ABSTRACT
Many health hazards plus other contagious diseases and skin infections are related to barbers’ occupation, to which their clients are exposed to. Barbers’ awareness and practice plays a vital part in the hindrance and management of these health related risks. The objective of this study is to assess the knowledge and practice of barbers regarding biological hazards related to their occupation in Hawassa Town, Southern Ethiopia. This is a cross-sectional study conducted from September 1st, 2014 to January 31st, 2015. The overall number of barbers within the town was 1360, of which 516 barbers participated in this study. The sample size determination was done using the formula for a single population proportion by considering 51% knowledgeable barbers from – Jimma Ethiopia, 95% level of confidence with 5% margin of error. About 15% of the none-response rate was added in this study. The systematic random sampling technique was implemented during data collection. By using structured and pre-tested questionnaires, face to face interview was applied to determine knowledge level of the participants. Different statistic methods like multivariate logistic regression were conducted to spot factors associated with knowledge and practice of barbers. Of the 516 barbers, 515 (99.9%) had smart knowledge on biological hazards associated with their profession, whereas 369 (71.5%) practice safe during barbering. An academic status, holder of the business, operating hour and toil expertise of the barbers were associated considerably with the knowledge of the barbers. However, the practices of the barbers were related solely through handiness of ultraviolet (UV) sterilizers in the room and toiling hour. Long practices of barbers with smart knowledge have good association with forestall biological hazards on their profession. However, giving more coaching to the barbers is necessary to prevent biological risks related to their occupation.
Key words: Barbers, hazards, occupation, knowledge, practice, Hawassa.
The term barber is derived from the Latin word barba meaning beard. A person whose occupation is hair cutting, shaving and trimming of beards is called barber (Http://www.wikipedia.org.com, 2013). The common risk factors in barbers’ occupation are razors, scissors, nail files and baby piercing instruments. In the rural area, the barbers are involved in circumcision, incision and drainage of abscesses (Waheed et al., 2011).
The main service of the barber shop is shaving, haircutting and hair reforming for men using different sharp materials. There is need to give attention to the use of sharp instruments at different sites including barber house to minimize the risks of blood borne infections like viruses. It is a serious health problem for both barbers and their clients (Wazir et al., 2008; Khandait et al., 1999).
The barbers’ work related infection remains the major cause of morbidity and mortality in human beings particularly in developing and underdeveloped countries due to poverty and overcrowding. Even though many infectious diseases are preventable and treatable in developing countries, personal and environmental hygiene, ignorance and poor political commitments persist (Wazir et al., 2008, Khandait et al., 1999).
An ancient profession called barbering is intensively associated with the use of blades, towels, knives and combs, etc. If these are not appropriately disinfected, it leads to transmission of a range of infections, which include fungal infections, infestations of head louse, scabies, staphylococcus infection, human immuno-deficiency virus (HIV), hepatitis B and C viruses, etc (Amodio et al., 2010). A large number of residents receive services from barbers in our society. Barbers’ profession and work place may be a possible group for the spread of various infections related to their job to which their visitors are exposed (Beyen et al., 2012). Hence, awareness about these health hazards among barbers would play a vital role in the prevention and control of these infections. The purpose of our study is to assess awareness among barbers regarding health hazards related to their profession and to identify practices linked to acquisition of infections in barbers’ shops.
Study design
Cross sectional study was carried out in Hawassa town involving all barbers with the help of pretested questionnaire through interview method.
Study area
The study was conducted in selected 8 sub-cities of Hawassa town found in the technology village of Hawassa University in Sidama Zone, Southern Ethiopia. It was conducted from September 1st 2014 to January 31st, 2015.
Source population
The source and study population were all barbers in 8-sub cities of Hawassa town.
Study population
The study population was actively working barbers in the selected sub-city where the actual sample is drawn from.
Sampling strategy
Approximately 1360 barbers render services to the residents in the town. Five hundred and sixteen barbers were randomly selected to participate in this study. About 65 barbers were interviewed from each sub-city. The structured number and name of the barber’s house were obtained using systematic random sampling system. From each barbers’ house, the clients participated in this study using lottery system. The sample size was determined using the formula for single population proportion by considering 51% proportion of knowledgeable barbers (Zewudie and Kurkura, 2002)with 95% level of confidence. Five percent (5%) margin of error and 15% of none response rate were included.
Inclusion and exclusion criteria
An individual worker assisting the main workers was excluded. All permanent barbers were included.
Data collection
A standardized pre-tested questionnaire was provided to the workers, and was convinced to provide actual information during interview.
Data quality management
Ethical clearance was obtained from the institutional ethical committee. Voluntarily participated individuals were clearly informed about the purpose of the study. An informed consent was obtained from the willing participants. Only the consented individuals were involved. A structured and pretested questionnaire was used for the study which included the personal details of the participants such as age, education, income, duration of profession and knowledge of risk factors of their occupation.
Data were collected by interview method and by informal inspection of workplace, after informed consent was taken. Data collected were tabulated in Microsoft excel sheet, and statistical analysis was done using Open-Epi info software. Chi-square test was applied for proportions of p<0.05 considered for level of significance.
Ethical clearance was obtained from College of Medicine and Health Sciences, Hawassa University-Institutional Ethical Review board IRB, and consent form was signed by each individual before data collection.
Socio-demographic characteristics of barbers
The response rate of this study was 100%. A total of 516 study subjects were included in this study, among which 410 (79.5%) were males and the remaining were females. About 218 (42.2%) were singles, 290 (56.2%) were married and 8 (1.6%) were divorced. The mean (standard deviation) age was 26.8 (±3.12) years (ranging from 15 to 38 years). The average numbers of barbers per house were four. Everyday mean (standard deviation) revenue of the participants was 27.65 (±19.32) Ethiopian birr. The dominant religions of the study participants were orthodox 253 (49.0%) and protestants 251(48.6%). About 396 (76.7%) respondents have TV and radio in their working rooms (Table 1).good knowledge about diseases transmission mechanisms from person to person during their work. They knew the existence of biological hazards related to their profession and source of infection from different sources; for instant from health care center, 215 (41.7%), television (TV) 213 (41.3%), from training related to health and safety, 14 (2.7%), by reading newsletters related to health and safety 71 (13.8) and from radio 3 (0.6%) (Table 2). Four hundred and twelve, 412 (79.8%) and 383 (74.2%) participants had good knowledge about human immunodeficiency virus (HIV/AIDS) and dandruff (Table 3).


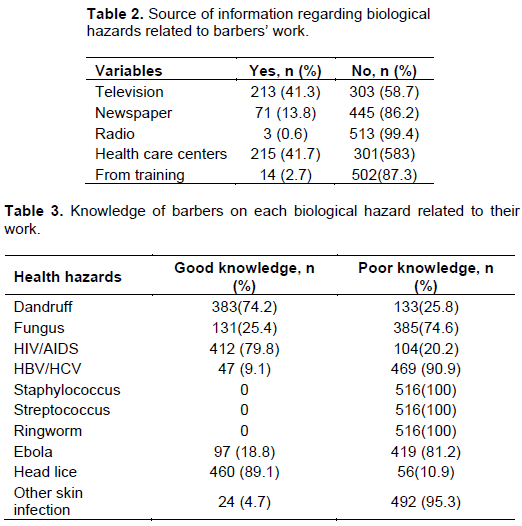
However, the remaining had relatively less knowledge about fungal infection, 131(25.4%), viruses like Ebola, 97 (18.8%), HBV and HCV, 4 (0.8%), head lice, 56 (10.9%) and other skin infections, 22 (4.3%); for the others, there was a poor knowledge about eczema, allergy, staphylococcus and streptococcus.
Barbers’ practice to prevent biological hazards
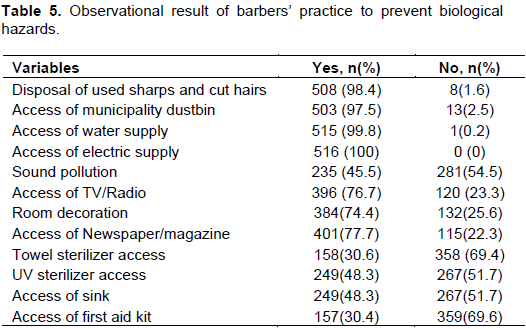
About 147(28.5%) respondents do not wash hands for new customers, while 79 (15.3%), 38 (7.4%), 71 (13.8%), 61 (11.8%), 60 (11.6%) and 3 (0.6%) neither change nor sterilize razors, shavers, scissors, brushes, combs and towels while barbering the hair of different customers, respectively. Of the total study participants, 79 (15.3%) neither wash nor change apron for new customers during barbering (Table 4). In general, only 98 (18.9%) participants practice safe while barbering.

More than 369 (71.5) work safely all the way while barbering the hair of different customers. In this study, about 496 (97.3%) prefer dry hot oven sterilization technique to autoclaving, 12 (2.4%) and 2 (0.4%) direct flaming. About 515 (99.8%) barbers commonly apply disinfection on their daily practice. However, only 147 (28.5%) use alcohol and 365 (70.9%) use bleach called “Barakina”. 418 (81.2%) get their disinfectants from any unknown shops, while about 318 (61.7%) of them do not know the concentration of their disinfectants at all. Even though 447 (86.8%) of the Hawassa town barbers are inspected, the lion share of the inspection is done by health professionals, 482 (93.6%) from the health center. About 258 (50%) of the barber houses are inspected every 6 months (Table 5). are self-owners [AOR=4.85, 95% CI: 1.89, 11.60]. Similarly, the shared barbers’ owners have more knowledge than self-owners [AOR=1.89, 95% CI: 1.46, 4.88]. The likely reason of this is the barbers’ knowledge disparity between these groups and educational levels of the groups. Different studies showed that the shared barbers need higher education level to provide better service.
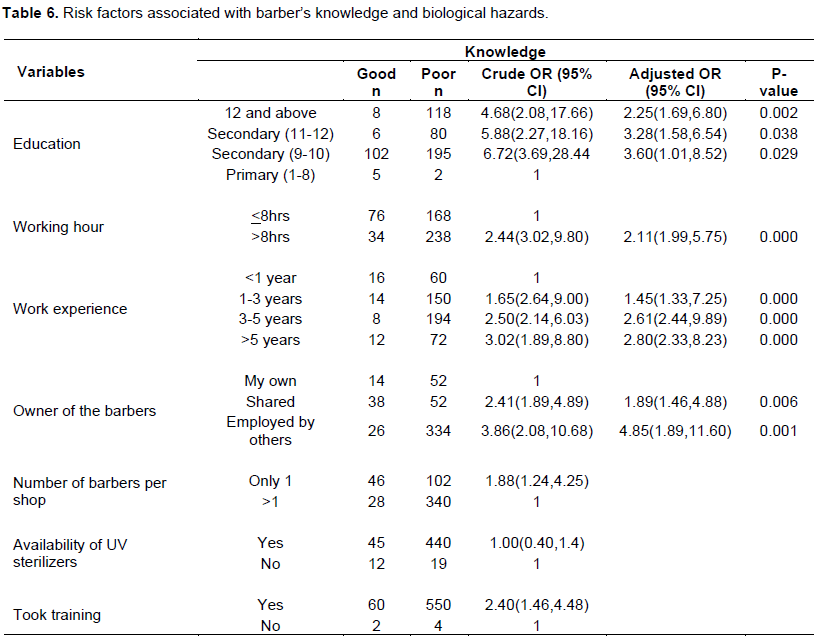
Barbers who spend less than eight hour per day on work are likely to have knowledge about biological risks related to their occupation as compared to those who spend more than eight hour per day on work [AOR=2.11, 95% CI: 1.988, 5.745]. This result is contradicting with the study conducted in Jimma, Ethiopia, Pakistan, Kharian city of Gujrat (Wazir et al., 2008). This might be because those who have more experience in their daily work are exposed to the problems and know the source of biological hazards. Moreover, they may have good access to media since they have media line in their working place.
According to this study, barbers who had better job practice know the risks of the biological hazards very well. Therefore, more than five years, 3-5 years and 1-3 years were more than two times more likely to be knowledgeable about biological hazards associated with their labor than those who had one or less work experience [AOR=2.80, 95% CI: 2.33, 8.23], [AOR=2.61, 95% CI: 2.44,9.89] and [AOR=1.45, 95% CI: 1.33,7.25]. This result is in line with studies conducted in Jimma, Ethiopia, Pakistan, Kharian City of Gujrat (Wazir et al., 2008). The barbers are more experienced as they encounter hazards and have increased knowledge.
In this study area, the barbers’ practice to decrease biological hazards related to their work is slightly low. Accordingly, about 369 (71.5%) practice safe to avert biological risks associated with their work.
This finding is higher than the studies conducted in Jimma Ethiopia, Pakistan; Kharian City of Gujrat District (Wazir et al., 2008), Bahra Kahu, Islamabad (Chaudhry et al., 2010), Rawalpindi and Islamabad and Sana’a City, Yemen (Al-RabeeI and Dallak, 2011). However, the stated studies used a solitary practice to define the practice of the study subjects.
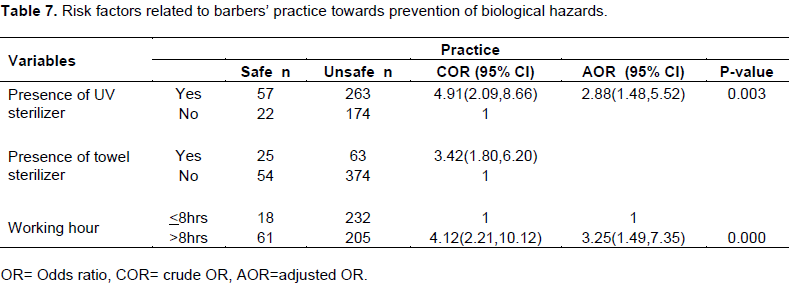
This study also revealed that the presence of UV light more likely supported the barbers to practice safely in their working room than those who had no UV light (Table 7). Also, those barbers who spent more than 8 h a day on work were more than three times likely to apply safety knowledge to avert biological hazards associated with their work as compared to those who spent eight or less hours on work. The likely explanation for this could be that barbers who work more than 8 h per day got more profits so that they can buy safety materials like ultra violet light sterilizer machine which are significant to remove health related hazards.
There were certain limitations in this study, depending on self- reported data of the participants which was liable to social desirability bias under or over estimation. Also, this study has not addressed the effect of attitude of the barbers on awareness and performance or practice. Although, this study tried to address some important factors, duration for sterilization and the type of chemical disinfectants were not addressed. Also, this study did not address the microbiological analysis.
In conclusion, the knowledge level of the employed barbers in Hawassa area was very good; however, greater part of the barbers practice is risky during their work.
Accessibility of UV sterilizers, advanced equipment in the barbers’ room and more working hours had significant association with the application of the barbers. Also, educational level, being self -owners, working hours and work experience had significant association with the knowledge of the barbers. Thus, provision of training on advancement of their knowledge minimizes the health risk related to their occupation. Also, it is better to address microbiological analysis of the tools that they use in barbering room.
The authors declare that there is no conflict of interest.
REFERENCES
|
Al-RabeeI NA, Dallak AM (2011). Knowledge, attitudes and practices of barbers regarding Hepatitis B and C viral infection in Sana'city, Yemen. J. Commun. Health 35:935-939.
|
|
|
|
Amodio E, Di Benedetto MA, Gennaro L, Massimo MC, Romano N (2010). Knowledge, attitude and risk of HIV, HBV and HCV infections in hairdressers of Palermo city (South Italy). Eur. J. Public Health 20(4):433-437.
Crossref
|
|
|
|
Arulogun O (2009). Attitude and sources of information about HIV/AIDS among Barbers in Ibadan, Nigeria. Niger. J. Heal Biomed Sci. 8(2):50-55.
|
|
|
|
Beyen T, Tulu K, Abdo A, Tulu A (2012). Barbers' knowledge and practice about occupational biological hazards was low in Gondar town, North West Ethiopia. BMC Public Health 12(942).
Crossref
|
|
|
|
Chaudhry M, Ashraf M, Afzal M, Niazi S (2010). Knowledge and practices of barbers regarding hepatitis B and hepatitis C in Bahra Kahu, Islamabad-Pakistan. Rawal Med. J. 35(1):37-40.
|
|
|
|
Ibrahim M, Tanimomo T (2007). Knowledge of HIV/AIDS, infection prevention practice and accidental skin cut in Barbing saloons in Sokoto. Nigeria. Niger. Med. Pract. 51(6):123-127.
Crossref
|
|
|
|
Khandait DW, Ambadekar NN, Vasudeo ND (1999). Knowledge and practice about HIV transmission among barbers of Nagpur city. Indian J. Med. Sci. 53:167-171.
|
|
|
|
Waheed Y, Safi S, Chaudhry W, Qadri I (2010). Awareness and risk factors associated with barbers in transmission of hepatitis B and C from Pakistani population: barber's role in viral transmission. Asian Biomed. 4(3):435-442.
|
|
|
|
Waheed Y, Sher ZS, Qadri I (2011). Role of Potash Alum in Hepatitis C virus Transmission at Barber's Shop. Virol. J. 8(1):211.
Crossref
|
|
|
|
Wazir MS, Mehmood S, Ahmed A, Jadoon HR (2008). Awareness among barbers about health hazards associated with their profession. J. Ayub Med. Coll. Abbottabad 20(2):35-38.
|
|
|
|
Zewudie T, Kurkura G (2002). Knowledge, attitudes and practices among barbers in South-Western Ethiopia. Afr. Newslett. Occup. Health Saf. 12(3):69-71.
|



