This may be directly associated with the effects of the Ebola epidemic from 2013 to 2016, during which much ICP training was organized for health workers. Although this research covered all public structures in the capital, this study has certain limitations: first of all, private structures were not included, nor were informal spaces for the production of care or the dispensing of medication products. In addition, assessing the level of knowledge about a new virus such as Covid-19, for which knowledge is evolving daily, may seem a challenge. Inspite of these limitations, this study is of definite interest at a time when Guinea, along with the African continent, is organizing its response to the emergence of a new epidemic. This study has the advantage of giving us an overview of the knowledge and attitudes of health staff regarding COVID-19 in the pandemic preparedness situation.
CONCLUSION
About 70.62% of the health personnel surveyed had a good knowledge of the coronavirus disease. This good knowledge of the virus contrasted with their attitudes as only 57.66% had a good preventive attitude as around 98% of the agents did not know the emergency number. In all, four variables were associated with low knowledge of COVID-19: female gender, lack of IPAC training in the past, and officer rank. As for the bad attitude, the associated factors were the notification of a case of Ebola in the department during the epidemic of 2013 and 2016, the profession of pharmacist and the level of structure in the health pyramid. It would be advisable to associate to this CAP survey an observation of long-term practices allowing in situ observation of actors' practices in order to avoid desirability bias
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors appreciate all the authorities and health personnel for their availability for this study.
FUNDING
The authors financed the costs of the field investigation, the publication costs are borne by École Normale Supérieure de Lyon, France, which also has a teacher who participated in the work.
REFERENCES
|
Chen N, Zhou M, Dong X, Qu J, Gong F, Han Y, Qiu Y, Wang J, Liu Y, Wei Y, Xia J, Yu T, Zhang X, Zhang L (2020). Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: a descriptive study. The Lancet 0. |
|
|
Convenience Sampling (2008) in: Encyclopedia of Survey Research Methods. Sage Publications, Inc., 2455 Teller Road, Thousand Oaks California 91320 United States of America. |
|
|
Coronavirus disease 2019 [WWW Document], n.d. URL |
|
|
Delamou A, Ayadi AME, Sidibe S, Delvaux T, Camara BS, Sandouno SD, Beavogui AH, Rutherford GW, Okumura J, Zhang WH, De Brouwere V (2017). Effect of Ebola virus disease on maternal and child health services in Guinea: a retrospective observational cohort study. Lancet Global Health 448-457. |
|
|
Ebola-Virus-Disease-National-KAP-Study-Final-Report_-final.pdf, n.d. |
|
|
Elston JWT, Cartwright C, Ndumbi P, Wright J (2017). The health impact of the 2014-15 Ebola outbreak. Public Health 143:60-70. |
|
|
Iliyasu G, Ogoina D, Out AA, Dayyab FM, Ebenso B, Otokpa D, Rotifa S, Olomo WT, Habib AG (2015). A Multi-Site Knowledge Attitude and Practice Survey of Ebola Virus Disease in Nigeria. PLoS ONE 10. |
|
|
Leno NN, Delamou A, Koita Y, Diallo TS, Kaba A, Delvaux T, Van Damme W, Laga M (2018). Ebola virus disease outbreak in Guinea: what effects on prevention of mother-to-child transmission of HIV services? Reproductive Health 15:60. |
|
|
Novel Coronavirus (2019-nCoV) situation reports [WWW Document], n.d. URL |
|
|
OMS | Maladie à virus Ebola - République démocratique du Congo [WWW Document], n.d. . WHO. URL |
|
|
Rahnavardi M, Rajaeinejad M, Pourmalek F, Mardani M, Holakouie-Naieni K, Dowlatshahi S (2008). Knowledge and attitude toward Crimean-Congo haemorrhagic fever in occupationally at-risk Iranian healthcare workers. Journal of Hospital Infection 69:77-85. |
|
|
Rapports d'enquêtes - RGPH 2014 - stat-guinee.org [WWW Document], n.d. URL |
|
|
Sidibé S, Camara BS, Delamou A, Touré A, Bouedouno P, Samake AT, Beavogui AH (2018). [Knowledge, attitudes and practices of healthcare providers on suspected Ebola cases in Guinea]. Rev. Epidemiol. Sante Publique 66:369-374. |
|
|
Transmission of Novel Coronavirus (2019-nCoV) | CDC [WWW Document], 2020. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


