Full Length Research Paper

ABSTRACT
Hepatitis B is the world’s most common serious liver infection caused by Hepatitis B virus (HBV). Rate of vertical transmission is very high from infected mother to baby and has adverse effect on both. A cross-sectional study involving a total of 384 pregnant women attending Gandhi Memorial Hospital in Addis Ababa from April to June 2017 was conducted to determine the seroprevalence and risk factors of HBV among the clients. A structured questionnaire was used to collect socio-demographic data and information regarding possible risk factors for HBV infection and screening was performed by emmuno-chromatographic method using advanced quality one step hepatitis B surface antigen (HBsAg) test card. The seroprevalence of HBsAg among the participants was 2.3%, which is a moderate prevalence according to the WHO classification. HBsAg positivity was significantly associated to age (P=0.020) and ethnic group (P=0.023). About 67% of the HBsAg positive participants belonged to the Gurage ethnic group. No significant association was found between HBsAg positivity and other variables such as marital status (P=1.00), history of multiple sexual partners (P=0.740), history of blood donation (P=1.00), history of tattooing (P=0.070), and history of female genital mutilation (P=0.188). Further study should be conducted to identify the reasons for the highest prevalence of the HBsAg among women from Gurage ethnic group.
Key words: Chronic hepatitis, pregnancy, hepatitis B virus, vertical transmission.
INTRODUCTION
Hepatitis is an inflammation of the liver, most commonly caused by a viral infection. Of these viruses, hepatitis B virus (HBV) and hepatitis C virus infections account for a substantial proportion of liver diseases worldwide. Hepatitis B is a viral disease process caused by the HBV. The virus is endemic throughout the world. It is shed in all body fluids by individuals with acute or chronic infection (Hailay et al., 2014). Hepatitis B virus is easily transmitted to non-immune persons, via contact with infected blood or body fluids such as saliva; hence, it could be acquired through blood transfusion with infected blood, intimate sexual contact, particularly during unprotected sex, sharing of contaminated sharp objects such as needles, and close personal contact in over-crowded households.
It could also be transmitted from an infected mother to her un-born child through the placenta (Edia-Asuke et al., 2015). Perinatal and early childhood transmissions are the main routs of HBV infection in high and intermediate endemic areas. Administering HBV vaccination to 90% of newborns within 24 h from birth would prevent 84% of global HBV-related deaths (Umare et al., 2016).
Worldwide, HBV is a major cause of primary cancer of the liver, or hepatocellular carcinoma (HCC) (Jinlin et al., 2005) accounting for about 60 to 80% of the disease (Dessie et al., 2014). In 2012 alone, it is estimated that more than 2 billion people were infected with the virus of which about 350 million were chronically infected with 1.2 million annual deaths (Erena and Tefera, 2012; Dessie et al., 2014).
About 50% of HBsAg positive people are infected in the prenatal or neonatal period, especially in countries where HBV has a high prevalence (Hailay et al., 2014). Infants infected due to vertical transmission (mother to child) are nearly 90 % at higher risk of developing chronic liver disease and cancer (Dessie et al., 2014).
According to WHO Africa has the second largest number of chronic carriers after Asia and is considered as a region of high endemicity, despite the fact that the exact burden of hepatitis B in Africa is difficult to assess due to inaccurate records and under-reporting, it is estimated that between 70 and 95% of the adult population show evidence of past exposure to HBV infection and the estimated HBsAg seroprevalence ranges from 6 to 20% (Hailay et al., 2014). In Ethiopia, studies among pregnant women from some parts of the country have shown moderate endemicity with prevalence of HBsAg positivity ranging from 3 to 6.1% (Yeshi et al., 2016).
Viral hepatitis during pregnancy is associated with high risk of maternal complications and high rate of vertical transmission. Fetal and neonatal hepatitis acquired from mother during pregnancy lead to impaired cognitive and physical development in later life of the children Olaitan and Zamani 2010). About half of new infections result from vertical transmission during pregnancy, a statistic that is linked to the fact that HBV screening is not part of routine antenatal care in Africa and Asia (Tsegaye et al., 2016). Several studies around the world recommended that pregnant women should be screened for hepatitis B before delivery, as this offers an opportunity to prevent another generation from being chronically infected by the virus. However, in Ethiopia laboratory diagnosis of HBV infection is not part of routine care in ANC of all health facilities. Moreover, there is little information concerning seroprevalence of HBV infection among pregnant women and the existing data indicate that it differs from region to region (Tsegaye et al., 2016).
Antenatal screening for HBsAg to all pregnant women and vaccination of their babies at birth has been recommended widely, yet it is not a routine practice in most health settings of Ethiopia (Umare et al., 2016). Cross-sectional community studies of serological markers of HBV infection have an important role in identifying population endemicity, possible routes of transmission and associated risk factors and such data help in the development of appropriate control measures (Abebe et al., 2003).
Therefore, the aim of this cross-sectional study was to determine seroprevalence of HBV infection and to identify associated risk factors among pregnant women attended antenatal care (ANC) in Gandhi Hospital, Addis Ababa from April to June 2017.
MATERIALS AND METHODS
Description of the study area
The study was conducted at Gandhi Memorial Hospital which is one of the six hospitals running under Addis Ababa City Administration Health Bureau.
Study design and study population
A cross sectional study design was conducted from April to June 2017. The study population was all pregnant women who visited Gandhi Memorial Hospital to follow antenatal care service and were referred to the laboratory of the hospital by the physicians for different hematological diagnostic purposes during the study period and were willing to sign a written consent to provide additional 2 ml blood sample and to fill the questionnaire. Three hundred eighty-four consecutive pregnant women which qualified the inclusion criteria were selected for the study.
Study variables
The dependent variable in the study was serological result for hepatitis B virus surface antigen (HBsAg) of pregnant women involved in the study while the independent variables were having multiple sexual partner in life, blood donation history, history of abortion, history of FGM, history of teeth extraction, history of surgery, history of contact with jaundiced person, history of using barberry machine, history of nose piercing, history of ear piercing, ethnic group of the study participants.
Data collection
Data were collected through structured questionnaire focused on independent variables like socio-demographic characteristics, history of abortion, blood donation, surgery, and ethnic group of the study participants. The questions were read face-to-face for each participant by the first author and the responses were recorded.
Following the questionnaire, 5 ml of blood sample was taken from each participant by laboratory technitians, 3 ml of the collected blood was used for different diagnostic purpose based on the laboratory request they brought to the laboratory and the remaining 2 ml of blood was transferred to serum separator tube, centrifuged and stored in refrigerator in 2 to 8°C for later analysis.
The serum from each blood sample was tested for the presence of HBsAg according to standard operating procedure of HBsAg test of the Hospital using rapid diagnostic tests employing the principle of immune chromatography using Advanced Quality One step HBsAg test card (InTech products, INC. China) following the procedure given by the manufacturer.
Immune chromatography test for diagnosing HBsAg in the serum
The Advanced Quality One step HBsAg test is a colloidal gold enhanced immunoassay for determination of HBsAg in human whole blood, serum or plasma. Anti-HBsAg antibody is immobilized in the test region on nitrocellulose membrane. During the assay the specimen was allowed to react with the colored conjugate (antibody-colloidal gold conjugate); the mixture then migrates chromatographically on the membrane by the capillary action. An HBsAg positive specimen produces a distinct red or pink color band on the test region, formed by the specific antibody-HBsAg colored conjugate complex. Absence of this colored band on the test region suggests a negative result. The same colored band always appears in the control region serving as procedural control regardless of the test result.
Interpretation of the results
Appearance of one red or pink line in the control line and absence of line in test region was indicative of negative result. Appearance of a distinct red or pink color band in the test region, in addition to a red or pink colored control line was it indicative of positive result. A positive result may develop even sooner at a high viral concentration of HBsAg in the serum. However, the lower the concentration of HBsAg, the longer time it takes to develop a color band on a test region; therefore, a negative result should be determined at 15 min to insure it is truly negative instead of weak positive.
A total absence of color in both regions or the formation of color in test region in the absence of color in control region is an indication of procedure error or the test reagent has deteriorated (invalid). The test should be repeated using a new test card.
Quality control
The validity and completeness of the data were daily verified by the principal investigator and the performance of the Advanced Quality One step HBsAg test was evaluated using the internal quality control of the test and by known positive and known negative blood serum controls obtained from National Blood Bank which was ELISA-tested.
Data analysis
Data collected through questionnaires were entered into Microsoft office Excel and processed using SPSS version 24 statistical software for comparison and testing the relationship of HBsAg positivity and various variables included in the study. Chi-square test was used for bivariate analysis of the association between HBsAg seropositivity and the independent variables (predisposing factors). P value < 0.05 at 95% CI was considered as statistically significant. Percentage frequencies of Positive and Negative participants for HBsAg for the different independent variables were also calculated and compared.
Ethical consideration
Ethical clearance was obtained from Addis Ababa Regional Health Bureau. Written consent was obtained from respondents and data were collected and handled confidentially. No name of the respondents was written and only numerical codes were used on the questionnaire.
RESULTS
Socio demographic characteristics
Socio demographic characteristics of the participants and prevalence of HBsAg in relation to risk factors among pregnant women attending antenatal care at the hospital are depicted in Tables 1 and 2. Of the 384 pregnant women participated in the study, most (49%) of them were in the age group of 25-29 years followed by 30-34 years (24.5%). Most of them (96.9%) were married. About 29% (n = 112) were educated up to college and above, most (44.5%) of them had formal education of grades 5-10 while only 8.3% had no formal education. Majority (50.8%) of the pregnant women involved in the study were housewives followed by private employee (25%) and government employees (11.7%). Most of the participants (94.8%) resided in Addis Ababa and about 27% earn below 1000 birr while an equal percentage earn over 2000 birr monthly.
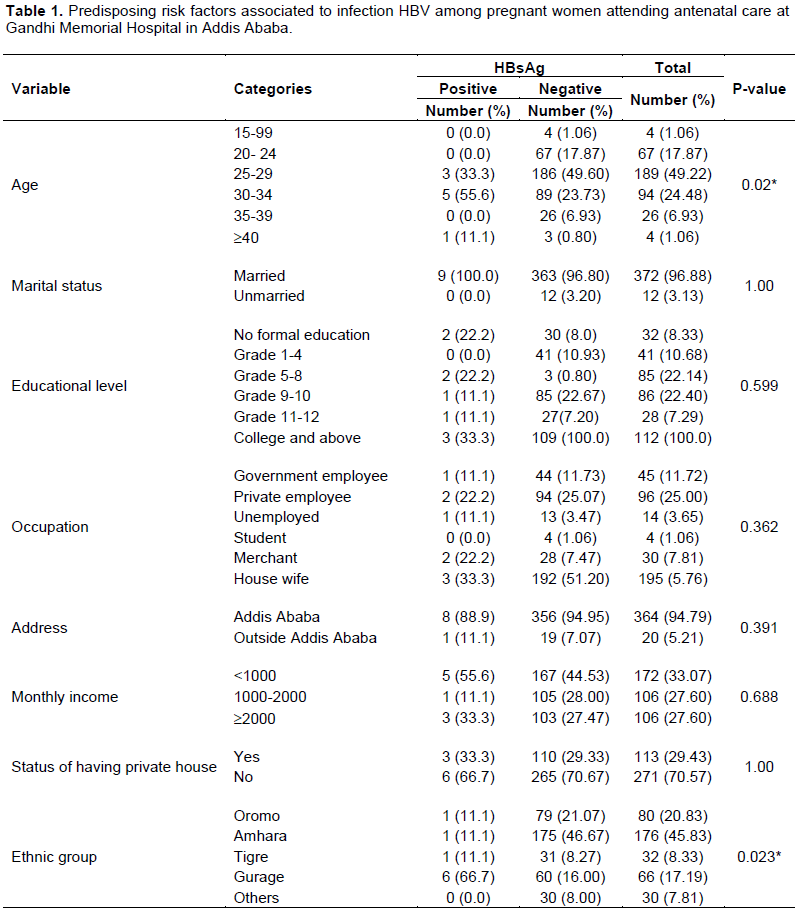
The highest percentage of the participants belonged to Amhara (46.8%) ethnic group followed by Oromo (20.8%) and Gurage (17.2%) in order. However, 66.7% of the HBsAg positive women belonged to Gurage ethnic group and the result showed that there was statistically significant association (P = 0.023) with respect to ethnic group.
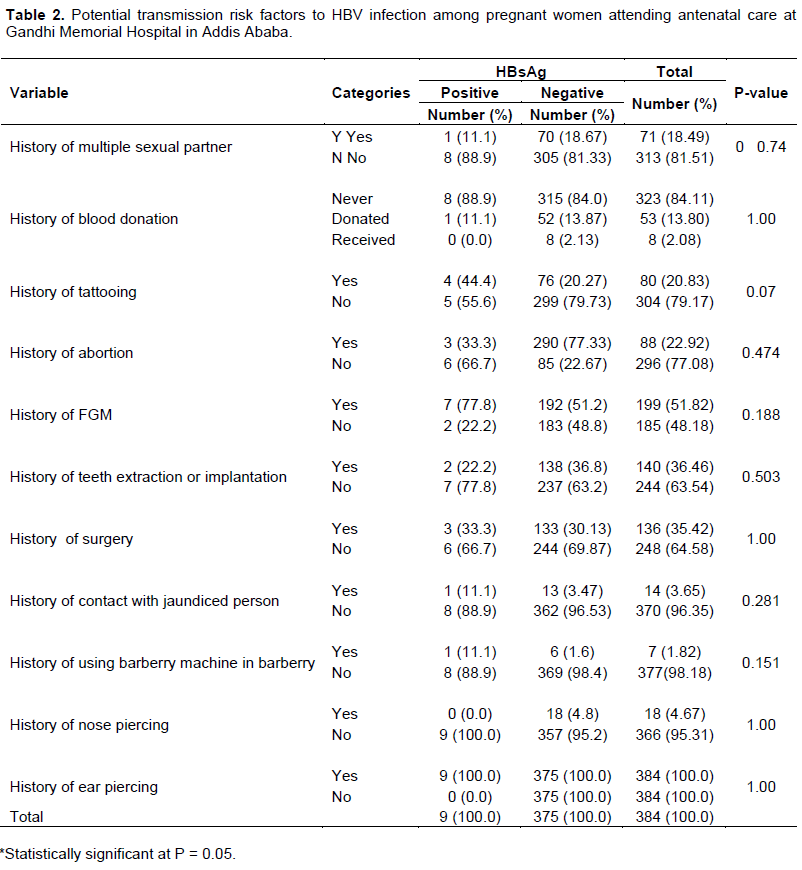
Only 2% (n = 8) of the total participant had received blood and all of them were found HBsAg negative. About 19% (n = 71) had history of multiple sexual partners and of these only about 1% (n = 1) was HBsAg Positive. About 23 and 52% of the participants had history of abortion and female genital mutilation, respectively.
Of the study participants (N = 384) only about 2.3% (n = 9) were found to be HBsAg positive and none of them had acute clinical hepatitis. Most (55.5%) of the seropositive individuals were found in the age group 30-34 followed by 25-29 (33.3%). Most (94.8%) of the participants were from Addis Ababa and also most (88.9%) of the seropositive were from this area.
Of the different variables considered as associated risk factors, HBsAg positivity was significantly correlated only with age group (P = 0.02) and ethnicity (P = 0.023). Of the total seropositive pregnant women (n = 9), most (66.6%) of them belonged to Gurage ethnic group. However, no significant association (P > 0.5) was found between HBsAg positivity and other variables such as marital status, monthly income, history of multiple sexual partners, history of blood donation, history of tattooing, history of female genital mutilation and history of using barberry machine in barberry. Most (78%) of the HBsAg seropositive individuals had history of female genital mutilation (FGM).
DISCUSSION
This study showed that the prevalence of HBsAg seropositivity in the tested pregnant women was 2.3% and it is moderate according to WHO (2017) criteria of classification of the level of endemicity of HBV infection. The prevalence of chronic HBV infection is categorized as high (≥ 8%), intermediate (2-7%), and low (< 2%) (Tsegaye et al., 2016). The result was lower than the prevalence of HBV reported in previous similar studies conducted in Addis Ababa and different regions of Ethiopia outside Addis Ababa. Walle et al. (2008) reported 5.3% prevalence among pregnant women in Debre Tabor Hospital, 3.7% in Jimma and its neighboring towns (Mohammed and Solomon, 2005), 3.8% in Bahir Dar city (Yohannes et al., 2014), 7.8% in southern Ethiopia (Yeshi et al., 2016). Similarly, 4.7% prevalence of HBV was recorded among blood donors in Arbaminch (Ayele and Gebru, 2016), 3.73% among blood donors in Dire Dawa (Yosef and Tadesse, 2016), 7.4% among individuals visiting Goba General Hospital, southeast Ethiopia (Erena and Tefera, 2012), and 5.7% among visitors of voluntary counseling center of Shashemene Hospital (Asfaw et al., 2011).
In a community-based sero epidemiological survey in Addis Ababa, a prevalence of 7% of HBV was recorded (Abebe et al., 2003) and it was 3% among delivering women in St. Paul’s Hospital Millennium Medical College and Selam Health Center (Dessie et al., 2014). The lower prevalence of HBV among pregnant women in this study could be because of better current community awareness towards HIV/AIDS which has mostly the same transmission route with HBV and partly it can be attributed to the fact the poor women do not have access to hospitals due to economic reasons and thus visit public health stations/clinics where they can get treatment with reasonable price. Belyhun et al. (2016) also reported that a recent systematic review and meta-analysis about Hepatitis viruses in Ethiopia shows a decreasing pattern of overall HBsAg prevalence rate in general population. This might be because of prevention and control measures done for prevention of HIV as both infections are sexually transmitted and this could indicate a need for integrating HBV management to the HIV prevention and control programs in Ethiopia.
Of the different variables considered as associated risk factors, HBsAg positiveity was significantly correlated only with age group (P = 0.02) and ethnicity (P = 0.023). Most (55.5%) of the seropositive individuals were found in the age group 30-34 followed by 25-29 (33.3%). The highest prevalence in the former age group can be accounted for the increasing risk of exposure with time. There is no uniformity among the results of different studies on seroprevalence of HBV conducted in different parts of the country with respect to age group. Yosef and Tadesse (2016) reported higher prevalence in 33-40 age group in a study conducted in Dire Dawa among blood donors and Mohammed and Solomon (2005) reported similar seroprevalence in all age groups in a study conducted in Jimma. Based on the fact that all the seropositive pregnant women participated in the study were married, it is predictable that at the age levels of 29-34, most women come to marriage and become sexually active with great probability of practicing unprotected sex with their spouse. As a result this age related serological result of the study indicated that sexual intercourse mainly in marriage might be the main route of transmission of HBV in the study area which is comparable to the result of the study conducted in Jimma town and its surrounding in which sexual contact and vertical transmission are identified as a means of transmission Mohammed and Solomon (2005).
Although level of education is known as the determining factor for HBV infection which might be due to the level of awareness, according to the finding of the present study, higher seroprevalence (33.3%) was observed among pregnant women having college and above education level. Accordingly, literacy and income had no association with HBsAg positivity in this study which is contrary to the study conducted among pregnant women in Jimma (Mohammed and Solomon, 2005) and the study conducted among pregnant women in southern part of Ethiopia (Yeshi et al., 2016) which showed high HBsAg positivity rate among with no formal education and those with low income. This could be because of better community awareness in in Addis Ababa city about sexually transmitted infection than in Jimma and its surrounding towns.
Although other studies conducted in Ethiopia have reported that blood transfusion (Yohannes et al., 2014), body tattooing (Eke et al., 2011), circumcision (Elsheikh et al., 2007), and surgery (Walle et al., 2008) were potential risk factors for HBV infection. In this study in general, risk factors such as history of multiple sexual partner, blood transfusion, history of surgery, tooth extraction and implantation, contact with jaundiced person, tattooing, nose and ear piercing, abortion and shaving hair at barberry were not associated with HBV infection. This result is comparable with the former study conducted in pregnant women in southern Ethiopia (Yeshi et al., 2016), but contrary to the study conducted among visitors of Shashemene General Hospital voluntary counseling and testing center in which FGM, tooth extraction, abortion, ear piercing, unsafe injection and hospital admission were significantly associated to HBV infection (Asfaw et al., 2011).
The result showed that there was statistically significant difference (association, P < 0.05) between HBsAg positivity and ethnic group. The highest percentage of the participants belonged to Amhara (46.8%) ethnic group followed by Oromo (20.8%) and Gurage (17.2%). However, 66.7% of the HBsAg positive women belonged to Gurage ethnic group. Contrary to this result, in a similar study conducted in Jimma, Mohammed and Solomon (2005) reported zero prevalence among Gurage ethnic group and higher prevalence among Oromo ethnic group. Therefore, further study is required to investigate the reasons for the highest prevalence of HB infection in Gurage ethnic group living in Addis Ababa.
CONCLUSION AND RECOMMENDATION
The prevalence of HBsAg among pregnant women in the present study was 2.3%, which is a moderate prevalence according to the WHO criteria which justifies the need for routine screening of pregnant women in order to identify and treat the infection, so that risk of vertical transmission of the virus is reduced. In this study except age group and ethnic group of the participants of the study, none of the risk factors included in the study was associated with HBV infection. However, higher age specific and ethnic group specific prevalence of HBV infection was observed. Further study should be conducted to identify the reasons for the highest prevalence of the HBsAg among pregnant Gurage women to take intervention measures.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abebe A, Nokes DJ, Dejene A, Enquselassie F, Messele T, Cutts FT (2003). Seroepidemiology of hepatitis B virus in Addis Ababa, Ethiopia: transmission patterns and vaccine control. Epidemiology Infectious 131:757-770. Crossref |
||||
|
Asfaw A, Zufan S, Girmay M (2011). Prevalence of Hepatitis B surface antigen (HBsAg) among visitors of Shashemene General Hospital voluntary counseling and testing center. BMC Research Notes 4:35. Crossref |
||||
|
Ayele AK, Gebru MW (2016). Prevalence and associated risk factors of Hepatitis B and Hepatitis C virus among volunteer blood donors in Arba Minch Blood Bank SNNPR, Ethiopia; Journal of Medical Laboratory and Diagnosis 7(4):20-27. Crossref |
||||
|
Belyhun Y, Maier M, Mulu A, Diro E, Liebert UG (2016). Hepatitis viruses in Ethiopia: a systematic review and meta-analysis. BMC Infectious Diseases 16:761. Crossref |
||||
|
Dessie T, Kassu D, Belete T, Tesfaye T (2014). Seroprevalence and transmission of hepatitis B virus among delivering women and their new born in selected health facilities, Addis Ababa, Ethiopia: a cross sectional study. BMC Res Notes 7:239. Crossref |
||||
|
Edia-Asuke UA. Abubakar Z, Asuke S (2015). Seroprevalence of Hepatitis B Infection among out Patients Attending a Public Tertiary Hospital in Kaduna State, Nigeria. Tropical Medicine Surgery 3:189. doi:10.4172/2329-9088.1000189 Crossref |
||||
|
Eke AC, Eke UA, Okafor CI, Ezebialu IU, Ogbuagu C (2011). Prevalence, correlates and pattern of Hepatitis B surface antigen in a low resource setting. Virology Journal 8:12. Crossref |
||||
|
Elsheikh RM, Daak AA, Elsheikh MA, Karsany MS, Adam I (2007). Hepatitis B virus and hepatitis C virus in pregnant Sudanese women. Virology Journal 4:104. Crossref |
||||
|
Erena S, Tefera E (2012). Prevalence of hepatitis B surface antigen (HBsAg) and its risk factors among individuals visiting Goba General Hospital, South East Ethiopia. BMC Research Notes 7:833. http://doi.org/10.1186/1756-0500-7-833. Crossref |
||||
| Hailay A, Fikru D, Sahilu A (2014). Sero- Prevalence of HBSAg and factors among pregnant women in Ethiopia. Lap Lambert Publishing P 62. | ||||
|
Jinlin H, Zhihua L, Fan G (2005). Epidemiology and Prevention of Hepatitis B Virus Infection. International Journal of Medical Sciences, 2(1):50-57. Crossref |
||||
|
Mohammed A, Solomon G (2005). Seroprevalence of HBsAg and its risk factors among pregnant women in Jimma, Southwest Ethiopia. Ethiopian Journal of Health Development 19(1):45-50. Crossref |
||||
| Olaitan AO, Zamani LG (2010). Prevalence of hepatitis B virus and hepatitis C virus in ante-natal patients in Gwagwalada-Abuja, Nigeria," Report and Opinion 2(7):48-50. | ||||
|
Tsegaye Y, Zerihun Z, Nega C (2016). Seroprevalence and Predictors of Hepatitis B Virus Infection among Pregnant Women Attending Routine Antenatal Care in Arba Minch Hospital, South Ethiopia. Hepatitis Research and Treatment. Crossref |
||||
|
Umare A, Seyoum B, Gobena T, Hailemariyam T (2016). Hepatitis B Virus Infections and Associated Factors among Pregnant Women Attending Antenatal Care Clinic at Deder Hospital, Eastern Ethiopia. PLoS ONE 11(11):e0166936. Crossref |
||||
| Walle F, Asrat D, Kasu, Alem A, Tadesse E (2008). Prevalence of hepatitis B surface antigen among pregnant women attending antenatal care service at Debre-Tabor Hospital, Northwest Ethiopia. Ethiopia Journal of Health Sciences 17(1). | ||||
|
World Health Organization (WHO) (2017). Weekly epidemiological record 92(27):369-392 |
||||
|
Yeshi M, Walelign D, Ibrahim A, Anteneh A (2016). Seroprevalence and associated risk factors of hepatitis B virus among pregnant women in southern Ethiopia: a hospital-based cross-sectional study. Epidemiology and Health 38:e2016027. Crossref |
||||
|
Yohannes Z, Wondemagegn M, Mulat Y, Bayeh A (2014). Sero-prevalence and risk factors of hepatitis B virus and human immunodefciency virus infection among pregnant women in Bahir Dar city, Northwest Ethiopia: a cross sectional study. BMC Infectious Diseases 14:118. Crossref |
||||
|
Yosef H, Berhanu S, Tadesse A (2016). Hepatitis B Virus Infection and Associated Factors among Blood Donors at Dire Dawa, Eastern Ethiopia. Journal of Antivirals and Antiretrovirals 8(4):103-106. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


