ABSTRACT
Diabetes is a global health issue as it is a metabolic disease that affects individuals of all ages. The success of long term maintenance therapy for diabetes mellitus depends largely upon the patient’s compliance with a therapeutic plan. This study investigated the level of compliance with treatment regimen among clients with diabetes mellitus in selected hospital in Benin City, Edo state. A descriptive cross sectional design was used, A total of 300 hundred and six (306) diabetic patients were selected using the convenient sampling technique. The instrument for data collection was a self-structured questionnaire. Data collected were analyzed using descriptive statistic in Statistical Package for Social Sciences (SPSS) version 21. Results from the study showed that 59.3% of the respondents had good knowledge of diabetes while 37.7% of the respondents had fair knowledge, and 3.0% of the respondents had poor knowledge. Majority 184 (61.3%) of the respondent had poor compliance to their treatment regimen. Significant relationship between the level of compliance and demographic characteristics of the respondents like sex (p=0.0011), religion (p=0.040) and ethnic group (p=0.007) was found. There was also a significant relationship (p=0.000) between the knowledge of diabetes and rate of compliance of the respondents. More also, a significant difference was found in the level of knowledge of diabetes among the respondents in the two hospitals (p. = 0.000). Similarly, there was a significant relationship in the rate of compliance to diabetic regimens among the respondents in the selected hospitals (p = 0.010) Therefore, it is recommended that government should subsidized drugs and laboratory investigation for diabetics patient as well made the drugs available in the government owned pharmacy.
Key words: Non-compliance, compliance, diabetic patient, diabetes treatment regimen.
Diabetes is a serious public health problem that threatens the quality of life of patients with the disease; it can lead to acute and chronic complications. It is a significant cause of disability and death in many countries (Amokute and Hussein, 2011). Diabetes is a chronic disease of life long duration and its management requires a fundamental change in the patients’ life style. The most important member of the diabetic care team is the patient. The success of long term maintenance therapy for diabetes mellitus depends largely upon the patient’s compliance with a therapeutic plan (Adejoh, 2014). Compliance has been defined as the extent to which individuals follow the instructions they are given for prescribed treatments (Haynes et al., 2008). The term 'compliance ' is intended to be non-judgemental -a statement of fact rather than of blame of the individual, the prescriber or the treatment. Compliance with a prescribed therapeutic regimen is a complex health behaviour and can reduce morbidity or mortality of chronic illness where information provided to the patient increases their knowledge and understanding of the risk factors for their illness and teaches preventive behaviours like exercises, smoking cessation, dietary changes, medication and stress management (Evans and Haynes, 2013).
Non-compliance is the failure or refusal to conform to a prescribed medication, diet or to follow a prescribed course of treatment. It is described as an act of not yielding, cooperating or responding to a particular demand, regimen, and request. In spite of advanced technology in the medical field and the management of diabetic clients in terms of drugs and diet, the problem of non-compliance to prescribed therapy continues to occur among diabetic clients. This attitude of non-compliance has called for a greater concern in the follow- up of clients to treatment and the overall response to the diabetic management in our hospitals. Despite several approaches and strategies taken to tackle the problem of non-compliance of client to diabetic treatment, noncompliance to diabetes treatment remains a public health challenge (Alberta et al., 2012). For example, a descriptive correlational design study by Nadia (2011), to examine the level of non-compliance to diabetes management in Zagazig university hospital, Zagazig city, Egypt . Results showed that more than half of the patients (56.3%) had adequate total compliance to diabetes management. The highest compliance was with follow up (88.8%) while the lowest compliance was with self-care activities (17.5%) and self-testing (36.3%).
In another study conducted by Samia (2010), to assess the level of non-compliance to treatment regimen among diabetic clients attending the internal medical department and outpatient clinic at Assiut university hospital. Results revealed that most of the patients had good compliance with treatment regimen and 60% had good compliance with diet regimen, while only 26% of patient had good compliance with foot care, 15% did not follow regimen at all, 35% of the subjects considered that routine daily physical activities as exercise and only 2% of the subjects considered walking as exercise but not daily. Majority of the patients (78%) adhered to medical treatment prescribed. Also, according to a retrospective cohort study conducted by Donnan et al. (2011), in the Tayside centre for general practice, department of medicine, university of Dundee, Uk to examine the diabetic clients level of non-compliance to their therapeutic regimen. Results showed that in those prescribed sulphonyureas alone, 31% had adequate compliance compared with 34% in those metformin alone. Those with better compliance tended to be younger and have a significantly shorter duration of diabetes. For the sulphonyureas, 35% of those taking one tablet a day had adequate compliance compared with 27% of those taking more than one tablet per day. However, a descriptive correlational design was conducted by Simon (2007), to examine the level of non-compliance to treatment regimen among diabetic patients in department of medicine, veterans Administration hospital, university of Washington. Results revealed that non-compliance was common among patients prescribed oral hypoglycemic medications; the average population of non-compliance was 53.7%. 47.8% of the population engaged in exercise sessions only once a week or less, whereas 10% reported that they rarely followed a healthy diet plan.
Furthermore, a cross sectional study by Taruna (2014), among diabetic patients attending Doon Government hospital, Dehradu, Uttarakhnad, India to assess the level of non-compliance of among diabetic clients. Results revealed that non-compliance was highly significant (61.5%) associated with frequent dosing and multiple drugs in the prescription, especially attributed to the forgetfulness in the older/occupationally retired age groups. Only 23.3 and 31.7% of the participants were found to be compliant to diet and exercise regimen. Similarly , a cross sectional descriptive study by Abdulazeez (2014), to assess the level of non-compliance of diabetic clients to their treatment regimen in the outpatient clinic of the university of Ilorin teaching hospital, Nigeria. Result shows the number of males was 45.45% and the female 54.55%, and the total number of male patients that were found to be compliant with their medications was 22.3% as compared to the female patients that were compliant with their medication which was 36.2%. The numbers of female and male patients found not to be compliant with their medication were 58% and those not compliant to be 25.8%. This shows that about one third or more of patients have poor compliance with prescribed medications. Individuals with diabetes are of greater risk of long term complications such as kidney disease, infections, peripheral vascular disease, lower extremity ulcers, amputations, neuropathy and retinopathy.
Statement of the problem
According to the data from the World Health Organisation (2011), over 3million people die worldwide from diabetes and its related complications every year as a result of non-compliance. In 2011,about 282,000 emergency room visits for adults aged 18years or older had hypoglycaemia as a result of non-compliance to their diet while about 175000 emergency room visits for people of all ages had hyperglycaemic crisis for example, diabetic ketoacidosis due to non-compliance to their treatment regimen. In 2010, among adults aged 20years or older, hyperglycaemic crisis caused 2361 deaths. In 2009 to 2012, of adults aged 18years or older with diagnosed diabetes, 71% had blood pressure greater than 140/90 mmhg, 65% had blood low density lipoprotein (LDL) cholesterol greater than or equal to 100mg/dl. In 2011, 49677 people of all ages began treatment for kidney failure due to non-compliance to diabetic therapy. In 2010, about 73000 non-traumatic lower limb amputations were performed in adults aged 20years or older due to non-compliance to therapeutic regimen. In 2009, death rates were about 1.5 times higher among adults aged 18 years or older with diagnosed diabetes who did not comply to their treatment (WHO, 2011). Omorogiuwa et al. (2010) in a survey carried out on a university community, Ekpoma, Edo State, Southern Nigeria, reported an overall prevalence of as high as 9.8%. In another study among adults aged 18 years and above residing in five rural communities in Edo State, an overall crude prevalence of 4.6% with sex differences (males 1.9%, females 5.8%, P = 0.012) was reported (Isara and Okundia, 2015). The researcher's curiosity was prompted during clinical posting in one of the hospital, where a diabetic patient was brought in for amputation for severe diabetic foot ulcer. From the history taken, it was observed that the patient has been non-compliant with his diet and medication which led to the complication. There are few empirical studies on compliance to diabetic treatment regimen in this part of the country especially from Edo state, hence the need for this study.
Purpose of the study
The purpose of this study is to assess the compliance to treatment regimen among clients with diabetes mellitus in selected hospitals in Benin City, Edo state.
Objectives of the study
The Objectives of this study is to;
(1) Assess the level of knowledge of diabetic client on diabetes mellitus in selected hospitals in Benin City, Edo state
(2) Assess the level compliance with treatment regimen among clients with diabetes mellitus in selected hospitals in Benin City, Edo state.
(3) To find out the relationship between the diabetic patients level of compliance and social demographic characteristics (sex, age, educational status, economic status) among other patients in selected hospitals in Benin City, Edo state.
Research hypothesis
(1) There is no significant relationship between the level of knowledge about diabetes mellitus and the rate of compliance among diabetic patients in selected hospitals in Benin City, Edo state.
(2) There is no significant difference in knowledge of diabetic mellitus among the clients in the selected Hospitals.
(3) There is no significant difference in the level of compliance to diabetic treatment regimen among the diabetic patients in the selected Hospitals.
Significance of the study
The results of the study will contribute to increase the knowledge of diabetic patients, the family, community, society, and the country as a whole about nutrition, exercise, medication and preventive strategies. It will also help the health care institutions in conducting education and training programs which are directed to promote sound practice and improved participation in patient's care. It will also increase the awareness of the health professionals on strategies to enhance patients compliance and efforts to improve the health care services rendered to the diabetic clients which in -return will encourage the patients. It will also motivate the nurses, dieticians, social welfare workers, community and religious leaders to provide help for the less privileged clients through non-governmental organisations (NGOs) and philanthropic organisations to assist in the improvement of diabetic patient’s compliance. Further-more, this study will add to an existing body of knowledge on the level of non-compliance among diabetic patients and will also serve as secondary data for further researches.
Research design
The researcher adopted a cross- sectional research design.
Research setting
University of Benin Teaching hospital and Central hospital, Benin City were purposely selected for this study.
University of Benin Teaching hospital (UBTH)
UBTH is a tertiary health facility located on the Benin Lagos Express-way, in Egor Local Government Area of Edo state, Benin City and came into being in 1973 following the enactment of an edict (number 12). As the sixth of the it’s generation teaching hospitals in Nigeria. It was established to complement her sister institution, University of Benin and to provide secondary and tertiary care to the then Mid-western Region (now Edo and Delta state) and it's environs.
Central hospital
Central hospital was created in 1902 by the then colonial masters who were owned by the British government before independence under the colonial master. It is a government hospital located in the serene centre of Benin, on Sapele road, Oredo Local Government Area of Edo state, Benin City.
Target population
The target population comprised of 415 and 497 diabetic patients both males and females attending the out -patient department in the University of Benin Teaching hospital and Central hospital, Benin city respectively. This population was gotten by taking a retrospective review of daily attendance to the outpatient diabetic clinic in both hospitals from January to July 2017. This review shows an average monthly attendance of 415 and 497 in both hospitals respectively. Making the total population to 912 as seen in Table 1.
Sample size
A sample size of three hundred and nine (306) was used for the study. This was gotten from the total population of 912, using Taro Yamane (1967) formula as shown below:

Where:
n = sample size, N = population size, d = level of precision (confidence interval)
N = 912, d = 0.05
Thus = 912/1+912(0.05)2
n = 912/1+912*0.0025
n = 912/1+2.28
n = 912/3.28
n = 278
10% Attrition rate =27.8
278 +27.8 =305.8
= 306, Therefore, sampling size is 306.
Sampling technique
Convenient sampling techniques were used.
Instrument for data collection
The instrument was a self-structured questionnaire comprising of three sections:
Section A: Comprises of 7 items of demographic data of the participants.
Section B: Comprises of 11 items close ended questions on the level of knowledge about diabetes. The knowledge will be classified as poor (0 to 3), average (4 to 7) and good (8 to11).
Section C: Comprises of 13 items close ended questions on compliance to diabetic therapy using 4-point lirket scale. This compliance will be classified as poor compliance and good compliance based on an average mean score for each item using 2.5 as the decisional rule.
Validity of the instrument
Validity of the instrument was ensured by two consultant endocrinologist from the selected hospital and an expert in measurement and evaluation from University of Benin.
Reliability of the instrument
This was done by administering 20 of the questionnaire to similar respondents with same characteristics in another hospital. Data generated were analysed using split-half method, and the cronbachs Alpa scored was 0.780 which shows that the instrument is reliable and can be used for the study.
Method of data collection
Two research assistants, a male and a female nurse who worked in the selected hospital were recruited. They were trained by the principal researcher on how to administer the questionnaire. The research assistant after training were subjected to interrater reliability test and to know if both will achieve the same result as stated in the objective of the study. The result shows that both were able to measure the same thing using the instrument. The researcher and the assistants visit the hospital on the various clinic days to obtain data from the respondent after due explanation of the purpose of the study to them. Questionnaires were distributed to them while waiting for their turn to see the doctor or after seeing the doctor to ensure that their major aim of coming to the clinic was not obstructed or denied. Immediately after filling, the questionnaires were retrieved from them.
Method of data analysis
The researcher used descriptive statistics. Statistical Package for Social Sciences (SPSS) version 21 was used to analyse the data.
Ethical consideration
Ethical clearance with protocol number ADM/E22/AVOL.VII/14571 was obtained from the ethical and research committee of the university of Benin teaching hospital, Benin City after thorough review the proposal. Administrative permit was also obtained from the Nursing Services Department of UBTH and Central Hospital. Consent of the respondents was sort for before proceeding and confidentiality was held in high esteem.
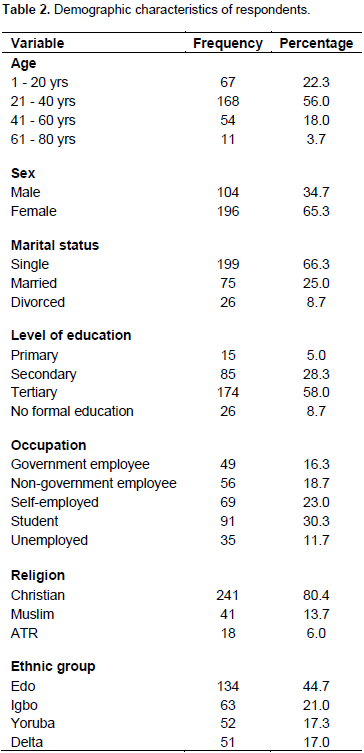
Socio-demographic characteristics
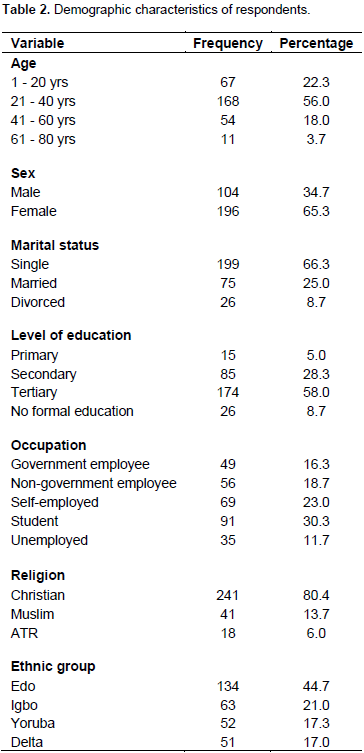
Table 2 shows that majority 168 (56.0%) are between the ages of 21 to 40 years which is the highest, 67 (22.3%) are between 1 to 20 years, 54 (18.0%) are in the 41 to 60 years range, while the lowest 11 (3.7%) are in the age group 61 to 8 years. Majority 196 (65.3%) of the respondents are females, most of the respondents in this study are single 199 (66.3%) with only 75 (25.0%) married and 26 (8.7%) divorced. 174 (58.0%) of the respondents had tertiary education, this is followed by secondary school with 85 (28.3%), the least was primary education 15 (5.0%). Occupation had majority 91 (30.3%) as students, this was followed by 69 (23.0%) who are self-employed and 35 (11.7%) unemployed. Majority 241 (80.4%) of the respondents are Christians.
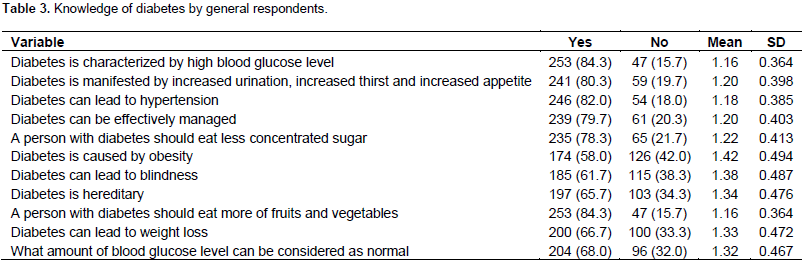
Objective one: Respondents knowledge of diabetic mellitus
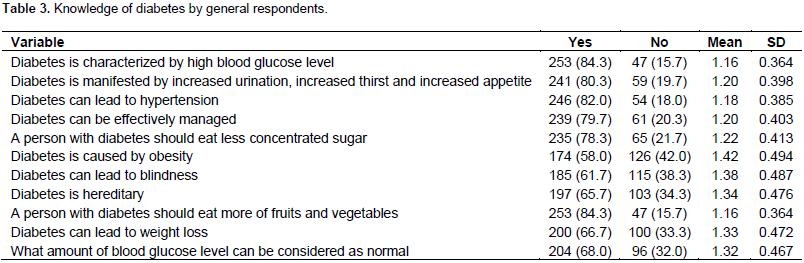
The knowledge of diabetes was tested and is shown in Table 3. 253 (84.3%) said diabetes is characterized by high blood glucose level, 241 (80.3%) said diabetes is manifested by increased urination, increased thirst and increased appetite. 256 (82.0%) said diabetes can lead to hypertension, 239 (79.7%) said diabetes can be effectively managed. A person with diabetes should eat less concentrated sugar was mentioned by 235 (78.3%) respondents, diabetes is caused by obesity had 174 (58.0%), 185 (61.7%) of the respondents said diabetes can lead to blindness, while diabetes is hereditary was mentioned by 197 (65.7%) of the respondents. 253 (84.3%) said a person with diabetes should eat more of fruits and vegetables, 200 (66.7%) said diabetes can lead to weight loss and 204 (68.0%) said 80 to120 mg/dl is the normal blood glucose level.
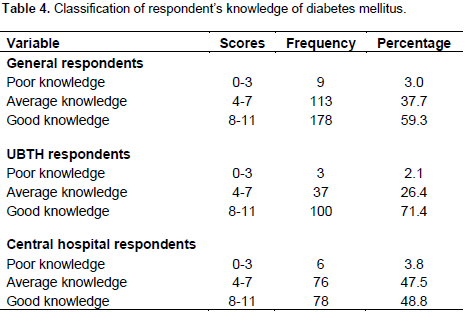
Classification of respondent’s knowledge of diabetes mellitus
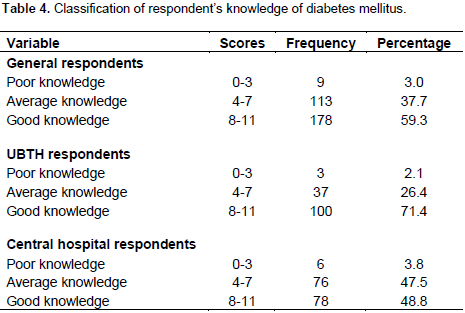
Table 4 shows the knowledge of diabetes of respondents. For the general knowledge of the respondents, 9 (3.0%) had poor knowledge, 113 (37.7%) had fair knowledge and 178 (59.3%) had good knowledge. The knowledge of the UBTH respondents also follow the same trend of the knowledge of the general population by reporting, 3 (2.1%) had poor knowledge, 37 (26.4%) had fair knowledge and 100 (71.4%) had good knowledge. A similar upward trend was also recorded for the central hospital respondents with 6 (3.8%) having poor knowledge, 76 (47.5%) with fair knowledge and 78 (48.8%) with good knowledge.
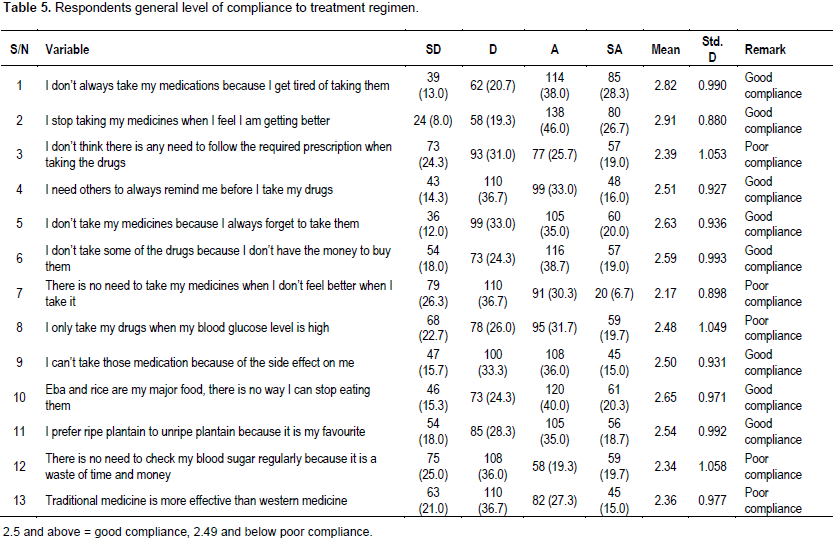
Objective two: Compliance to diabetic treatment regimen by respondents
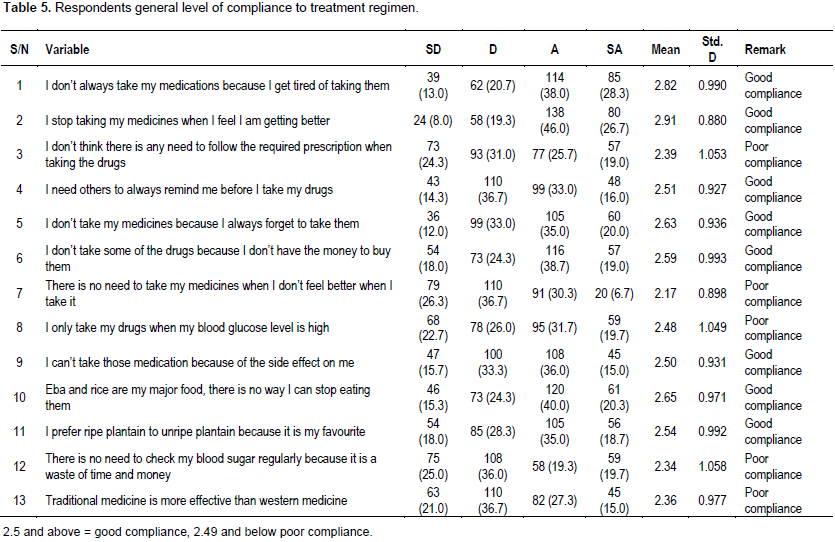
Table 5 shows the general rate of compliance to diabetic treatment regimen by respondents. The analysis revealed that items 1 (2.82±0.990), 2 (2.91±0.880), 4 (2.51±0.927), 5 (2.63±0.936), 6 2.59±0.993), 9 (2.50±0.931), 10 (2.65±0.971) and 11 (2.54±0.992), had good compliance with treatment regimen. Items 3 (2.39±1.053), 7 (2.17±0.898), 8 (2.48±1.049), 12 (2.34±1.058) and 13 (2.36±0.977) showed poor compliance.
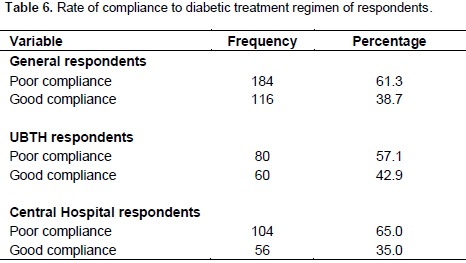
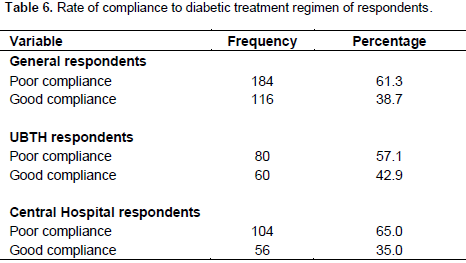
Rate of compliance to diabetic treatment regimen of respondents
Table 6 shows the rate of compliance to diabetic treatment regimen of respondents. For the general rate of compliance of respondents, 184 (61.3%) had poor compliance, 116 (38.7%) had good compliance to diabetic treatment regimen. The rate of compliance for UBTH respondents also follow the same trend of the general population, were majority 80 (57.1%) had poor rate of compliance and 60 (42.9%) had good rate of compliance to treatment regimens. A similar downward trend was also recorded for the central hospital respondents with majority 104 (65.0%) having poor rate of compliance, while 56 (35.0%) having good knowledge to treatment regimen.
Perceived factors affecting compliance to diabetes treatment among the general respondents
Table 7 shows that lack of finance (2.93), diabetic medications and investigations are too expensive (2.77), and unavailability of the medication in the hospital (2.63). As the average mean of this item on a four point lirket scale are above 2.5, hence they are consider as strong determinant of non-compliance.

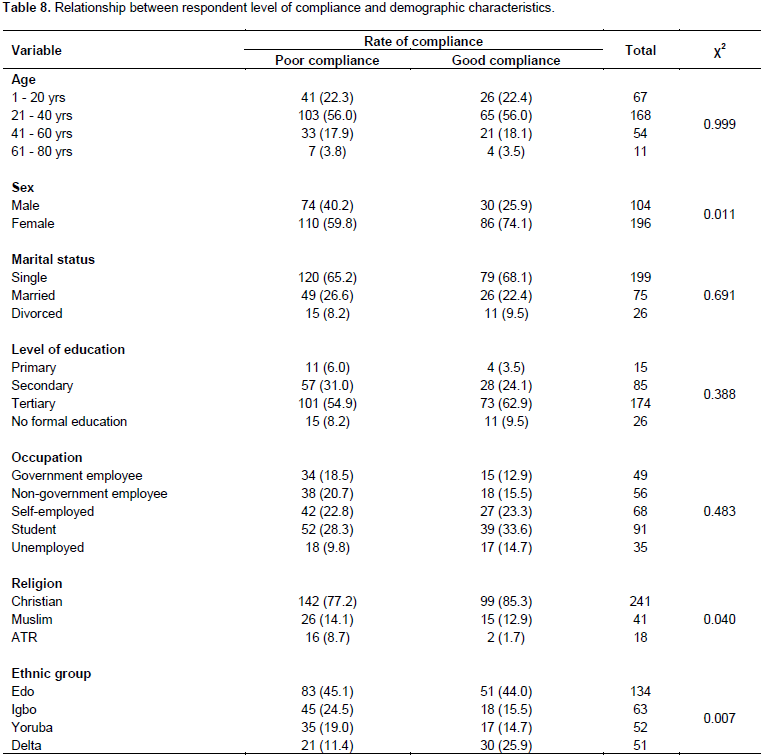
Objective three: To find out the relationship between the diabetic patients level of compliance and social demographic characteristics (sex, age, educational status, economic status) among other patients in selected hospitals in Benin City, Edo state
Table 8 shows the relationship between rate of compliance to diabetic treatment regimen and the demographic characteristics of respondents. The results shows that the rate of compliance to diabetic treatment regimen did not show any relationship with the age of respondents (p=0.999), sex on the other hand had a significant relationship with rate of compliance to diabetic treatment regimen (p=0.011), marital status (p=0.691) showed no significant relationship with the rate of compliance to diabetic treatment regimen. The rate of compliance to diabetic treatment regimen and educational level also did not show any significant relationship (p=0.388), also with the occupation of the respondents (p=0.483). Religion and ethnic group on the other hand showed a significant relationship with the rate of compliance to diabetic treatment regimen (p=0.040 and 0.007) respectively.

Hypothesis one
Table 9 shows the relationship between the rate of compliance of diabetic patients to treatment regimen and knowledge of diabetes. The results shows that there is a highly significant relationship (p=0.000) between the knowledge of diabetes and rate of compliance of the respondents.

Hypothesis two
Table 10 shows the difference in the knowledge of diabetes between respondents of UBTH and Central hospital. The result shows that there is a significant difference in the level of knowledge of diabetes between the two hospitals (Sig. = 0.000).
Hypothesis three
Table 11 shows the difference in the rate compliance of diabetic regimens of respondents in UBTH and Central hospital. The result shows that there is a significant relationship in the rate of compliance to diabetic regimens between the hospitals (Sig. = 0.010).

Findings from the study shows that majority 168 (56.0%) are between the ages of 21 to 40 years which while the lowest 11 (3.7%) are in the age group 61 to 80 years. Majority 196 (65.3%) of the respondents are females, with only 75 (25.0%) of the respondents being married. 174 (58.0%) of the respondents had tertiary education and primary education 15 (5.0%). majority 91 (30.3%) are students, 69 (23.0%) self-employed and 35 (11.7%) unemployed. Majority 241 (80.4%) of the respondents are Christians. 134 (44.7%) are of the Edo ethnic group. This study revealed that majority of the respondents 59.3% had good knowledge of diabetes, 37.7% had average knowledge, while 3.0% had poor knowledge of diabetes. This is in line with the study conducted by Jansirani (2013) who revealed that most of the clients (59.9%) had adequate knowledge of diabetes while those with poor knowledge were 32.4%, majority of the informants expressed that the disease can cause damage to vital organs while few declared that they did not know anything about the complications. Also, Nwaokoro (2010) in Owerri, Imo state of Nigeria, reported that most of the patients (62%) understood the value of blood glucose control; the others were not knowledgeable about diabetes (40.3%). This finding is higher than that reported by Chutiyami (2016) in Maiduguri Borno state, Nigeria, who revealed that almost less than half (47.2%) of respondent were able to defined diabetes mellitus correctly as a disease characterised by high blood sugar level as against various opinions by other clients.
These findings indicated that quite a high percent of the clients are not knowledgeable about diabetes which by implication will reduce compliance to diabetes treatment regimen. Also Nadia (2011), in Zagazig city, Egypt reported that the knowledge of the clients about diabetes was even low with only 28.8% reaching satisfactory level and 68.7% are not knowledgeable about diabetes. Similar findings was also reported by Mohamed (2010), who showed that only 38% of the clients had adequate knowledge about diabetes mellitus which prompted their compliance while 62% of the clients did not properly understand what diabetes is all about and treatment. The high level of knowledge recorded in this index study is highly associated with social-demographics characteristics such as educational level, level of income and religion. As majority had tertiary education meaning they are well read and can source for information themselves, majority are Christians, many churches dedicate some days or Sundays to teach their member some of these non-communicable diseases, their causes and management and prevention, Findings from the study show a low level of compliance as 61.3% of the respondents had poor compliance to treatment regimen. This is in line with the study conducted by Taruna (2014) which revealed that majority of the respondents had poor compliance with treatment regimen (61.5%).
Similar findings were reported by Taruna (2014), in India who revealed that 61.5% of the respondents were non complaint to treatment, as only 23.3 and 31.7% of the participants were found to be compliant to diet and exercise regimen. Further collaborating the findings of this index study is Simon (2007), in Washington. Who revealed that non-compliance was common among patients prescribed oral hypoglycaemic medications; the average population of non-compliance was 53.7%. 47.8% of the population engaged in exercise sessions only once a week or less, whereas 10% reported that they rarely followed a healthy diet plan. However, in contrast with these findings is that of Nadia (2011), in Egypt who reported that more than half of the patients (56.3%) had adequate total compliance to diabetes management. The highest compliance was with follow up (88.8%) while the lowest compliance was with self-care activities (17.5%) and self-testing (36.3%). Also, Samia (2010) revealed that majority of the patients (78%) adhered to medical treatment prescribed, and 60% had good compliance with diet regimen. Furthermore, Abdulazeez (2014), Ilorin Nigeria reported 58% of the respondents in his study were found to be compliant with their medication were while 42% were not compliant. Nadia (2011) study also differs from the findings of this index study, the study shows that more than half of the respondents were compliant (56.3%). Many factors could be attributed to the poor compliance reported in this index study; lack of finance, diabetic medications and investigations being too expensive and unavailability of the medication in the hospital were the major reason given by the respondents.
This reason might be connected to the fact that majority of the respondents were single who by implication may not have a job, are job seeker or even students as reported in the study. This no doubt might have resulted in the poor compliance as diabetic treatments are quite expensive and life style medications that accompany it need money for it to be effective. However this is another area that calls for more studies. This study found significant relationship between the level of compliance and demographic characteristics of the respondents like sex (p=0.0011), religion (p=0.040) and ethnic group (p=0.007) but showed no significant relationship with age, marital status, educational level and occupation (p = 0.999, 0.691, 0.388 and 0.483). There is also a highly significant relationship (p=0.000) between the knowledge of diabetes and rate of compliance of the respondents. This shows that the more knowledgeable a patient is about diabetic, the more the rate of compliance to treatment. More also, a significant difference was found in the level of knowledge of diabetes between the two hospitals (p. = 0.000) with respondent in UBTH having more knowledge than those in central hospital. Similarly, there was a significant relationship in the rate of compliance to diabetic regimens between the hospitals (p = 0.010) as those in UBTH were more compliant to treatment than those in central hospital, this might be associated to the higher knowledge reported by the respondents in UBTH.
There appears to be a high level of knowledge about diabetes, and the effect of family support towards diabetic patients is good. However, the rate of compliance was poor; this therefore means that the nurses and medical personnel need to enlighten the patients on the importance of compliance to treatment regimen.
IMPLICATION FOR NURSING AND OTHER HEALTH CARE PROFESSIONALS
Due to the important role nurses play in health care, they are in the best position to educate and provide enlightenment to these patients so as to enhance the compliance to diabetic treatment, educating patients on diabetes, causes and various complications. Creating a good nurse and patient relationship in order to give room for patient to confide in the nurse is also recommended. Good interprofessional relationship with other health care professionals’ for example, doctors, pharmacist etc is needed to ensure that patients are seen regularly and drugs given to them regularly as well is one of the key to encourage compliance among patients.
(1) Government should subsidize the cost of management of diabetes, for example, drugs and laboratory investigations
(2) More community health facilities should be established to reduce the travelling distance of these patients going for check-up.
(3) Government in conjunction with the health facility should ensure the pharmacy of the government-owned hospitals is well stocked to reduce the burden of searching for prescribed medications in private pharmacy at exorbitant prices.
SUGGESTIONS FOR FURTHER STUDIES
Study should be conducted on the following:
(1) Factors affecting the level of compliance with treatment regimen among diabetic patients in selected rural communities of Edo state.
(2) Satisfaction with treatment regimen among diabetics patient attending selected tertiary institution in south-south Nigeria.
(3) Perception of health care workers towards compliance of diabetic patients to treatment regimen in selected hospitals in Edo state.
The authors have not declared any conflict of interests.
REFERENCES
|
Abdulazeez FI, Omole M, Ojulari SL (2014). Medication adherence amongst diabetic patients in department of clinical pharmacy, university of Ilorin, Kwara State. Trop. J. Pharm. Res. 13(6):997-1001.
Crossref
|
|
|
|
Adejoh SO (2014). Diabetes Knowledge, Health Belief, and Diabetes Management among the Igala, Nigeria SAGE Open. pp. 1-8.
Crossref
|
|
|
|
|
Alberta DN Mildred J, Ekaette FA, Mgbeken MA Ndiok A (2010). Diet and activity control reginems;compliance amomg congestive cardiac failure clients. Niger. J. Nurs. 1(3):15-20.
|
|
|
|
|
Amokute CC, Hussein S (2011). Screening of King Saud University community of diabetes mellitus. Pract. Diabetes Mellitus". pp. 87-88.
|
|
|
|
|
Chutiyami M, Umar NT, Salihu D (2016). Non-compliance with treatment regimen among clients with diabetic M in university of Maiduguri teaching hospital, North-Eastern Nigeria. J. Res. Nurs. Midwifery 5(1):011-020.
|
|
|
|
|
Donnan PT, MacDonald TM, Morris AD (2011). Adherence to prescribed oral hypoglycemic medications in Tayside centre for general practice, department of medicine, university of Dundee Uk". Diabetic Med. 1(17):1464-5491.
|
|
|
|
|
Evans CE, Haynes RB (2013): Patients compliance. In: Rakel RE, Ed. "Essentials of family practice Philadelphia", WB Saunders Company. pp. 103-118.
|
|
|
|
|
Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X (2008). Intervention for enhancing medication adherence. Cochrane database system review 2: CD0000011 10.1002/14651858.CD000011.PUB3 (PUBMED)
Crossref
|
|
|
|
|
Isara AR, Okundia PO (2015). The burden of hypertension and diabetes mellitus in rural communities in southern Nigeria. Pan Afr. Med J. 20:103.
Crossref
|
|
|
|
|
Jansirani N (2013). Diabetic compliance; a qualitative study from patients perspective in developing countries. IOSR J. Nurs. Health Sci. (IOSR-JNHS). 1(4):29-38.
|
|
|
|
|
Nadia MT, Abdel-Azeaz M, Bahia GA (2011). Factors affecting compliance of diabetic patients towards therapeutic management in the department of medical-surgical nursing, Zagazig university hospital, Zagazig. Med. J. 79:211-218.
|
|
|
|
|
Nwaokoro JC, Okokon BE, Nwaokoro AA, Emerole CO, Ibe SN, Onwuluri V. Aputa RN, Chukwuocha UM (2010). Problems associated with treatment compliance among type 2 diabetic patients in federal university of technology, Owerri, Imo State. Afr. J. Diabetes Med. 22(1):148-226.
|
|
|
|
|
Omorogiuwa A, Oaikhena GA, Okioya P, Akubueze D, Owobu E, Enahoro I (2010). Diabetes mellitus: Prevalence amongst university staff in Southern Nigeria and attitude towards routine glycemic/glucosuric checkup. Int. J. Biomed. Health Sci. 6:25-29
|
|
|
|
|
Samia MT, Ashraf AE (2010) .Compliance of diabetic patients to therapeutic regimen in medical-surgical nursing and internal medicine department, Assiut University": Ass. Univ. Bull. Environ. Res. 6:289-371.
|
|
|
|
|
Simon GE, Lin HB, Wayne. K, Katon WR, Ciechanowski P, Oliver MC, Evette JL, Bush T, Young B (2007). Relationship of depression and diabetes self-care, medications, adherence and preventive care. 5:279-308.
|
|
|
|
|
Taruna S, Juhi K, Dhasmana DC, Harish B (2014). Poor adhercence to treatment: a major challenge in diabeteis. JIACM 2014 15:26-29
|
|
|
|
|
World Health Organisation (2011). Management of Peripheral Arterial Disease, Geneva. Available at:
View.
|
|