Full Length Research Paper

ABSTRACT
Diarrhoea is a disease condition of having at least three loose or liquid bowel movements each day. It often lasts for a few days leading to dehydration as a result of fluid and electrolyte losses. The aim of this study was to identify epidemiological factors leading to diarrhoea amongst children (0–5) years in selected hospitals in Makurdi, Benue State. An interviewer structured questionnaire was administered to 377 respondents. This was to enable the identification of certain risk factors that the respondents may be exposed to as well as potentially confounding variables and some basic demographic and clinical information regarding the people and their practices. Out of 377 cases examined, 51 (13.5%) were found positive for diarrhoea, which comprised 17 (13.2%) out of 129 male and 34 (14.3%) out of 248 female children. Highest prevalence was in children between aged 13-24 months, 23 (29.5%) and the least was among children between the aged 49-60 months and ≤ 12 months. There was statistically significant difference (P<0.05) between the ages and diarrhoea. The prevalence was highest in Federal Medical Centre (15.2%) and least was from Bishop Murray Memorial Hospital, Makurdi (9.9%). The findings indicated that hand washing, exclusive breast feeding and other hygienic practices reduce the chances of diarrhoea infection in infants.
Key words: Benue, children, diarrhoea, epidemiological, infection.
INTRODUCTION
Diarrhoea is defined as either watery stool or increased frequency (or both) when compared to a normal stool. It is a common problem that last few days and disappears on its own. It often lasts for a few days leading to dehydration as a result of fluid and electrolyte losses (Sinclair et al., 2013). Diarrhea is one of the waterborne diseases reported as the leading cause of death in children under-the age of five (Mamo and Hailu, 2014). Very unfortunately, 46% of under-five child mortality is due to diarrhea in which water related diseases take the higher percentage. According to WHO, diarrhea is the passage of 3 or more times loose or liquid stools per day or more frequently than the normal for the individual. Globally, diarrheal disease remains one of the principal causes of morbidity and mortality in children. In the world, children under-five years’ experience an average 3.2 instances of diarrhea every year (Kosek et al., 2003) and consequently 1.87 million children die from dehydration associated with diarrheal disease (Boschi-Pinto et al., 2008). In the developing countries especially Nigeria, diarrheal disease among under-five children accounts for about 21% of all deaths (Parashar et al., 2003; WHO, 2003). Of this, it is estimated that 15-20% or more percentage of community diarrheal disease is caused by unsafe drinking water (Mengistie et al., 2013). There are three types of diarrhoea which include; short duration watery diarrhoea, short duration bloody diarrhoea and persistent diarrhoea which lasts for more than two weeks (Agho et al., 2011). The short duration watery diarrhoea may be as a result of infection by cholera. It is rare in developed countries. If blood is present, it is also referred to as dysentery (Agho et al., 2011). The most severe threat posed by diarrhoea is dehydration. During the diarrhoea episode, water and electrolytes (sodium, chloride, potassium and bicarbonate) are lost through liquid stools, vomit, sweat, urine and breathing. Dehydration occurs when these losses are not replaced. The degree of dehydration is rated on a scale of three (Alikhani et al., 2007). Severe dehydration (at least two of the following signs): Lethargy/unconsciousness, sunken eyes, unable to drink or drink poorly, skin pinch goes back very slowly (≥2 s), restlessness, irritability and thirsty. The signs of dehydration often begin with loss of normal skin stretches irritable behavior and progress as a decrease in urination, loss of skin color, a fast heart rate, and decrease in responsiveness as it increases in severity (Addy et al., 2004). The diarrhoea may be acute (short-term, usually lasting several days), which is usually related to bacterial or viral infections (Chika et al., 2013). Diarrhoea infection is more common when there is a shortage of adequate sanitation and hygiene as well as safe water for drinking, cooking and cleaning. Rotavirus and Escherichia coli are the two most common etiological agents of moderate- to severe diarrhoea in low-income countries.
It is usually a symptom of gastrointestinal infection. Diarrhoea diseases due to infection constitute a major burden of disease (Okeke et al., 2000). Gastroenteritis is defined as an inflammation of the stomach, large and small intestines. It is said to be one of the most common illnesses in humans worldwide. Diarrhoea can affect individuals irrespective of age and sex; it represents a significant health risk to those at extremes of age, the very young and the very old. It is the second most common cause of death in adults, and a leading cause of childhood death worldwide (Ciccarelli et al., 2013). The causes of child mortality and morbidity in developing countries are multi-factoral. Although, Enterotoxigenic E. coli, Salmonella Paratyphi, Shigella species and viruses appeared to be the most common etiological agents,
however, certain circumstances are associated with and especially high incidence of acute diarrhoea disease (WHO, 2017). Interaction of socio-demographic, environmental and behavioral factors influences the occurrence of childhood diarrhoea morbidity (Dessalgon et al., 2011). Comparisons over time of the burden of diarrhoea diseases have revealed secular trends and demonstrated the impact of public health interventions (GBDDC, 2017). Though there are figurative decline in deaths due to diarrhoea disease among infants and children in developing countries, diarrhoea still remains the significant cause of morbidity and mortality in Africa (Keusch et al., 2006). Nevertheless, the causes of approximately 40% of the diarrhoeal cases are still unknown (UNICEF, 2010). Increased resistance of bacteria associated with diarrhoea is commonly linked to wrong application of antibiotics at home during treatment which is the first step some caregivers do and has presented a new challenge in the management of diarrhoea in children (0–5) (Ogbeyi et al., 2016; Aye et al., 2019). Due to this problem, the Benue State government in February 2017 had to undertake an enlightenment tour of all the 23 local government areas to educate caregivers on the dangers of managing diarrhoea using antibiotics. Diarrhoea can be acquired through consumption of food or water that has been contaminated with faeces or through direct contact with an infected person (WHO, 2017). Diarrhoea is a disease of global public health problem causing considerable morbidity and mortality in developing African countries (WHO, 2017). It is responsible for annual global deaths of about 2.6 million people mostly among African children under the ages of five years (Ademola et al., 2014). In Nigeria and particularly in Benue State, there is paucity of information on the epidemiological and demographic factors associated with diarrhoea infection in children (0 – 5 years) of age.
MATERIALS AND METHODS
Study area
Makurdi is the capital of Benue State, Nigeria; the city is located in the North central part of Nigeria along the Benue River. The major ethnic groups are Tiv, Idoma and Igede. Makurdi is home to Benue State University and the Federal University of Agriculture. Makurdi is located on the banks of Benue River, a major tributary of the Niger River. It shares boundaries with five other states in Nigeria namely: Nassarawa to the North, Taraba to the East, Ebonyi and Cross-River to the South-West with a common boundary with the Republic of Cameroon on the South-East (Figure 1).
Sample size determination
Samples sizes were determined by the Rao soft online calculator using accepted standard error of 5% at 95% confidence interval (Rao Soft Sample Size Calculator, 2014). For this study, a minimum of 301 children were required; however, sample size of 377 children was used for the study.
The equation for calculating sample size is shown below:
Where
Z is the z score (95%= 1.96).
Ε is the margin of error = 5% (0.05).
N is the population size.
p̂ is the population proportion= Standard deviation =0.5.
Ethical clearance
Ethical approval was obtained from Benue State Ministry of Health, and Federal Medical Centre. Informed consent was obtained from the participating patient’s guardians and caregivers. All the participants were asked for permission to be interviewed. The researcher handles those who accepted to participate and those who did not accept were left freely without any objection. Demographic information was obtained from the patient’s guardian or patient care-giver using a questionnaire.
Questionnaire administration
An interviewer structured questionnaire was administered to subjects. This was to enable the identification of certain risk factors that the respondents may be exposed to as well as potentially confounding variables and some basic demographic and clinical information regarding the people and their practices. Parents and care-givers of children of 0–5 years suffering from diarrhoea and who seeks medical attention in the designated health care centers were considered for inclusion in the study. Data were collected with the aid of this questionnaire adapted from NDHS.
Study population
The patients within the age of 0 - 5 years from the three selected hospitals in Makurdi were considered; both male and female were randomly chosen.
Sample collection
A total number of 377 parents and care-givers of children of 0-5 years suffering from diarrhoea and who seeks medical attention in the three different designated health care centers (hospitals) in Makurdi, namely Federal Medical Centre, Bishop Murray hospital and General hospital North Bank were interviewed. Out of the 377 subjects involved in the study, 248 were female and males were 129.
Statistical analysis
All data that were obtained from this study were entered into Microsoft Excel and analyzed using statistical package for social sciences (SPSS) version 19.0 statistical software. Both descriptive and analytical statistics were employed. Comparison based on age, sex and epidemiological factors were performed using chi square test to analyze data at P<0.05 significant level (Guerra et al., 2014).
RESULTS
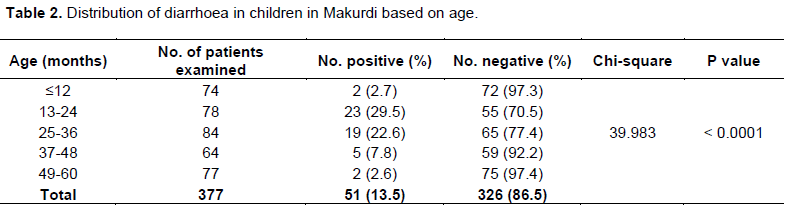
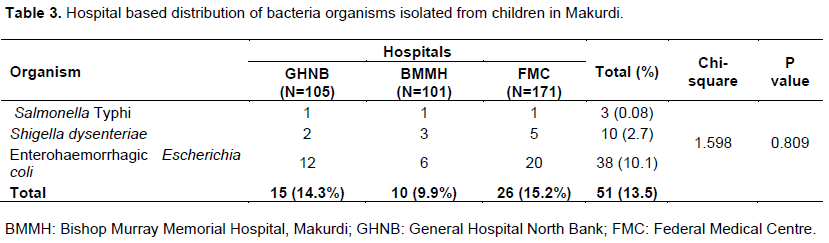
A total of 377 children in the 0-5 years age group were examined for the prevalence of bacteria causing diarrhoea among children attending Federal Medical Centre, Bishop Murray Memorial Hospital and General Hospital North Bank all in Makurdi. Out of the 377 stool samples analyzed, 51 (13.5%) were infected with diarrheal causing organisms. Of the 129 stool from male children examined, 17 (13.2%) were infected, while out of the 248 stools from female children 34 (13.7%) were infected. There was no significant association (P>0.05) between the diarrhea and the sex of the children examined (Table 1). Table 2 shows the distribution of diarrhoea in children based on age; children between 13-24 months of age were infected more than the other age groups 23 (29.5%) and the least were in children between 49-60 months and ≤ 12 months, 2 (2.6%) and 2 (2.7%) respectively. There was a statistical significant difference (P<0.05) between the age of the children and the diarrhea infection. Table 3 showed distribution of the organisms isolated from children in different hospitals in Makurdi, entero-haemorrhagic E. coli was highest in occurrence amongst the three bacteria organisms isolated followed by Shigella dysenteriae and the least was Salmonella Typhi, 38(10.1%), 10(2.7%) and 3(0.08%) respectively. There was a statistical significant difference (P<0.05) between the organism isolated and the diarrhea infection. Based on the distribution of the hospitals, stool samples collected from Federal Medical Centre Makurdi (15.2%) had the highest level of infection rate than General Hospital North Bank Makurdi (14.3%) and Bishop Murray Memorial Hospital (9.9%). There was no significant association (P>0.05) between the diarrhea and the hospital based distribution of the children examined (Table 3).

Risk factors
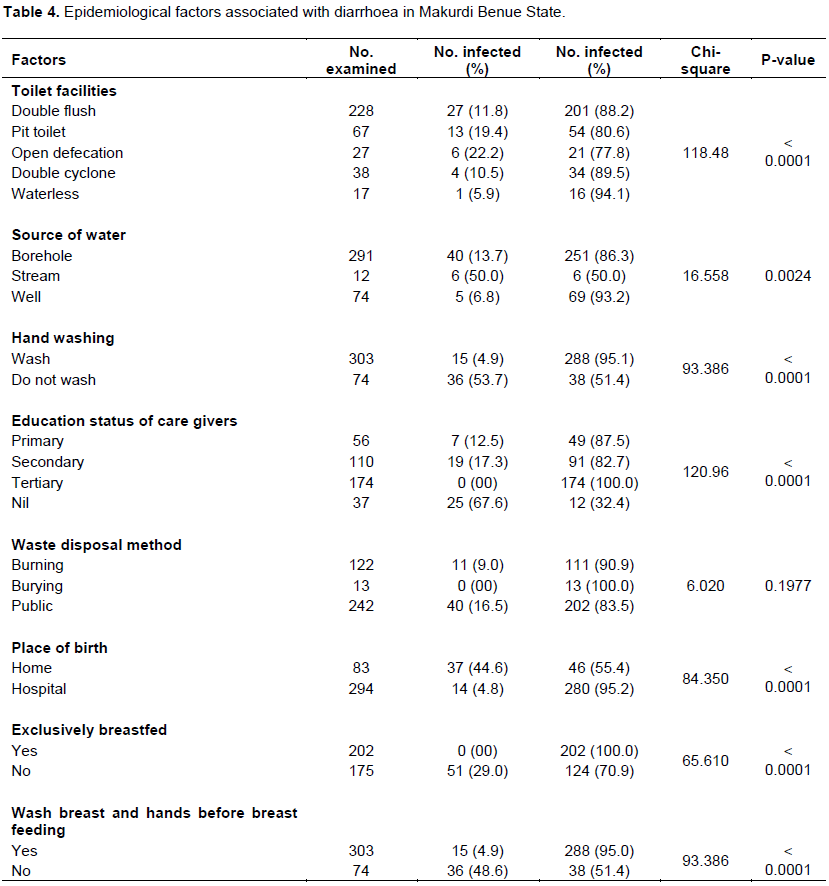
The chi-square analysis of different assumed factors with diarrhea in children showed significant association of toilet facilities, source of water, hand washing, educational status of the care givers, place of birth, exclusive breast feeding and washing of breast and hands before breast feeding. The factor waste disposal presented non-significant association (P>0.05) with diarrhea in children (Table 4).
DISCUSSION
This study investigated the prevalence of diarrheal occurrence and sociodemographic characteristics among children under the age of 5 years in Makurdi Benue State, Nigeria. The overall prevalence of diarrhea in this study was 13.5%; which was higher than the finding of the Ethiopian Demographic and Health Survey (EDHS) (2016), in which the magnitude of diarrheal disease among children less than 5 years old was 12% (CSA, 2016). However, this was lower than the works reported in the studies conducted in Burundi rural areas, 32.6% (Diouf et al., 2014); nomadic population in Afar region, 26.1% (Woldu et al., 2016); Arba Minch, Southern Nationalities, and Peoples’ region, 30.5% (Woldu et al., 2016); and Jijiga, Somalia region 27.3% (Hashi et al., 2016). The possible explanation for this difference could be the variation in the sociodemographic characteristics of the study subjects, socioeconomic development, and study periods. Peoples living style, behavioral change, and communication strategies of these areas could also contribute notably to such variations.
Type of toilet facility showed that care-givers that used open defecation had their children more infected than those that use pit toilet, waterless, double flush and double cyclone. The result further revealed that children whose care-givers depend largely on stream as source of water were significantly infected compared to those that depend on other sources of water like borehole and well in this order 50, 13.75 and 6.8% respectively. Infection was also higher amongst the children whose care-givers do not wash their hands and breasts before breastfeeding them. The result was statistically significant. Care-givers with no record of formal education had children who were more infected compare to the children of those with primary and secondary education certificates. The result shows that the prevalence was higher in Federal Medical Centre as compared to Bishop Murray Memorial Hospital and General Hospital, North Bank. The difference shown by our data is similar to the report of a previous surveillance study in Abuja (Ifeanyi et al., 2009). Although there are geographical differences in the spectrum of factors incriminated in childhood diarrhoea, several studies have shown the beneficial effects of breast-feeding in preventing morbidity and mortality from diarrhoea in infants. A case-control study in Brazil has shown that young infants who are not breast-fed have a 25-times greater risk of dying of diarrhoea than those who are exclusively breast-fed. We found that the children who were not exclusively breast-fed had greater risk of getting diarrhoea than those who were exclusively breast-fed. A longitudinal study in the urban slums of Lima, Peru found that exclusively breast-fed infants had a reduced risk of diarrhoea morbidity when compared with infants receiving only water in addition to breast-milk (Karambu et al., 2013). Infants who were partially breastfed or not breastfed had a risk of diarrhoea death than exclusively breastfed infants. According to Baker and others, an episode of diarrhoea was significantly less likely to last for six or more days if an infant was breastfed for three or more months. The risk of developing diarrhoea increases as the amount of breast milk an infant receives decreases. Studies by Pande et al. (2008) have compared exclusively breastfed infants, to infants who were exclusively formula-fed and were found to have an 80% increase in the risk of developing diarrhoea in the first year of life. Incidence of diarrhoea illnesses among breastfed infants was half that of formula-fed infants (Begum and Absar, 2016). These findings are in agreement with the findings of Begum and Absar (2016) that reveals a significant association of diarrhoea with children who were not exclusively breastfed. From the result of this study, along with numerous others in developing countries, the need to extend the duration of exclusive breast-feeding to at least 4-6 months cannot be over emphasized (Pande et al., 2008).
Also, diarrhoea infection was significantly high amongst care givers that do not wash their breast before breastfeeding. This likely implies that the children might have contracted the bacteria infection from unhygienic care-givers. Similarly, care givers that use open defecation had their children more infected than pit toilets and water flush systems. Water sources are one of the main risk factors associated with diarrhoea in children less than 5 years (Pande et al., 2008). Children whose care-givers use streams as their source of water were significantly infected with diarrhoea compared to those that use borehole and well. In a different study, treatment of unsafe water before drinking was done by about half of the study participants with majority of participants identifying with boiling method; however, none of the method was found to have any association with diarrhoea (Ehiri et al, 2015).
Children who washed hands before eating are at less risk to get diarrhoea infection as compared to those who did not wash their hands and about three times less likely to those who wash hands after visiting toilet respectively. The same opinion was found by Cochrane Database of Systematic Reviews (CDSR) who revealed that hand washing reduced episodes of diarrhoea by 30%, an intervention that has been shown to reduce transmission of diarrhoea-causing organisms (Ehiri et al, 2015). These findings are in harmony with a study done on a systematic and meta-analysis of sanitation, water and hygiene in less developed countries, expounding that washing one's hands with soap is another important barrier to transmission. Hand washing promotion and interventions are estimated to have the potential to prevent one million deaths from diarrhoea diseases. This study found out that children whose care-givers do not wash their hands were significantly infected with diarrhoea illness more than one and half times as compared to those washing hands.
CONCLUSION
This study has shown that children within 13 to 24 months were more infected with diarrhoea. Source of drinking water, inability to exclusively breastfeed the infants and some unhygienic practices of care-givers significantly increased the prevalence of diarrhoea in the study area. Hand washing promotion probably reduces prevalence of diarrhoea infection in infants. There is a strong association between source of drinking water and bacteria causing diarrhoea. Most of the children whose care-givers admitted the use of streams as source of water had a high prevalence of diarrhoea infection. Also from the result, it could be concluded that exclusive breastfeeding reduce the chances of diarrhoea infection. Open defecation should be discouraged and pit toilet and water flush system be encouraged.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Addy PAK, Antepim G, Frimpong EH (2004). Prevalence of Pathogenic Escherichia coli and Parasites in infants with diarrhoea in Kumasi, Ghana. East African Medical Journal 81(7):353-357. |
|
|
Ademola O, Oluwatoyin I, Andebola (2014). A study of the prevalence of diarrheogenic Escherichia coli in children from Gwagwalada, Federal Capital Territory, Nigeria. The Pan African Medical Journal 17-146. |
|
|
Agho KE, Dibley MJ, Odiase JI, Ogbonmwan SM (2011). Determinants of exclusive breastfeeding in Nigeria. Biomedical Centre, Pregnancy and Childbirth 11(2):1471-2180 |
|
|
Alikhani MY, Mirsalehian A, Fatollahzadeh B, Pourshafie MR, Aslani MM (2007). Prevalence of Enteropathogenic and Shiga Toxin-producing Escherichia coli among Children with and without Diarrhoea in Iran. Journal of Health Population Nutrition 25(1):88-93. |
|
|
Aye AM, Gberikon GM, Aguoru CU, Onyilokwu SA (2019). Molecular Characterization of Bacteria Associated with Diarrhoea in Children (0-5) from some selected Hospitals in Makurdi, Benue state. International Journal of Scientific Research and Publication 9(11):311-316. |
|
|
Begum MUH, Absar MN (2016). Diarrhea in Breastfed versus Formulafed Baby. A Hospital Based Study in 150 Children. Journal of College of Physicians and Surgeons 34(1):1-25. |
|
|
Boschi-Pinto C, Velebit L, Shibuya K (2008). Estimating child mortality due to diarrhoea in developing countries. Bulletin of the World Health Organization 86(9):710-717. |
|
|
Central Statistical Agency (CSA) (2016). Ethiopia demographic and health survey. Addis Ababa, Ethiopia, and Rockville, Maryland, USA. |
|
|
Chika E, Ugwu M, Ifeanyichukwu I, Thaddeus G, Carissa D (2013). Detection and antimicrobial susceptibility of some gram negative bacteria producing carbapenemases and extended spectrum β-Lactamases. International Journal of Microbiology and Immunology Research 2:64-69. |
|
|
Ciccarelli S, StolfiI, Caramia G (2013). Management strategies in the treatment of neonatal and pediatric gastroenteritis. Infection and Drug Resistance 6:133-161. |
|
|
Dessalgon M, Kumie A, Tefera W (2011). Predictors of under-five childhood diarrhea at Mecha District, West Gojam, Ethiopia. Ethiopian Journal of Health and Development 25(3):193-199. |
|
|
Diouf K, Tabatabai P, Rudolph J, Marx M (2014). Diarrhoea prevalence in children under five years of age in rural Burundi: An assessment of social and behavioural factors at the household level. Global Health Action, 7:1. Article ID 24895, 2014. |
|
|
Ehiri JE, Arikpo D, Martin M, Meremikwu MM, Critchley JA, Ejemotâ€Nwadiaro RI (2015). Hand washing promotion for preventing diarrhoea Cochrane Library. Cochrane Database of Systematic Reviews (9). |
|
|
Global Burden of Diarrhoea Diseases Collaborators (GBDDC) (2017). Estimates of global, regional, national morbidity, mortality, and aetiologies of diarrhoea diseases: a systematic analysis for the Global Burden of Disease Study. The Lancet Infectious Diseases 17:909-948 |
|
|
Guerra JA, Romero-Herazo YC, Arzuza O, Gómez-Duarte OG (2014). Phenotypic and Genotypic Characterization of Enterotoxigenic Escherichia coli Clinical Isolates from Northern Colombia, South America. Biomedical Research International 10:1-11. |
|
|
Hashi A, Kumie A, Gasana J (2016). Prevalence of Diarrhoea and Associated Factors among Under-Five Children in Jigjiga District, Somali Region, Eastern Ethiopia. Open Journal of Preventive Medicine, 6(10):233-246. |
|
|
Ifeanyi CIC, Nnennaya IR, Casmir AA, Nkiruka I (2009). Enteric Bacteria Pathogens Associated With Diarrhoea of Children in the Federal Capital Territory Abuja, Nigeria. New York Science Journal 2(7):62-69 |
|
|
Karambu S, Matiru V, Kiptoo M, Oundo J (2013). Characterization and factors associated with diarrhoeal diseases caused by enteric bacterial pathogens among children aged five years and below attending Igembe District Hospital, Kenya. The Pan African Medical Journal 16(37):2947. |
|
|
Keusch GT, Fontaine O, Bhargava A, Boschi-Pinto C, Bhutta ZA, Gotuzzo E, Rivera J, Chow J, Shahid-Salles S, Laxminarayan R (2006). Diarrheal Diseases. In: Disease Control Priorities in Developing Countries, 2nd edition |
|
|
Kosek M, Bern C, Guerrant RL (2003). The global burden of diarrhoeal disease, as estimated from studies published between 1992 and 2000. Bulletin of the World Health Organization 81(3):197-204. |
|
|
Mamo A, Hailu A (2014). Assessment of prevalence and related factors of diarrheal diseases among under-five year's children in debrebirehan referral hospital, Debre birehan town, North Shoa Zone, Amhara Region, Ethiopia. Open Access Library Journal 1(1):1-14. |
|
|
Mengistie B, Berhane Y, Worku A (2013). Prevalence of diarrhea and associated risk factors among children under-five years of age in Eastern Ethiopia: A cross-sectional study. Open Journal of Preventive Medicine 3(7):446-453. |
|
|
Ogbeyi GO, Onyemocho A, Ogbonna C (2016). Assessment of caregivers' knowledge of diarrhoea and practice of home management of diarrhoea disease among under two children in Opialu, a rural community in Benue State, Nigeria. Global Journal of Public Health Medicine 5(2):2277-9604 |
|
|
Okeke IN, Lamikanra A, Steinruck H, Kaper JB (2000). Characterization of Escherichia coli strains from cases of childhood diarrhea in provincial southwestern Nigeria. Journal of Clinical Microbiology 38(1):7-12. |
|
|
Parashar UD, Bresee JS, Glass RI (2003). The global burden of diarrhoeal disease in children. Bulletin of the World Health Organization 81:4. |
|
|
Rao soft Calculator (2014). Www.Raosoft.Com/ Samples size International. |
|
|
Saket P, Michiel A, Keyzer AA, Ben GJS S (2008). Addressing diarrhoea prevalence in the West African Middle Belt: social and geographic dimensions in a case study for Benin. International Journal of Health Geographics 7 (17):1476-072. |
|
|
Sinclair MI, Harris AH, Kirk M, Fairley CK (2003). Cost of community gastroenteritis. Journal of Gastroenterology andHepatology18:322-328. |
|
|
UNICEF (2010). Diarrhoea disease. Child information monitoring the situation of children and women. |
|
|
Woldu W, Bitew BD, Gizaw Z (2016). Socioeconomic factors associated with diarrheal diseases among under-five children of the nomadic population in northeast Ethiopia. Tropical Medicine and Health 44(1):40. |
|
|
World Health Organization (2017). Diarrhoeal disease Diarrhoeal disease is the second leading cause of death in children under five years old. It is both preventable and treatable |
|
|
World Health Organization (2003). Guidelines for Safe Recreational Water Environments: Coastal and Fresh Waters, World Health Organization. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


