Full Length Research Paper

ABSTRACT
Seasonal malaria chemoprevention (SMC) is effective to prevent malaria in children 3 to 59 months in the Sahel region. Mother’s seasonal malaria chemoprevention related knowledge and attitudes and the coverage of the strategy among targeted children were assessed. A cross-sectional survey was conducted in 1828 children aged 3 to 59 months from November 7 to 18, 2018 in eight health regions of Burkina Faso where SMC was implemented with Malaria Consortium supported fund. Data were collected using structured questionnaire and direct inspection of SMC card. MAGPI software was used for data collection and STATA 12.0 was used for the analysis. A total of 1828 children 3 to 59 months were enrolled and 951 mothers interviewed on different aspects of SMC. Overall, the SMC coverage was high for single cycle or for cumulative coverage basis. Single cycle coverage increased over rounds, from mother and tutor's interview (from 87.09% (1592/1828) to 91.19% (1667/1828); p=0.001). Over 91.18% (869/951) knew that SMC objective was to prevent malaria. Overall SMC was well tolerated and most 95.2% (296/320) of mothers and tutors surveyed owned treated bed nets. Despite combining high coverage and treated bed-net use, at least 16.19% remained rapid diagnosis test positives during the survey. SMS coverage was high in the current survey and most mothers knew the relevance of SMC administration with high bed-net coverage.
Key words: Coverage, seasonal malaria chemoprevention, children 3 to 59 months, Burkina Faso, 2018.
INTRODUCTION
Seasonal malaria chemoprevention (SMC) is a strategy which administers therapeutic doses of antimalarial medications to children aged 3 to 59 months during the period of high malaria transmission, to prevent them from contracting the disease (Wilson and IPTc, 2011). This strategy, formerly called Intermittent Preventive Treatment of Malaria in Children (IPTc), administers a combination of sulfadoxine-pyrimethamine and amodiaquine for three days. The epidemiology of malaria in Burkina Faso is dominated by a high prevalence and incidence, especially in the rainy seasons . Burkina Faso is one of the 10 countries in sub-Saharan Africa that host 70% of the global malaria burden (WHO, 2018). According to the report for health statistics in 2018 by the Ministry of Health, malaria was the first reason for consultations in all health facilities (peripheral level, medical centers and hospitals), accounting for 67.2% of all consultations (MoH, 2018). Severe malaria ranked first as the cause of death over the same period with 16.4% in hospitals and medical centers, and 36.3% in peripheral health facilities in children under five years old (Ministry of Health, 2019).
The effectiveness of SMC has been demonstrated in clinical trials conducted in the Sahel region (Bojang et al., 2010; Cisse et al., 2009; Dicko et al., 2011; Konate et al., 2011; Zongo et al., 2015) where it is likely to have a beneficial effect for the target children (Cairns et al., 2012). Following these successes in malaria prevention (Wilson and IPTc, 2011), the World Health Organization (WHO) endorsed the strategy and recommended it for all Sahelian countries where malaria transmission is highly seasonal (WHO, 2012). Starting in 2014 with a pilot introduction in Séguénéga, Tougan, Boussé, and Kongoussi health districts, the implementation quickly spread out nationwide in 2018, with the financial support of international donors.
Coverage surveys conducted at the end of distribution campaigns between 2015 and 2017 (Zongo et al., 2018) showed very high coverage. In order to ensure that high coverage is achieved in 2018, this survey was carried out to estimate the coverage and describe the mother’s seasonal malaria chemoprevention related knowledge and attitudes.
MATERIALS AND METHODS
This assessment was carried out in the Hauts Bassins, Cascades, North and Central Plateau health regions between November 7 and 18, 2018. These sites are pre-defined sites and supported through Malaria Consortium. These sites are spread out over the different transmission settings of malaria: the long transmission area (Haut Bassin and Cascades), the medium transmission area (Centre West, Centre North, Centre South, Centre East and Plateau Central) and the short transmission setting (North).
Study population and eligibility
The study population was children aged 3 months to 10 years of both sex living in the targeted districts at the beginning of the campaign; and children who had recently immigrated into the districts. Children born during the campaign and who reached 3 months were eligible to receive preventive chemotherapy.
Study design
This was a descriptive cross-sectional epidemiological survey.
Sampling procedure
A total of 55 villages (clusters) were selected as pe proportional to cluster size technic. All villages from each district were listed with their respective population (general and under 5 years old). Then a random number was chosen between 1 and the cluster pitch; the number of clusters being the quotient of the total population under 5 years of age over the expected number of clusters (55 clusters).
After the clusters were selected and in the absence of a sampling frame, we proceeded as follows for the selection of compounds, households and children. The survey team once in the center of the village threw a ball-point pen and walked in the direction the pen pointed. The first compound to be investigated was chosen in the direction indicated by the pen. In this compound, households were systematically surveyed. In case there is no eligible child in the household, the team progressed step by step to the next compound until they got the desired size. If the expected size was not reached at the end of the compound from the initial direction, the team from the last concession turned (right or left by random choice) and continue until they reached the required size.
This study was conducted in collaboration with Malaria Consortium office in Burkina Faso, who sent one technical staff (qualified as Monitoring and Evaluation Specialist) to train the team in the use of the MAGPI software, the dedicated software for data collection in the coverage surveys carried out by Malaria Consortium. The research team organized a two-day training which covered the protocol of the survey, the data collection tools, the procedure for administering the informed consent, the first step in the data collection process and finally a pre-test of the tools. Then additional training and reorganization of the questionnaire were carried out.
Data collection and management
Data collection consisted of an interview on socio-demographic characteristics and information (period of administration, sensitization messages, persons in charge of the drug distribution, strategy of distribution) on the seasonal malaria chemoprevention. The data were collected on electronic devices (Android) in the selected villages over three weeks by data collectors. Data collected were later transferred to the MAGPI platform. The data was extracted from the platform for cleaning purposes . The clean data were then re uploaded into the server and ready for analysis.
The number of concessions to visit was determined according to the following formula:
n = (z a) 2 p (1 – p ) / d 2.
Assuming that the coverage rate of the concessions is around 50% (cut -off of 50% gives a maximum size), the expected sample size is 940 concessions accounting for cluster effect and non-respondents. Approximately, 17 compounds were visited per cluster and one mother was interviewed per compound. Although the coverage of SMC about children receipt of SMC, an in-depth interview was conducted with a randomly selected mother in each of the compounds visited to assess a number of parameters on SMC. While one mother was randomly selected per compound, all eligible children found in the compound household were included in the survey.
Data analysis
Data were analyzed with STATA software version 12.0. The number of children who received SMC was presented as proportions with 95% confidence intervals.
Ethical consideration
The protocol was approved by the Ethics Committee for Health Research of the Ministry of Health before the start of the survey. The study was clearly explained to the children's parents, and only children whose parents consented (provision of informed consent dated and signed by the parent) actually participated in the survey. Parents were informed that participation in this study was entirely voluntary and that they could stop their participation at any time without prejudice. The survey did not involve invasive methods and staffs were well trained in administering informed consent and maintaining the confidentiality of information collected about participants.
RESULTS
The socio-demographic characteristics of the enrolled mothers
During the survey, a total of 951 mothers were interviewed in 951 compounds in which 1828 children aged 3 to 59 months were identified. The questionnaire was administered about these 1828 children.
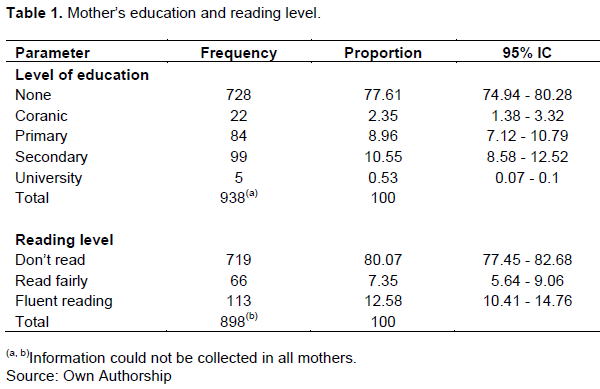
Most mothers had no formal education, 77.35% (736/951). Less than 1% (5/951) had high education while 2.44% (23/951) religious education (Table 1). Mother’s ability to read the message given during seasonal malaria chemoprevention sensitization sessions was also checked and it was found that 80.65% (766/951) could not read these messages.
SMC card ownership and mothers' knowledge of seasonal malaria chemo-prevention
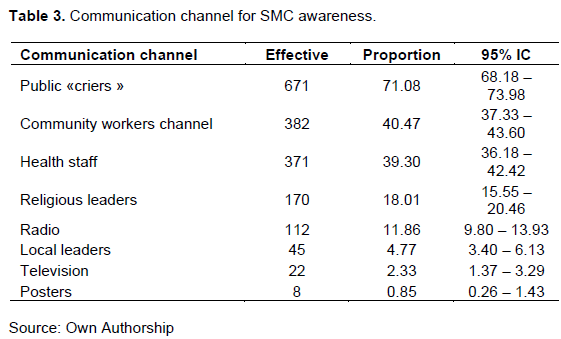
The survey which took place about a month after the last SMC visit, revealed that 81.18% (772/951) of the mothers questioned kept the SMC card. The interview revealed that more than 91.38% (869/951) of the mothers and guardians knew that the SMC was aimed at preventing malaria in their children, but still almost 2.84 (27/951) gave inadequate answers. A total of 99.89% (950/951) and 99.68% (948/951) of mothers, respectively knew the dosage for days 2 and 3 for the treatment. About a proportion, majority of mothers 68.6% (652/951) knew that the cards should be kept to report information on subsequent rounds of SMC (Table 2). About 64.51% (613/951) understood that doses given to children at home should be administered. Regarding the sources of information on SMC, mothers and guardians were most often informed by public criers 70.66% (672/951), community health workers 40.47% (382/951) and health workers 39.01% (371/951)

Use of insecticide-treated mosquito nets
Insecticide treated mosquito nets usage rate was 95.2% (1740/1828) during the study. Considering the children who slept under a mosquito net the day before the interview, malaria was diagnosed (positive TDR) in 15.3% of them.
Malaria during SMC period
According to the interview with the mothers/guardians, 19.04% (348/1828) of the children were sick during the period of SMC administration, most of them 91.95% (320/348) consulted a formal health facility. A rapid diagnostic test was performed on 92.5% (296/320) of sick children and 95.27% (282/296) tested positive.
Immediate tolerance and adverse events
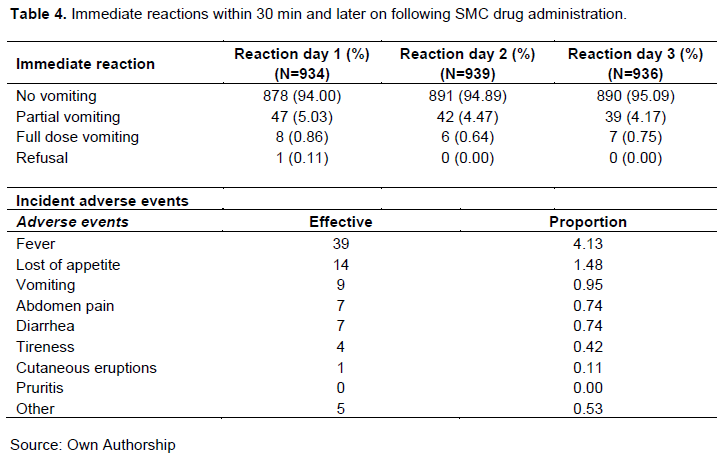
Table 3 indicates that 94.01% (894/951) of mothers reported that children did not vomit the first, second and third doses of SMC drugs; less than 1% vomited the entire doses or refused. Very few children presented adverse events following the administration of SMC with sulfadoxine -pyrimethamine plus amodiaquine. The most common signs were fever 4.10% (39/951), loss of appetite 1.47% (14/951) and vomiting 0.95% (9/951).
Coverage of seasonal malaria chemoprevention reported during the survey
A total of 1828 children aged 3-59 months were included in the survey. Each child had received an average of 3.55 cycles.
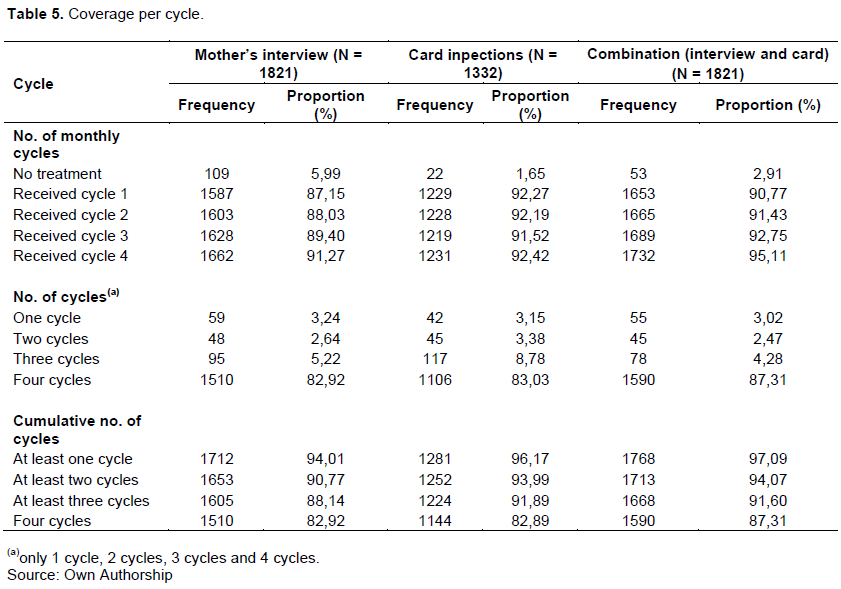
Monthly coverage of SMC had significantly increased over cycles (cycle 1 versus cycle 4, p?0.001 according to the interview of the mothers; direct inspection of SMC card did not reveal a significant progress, p=0.8842, cycle 1 versus cycle 4).
The survey revealed that around 94% of targeted children had at least one contact for SMC drug administration as per mother’ interview and more than 98% according to the cards (p?0.001). Table 5 indicates that 90.7% of children received at least 2 cycles of SMC according to the mothers against 93.99% according to the SMC cards direct inspection (p?0.001). Finally, the proportion of children completely treated was comparable according to the two sources (p=0.9101) even though significantly more children received at least 3 cycles according to the report of the cards compared to mother’s report (p?0.001) (Table 4).
DISCUSSION
Following the implementation of seasonal malaria chemoprevention, coverage surveys are regularly carried out to check whether the objective to reach all eligible children is achieved. The current survey was conducted about one month after the last round of the implementation of SMC in eight health regions. The survey found that a high proportion of mothers still have the SMC cards. Furthermore, the coverage rate (single cycle or cumulative cycles) significantly increased over the cycles in the study population according to mothers’ interview. A similar trend was observed according to direct inspection of SMC cards. The coverage rate by card was however, significantly higher than that reported by mothers. It can reasonably be concluded that the 2018 SMC implementation campaign achieved a very high level of coverage, an essential condition for achieving the strategy's objective to significantly reduce the prevalence and incidence of malaria in children 3 to 59 months in the study areas. This high coverage level is comparable to those reported in 2017 (Zongo et al., 2018) and between 2015 and 2016 (ACCESS-SMC Partnership, 2020). These particularly and regularly high rates are the result of the conjunction of several factors. Indeed, before the deployment of field teams, local awareness campaigns with public “criers” (person with a megaphone) are undertaken. The messages delivered concern the context of the SMC, its objective (prevention of malaria), the period of treatment, the importance of adhering to the three doses, the action to take in case a child is missed during home visit. These messages were repeated before the start of each cycle to remind the mothers and other guardians. This survey revealed the diversity of channels used to inform mothers, of which community “criers” remained the main channel through which most of the mothers got information about SMC.
The survey showed that nine out of 10 mothers/ guardians/caregivers knew that the purpose of SMC was to prevent the malaria. In addition to all these factors, it should be noted that the SMC drugs sulfadoxine -pyrimethamine and amodiaquine retain good clinical efficacy in the West African region in general and in Burkina Faso in particular. The survey also revealed that the immediate tolerance of the intervention was very good because more than 9 children out of ten received all the doses of the drugs without vomiting. The incidence of adverse events was relatively low as reported in other studies (ACCESS-SMC Partnership, 2020). This good tolerance certainly contributed to the good adherence of the mothers to the strategy. This survey has reported high coverage.
The results reported in this survey may have been impacted by the absence of a sampling frame at the village or cluster level allowing a random choice of concessions hence the use of alternative strategies. Sampling and the various sources for the coverage evaluation (interview of the mothers (recall bias) and on the SMC card. Nevertheless, the relatively short time between the end of the administration of the SMC and the implementation of the survey may have contributed to reduce such recall bias, Therefore, these findings retain a certain validity and usefulness.
CONCLUSION
The seasonal malaria chemoprevention coverage survey provided an opportunity to measure the results achieved in comparison with the objectives set at the start of the campaign. Although it revealed high levels of coverage, more efforts need to be made to raise awareness in order to improve current performance.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Bojang K, Akor F, Bittaye O, Conway D, Bottomley C, Milligan P, Greenwood BA (2010). Randomized Trial to Compare the Safety, Tolerability and Efficacy of Three Drug Combinations for Intermittent Preventive Treatment in Children. Keizer J, editor. PLOS ONE 5(6):e11225. |
|
|
Cairns M, Roca - Feltre A, Garske T, Wilson AL, Diallo D, Milligan PJ, Ghani AC, Greenwood BM (2012). Estimating the potential public health impact of seasonal malaria chemoprevention in African children. Nature Communication 3:881. |
|
|
Cisse B, Cairns M, Faye E, NDiaye O, Faye B, Cames C, Cheng Y, NDiaye M, Lô AC, Simondon K, Trape JF, Faye O, NDiaye JL, (2009) Randomized Trial of Piperaquine with Sulfadoxine -Pyrimethamine or Dihydroartemisinin for Malaria Intermittent Preventive Treatment in Children. Beeson JG, editor. PLOS ONE 4(9):e7164. |
|
|
Dicko A, Diallo AI, Tembine I, Dicko Y, Dara N, Sidibe Y, Santara G, Diawara H, Conaré T, Djimde A, Chandramohan D, Cousens S, Milligan PJ (2011). Intermittent Preventive Treatment of Malaria Provides Substantial Protection against Malaria in Children Already Protected by an Insecticide-Treated Bednet in Mali: A Randomised , Double-Blind, Placebo-Controlled Trial. Rogerson SJ, editor. PLoS Medicine 8(2):e1000407. |
|
|
Konate AT, Yaro JB , Ouédraogo AZ, Diarra A, Gansané A, Soulama I, Kangoyé DT, Kaboré Y, Ouédraogo E, Ouédraogo A, Tiono AB, Ouédraogo IN, Chandramohan D (2011) Intermittent Preventive Treatment of Malaria Provides Substantial Protection against Malaria in Children Already Protected by an Insecticide-Treated Bednet in Burkina Faso: A Randomised , Double-Blind, Placebo-Controlled Trial. Rogerson SJ, editor. PLoS Medicine 8(2):e1000408. |
|
|
Ministry of Health (MoH) (2018). Health Statistics Yearbook 2017 [Internet]. |
|
|
Ministry of Health (MoH) (2019). Health Statistics Yearbook 2018 [Internet]. |
|
|
Wilson AL, IPTc Taskforce (2011). A systematic review and meta-analysis of the efficacy and safety of intermittent preventive treatment of malaria in children (IPTc). PloS ONE 6(2):e16976. |
|
|
World Health Organization (WHO) (2018). Partnership to End Malaria. High burden to high impact: a targeted malaria response. Report No.: WHO/CDS/ GMP. |
|
|
World Health Organization (WHO) (2012). WHO policy recommendation: seasonal malaria chemoprevention (SMC) for Plasmodium falciparum malaria control in highly seasonal transmission areas of the Sahel sub-region in Africa. March, 2012. |
|
|
Zongo I, Milligan P, Compaore YD, Some AF, Greenwood B, Tarning J, Rosenthal PJ, Sutherland C, Nosten F, Ouedraogo JB (2015) Randomized Noninferiority Trial of Dihydroartemisinin -Piperaquine Compared with Sulfadoxine -Pyrimethamine plus Amodiaquine for Seasonal Malaria Chemoprevention in Burkina Faso. Antimicrobial Agents Chemotherapy 59(8):4387-4396 |
|
|
Zongo I, Ouedraogo JB, Lal S, Cairns M, Scott S, Snell P, Moroso D, Milligan P (2018). Coverage of seasonal malaria chemoprevention in Burkina Faso 2017 P 46. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


